
Abstract
Although a body of research suggests that interprofessional collaboration is hindered by the presence of professional boundaries, more recent work has demonstrated that removing these boundaries also has negative consequences for collaboration. To address these paradoxical findings, we examine two different team-level initiatives that aimed at softening and breaking down professional boundaries, drawing on data gathered from 78 in-depth interviews and two years of observations of four cross-occupational teams in the English National Health Service. Our inductive analysis of this data shows that professionals use boundaries and their manifestations – which become apparent through materialization, articulation and embodiment – to identify and retrieve professional categories. The conspicuous presence of boundaries allows professionals to anticipate other team members’ expertise and roles, as well as different aspects of team tasks. We theorize our findings by showing how professional boundaries can be positively interlaced with interprofessional collaboration by making visible and grounding naturalized systems of classification.
Introduction
Under contemporary conditions of multidisciplinary collaboration, government agents and managers understand professional boundaries as counterproductive to effective work. Therefore, there have been increasing efforts across different sectors to re-delineate or even break down professional boundaries to foster interprofessional collaboration (Bucher, Chreim, Langley, & Reay, 2016; Denis, Lamothe, Langley, & Valette, 1999). The general consensus is that professional boundaries are barriers that hinder integration among professional groups, as professionals strategically use boundaries to control and protect their own turf (Abbott, 1988). This seems to be increasingly relevant in the case of professional bureaucracies, created around the principles of ‘pigeonholes’ and professional autonomy (Mintzberg, 1979; Scott, Ruef, Mendel, & Caronna, 2000), where boundaries are considered dysfunctional entities that should be loosened if integration across professions is to be achieved (Heracleous, 2004).
The examination of the relationship between professional boundaries and interoccupational interaction has been a key aspect of the research on professions (Heracleous, 2004; Lamont & Molnár, 2002; Langley et al., 2019), yet the literature shows conflicting messages as to the consequences of boundaries for collaboration. On the one hand, most studies conceptualize boundaries as conditions for separation and exclusion between occupational groups, treating them as zones of jurisdictional conflict among professions (Abbott, 1988; Gieryn, 1983). This work focuses on the constraining role of boundaries for interprofessional collaboration and explores different ways of overcoming or spanning them (Bucher et al., 2016; DiBenigno & Kellogg, 2014).
On the other hand, recent studies of the configurational boundary literature show some paradoxical findings (Langley et al., 2019): blurring or breaking down professional boundaries seems to have mixed or even negative consequences for collaboration and coordination (Wolbers, Boersma, & Groenewegen, 2018). A close analysis of some of these studies reveals that in the absence or blurring of professional boundaries, substitutes must be devised if interprofessional collaboration is to be achieved (Cartel, Boxenbaum, & Aggeri, 2019; Majchrzak, More, & Faraj, 2012; Valentine & Edmondson, 2015). This paradox prompts the following research question: How do professional boundaries influence interprofessional collaboration?
To address this question, we studied cross-occupational teams in the English National Health Service (NHS). Health care systems are a fitting context to examine boundary-breaking initiatives given that they are constituted by numerous professions organized around well-demarcated professional boundaries. In addition, government-led reforms have targeted health care structures and practices with the aim of re-delineating, softening and/or breaking down professional boundaries to increase integration and efficacy in health care delivery. In this paper, we focus on two such government-led initiatives: one that aimed at softening professional boundaries in a traditional hospital setting, and another that aimed, more radically, at breaking down professional boundaries in a novel and hybrid health organization.
Our findings reveal that professional boundaries can be positively interlaced with interprofessional collaboration through the process of categorization, which is the identification and use of existing categories to anticipate, segment and act upon the world professionals confront. Professionals use boundaries and their manifestations – which become apparent through three mechanisms: materialization, articulation and embodiment – to identify and retrieve professional categories that help forestall other team members’ expertise and roles, understand different aspects of team tasks, and collectively anticipate and coordinate paths of action or decision at the team level. Furthermore, to make sense of the various influences of boundaries we identified in the cases, we analytically distinguished the influence of boundaries on the use of categories for ‘thinking’ and ‘acting’ (Ellen, 2006; Mintzberg, 1979). Our findings call into question the guiding principles of many recent public sector reforms – namely, that dismantling professional boundaries is an effective way of achieving interprofessional collaboration (Martin, Currie, & Finn, 2009). Our results suggest a more nuanced re-conceptualization of professional boundaries as potentially enabling interfaces for interprofessional collaboration. Boundaries enable collaboration to the extent that they provide the social ontologies (Schatzki, 2001) to anticipate and represent professionals’ own and others’ expertise and roles, as well as the nature of problems and interventions, by grounding professional classificatory schemes.
Theoretical Background
The concept of boundaries is a central element in discussions about the creation and maintenance of professions and the interaction across them, as it is essential for understanding how professions institutionalize differences between one another (Lamont & Molnár, 2002). Boundaries as ‘sites of differences’ (Abbott, 1995) help produce and sustain distinctions between ‘us’ and ‘them’, what is legitimate or illegitimate, or acceptable and unacceptable (Heracleous, 2004, p. 95).
The notion of the professional boundary, and its related concept of border, is multi-dimensional (Heracleous, 2004). As socially constructed, boundaries have both a material and a symbolic dimension. The material aspect makes the boundary ‘visible’, regulating interactions and allowing the development of further symbolic elaborations (Hernes, 2004). In turn, the symbolic aspect, as argued by Lamont and Molnár (2002), facilitates the development of conceptual and interpretative distinctions common to members of an occupation. Hernes (2004, p. 13) expands on this analysis by incorporating the actual processes that the boundary circumscribes: ordering (regulation of internal interactions), distinction (or the demarcation between the external and internal spheres) and threshold (the regulation of interaction and flows between the external and internal spheres).
