
Abstract
A global economic crisis should not prevent aid towards developing countries, but it calls for wiser and more effective policies. This article proposes specific interventions with regard to drug donations, as well as a more general mentality which should govern related policies. It is generally acknowledged that donations in cash are preferable to donations in kind, but many problems persist either way, rendering obvious that some alternative approaches need to be adopted or enhanced. In the long run, independency from foreign interventions is significant for any developing country. Therefore, we recommend interventions which have the potential to sustain healthy economic development.
Keywords
Introduction
Inequalities between developed and developing countries are strongly correlated to continuing problems which the latter countries face, and which concern the income and its distribution, wealth, education, health level, and other factors. These problems have direct impact on many aspects with important social and economic extensions, such as poverty, lack of food and water, diseases, armed conflicts, natural disasters, mass immigration, lack of medicines and healthcare treatment, and so on. Countries of the developed world (let us call them “Western” countries) have been demonstrating increasingly good intentions to help with some of these problems. As a result, there are many development aid programs which aim to the radical reduction of the existing inequalities as well as their consequences. However, the compassion, the willingness, and the incentives of these efforts are ambiguous, while very few problems of the developing world have been effectively handled throughout the years. Specifically, former World Bank economist William Easterly estimates that the West has spent $2.3 trillion on foreign aid over the last five decades, but they still have not managed to get twelve-cent medicines to children to prevent half of all malaria deaths (Easterly, 2006, p. 4). At the very least, this observation calls for a new approach to dealing with problems of the developing world.
It is noteworthy that prosperity, welfare, and development are issues which have many dimensions and call for different approaches. Furthermore, development, which is one of the key determinants in order to achieve a prosperous situation, is not accurately reflected on the level and the growth of Gross Domestic Product (GDP). Obviously, the growth of GDP is a matter of great importance, however nowadays economists tend to a view that accepts a more general consideration about development. Thus, the use of Human Development Index (HDI) is a way to achieve a more comprehensive approach to the various phenomena. Specifically, the HDI focuses on measuring life expectancy, literacy education, and living standards worldwide. As a result, this index is able to categorize the level of development for several countries and to estimate the effectiveness and the impact of economic policies on the quality of life.
The brief reference to the HDI was made in order to indicate that life expectancy, and therefore the level of health is very significant throughout the development process. Therefore, given that the lack of access to essential medicines is a problem in the developing countries, the development aid includes drug donations. The lack of access to medicines is supposedly easy to be understood, as it is based on some particular causes. For example, one can claim that medicines are expensive, few governments can afford to provide them for free, and few people can afford to purchase them or even to participate in a cost-sharing procedure. As a result, it is obvious that some countries face a pressing problem concerning the available drugs, and drug donation is often considered as the easiest and most direct solution (APAC, 2001, p. 2).
The issue of access to medicines in developing countries is crucial, not only due to moral or humanitarian terms, but also in terms of development. Obviously, there are ways in order to improve the access and the opportunity of developing countries to consume medicines. Specifically, in the long term, the solution seems to lie in encouraging generic competition and in fostering local pharmaceutical companies; in this way, there is hope that these countries shall eventually be able to produce sufficient amounts of their own medicines, and cease to rely on Western aid. However, for the time being, Western drug donations constitute an essential intervention, which can bring very good results for needy people, under certain circumstances. On the other hand, drug donations have not always been particularly helpful, and it is certain that more carefully planned and properly monitored policies would have been more cost-effective and less prone to be manipulated. Although drug donations seem to be philanthropic, the effects of a wrong and inappropriate donation can be very dangerous, due to the specificities of drug donations, compared with other donated products (Doro, Mustafa, Eldalo, & Yousif, 2012). For example, a drug and medical supplies donation after the 1988 earthquake in Armenia was sent, which was about 5,000 tons with an estimated value of $55 million. Finally, 30 percent of these drugs were easily identified and 42 percent were helpful and relevant for this situation (Autier et al., 1990). Additionally, there are similar examples in other regions, such as Eritrea (Woldeyesus & Snell, 1994) and Sudan (Cohen, 1990), while the same problems can be also identified in the case of the World Health Organization field office in Zagreb in 1994; specifically, 15 percent of the drugs were unusable and about 30 percent were unneeded (WHO Department of Essential Drugs and Other Medicines, 1999).
