
Abstract
Background:
Community-based studies on postpartum depression (PPD), a major maternal and public health issue, are scarce in India. We aimed to assess the proportion of postpartum mothers with depressive symptoms in the Malappuram district of Kerala and examine the correlates of PPD in this group.
Methods:
Between August and December 2024, we recruited eligible postpartum mothers using a cross-sectional, community-based design through a multistage cluster sampling procedure. We used the Edinburgh Postnatal Depression Scale to screen the sample for PPD symptoms. Multivariable linear regression analysis was employed to investigate the relationship between socio-demographic, maternal, or infant-related factors and postpartum depressive symptoms in mothers.
Results:
The mean age of the sample (N = 560) was 27.3 (±4.6) years. The mean years of education were 13.3 (±1.8) years. Eleven percent of women (n = 63) screened positive for PPD symptoms. Higher risk of PPD symptoms was linked to living separately from husband (B = 0.91, 95% confidence intervals [CI] = 0.17–1.65), adverse birth outcomes (B = 0.99, 95% CI = 0.17–1.82), antepartum depression (B = 8.26, 95% CI = 4.07–12.46), antenatal anxiety (B = 5.39, 95% CI = 1.07–9.71), and chronic diseases (B = 2.87, 95% CI = 0.78–4.96).
Conclusions:
More than one in 10 mothers reported PPD symptoms. Not living with a husband, anxiety or depression during pregnancy, maternal chronic illnesses, and adverse pregnancy outcomes were all linked to PPD symptoms. These findings suggest the need for routine mental health screening during postnatal and immunization visits. Integrating screening using task-shifting models may enhance sustainability and scalability.
One out of 10 mothers studied was at risk of postpartum depression (PPD). Factors linked to PPD symptoms included living separately from a spouse. Other factors were a history of psychiatric morbidity during pregnancy, the presence of chronic medical illness, and adverse pregnancy or neonatal outcomes. The community-based design and probability proportionate sampling employed were important study strengths. Key limitations included purposive selection of one district in Kerala and single-stage assessment using screening tools.Key Messages:
Postpartum depression (PPD) is an important maternal health concern and a significant public health issue. 1 Globally, PPD affects around 10%–20% of mothers with a disproportionately higher prevalence in low- and middle-income countries (LMICs) like India. 2 The pooled prevalence of PPD in India is 22% with considerable regional variations 3 ; the highest prevalence was found in the south (26%), followed by the east (23%), and the western region (21%); prevalence was lowest in north India (15%).4,5 Frequently identified risk factors include a personal or family history of psychiatric illness, antenatal anxiety or depression, obstetric complications,6–9 low social support, marital conflict, and stressful life events. 10
Maternal well-being is crucial, as it has a significant impact on the health of offspring and families. 5 Specifically, PPD may affect mother-child bonding and contribute to developmental delays in the child. 11 As an example, a large prospective cohort study found that PPD was a robust predictor of maternal indifference and alienation toward the child at one year after birth. 12 Early identification of PPD is essential for instituting appropriate pharmacological and psychosocial management and limiting its adverse impact. 13 However, stigma and limited knowledge often hinder the timely diagnosis and treatment of PPD. 14 Most Indian studies on PPD are hospital-based, limiting their generalizability to other settings. Community-based data in this group are scarce but nonetheless valuable for their better representativeness, ability to provide a more accurate picture of the true burden of PPD, and for eliciting information on context-specific risk factors, all of which may inform policy and program development.