These generative conceptualizations are nevertheless not central in most of the literature on professional boundaries, which instead focuses on how boundaries take on a restrictive and contesting character (Langley et al., 2019). Accordingly, a profession needs to ‘construct’ a boundary around itself so as to distinguish it from competing occupational groups, and to protect itself from external interference (Abbott, 1988). Critically, this conceptualization rests on the assumption that professions inhabit competitive ecologies, in which professions compete against each other for symbolic as well as material resources (Abbott, 1988).
Consequently, the problem of boundaries and their demarcation becomes inextricably associated with the study of professions and interprofessional dynamics. Demarcation is considered part of the ideological and strategic attempts to secure and legitimize professional boundaries. Gieryn originally coined the term ‘boundary-work’ to designate the discursive practices used by scientists to draw a ‘rhetorical boundary between science and some less authoritative, residual non-science’ (Gieryn, 1983, p. 781). Following this line of research, other authors have also explored different actions that professions implement to socially construct, maintain or reinforce boundaries (e.g. Martin et al., 2009) in order to avoid encroachments (Abbott, 1988) and to limit the number of entrants (Manley, 1995). Conceptualizations of professional boundaries as interfaces of conflict, contestation and seclusion are nevertheless beset with paradoxical tensions, as interprofessional connection, collaboration and coordination do occur in daily interactions in the workplace (Langley et al., 2019). In fact, many of these studies frequently describe different forms of overcoming or rearranging boundaries to facilitate interprofessional collaboration across them.
Overcoming boundaries for collaboration
Studies on professional boundaries and boundary-work tend to emphasize the problematic, contested and obdurate nature of boundaries, and their negative impact on interprofessional dynamics. In parallel, many studies have also detailed multiple forms collaboration across boundaries (e.g. Anteby, Chan, & DiBenigno, 2016; Bucher et al., 2016; Huq, Reay, & Chreim, 2017). Such apparent tension is solved by retaining the conceptualization of professional boundaries, and their constraining role for collaboration across occupational groups, and moving into identifying mechanisms (such as settlements, brokerage roles and practices, boundary-objects, or even boundary-subjects) that enable collaboration and ameliorate boundary contestation (Anteby et al., 2016; Bechky, 2006; Kellogg, Orlikowski, & Yates, 2006). For instance, it is argued that conflict around jurisdictional boundaries can be resolved by different types of settlement that in turn comprise various forms of collaboration and coordination work (Abbott, 1988; MacDonald, 1995).
As many studies focus on collaboration across boundaries, they often describe the means that make such cooperation possible, while showing that such collaboration is not in itself free of tensions. These tensions can be negotiated (Apesoa-Varano, 2013; Kellogg et al., 2006) or pasted over by individuals able to bridge the differences (Fleming & Waguespack, 2007), or by objects that allow for the appropriation and adaptation of differences across boundaries (Bechky, 2003; Star & Griesemer, 1989).
Conversely, a group of studies has recently begun to question the assumption of the problematic nature of boundaries, arguing that tensions can simply be downplayed or displaced to favour interprofessional collaboration (Meier, 2015; Pouthier, 2017; Quick & Feldman, 2014). For example Meier (2015), in his comparative analysis of two hospital wards, observes how the pressure of time, resources and bed capacity ‘dissolves’ the contested nature of boundaries, facilitating daily collaboration. In this line, Pouthier’s (2017) study of a cross-occupational team for palliative care and oncology patients shows how existing boundaries can be leveraged by griping and joking to make roles, responsibilities and mutual expectations salient. Finally, in their conceptual paper, Quick and Feldman (2014) go further, arguing that boundaries can be seen as ‘junctions’, where things can be joined, rather than as separations to be worked around.
Rearranging boundaries for collaboration
Mirroring the scholarly understanding of professional boundaries as hindering interfaces for interprofessional collaboration, many organizational and policymaking initiatives have aimed to reshape or even dismantle boundaries with the expectation that greater integration and collaboration could be achieved (Gassman & Enkel, 2004). In the private sector, a wave of changes aims at breaking down professional or functional boundaries by means of creating project teams or cross-functional teams composed of members from newly created ‘tribes’ or ‘chapters’, or by means of temporal or free spaces (Majchrzak et al., 2012). In the public sector, a related body of research has focused on how boundaries are externally rearranged so as to influence dynamics and practices across professions (Bucher & Langley, 2016). These attempts to achieve integration through boundary redefinition have been comprehensive and spanned multiple levels, from novel governance and work structures (Bucher & Langley, 2016) to health policy discourses that promote the crisscross of sectoral boundaries to improve population health (Hayes & Dunn, 1998).