This article aims at examining briefly the issues surrounding drug donations, before proposing a direction to which, at least in theory, future donations should be guided. A complete and coherent proposal cannot be constituted by any means, and many practical implications shall be left without being discussed. However, in the continuing effort to ameliorate drug donation policies, it is expected that some useful remarks and conclusions can be drawn here.
The Main Problems of Drug Donations
Before analyzing the main problems of drug donations, it is useful to mention the instances under which drugs are donated. First, drug donations can take place at a time of crisis, such as after a natural disaster, armed conflicts, or other emergency situations where needs for drugs are high; and second, donations can be part of development aid in non-emergency situations.
Drug donations in the first instance are difficult to be ideally organized; at the time of emergency, where time is of essence, facts are often unclear and many different parties are suddenly mobilized (such as foreign governments, religious facilities, nongovernmental organizations, the private sector, and even random volunteers), there are a lot of procedures which do not go as planned – sometimes a specific plan does not even exist. The desire to respond quickly overrides good practice, and experience shows that drug donations in these settings can create many problems, rather than solve any (Saunders, 1999). This led the WHO Department of Essential Drugs and Other Medicines to issue the Guidelines for Drug Donations in 1997 (revised in 1999), which stress the importance of effective communication between donor and recipient, and define the standards of quality which donated drugs have to comply with, especially when it comes to expiry dates (WHO Department of Essential Drugs and Other Medicines, 1999, p. 8). These guidelines are certainly helpful, but the fact remains that emergency situations can often render plans and policies ineffective.
Therefore, the second instance in which drugs are donated is what interests us mostly. In-kind drug donations as part of development aid are quite common, with many big pharmaceutical companies demonstrating a noteworthy commitment to be actively involved in such efforts. For example, Boehringer Ingelheim regularly donates neviparine to prevent HIV vertical transmission (Pérez-Casas, Herranz, & Ford, 2001). Also, under an agreement with the WHO in 2004, Novartis decided to donate $7 million worth of drugs to 500,000 patients with tuberculosis in poor countries, which has raised hopes that other drug companies will follow suit to fight HIV/AIDS and malaria (Fleck, 2004). Smaller scale corporate drug donations in developing countries have been ongoing for years, having thus created a high reliance on donors for resources to underpin health provision (Shretta, Walt, Brugha, & Snow, 2001). However, as in the case of emergency situations, not all drug donations can be described as really helpful. We do not fully agree with Gopal Dabade, the Indian health activist who claims that “drug donations don’t help people” (Dabade, 2004), but we have to admit that there are many problematic aspects which need to be carefully considered.
First of all, some common issues arise with regard to the quality and the proper use of donated drugs. Many of them arrive unsorted and labeled in a language which is not easily understood (Hogerzeil, Couper, & Gray, 1997), or they may come under trade names which are not registered for use in the recipient country. Also, donated drugs may have expired before they reach the recipient, or they may be drugs or free samples returned to pharmacies by patients or health professionals. Pinheiro (2008) notes that “drug donations provide benefits such as tax deductions and are a very convenient way for industries to get rid of stagnant stocks without having to pay for their controlled and expensive destruction in their country of origin.” In addition, a high declared value of donated drugs may indirectly affect the government pharmaceutical budget. There are also issues of import taxes and overheads for storage and distribution, which clearly show that drug donations are not for free; sometimes, their costs to the recipient countries surpass the very fair value of the donations (Pinheiro, 2008). Furthermore, the distribution plan of the donor agencies may conflict with the wishes of national authorities, thus resulting to mutual distrust and serious obstacles to well-intended initiatives. For example, in November 1996, Glaxo-Wellcome, Inc., announced the Malarone® Donation Programme, but this only began three years later, after much disagreement, dispute, and lack of communication (Shretta et al., 2001).