Against this background, we conducted this community-based study to estimate the proportion of mothers experiencing PPD symptoms in a district within a state with high literacy and social development indices, namely Kerala, India. Specifically, our objectives were (a) to estimate the proportion of mothers with PPD symptoms in Malappuram, Kerala, and (b) to identify the correlates of depressive symptoms in this group. The Malappuram district of Kerala was chosen for the study due to its unique socio-demographic properties. With a population of 4.1 million, Malappuram is the most populous district in Kerala. 15 It exhibits the highest fertility rate in the state, with a crude birth rate (CBR) of 18.44 per 1,000 population, substantially exceeding the state average of 11.94. 16 Additionally, the district records the highest percentage of higher-order births (birth order three or above) (27.7%) compared to the state average of 16.6%. Furthermore, female literacy is nearly universal (99.2%), and the district has the highest number of out-migrants among all other districts in Kerala. 17
Methods
Ethical and Administrative Aspects
The pertinent institutional ethics committee approved the study. Subsequently, we obtained permission from the District Medical Officer (DMO) of Malappuram district and the corresponding medical officers of block panchayats to approach postpartum mothers in the respective wards. Informed consent was obtained from all study participants.
Study Design and Setting
Between August and December 2024, we conducted a cross-sectional study among postpartum mothers in the Malappuram district of Kerala. Spanning 3,554 square kilometers, Malappuram is the third-largest district in the state by area. It has a population of 4,112,920, a literacy rate of 93.57%, and a sex ratio of 1,098 females to 1,000 males. 15 The district is administratively divided into 94 gram panchayats and further subdivided into 1,778 wards; a ward contains an average of 367 households.
The district’s maternal and child health programs are run mainly by the National Health Mission. Two major programs are the Janani Suraksha Yojana (JSY) and Janani Shishu Suraksha Karyakram (JSSK). The former encourages institutional deliveries among economically and socially disadvantaged groups with financial incentives, while the latter provides free drugs, diagnostics, and transport to pregnant women and newborns. The district also launched “Amma Manassu” in 2017, a statewide integrated maternal mental health program that utilizes an online data entry platform to identify pregnant mothers and their babies, providing mental health screening during the antenatal and postnatal periods, along with information on nutrition and immunization. 18
Participants