A closer analysis on this stream of research, which has been labelled configurational boundary literature (Langley et al., 2019) for its interest in studying the reshaping of boundary landscape to orient patterns of competition/collaboration, shows some paradoxical findings. As boundaries are purposively blurred or rearranged to enable collaboration and coordination, interprofessional interaction ironically needs to find substitutes for boundaries to make them happen (Cartel et al., 2019; Majchrzak et al., 2012; Valentine & Edmondson, 2015). For example, Majchrzak and colleagues (2012), in their study of multifunctional teams that have to perform novel tasks, show how teams needs to develop frameworks or ‘scaffolds’ that guide their work and sustain collaboration. Only when scaffolding is established can professional boundaries be ‘transcended’. Similarly, Valentine and Edmondson’s (2015) study of a hospital emergency department redesign shows how the development of team scaffolds allows temporary or fluid groups (where roles and boundaries are ill-defined) to build effective coordination at the team level. Finally, Cartel and colleagues (2019) show how the creation of a temporary and experimental space facilitated innovative exploration among field actors in the future carbon market. This collaboration, the authors argue, was made possible by a simulation that structured and coordinated the interactions of and preassigned roles to the different actors in a space that otherwise did not have the pre-existing boundaries.
In sum, many of the studies that have explored the implementation of boundary rearranging initiatives in professional institutionalized settings depict mixed results (Bucher et al., 2016; Croft et al., 2015), and those that have studied more radical forms of boundary-breaking ironically show the need to develop instead temporal structures and scaffolds that support interaction and order coordination between professionals (Majchrzak et al., 2012; Valentine & Edmondson, 2015). In light of these tensions and paradoxes, and given the growing effort in different sectors to realign pre-existing professional boundaries, it is worth asking not only if breaking down professional boundaries can affect collaboration, but ultimately if professional boundaries may positively influence interprofessional collaboration and coordination. Recognizing these tensions and studying the differentiated consequences are central for developing a deeper understanding of the influential character of boundaries in interprofessional work.
Methodology
Research setting
To explore the rearranging of professional boundaries and the consequences on interprofessional collaboration, we position our empirical work in the context of the NHS. A markedly professionalized organization, the NHS is an ideal setting as it comprises multiple well-demarcated spaces of interprofessional interactions. Recently, different government-led initiatives have attempted to redefine traditional professional boundaries with the aspiration to promote closer interprofessional collaboration and integration within the NHS (Farchi & Salge, 2017).
Professional boundary redefinitions have become widespread across different sectors (Langley et al., 2019), and the NHS, in particular, offers a wide variety of empirical experiences. Using the NHS as a study setting, we explore the consequences of two types of boundary rearranging initiatives at the intraorganizational level. The first initiative aims at softening professional boundaries between doctors, nurses and managers in hospitals, by creating joint governing structures responsible for the provision of patient care (within a specialty or group of specialties). The second initiative involves more radical forms of boundary-breaking, specifically, the creation of cross-occupational teams composed of professional hybrids (individuals with professional backgrounds who have moved into managerial, service improvement or policy roles (see Noordegraaf, 2007) in quangos responsible for improving quality and efficiency across the NHS, but removed from daily health care delivery.
Case selection and overview
We chose a range of ‘similar and contrasting’ cases (Eisenhardt, 1989) to gain a deeper understanding of the consequences of rearranging and breaking down boundaries on interprofessional collaboration. To this end, we adopted a criterion sampling strategy to explore the diverse configuration of boundaries and gain insight into their consequences. Table 1 summarizes the four selected cases. The two teams inhabiting established professional conditions and performing more operational and institutionally demarcated tasks (hereafter established teams) are referred to in this article as AcuGroup and MedGroup. They are both clinical directorate boards (management units formed around either a medical specialist or a support service who are tasked with managing both clinical services and their administrative and financial aspects) within one of the largest NHS teaching hospital in the United Kingdom. The two teams inhabiting more hybrid conditions and performing more novel and hybrid tasks (hereafter hybrid teams) are referred to as CommGroup and SaferGroup. These groups are part of an NHS quango. This organization was created in the early 2000s by the English Department of Health (DH) with the goal of supporting the NHS to transform ‘healthcare for patients and the public by rapidly developing and spreading new ways of working, new technology and world class leadership’ (internal document, 2009).