Another main problem which recipients have identified is the insufficient quantity of donated drugs for sustainable treatment (Gehler-Mariacher et al., 2007). This is a serious issue, especially in the case of HIV/AIDS therapy, which should be provided for life; if donated antiretroviral drugs fall short, many patients will have to interrupt their treatment. Such an interruption can easily result in the emergence of resistant strains of HIV (Stevens, Kaye, & Corrah, 2004), which should always be an important consideration. The same risk applies to incoherent treatment of malaria and tuberculosis, even though treatment for these diseases does not last for life. But apart from drug resistance, researchers point out that drug donations may have other adverse effects on therapeutic options: free products can deter or delay modification of national treatment guidelines to specify therapeutically better products, and can subtly undermine government motivation to weigh best therapeutic options independently. Moreover, free products can result in product familiarity, brand loyalty, and previous-use preferences by physicians and patients (Baker & Ombaka, 2009). This leads us to believe that some pharmaceutical companies donate drugs for public relations reasons, being more interested in maximizing profit than in providing efficient aid (Pérez-Casas et al., 2001). This is neither unlawful nor unethical for a private company; but it probably shows that a new framework is required for drug donations, one where the benefit of the recipients will become the absolute priority.
WHO experts recognize all the aforementioned problems and offer additional guidelines for drug donations as part of development aid. These mention that special care should be taken that the donated drugs respond to an expressed need, comply with the national drug policy, and are in accordance with national treatment guidelines in the recipient country. Also, donated drugs should be registered or authorized for use in the country through the same procedure that is used for government tenders (WHO Department of Essential Drugs and Other Medicines, 1999, p. 11). However, these guidelines do not constitute an international regulation. The fact that WHO officials recommend best practices does not mean that every party involved is willing to abide by them. This is clearly demonstrated by another very important point which they make, the one of transparency: “there must be due vigilance to ensure that donated products are not diverted for export, commercial sale, or into illicit channels” (WHO Department of Essential Drugs and Other Medicines, 1999, p. 13). This may be difficult in some areas of the developing – and indeed, the developed – world, where corruption is endemic and often out of control. Guidelines are certainly useful, and the response to the ineffective performance of drug donations can be related to the accurate implementation of given principles and guidelines. However, this is not enough; there are several difficulties in moving from theoretical approaches to implemented measures.
What Happens with Donations in Cash?
An in-kind transfer, such as drug donations, is either a transfer of ownership of a good or asset, other than cash, or the provision of a service, without any counterpart. On the other hand, cash transfer is defined as the payment of currency or transferable deposit by one unit to another, again without any counterpart (United Nations Statistical Division, International Monetary Fund, World Bank, Eurostat and OECD, 1993). In light of all these problems with in-kind drug donations, cash donations intended for local or regional purchase of essential drugs seem to be a more efficient solution. WHO experts note that “a cash contribution is very supportive to the activities of the local government or coordinating committee, it is supportive to the local and regional pharmaceutical industry, and it may also be more cost-effective.”
In addition, prescribers and patients are usually more familiar with locally produced drugs (WHO Department of Essential Drugs and Other Medicines, 1999, p. 11). A cash donation is also welcome in emergency situations, once the acute phase of the emergency ends, as it allows local or regional purchase of medical supplies (Khare, 1998). Therefore, provided that regional pharmaceutical companies have the ability to produce the required essential drugs or their generic counterparts, 1 foreign cash aid can be used to purchase them. The local drug industry is thus enhanced, motives are offered, and a more competitive market for priority drugs can be created; in the long term, this policy should eliminate the developing countries’ dependence on gifts. In addition, this strategy may enhance the economic perspectives in terms of employment, aggregate demand, and growth. This is based on the opinion that cash transfers have multiplier effects when recipients put their money to create additional income (Sadoulet, de Janvry, & Davis, 2001). Therefore, replacing drug donations with cash transfers may lead not only to the competitiveness of pharmaceutical industries but also to the general improvement of economic performance.