Study participants were consenting mothers residing in the wards of four-gram panchayats (Wandoor, Chokkad, Melattur, and Angadippuram) in Malappuram district, Kerala, India, during the 6-week postpartum period. The 6-week cutoff for the postpartum period was based on the International Classification of Diseases-11 definitions of PPD. 19 We excluded mothers who were physically unfit for interviewing (e.g., deaf and dumb mothers or those who were physically weak and unable to sit through the interview).
Sampling Technique
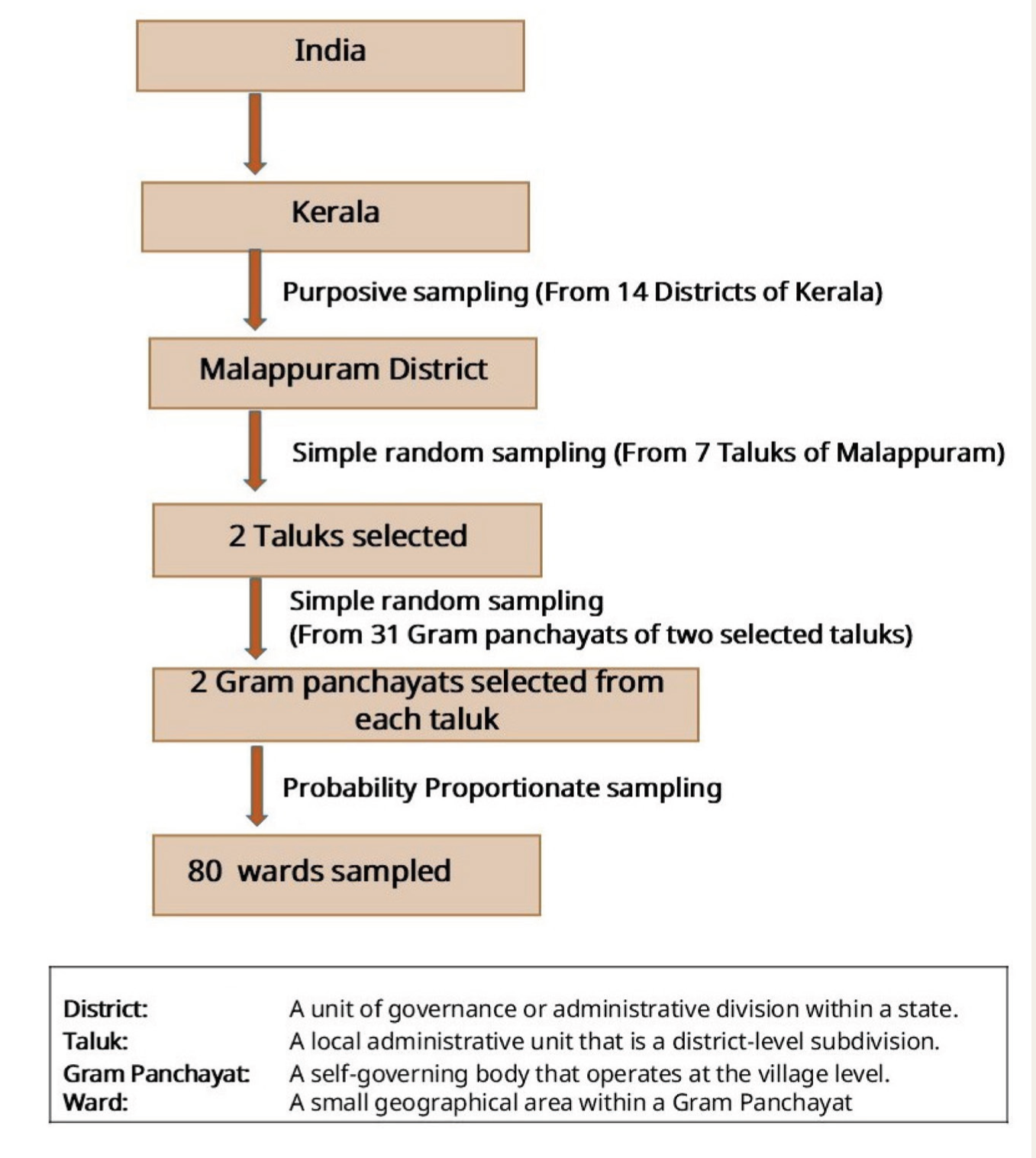
The study employed a multistage cluster sampling method to select participants, as shown in Figure 1. Malappuram district comprises seven taluks, fifteen blocks, 94 gram panchayats (A gram panchayat is a local self-governing body at the village level, established under Part IX of the Indian Constitution), 138 villages, and 1,778 wards. 20 Using simple random sampling, two taluks were selected as the sampling frame; one taluk comprised 16 gram panchayats, while the other had 15. Two gram panchayats were randomly selected from each taluk using the lottery method. Each gram panchayat in Malappuram, Kerala, has 16–23 wards, which served as sampling clusters. A total of 80 wards were available, and the sample was proportionally allocated to these clusters as enumeration blocks to achieve a final sample of 560 postpartum mothers (Figure 1). The total sample was assigned based on probability proportionate sampling: 161 mothers from Wandoor, 126 from Chokkad, 112 from Melattur, and 161 from Angadippuram gram panchayats.
From the selected wards, we gathered a database of postpartum mothers and their residence addresses, with the assistance of ASHA (Accredited Social Health Activists) and Anganwadi workers. ASHA workers are certified female community health workers in India who act as a bridge between the community and the public health system. In contrast, Anganwadi workers work for the Integrated Child Development Service (ICDS) program, targeting infants and mothers.
Sampling Method.
Assessments
We used a structured proforma to elicit relevant socio-demographic and clinical information. The Edinburgh Postnatal Depression Scale (EPDS) was used to screen for depressive symptoms in women within six weeks of delivery. 21 The EPDS consists of 10 questions assessing depressive symptoms experienced by postpartum mothers over the past seven days. Each question is scored on a scale of 0 to 3, resulting in a total score ranging from 0 to 30. Based on the criteria established by Cox et al., mothers with a total EPDS score of 13 or higher were classified as screen positive for PPD and coded as “1” (Yes), while those with a score below 13 were considered non-depressed and coded as “0” (No).