Description of Groups for Case Studies.
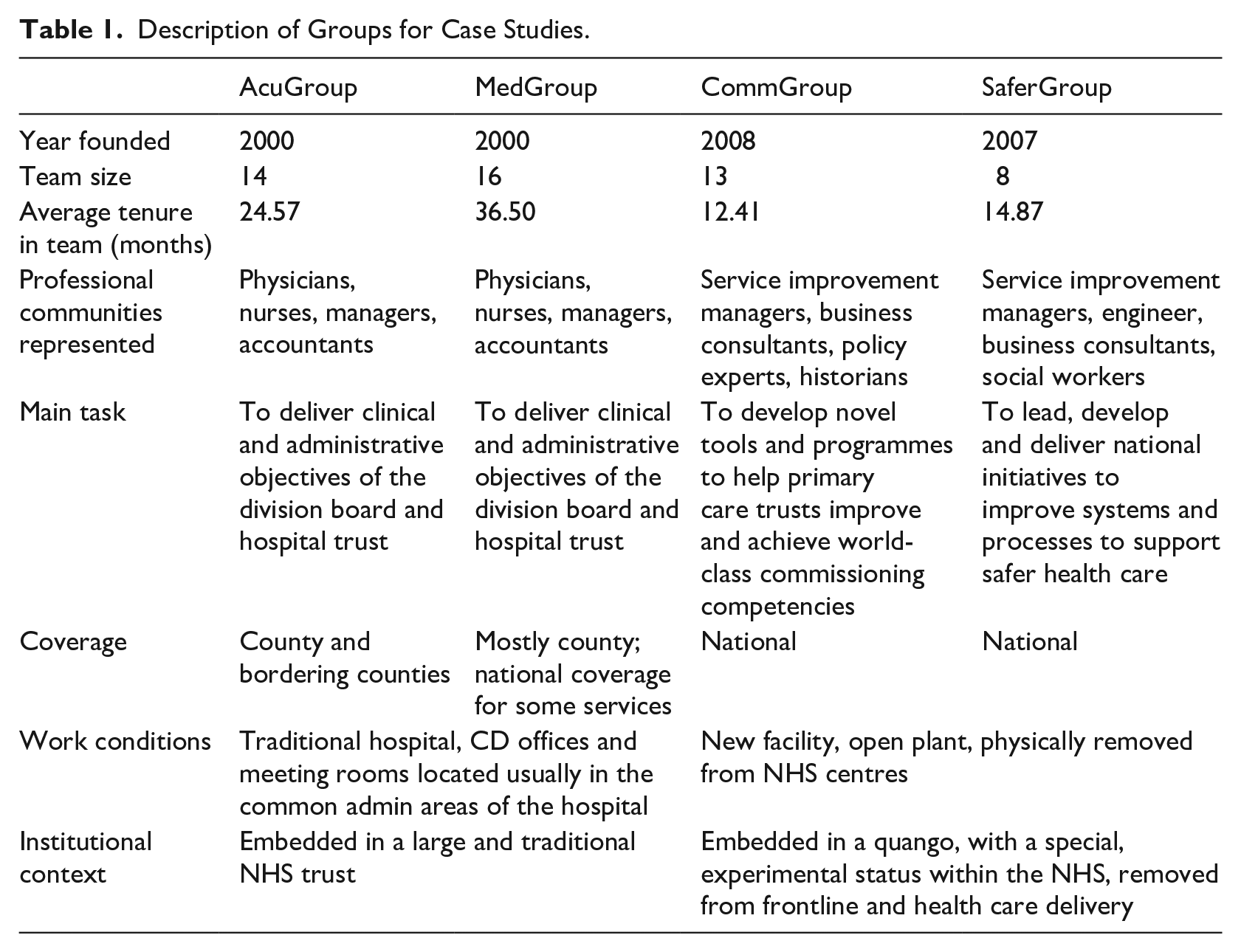
We now provide a brief description of each group, as well as its structure, main goals and boundary characteristics.
Established teams
MedGroup’s and AcuGroup’s primary task is to manage the quality and cost of clinical services delivered by their constitutive clinical units. They oversee and seek to improve existing clinical services and processes, meeting the needs of patients but also those of the hospital and its various professional groups. MedGroup is a clinical directorate board and has final responsibility – clinical and financial – for the provision of a large variety of very specialized clinical services – e.g. diabetes, immunology, endocrinology, among others. In turn, AcuGroup is the board of one of the largest clinical groups of departments in the trust hospital, and it is composed of three large and highly connected clinical units related to emergency care.
MedGroup and AcuGroup are both heterogeneous groups of managers and medical professionals with diverse clinical backgrounds. Each board includes one lead clinician and one manager (or nurse) from every medical department it oversees, chosen by the departments themselves. In addition to these appointed members, each board is led by a clinical director, who is supported by a CD manager, a finance officer and a nurse manager. Consequently, the softening of professional boundaries has occurred not so much in the content of the task, professional affiliation of their members, or in the institutional context in which it is performed, but in the shared responsibility of different professional groups for the overall management and governance of health care delivery (as opposed to the traditional medic-centred approach).
Hybrid teams
CommGroup’s and SaferGroup’s primary task is to develop new tools and programmes that benefit the NHS. Their work includes ideation, testing, development and, occasionally, delivery. CommGroup ultimate aim is to support primary care trusts (PCTs) (organizations within the NHS in charge of providing primary and community services, and commissioning secondary care from other providers) in achieving the world-class commissioning competencies promoted by the DH. Some examples of their projects include PCT Board Development, a tool that helps PCT Boards consider how they operate as corporate entities and enhance their effectiveness, and the Improving Patients’ Pathway, a series of tools that help promote improvements in care pathways.
SaferGroup emerged as a direct response by the quango to a DH report – ‘Safety First’ – (Carruthers & Philip, 2006). SaferGroup was set up specifically to respond to the safe care challenges outlined in the report. Since its inception, the team has created a series of different tools to provide education and training, develop senior NHS leaders to build organizational competences in this area, and help practitioners in primary care improve safety in areas such as hospital-acquired infections, reduction of medical errors, detecting patient safety incidents, etc.
As a result, the breakdown of professional boundaries occurs on multiple levels. First, the innovative tasks performed by the hybrid teams require developing new knowledge or a departure from existing skills. Second, teams are composed of members with hybrid professional affiliations and/or with non-conventional trajectories in the NHS. Finally, the working conditions and the institutional context of the quango are far removed in its material and symbolic aspects from the traditional institutions that constitute the NHS, which makes the breakdown of traditional professional boundaries all the more evident.
Data collection and analysis
As we started our fieldwork, we paid particular attention to interprofessional collaboration, and how this collaboration was enacted through the coordination, distribution and integration of tasks in the different teams. This approach is well-suited to understanding how demarcation occurs and how jurisdiction and professional boundaries are enacted (Bechky, 2003). Yet, we soon noticed that members of the hybrid teams frequently referred to the difficulty of ‘pigeonholing’ due to the fuzzy characteristics of demarcation and professional boundaries in their teams and in the quango, and the negative impact of this on interprofessional collaboration. Due to the relevance of this construct for the research participants, who understood ‘pigeonholing’ similarly to how the literature refers to the practice of categorization (see Alaimo & Kallinikos, 2021), we took it as a sensitizing concept (Given, 2008). Conducting our research across the four cases in parallel gave us the unique opportunity to explore whether this construct was also relevant for CDs members in hospitals. Iterating across sites and teams further sensitized us not only of the critical role of ‘pigeonholing’ across the four teams, but also its close association with boundaries and interprofessional collaboration.