The claim that cash transfers are better and more effective than drug donations is also based on a solid theoretical basis. Specifically, there are microeconomic models which prove that a person can never be made better off with an in-kind transfer (such as drug donations) that is equal in cost to a cash transfer. However, there are instances that the person is indifferent between the two choices. As a result, the accepted view of economics is that cash transfers are more preferable than in-kind transfers (Thurow, 1974). In the case we investigate, economics seems to support cash transfers for drugs rather than drug donations. It is noteworthy that the microeconomic analysis concerning this issue is based on the concept of utility. Figure 1 depicts the above-mentioned claim, which implies that a transfer in kind is theoretically less valuable to the recipient than an equal cash transfer.
We will only briefly analyze Figure 1 because its wide analysis surpasses the objectives of this article. Specifically, the recipient’s budget line is AB, before any transfer. We are going to mention the consequences of both the different types of transfers. First, if we suppose that there is an in-kind transfer of Drug B, the recipient will be able to consume a larger quantity of Drug B (from B to D) and the new budget line is AFD. However, there is no increase in the quantity of Drug A that the recipient will be able to buy if he spends all his income on Drug A. Second, in case of a cash transfer, there are some specific differences, as the new budget constraint is HFD. The differences between the two transfers can be represented by the dotted portion HF. The options given along HF are feasible only in cases of cash transfers. As shown in Figure 1, a cash transfer is the optimum choice due to the higher level of utility that offers.
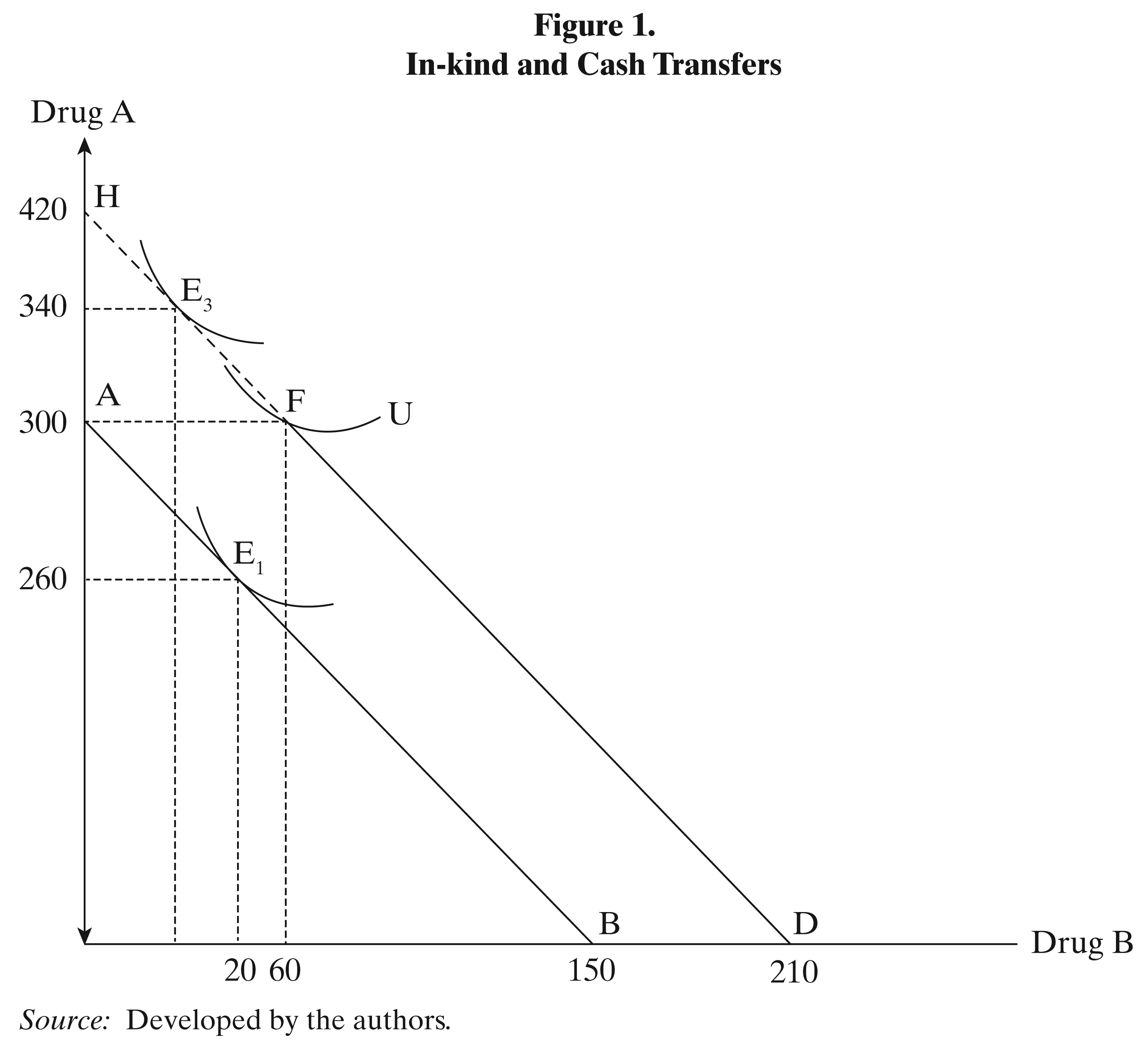
Despite the unavoidable assumptions and problems which this approach entails, it can be a useful indicator about the optimum policy. Otherwise, this approach can verify that from the standpoint of economic theory, cash transfers are more valuable to the recipient than in-kind transfers.
An example of cash transfer is the Global Fund to fight AIDS, Tuberculosis, and Malaria. Established in 2002, it can be described as a predictable, large-scale purchaser of medicines. Upon requests, it provides cash to local providers in order to buy what is necessary, thus offering substantial buying power and predictable guarantees of payment. Joined by other large initiatives, such as the President’s Emergency Plan for AIDS Relief, it has been responsible for pushing strong competition between different generic producers, while the security of sustained funding has motivated rapid entry by generic companies for the production of medicines for priority diseases (Baker & Ombaka, 2009). In addition, cash is regularly provided directly to developing countries by Western governments, NGOs, and religious organizations. Usually donors have no way of knowing what happens to the money once the intermediaries or the recipients get it. However, and especially at a time of global economic recess, one has to wonder whether these donations are handled in the most orthodox way.