In compliance with the WHO translation protocol,22,23 the English version of the EPDS tool was translated into Malayalam by bilingual experts, followed by a back translation to ensure semantic, conceptual, and technical equivalence. We pre-tested the Malayalam version by administering it to 43 postpartum mothers to identify and refine inappropriate words or expressions. In our sample, the Cronbach’s alpha for the EPDS was 0.85, indicating good internal consistency.
Exposure Variables
Socio-demographic characteristics of postpartum mothers, their obstetric status, and physical and psychological health components were the exposure variables. These included age, living with husband (yes/no; noting that in many households in the district, husbands are working abroad), type of family (nuclear/joint), type of delivery (normal/Cesarean section), history of birth outcome (full-term/preterm/ abortion/miscarriage/stillbirth), sex of the baby (girl/boy), planned pregnancy (yes/no), regular postnatal check-up (yes/no), child NICU (Neonatal Intensive Care Unit) admission (yes/no), diagnosed with antepartum anxiety (yes/no), diagnosed with antepartum depression (yes/no), and chronic diseases such hypertension, diabetes, goiter, asthma etc. (yes/no).
Sample Size Estimation
The sample size was estimated using OpenEpi Software (version 3). We estimated the minimum sample size using the Leslie Kish formula. This yielded a sample size of 551, based on a 95% confidence level, 3% absolute precision, a design effect of 1.5, and a prevalence rate of 9.5% for postpartum depressive symptoms, as reported in a prior study. 24 Accordingly, the final sample size was 560 postpartum mothers.
Statistical Analysis and Software
Descriptive statistics (mean ± standard deviation [SD] or frequency [%]) were used to represent baseline sample characteristics. Independent samples t-test and chi-square tests were employed to examine the relationship between socio-demographic and clinical characteristics and the status of PPD symptoms (screen positive vs. negative). Subsequently, we conducted a multiple linear regression analysis to ascertain the association between depressive symptom scores (continuous outcome assessed using EPDS scores) and exposure (socio-demographic and clinical) variables. The selection of independent variables for multivariable analysis was based on theoretical and clinical understanding, rather than significance in univariable analysis; this is a recommended approach to reduce overfitting in regression. 25 We used the “robust method” in Stata, version 17 [StataCorp. (2021). Stata: Release 17. College Station, TX: StataCorp LLC] to address heteroscedasticity in the linear regression analysis. Statistical significance was set at p < .05. All statistical analyses were performed using Stata version 17. 26
Results
Participant Characteristics
We screened 592 mothers for eligibility and included 560 eligible, consenting mothers. The mean age of participants was 27.3 (±4.6) years, and their mean years of education were 13.3 (±1.8). As shown in Table 1, the majority of respondents (n = 369, 65.9%) resided with their husbands and came from nuclear households (n = 339, 60.5%). Most mothers had full-term deliveries (n = 505, 90.2%), with the majority undergoing normal vaginal deliveries (n = 427, 76.2%). A smaller number of infants required NICU admission (n = 93, 16.6%). Only a small proportion of mothers (n = 126, 22.5%) received regular postnatal check-ups, and a minority reported having chronic illness (n = 40, 7.2%).
Participant Characteristics (N = 560).