We gathered data from a number of sources – including field interviews, observations and archival sources. We relied on 78 semi-structured interviews with team members as one of our primary data sources. All interviews were fully recorded and transcribed. In addition to interviews, we conducted non-participative observations of group meetings and other forms of formal and informal social gatherings for an average period of six months in each group. We observed 40 meetings in total (approximately 101 hours). Finally, we supplemented our primary data sources with archival data, collecting both proprietary and public documents that allowed us to contextualize and triangulate the findings.
We used an interpretive approach to analyse the data (Golden-Biddle & Locke, 2007; Reay, Zafar, Monteiro, & Glaser, 2019). Following multiple stages of inductive examination, we analysed the characteristics of professional boundaries and their influence on diverse instances of interprofessional collaboration. We began with a provisional list of codes composed of concepts and themes drawn from the research question and from the literature reviewed. We completed this list with a set of recurrent concepts and themes from the four cases. Based on the final list, we developed a coding protocol in the form of a set of structured codes. Furthermore, we relied upon the ‘insider/outsider’ coding method (Bartunek & Louis, 1996). One author, who had collected the data and had been immersed in the field for two years, initially coded the data following the coding protocol. In parallel, the ‘outsider’ authors, who had not been in the field, used the same coding protocol to analyse the data, looking for salient thematic patterns and consistency in the coding process. Fortnightly meetings between the ‘insider’ and the ‘outsider’ authors throughout this initial period helped to increase consistency in the coding process, and further added reliability to the overall analysis. Because professional boundaries are fundamentally a socially constructed phenomenon, we paid particular attention to the discourse articulated by the members of each group, which could expose common interpretation and meaning systems. To account for this emergent semantic consistency, we analytically focused on isotopies – i.e. recurrences of similar elements of meaning (Greimas & Courtés, 1982) – within and across teams.
In coding the data, we focused on descriptions provided by interviewees on different manifestations of professional boundaries, process of categorization and interprofessional collaboration in their teams. First, we coded the different ways in which team members perceived objects, people, practices, languages and spaces as belonging to other professional communities. For instance, members of established teams recognized multiple objects (e.g. stethoscopes, inverted watches, wards, etc.) or behaviours (e.g. professional affiliation becoming visible by specific utterances) as markers, and described how they use these boundary markers to anticipate their interactions. In hybrid teams, members referred instead to the instability of markers, and the difficulties to identify objects, people, practices and languages as pertaining to specific professional groups. Eventually, this led us to categorize the different forms of boundary manifestation into three mechanisms: materialization, articulation and embodiment. Second, we focused on interviewees’ expressions and language associated with pigeonholing, and how the perceived characteristics of boundaries influence such process of categorization. In further analysis of the data, we realized that for professionals ‘pigeonholing’ was a broad category that encompassed elements associated with different types of categories-in-use associated with expectations and with enactment that were found to be consequential and yet distinctive for interprofessional collaboration; and we coded them as categories for thinking and categories for acting (Ellen, 2006; Bechky, 2006; Mintzberg, 1979). Categories for thinking are the templates that allows professionals to represent and anticipate objects, concepts and relations. We hence coded team members’ references to acts or processes of representing or diagnosing team problems or tasks into this aggregated coding category. Conversely, categories for acting refers to the templates of actions and decisions that allow professionals to retrieve collectively predefined behavioral responses, defined here as the act of applying or executing standard programmes. Consequently, references to paths of action and decision were included in this coding category. Finally, we paid attention to observations and statements referring to different aspects of collaboration across professional boundaries, such as task allocation, coordination and anticipation of other team members’ expertise and role.