It was mentioned earlier that many developing countries face a transparency problem. It is not unusual for some of the donated drugs to be sold illegally, and this problem has been repeatedly mentioned by representatives of the local public sector (Gehler-Mariacher et al., 2007). Also, money donated with the intention to buy medicines can be used for the purchase of other, completely irrelevant goods. For example, in 2005, the Global Fund Secretariat suspended its five grants to Uganda following reports of mismanagement, evidenced by inadequate monitoring and accounting of grand expenditures, and inappropriate, unexplained, or improperly documented expenses (Kapiriri & Martin, 2006), a practice which can probably take place in other countries as well, without being noticed. Furthermore, if donated money is indeed used to purchase regionally produced drugs, these may end up being sold at a much higher price on the “grey” market in other countries, even developed ones. 2 And even if transparency is not an issue (that is, not a direct one), bureaucracy certainly makes things worse. As William Easterly notes, “because of the insistence on working through governments, funds get lost in patronage-swollen national health bureaucracies” (Easterly, 2006, p. 229). Does this mean that a policy of decentralized handling of the donated money, which would by-pass many strict governmental procedures, could be much simpler and more cost-effective?
Proposals for Future Donations
The aforementioned indicate that there are several problems concerning drug donations, as well as their consequences. However, this constitutes a widespread practice; the developed donate pharmaceutical products or cash to purchase them to developing or underdeveloped countries. At first sight this is a good practice which includes humanitarian aspects, but several problems concerning the intentions and the targets of donors have been identified. A recent review concludes that it is hard to evaluate the implementation of the WHO Guidelines issued in 1999, and that a reform of drug donations policy is still needed (van Dijk, Dinant, & Jacobs, 2011). As a result, it is important to examine the effectiveness of drug donations, to search for alternatives and to conclude to the preferable option. We have already explained that cash donations have important advantages, which can be used in order to enhance the effectiveness of both drug donations and development aid. By this we do not imply that drug donations have to be abolished, nor we believe that this is feasible. Besides, there are some very successful in-kind donations programs, such as the donation of Mectizan® for onchocerciasis control (Hopkins, 2012). However, these interventions seem to function better in localized settings. For example, with reference to the abovementioned Mectizan® and onchocerciasis, in Nigeria there are Onchocerciasis State Coordinators, who supervise personally the implementation of the program and, in collaboration with researchers, monitor adverse reactions and estimate acceptability and compliance (Otubanjo et al., 2008). And, as Easterly notes, “once the West is willing to aid individuals rather than governments, some conundrums that tie foreign aid up in knots are resolved” (Easterly, 2006, p. 322). In what follows, we shall stress on the importance of community-directed approaches and their advantages compared to centrally controlled procedures. The benefits of a localized, community-based approach can be better understood if they are considered in four broad categories, as given in the following.