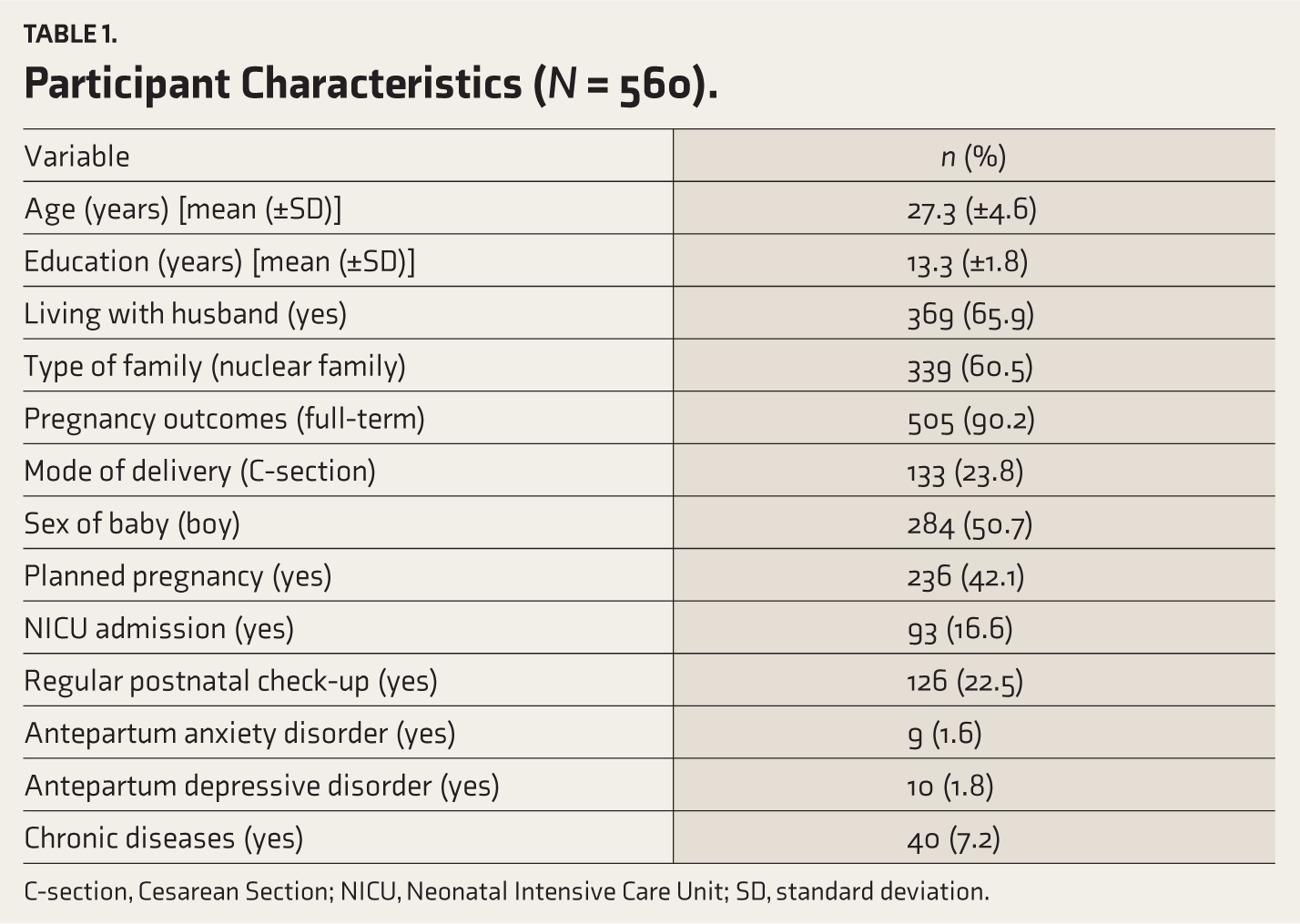
C-section, Cesarean Section; NICU, Neonatal Intensive Care Unit; SD, standard deviation.
Proportion of Mothers with PPD Symptoms and Their Correlates
The proportion of mothers with PPD symptoms was 11.3%; 63 out of 560 participants screened positive. The mean EPDS score was 4.7 (±5.1); the scores ranged from 0 to 24.
Between-group comparisons indicated that PPD symptoms were significantly more common among mothers with adverse pregnancy outcomes (preterm/abortion/miscarriage) (χ² = 4.67, p = .03); those whose children were admitted to the NICU (p < .001); ones who attended regular postnatal check-ups (p < .001); mothers diagnosed with anxiety and depression during pregnancy (p < .001); and those with chronic diseases (p < .001) (Table 2).