Findings
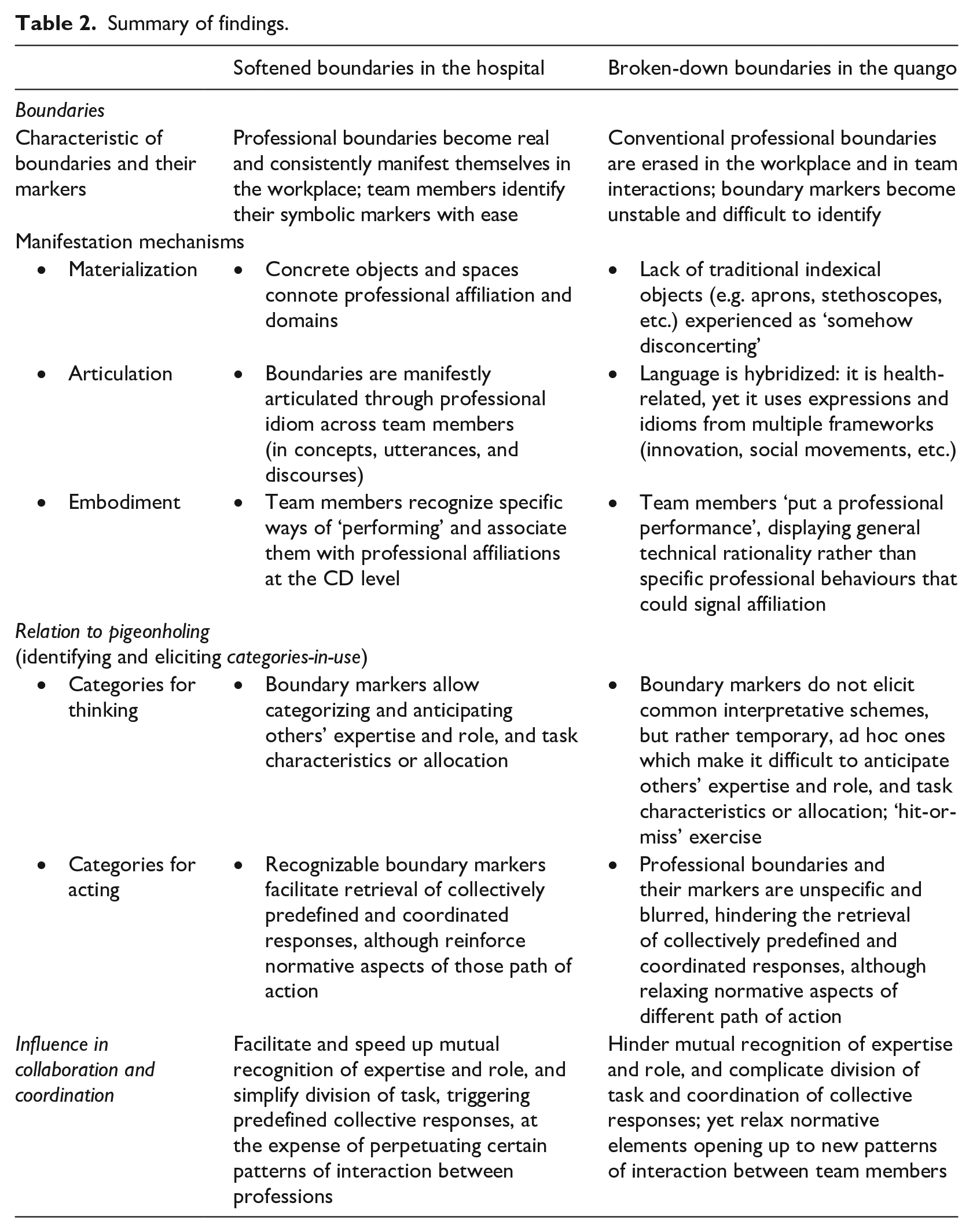
We now present participants’ narratives, vignettes and our field data and observations that show how different arrangements of boundaries influence the identification and use of professional categories (pigeonholing), ultimately affecting collaboration and coordination. We first present the findings from the two teams in hospital settings where professional boundaries have been softened but still remain clear. Second, we present the contrasting results from the teams in the quango, where professional boundaries have been purposefully erased. For each case of boundary configuration, softened or broken down, we begin by describing how professional boundaries manifest to team members through materialization, articulation and embodiment. We then show how each specific configurations of boundaries, and their manifestations, differentially influence the identification and use of categories for thinking (associated with how team members anticipate others’ expertise and roles, and the nature of task) and categories for acting (associated with the identification of predefined courses of action). Table 2 below shows a summary of these contrasting findings.
Summary of findings.
Softening of boundaries in established professional conditions
CDs in English trust hospitals sought to soften professional boundaries through shared governance structures and cross-professional teams. The guiding assumption was that such interventions could increase collaboration and coordination between professions. We found, however, that many boundaries persisted at the CD board level and became real and manifest in the workplace through three core mechanisms: materialization, articulation and embodiment. Additionally, and perhaps surprisingly, as our analysis uncovered, in this complex large teaching hospital, professional boundaries were actively used by team members to anticipate and increase mutual awareness of each other’s tasks, roles and expertise.
Materialization
Interestingly, both MedGroup and AcuGroup’s meeting rooms are removed from the clinical and governance areas of the hospital, and yet professional boundaries still materialize and become apparent at meetings through concrete material objects. Attire such as aprons, badges, stethoscopes, hanging inverted watches and two-piece suits serve as professional boundary markers. Team members frequently referred to these markers and their connotations as influencing interactions. Outside the meeting rooms, the architecture, including wards, hallways, signage and even technical equipment are recognized indicators of professional boundaries.
Articulation
Boundaries also became manifest via languages and utterances. Professional idiom used by team members and in the different documents not only conveyed meanings, but also references or traces that connect it with the professional community of origin as they are interwoven with professional practices and shared systems of reference.