Better Distribution
Developing countries have many peculiar needs, which are not easily understood by distant policy makers, and therefore, the problems, arising from these needs cannot be faced effectively. Moreover, problems may differ substantially from one developing country to another or from one area of a developing country to another. The various differences between countries and the arising problems lead to the conclusion that central management often causes Western donations to be used in a way which does not produce as much benefit as it could. If the distribution plan is designed by local agents, who are perfectly aware of the needs and the possibilities of each area, then no unnecessary efforts and unfeasible plans are made, while a lot of disagreement and delays can be avoided. Localized control of cash donations means that doctors get exactly what they ask for (provided that it can be purchased), and not simply what is sent to them. Also, this gives them the opportunity to design treatments in a more efficient way, as they can choose the drugs or the technology with which they can work better. For instance, the DOTS system of strict surveillance, which mainly deals with tuberculosis, allows for better control over specific therapeutic procedures, since it directly observes the participants, preventing them from stopping treatment or abusing the system. The increased cost-effectiveness of this intervention is beyond dispute. But in order for DOTS to be implemented, localized handling of resources is essential (Lienhardt et al., 2012).
According to the WHO guidelines (WHO Department of Essential Drugs and Other Medicines, 1999), the establishment of a coordinating body in the recipient country is important, as it can act as a mean between relief organizations and government departments. We believe that, on a local level, the coordinating body can handle the donations all by itself, without any governmental central intervention. This will reduce some of the delays, such as those derived from bureaucracy causes or from difficulties between the competent bodies. However, the structure, the responsibilities, and the operation of such a coordinating body are multidimensional matters. For example, the coordinating body could be an independent organization, a local representative, or a group of experts from various sectors; however, its accurate structure is still in question. The different needs, the specificities of each country, as well as the institutional and organizational framework may lead to different approaches concerning the role and the structure of a coordinating body.
More Transparency
Another important aspect which should be examined is that the whole donation procedure is very often plagued with transparency problems. Generally, it seems that a lot of aid money is not used in a proper way. It makes sense for a pharmaceutical company to seek ways to make a profit, but it is unacceptable for international agencies and government officials. Still, the aid, in most cases, is not given without motive on the part of the donor countries or agencies. Exploitation by international agencies is implicit in their aid giving activities. The people at the helm of affairs get a big share of the aid money (Begum, 2001). This claim summarizes some malpractices which take place during the aid procedure, while it creates a fundamental question about the optimum management of donated resources. Can the problem be solved by adopting a localized distribution with no central management? Some might say that this is not much of a change; it does not matter if “people at the helm of affairs” are more with fewer corresponding resources to handle. However, we think that this is an incorrect approach due to some specific causes. First, a local management implies that there will be a decentralization of the activities about development aid and drug donations. The international literature verifies that a decentralized system can be less corrupted (Fisman & Gatti, 2002), therefore a local management of the aid can lead to a more transparent and effective system. Second, a central management is very powerful, as the central managers handle plenty of resources. On the other hand, in case of local managements, the resources are not managed only by few central managers, but by a plenty of local. As a result, the power in local management is limited, especially when it is compared with that of central management. Another feature of local management, which is a direct consequence of the aforementioned power, is that there are not many “chances for corruption,” while the supervision and the evaluation of the whole activity are much more intense. Thus, the emphasis to local economic development and the increasing responsibilities of a community-based management can lead to a more transparent and cost-effective situation.