Comparison of Socio-demographic and Clinical Variables Between Groups (N = 560).

Values expressed as mean (±SD) or n (%); C-section, Cesarean section; NICU, neonatal intensive care unit; SD, standard deviation; *p < .05, **p < .01, ***p < .001.
Multivariable analysis (Table 3) indicated that not living with husband (p = .02), experiencing adverse pregnancy outcomes (p = .02) and normal delivery (p = .012), mothers with a girl child (p = .002), those who attended regular postnatal check-ups (p < .001), antepartum anxiety disorder (p = .015), antepartum depressive disorder (p < .001), and those with chronic diseases (p = .007) had a higher likelihood of PPD symptoms. The overall model fit the data significantly and explained 34.6% of the variance in PPD symptoms (R² = 0.346, p < .001).
Factors Associated with Postpartum Depressive Symptoms (N = 560).
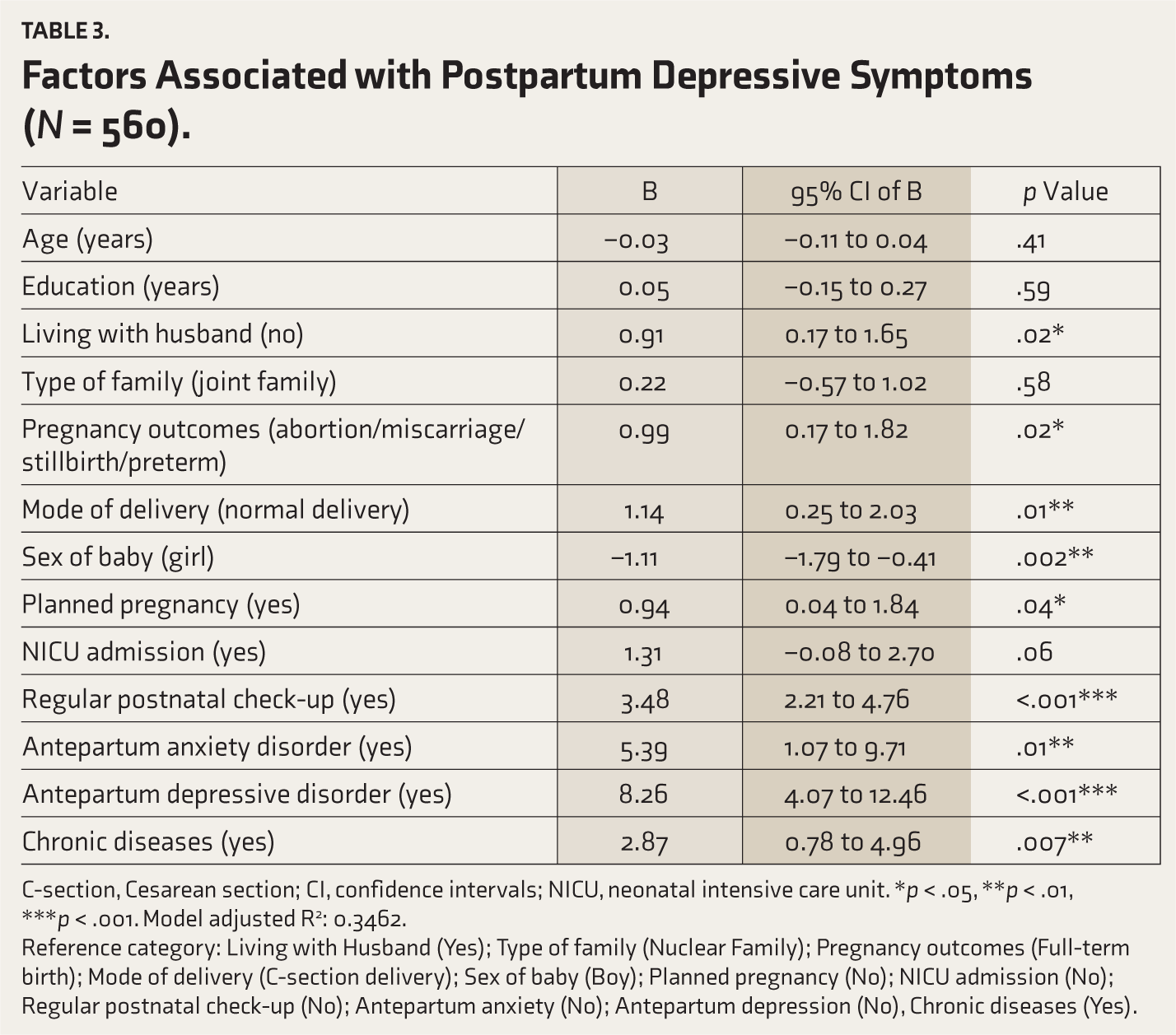
C-section, Cesarean section; CI, confidence intervals; NICU, neonatal intensive care unit. *p < .05, **p < .01, ***p < .001. Model adjusted R 2 : 0.3462.