I think it just depends on the background of the individual. So, for instance, in specialist medicine we’ve got some Clinical Unit Managers who come from a nursing background and equally those that don’t come from a nursing background, and so their understanding and language is different, you know, so I think that’s an issue. I think between specialties among doctors, there’s no problem with language, we talk very much a similar language. Directorate Managers who come from a non-medical background, again it’s interesting, they have a huge learning curve because we’ll be talking in terms which they’re not familiar with. They come and sit in clinics, they speak to the medical staff, and so they become familiar with the medical issues within the patch even though they don’t even know the language. (physician, Directorate Chair, MedGroup)
Team members easily identify the language used in the documents and by their colleagues as belonging to some of the professional communities represented on the CD even if they do not fully understand it. As linguistic differences became evident in meetings, so did requests for clarification when others’ language became too technical or opaque. After one meeting, when we observed that one manager openly asked for an explanation of a problem in non-medical terms, he later explained that these interventions are common in CDs: Well that’s my get out of jail, if you like, because I sort of say well hang on, I haven’t got a clinical background so could you just explain that to me in John-speak? That’s my way of getting around things, to say actually I don’t understand when you’re talking in big clinical words, tell me what that means in English. But I think people should be allowed and that’s, if you like, part of the role that we have, to be able to challenge. (administrator, AcuGroup)
Embodiment
Boundaries become also visible through embodiment, referring to the identification of members of different professional groups (nurses, medical doctors, managers, etc.) through how they ‘perform’ at work. Patterns of action and interaction, although subtle, were identifiable in the behaviours of CD members. From the white coat and bedside manners of doctors, to the suits and blunter ways of discussing of managers, the repetition of identifiable performances makes evident professional affiliation and simultaneously influence interactions: I think you can tell quickly who is who on the CD, not only by their identification badges and uniforms. Doctors tend to be more reflective and listen to different opinions, but they like to have the last word in the discussions. Nurses tend to focus on the concrete, they tend to come to meetings with lots of specific topics, and are usually more conciliatory. Managers tend to be more vocal on issues. I can even tell by the way they sit in the chairs, I don’t know . . .little things. Doctors tend to lean back in their seats, and nurses tend to sit on the edge of the chair. I don’t know, it’s funny. (nurse, MedGroup)
Consequences on categories for thinking
Materialization, articulation and embodiment enable the perceptual recognition of boundaries and work as markers, so helping team members to identify those signs as representing something (or somebody) that stands for something else. As professional boundaries become visible and identifiable, they then elicit and influence ‘pigeonholing’ as a subtle yet pervasive practice. For example, an AcuGroup nurse explained how she can quickly identify the professional affiliation of an unknown colleague through ties. Ties are primarily worn by both medical doctors and managers, however while managers wear ties in the normal fashion, doctors usually tuck the ends of their ties under their shirts, customarily between the third and the fourth button, to avoid contact with patients and possible transmission of hospital-acquired infections. The head of AcuGroup discussed the subtleties of these boundary markers, highlighting the difficulties an outsider would experience in grasping their meanings: Like I do, I know instinctively, and you might get it wrong but you know instinctively if. . . [you are] coming from outside it’s like a nightmare because the influential doctors won’t tell you they’re influential. But that’s the same everywhere, that’s like going into a foreign country and trying to talk to a big company, how do you know who is in charge. And they all smile sweetly and the person in charge you can’t even see, and the person you see isn’t in charge. Very, very important with lots of badges but isn’t in charge. (physician, CD Chair, AcuGroup)
Such recognizable professional boundaries facilitate pigeonholing. As one AcuGroup’s emergentologists put it, quickly identifying a person’s professional affiliation allows one to anticipate the associated type of expertise: One can anticipate basic knowledge and skills of each professional group or specialty. There are other things that a person may know, but they are not relevant to our work or are not part of the profession. I, for example, have been studying mathematics at the Open University for four years now, but nobody knows that, and I don’t think it’s relevant.
Similarly, articulation and embodiment of institutionalized boundaries allows recognition of other team members’ role, understood as socially constructed positions and performances in a given situation. In one meeting, the clinical governance manager raised a case within a surgical cancer ward where a patient had a myocardial infarction undetected for 15 hours. After the details of the case were presented and analysed at length, the group agreed it should be assessed as a serious incident (SI). While many group members (with clinical background) could have led the investigation, the group quickly agreed the task should lie within nursing. This quick anticipation of roles within the team facilitated continuity of behaviours and practices over time as team members generally understand that nurses have more detailed knowledge of patients’ circumstances because their work demands more time spent with patients so even doctors defer to those insights. The manager said: ‘You prefer blue rather than white coats for this. Everybody tends to have their own role. (. . .) It’s really quite clear’ (clerk, AcuGroup).
The ostensive nature of professional boundaries also influences the criteria determining the tasks to be performed. In particular, task allocation and interprofessional coordination was referred to as quick and straightforward because the rules from professional demarcations are adhered to by team members. Task allocation within the CD boards followed what some interviewees referred to as a ‘departmental allocation’ – namely, each task or work stream was assigned to a particular professional group, reflecting a shared understanding about assignment distribution. Novel or complex tasks were usually divided into smaller subtasks by either the CD manager or the Chair, and distributed to team members reflecting their affiliations with occupational groups and departments: Some of them are quite straightforward. If it’s related to emergency medicine it’s coming to me, if it’s related to acute medicine then it will go to Doctor (. . .). So if it’s actually very clear that it belongs to a particular department, then that’s it. If it’s affecting two departments mainly, then it will be a case of those tasks will be divided between the two relevant. (physician, AcuGroup)
A clear isotopy emerges when analysing how team members defined those aspects of collaboration related to task coordination and allocation. Members perceived tasks as falling ‘naturally’ within their expected responsibilities, reflected in the following categories for thinking: ‘Ongoing/odd’ tasks (administrator, AcuGroup) ‘Logically compartmentalized/non-logically compartmentalized’ tasks (physician, AcuGroup) ‘Obvious’ tasks (nurse, MedGroup) ‘Single/multiple department[s]’ tasks (physician, AcuGroup) ‘Departmental/generic’ tasks (financial analyst, AcuGroup) ‘Operational/strategic’ tasks (manager, MedGroup) ‘Territorial’ tasks (physician, AcuGroup)
This demarcation, ultimately drawn around occupational boundaries, enhanced the visibility of tasks and responsibilities among team members. Furthermore, team members anticipate division of work even in cases of a novel or ill-defined task. They do this on the basis of recognizable criteria of what responsibility, and area of work, each professional group has. In this case, pigeonholing meant dividing ill-defined or novel tasks into recognizable and agreed-upon sub-tasks.