With reference to the management of corruption incidents, and provided that public health has to come above else and that it is the main objective of aid and donations, we do not think that the solution against misbehavior lies simply in cutting funds, as the Global Fund did to Uganda (Kapiriri & Martin, 2006). There has to be a different kind of solution, with prevention of such phenomena being the weapon of choice – this means that the supervision of the whole procedure has to be consistent and continuous. The emphasis on a community-based approach and the importance of supervision are those matters that need to be examined in a new framework.
Future Independence from Western Interventions and from Black Market Policies
As it has already been implied, we think that independency from foreign interventions is significant for the developing country. One of the main problems with development aid donations in general is that they tend to create dependencies (Moss, Pettersson, & van de Walle, 2006). However, if a donation is considered only as a starting point and is handled in an efficient way, it can certainly help to eliminate the need for future interventions. Implicitly, long-term donations are expected to last until they are no longer needed. If an equivalent product can be purchased in the recipient country, donated drugs can reduce the local production or sale of this product (Bero, Carson, Moller, & Hill, 2010). Therefore, the ideal solution seems to lie in an in-kind donation at first, followed by donations in cash. If donated cash is used to foster the local pharmaceutical sector, it will be expected that an increasing potential will occur, and the needs of the local community will be satisfied. The most feasible solution seems to lie in the local production of generic drugs, and the subsequent purchase of these drugs by local hospitals using donated cash. It goes without saying that international regulations should be respected, otherwise a “national black market” may emerge, such as the one India has created by circumventing international patent law and copying medicines that have been patented elsewhere (Grzybowski, 2004). Apart from rendering Western gifts unnecessary in the long term, local generic competition can also bring drug prices down. In addition, the implementation of compulsory licensing to imports and the local production of generic drugs can guarantee a sustainable way to get cheaper drugs (Pérez-Casas et al., 2001). Therefore, a focus on local generic competition and the subsequent price reduction will have a direct positive effect on the problem of unregulated black market drugs.
Respect for Local Views on Just Allocation
There are core differences between donors and recipients with regard to the optimum allocation of donated resources, and this is an important reason why the Western countries are not able to offer an effective plan. This opinion is based on the fact that there are different wishes, needs, and targets between them. Moreover, the fundamental differences of the institutional and organizational framework lead to differences in implemented policies, even though the strategy is similar in both cases. Therefore, it is important to establish a process that respects local views. According to their experience with regard to rationing of donated antiretroviral treatment, Nguyen et al. (2003) observe a dynamic community response resulting in synergies with the public health care system, and conclude that new models of community-driven health care advocacy and private–public synergies will, if given adequate financial support, help to change the culture of public health and increase health equity in developing countries (Nguyen et al., 2003). In brief, local communities have to be actively involved in the decision-making and the rationing process of donated drugs (or drugs which are purchased locally with donated cash) even though their ideas of fair distribution may occasionally conflict with Western firmly established principles of justice. Western good intentions do not account for much if they fail to respect different worldviews.
Conclusion
In this article, we have argued that future drug donations to developing countries must be organized in a more community-oriented manner. We have also stressed the importance of enhancing donations in cash, as they seem to produce greater benefits for the recipient countries. These rather general remarks were supported with various examples, opinion papers by distinguished professionals, and with economic theory. However, it has to be admitted that no specific solutions were proposed; this is partly due to the assumption that each problem has to be addressed as unique, with a solution which must be discovered at a local level, by local people, and with the discreet help from foreign experts only when it is necessary. Western countries should offer guidance and, most importantly, funds to developing countries, but they should also provide them with the opportunity to handle their issues on their own. As Easterly notes, “it is easier to search for solutions to your own problems than to those of others” (Easterly, 2006, p. 303).
To be sure, the problems identified at the beginning of this article cannot be eliminated all at once. Mistakes are made, guidelines are not always fully implemented, corruption shall not cease to exist, and many procedures do not go as planned. This has to be accepted. Shortcomings should not be viewed as a waste of time, effort, and money, but as part of the continuing developing process.