Reference category: Living with Husband (Yes); Type of family (Nuclear Family); Pregnancy outcomes (Full-term birth); Mode of delivery (C-section delivery); Sex of baby (Boy); Planned pregnancy (No); NICU admission (No); Regular postnatal check-up (No); Antepartum anxiety (No); Antepartum depression (No), Chronic diseases (Yes).
Discussion
In this study, 11.3% of postpartum mothers exhibited symptoms of PPD. Key factors associated with PPD symptoms included not living with husband, experiencing adverse pregnancy outcomes (e.g., abortion, miscarriage, stillbirth), and attending regular postnatal check-ups. Medical and psychological factors, such as a history of antepartum depressive disorder, antepartum anxiety disorder, and chronic illnesses, were also significantly associated with higher depressive symptom scores.
The observed proportion of mothers at risk for PPD aligns with estimates from a prior six-nation study, which also assessed women with PPD symptoms. 27 However, it is lower than the pooled prevalence figures in a meta-analysis of PPD in LMICs, reported at 25.5%; the majority of the studies included in this review used a single-stage screening tool assessment for PPD, rendering the findings comparable. 28 Notably, these figures substantially exceed those reported from high-income countries such as Canada (5.6%) 29 and Denmark (3.2%). 30 These disparities may reflect differences in timing of assessment, social support and security systems, variability in measures used, and overall socioeconomic conditions. 5 For instance, an Ethiopian study found a near 50% prevalence of PPD, attributed to socioeconomic factors. 31
Notably, in India, prevalence estimates of PPD have varied considerably between community- and hospital-based studies. Two prospective observational studies at tertiary healthcare facilities noted a prevalence of 13.7% 32 and 31.4%, 33 while a 23% prevalence was found in a district hospital setting. 34 In contrast, community-based studies have shown lower rates: 11.4% in rural health training centers in Bangalore 35 and 12% in a prospective cohort study in Haryana. 36 Our figures were higher than the proportion of those with PPD symptoms in another community-based study from northern India. 24 This suggests regional differences in PPD symptom burden and merits further exploration.
Consistent with other studies,37–39 our study findings indicate that antepartum depression is significantly associated with PPD symptoms. Antepartum depression may be linked to PPD symptoms through common biological mechanisms (e.g., perturbations in neuroendocrine functioning) or by predisposing to adverse birth outcomes such as prolonged labor or premature birth. 40 The message is that clinicians should closely monitor and provide targeted interventions to women experiencing antepartum depression during both antenatal and postnatal periods.
Our findings also indicate a significant association between chronic maternal diseases and PPD. The combination of physical and psychological stress of pregnancy and stress of managing chronic health conditions may predispose one to the development of depression.41,42 We also found that mothers of infants admitted to NICU care were more likely to exhibit PPD symptoms, consistent with extant literature identifying NICU admission as a source of sustained maternal anxiety and stress.43,44 Prenatal anxiety disorder was another significant predictor of PPD, consistent with prior studies.45,46 Interestingly, higher PPD symptoms were found among mothers attending regular postnatal check-ups. This may indicate that such mothers are also more likely to experience complicated pregnancies or comorbidities such as eclampsia, puerperal infections, and cardiovascular infections, factors that have been associated with poor maternal mental health outcomes. 47
Our findings hold particular relevance for the Indian context, where significant progress has been made in reducing maternal mortality in the recent past. As maternal mortality declines, the focus needs to shift to maternal morbidity, particularly psychological health, which has traditionally been underemphasized. Notwithstanding the stated primary goal in the National Health Policy of strengthening the healthcare system, questions related to maternal mental health are overlooked mainly in national data collection exercises, such as the National Sample Survey (NSS) and the National Family Health Survey (NFHS). Our findings emphasize the importance of including items related to maternal mental health in these national surveys to better measure the burden of PPDs at the population level. This will be a low-burden but potentially impactful step in identifying and addressing this relevant public health issue.
These findings also highlight the need to integrate routine PPD screening into regular postnatal or vaccination visits at sub-centers, primary health centers, and community health centers. Given the shortage of the mental health workforce in India, task-sharing approaches offer a cost-effective and scalable solution. Programs such as ESSENCE (Enabling translation of Science to Service to Enhance Depression Care) and EMPOWER demonstrate the feasibility of training ASHA and Anganwadi workers to screen, counsel, and refer women using simple tools such as the EPDS, thus helping effectively bridge the maternal mental health treatment gap.48,49
For optimal benefits, PPD screening can be integrated into existing well-resourced programs like district maternal and child health initiatives instead of being a standalone new effort, which might be limited by funding and staffing shortages. Interdisciplinary collaboration between obstetric, pediatric, and mental health professionals is essential to enable a seamless transition from screening to treatment, thereby enhancing both patient outcomes and health system efficiency. 5 To ensure that early detection translates into meaningful improvements in maternal health and well-being, screening must be complemented by follow-up measures, including timely counseling and referral to specialized mental health services, when indicated.
Strengths and Limitations
Our findings must be interpreted in the context of their limitations. We employed a single-stage assessment using a screening tool. This implies that those who screened positive may or may not have been clinically depressed, and we are unable to comment on this possibility. The study was confined to one district in Kerala, characterized by a unique socio-demographic profile, and the findings may not necessarily generalize to other states or other districts in Kerala. Further, extensive population-based studies are required to enhance external validity. A major strength of this study is its community-based cross-sectional design, which contributes valuable data to fill the gap in Indian literature on PPD. Furthermore, we employed the probability proportionate sampling technique to select participants, thereby potentially reducing sampling error. Finally, we present both univariable and multivariable analyses to provide a more comprehensive understanding of the relationships between variables. Notably, the variable selection for the multivariable analysis was based on theoretical and clinical considerations rather than significance in the univariable analysis, as the latter approach has been found to have drawbacks, as explained earlier.
Conclusions
More than one in 10 postpartum mothers in the Malappuram district of Kerala exhibited symptoms of PPD. Key factors associated with PPD symptoms included not living with husband, adverse pregnancy outcomes, history of antepartum depressive or anxiety disorder, and chronic diseases. Given the considerable proportion of postpartum mothers at risk of depression and the shortage of mental health workforce, there is a need to incorporate PPD screening into routine postnatal care in a sustainable manner. Task-sharing approaches, which leverage the considerable pool of untrained community health workers, such as ASHA workers, offer a potentially sustainable and scalable solution in the Indian context.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Data Availability
Research data cannot be disseminated due to the inclusion of participant information.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
The study received approval from the Institutional Ethics Committee of the School of Public Health, SRM IST, Tamil Nadu, on May 16, 2024(IEC Ref no:00108/IEC/2024).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Not applicable.
Prior Presentations
No.
Simultaneous Submission to Another Journal or Resource
No.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.