Consequences on categories for acting
So well-defined professional boundaries were associated with the representation of other team members’ expertise and roles, and influencing task division. Yet their effects on categories for ‘acting’ were paradoxical. On one hand, the ostensive nature of boundaries in established professional conditions facilitates retrieval of collectively predefined and coordinated responses. Clinical professionals described this integration across boundaries as straightforward. One example was the case of cardiac arrest teams within AcuGroup. AcuGroup presided over and coordinated all the cardiac arrest teams. These teams were summoned to all situations where a patient or individual within hospital facilities was not breathing, and were composed of anaesthetists, cardiologists and nurses who were on call but dispersed around the hospital. Usually, there was no communication or contact among team members prior to attending a cardiopulmonary arrest; however, within a few minutes, they were expected to arrive, make a diagnosis, coordinate tasks and perform the resuscitation procedure. This required fast-paced coordination of complex tasks among team members with different professional backgrounds, including basic life support, the selection and dosage of the first drug administered, and the use of defibrillation. Such a fast and complex coordination was only made possible by existing shared interpretative schemes on the distribution of roles, expertise and responsibilities that were fully recognized, respected and followed by team members and triggered by boundary markers.
On the other hand, the communal nature of professional boundaries reinforces the normative and binding character of professional categories. CD members were aware that actions and decisions come with normative demands toward their own respective communities, and professional boundaries reinforce such awareness.
I represent the opinion of the doctors in the CD, as my colleagues do of their respective groups. In particular, many doctors are. . . don’t want to be or are not anyway on the management Boards. So if I want to get something done I’ve got to go and talk to a lot of other doctors to get them to agree to something, and that’s all done informally.
What happens if you don’t take into account their opinions?
It won’t happen.
How can they influence decisions if they’re not in the formal structure?
If you make a decision then you’re a bit like on the Titanic, it won’t happen. The doctors simply won’t do it, then. . . what do you do? They will think of a reason why it doesn’t apply to them and you can’t effect change. Some things you can do without doctors but anything that needs doctors to support, it won’t happen unless you get their support. There are lines you should not cross and you won’t get their support because the Director of managers says it works.
This was particularly evident when conflict existed between the proposed paths of action among team members. In such situations, not only did professional boundaries become apparent within the groups but also it was clear that higher-status professionals tended to ensure that their actions or decisions prevail.
Radically breaking down boundaries in hybrid professional conditions
We’re all fish out of water (. . .). We have all had to reset our measures of what’s around us and who’s around us and what their knowledge base is. (O2)
The quango was designed as a space removed from traditional NHS boundaries to allow for freer exploration of new ideas that can improve clinical services. Based on a new location, away from NHS and DH traditional decision centres, the quango sought to attract a broad range of professionals not only from the NHS but also from other sectors to develop novel approaches. Such distancing from traditional NHS practices and configurations, however, made boundary markers unstable and difficult to identify, as group members could not consistently associate them with any conventional professional boundary. This challenge was evident in the three mechanisms earlier identified.
Materialization
It is important to note that both teams were working in ‘open plan’ offices, with uniform office equipment and hot-desking practices. As team members experienced interactional workspaces protean, they equally noticed that the lack of traditional and highly indexical objects (such as badges, stethoscopes, etc.) and a rather similar way of dressing across team members (business casual) made it difficult to infer any kind of stable and recognizable materiality of any professional boundary. For many team members, the material fluidity and the limited spatial boundaries of the quango felt ‘strange’, ‘different’ and ‘somehow disconcerting’ given weak association with professional markers when compared with traditional NHS spaces.
Articulation
Multiple languages coexisted in the quango, yet were difficult to trace back to any specific professional community. In meetings, not only the language of the reports, documents and minutes, but also that used by the team members demonstrated that although most topics were health-related, they were framed using concepts borrowed from project and change management, consultancy and innovation. So, language was hybridized.
I think the fact that we don’t have [or] we don’t use a common language is a barrier. I think [it’s] because we’re describing things in a different way, the same thing in a different way. And sometimes it’s hard to know where some things come from. (Mk1)
Embodiment
Team members recognized that they put on a ‘professional’ performance, but struggled to connect such a performance with any professional affiliation, background or expertise. Putting on a professional performance, as observed during team meetings, was primarily associated with drawing heavily on and displaying technical rationality. Continuously referring to conceptual or analytical models, reminding one another of different elements of the DH white papers that originated some of projects, or asking to be stricter with the few quango processes were the most evident. Beyond these generic behaviours, as many team members recognized, there were few clues to derive any professional affiliation from the way colleagues embody their professional work.
So it’s, it’s professional backgrounds but with a small ‘P’; a kind of clinical as opposed to managerial. But that doesn’t stop us confusing each other, I promise you. (P4)
The quote above not only illustrates the self-perception of team members of their rather undetermined professional status but also that the lack of identifiable professional behaviours exacerbates ambivalence and confusion. In sum, fuzzy professional boundaries, and their corresponding boundary markers, complicated the emergence of collective symbolic representations, the consequences of which we will analyse below.
Consequences on categories for thinking
In the quango, boundary markers do not elicit common interpretative schemes, but rather temporary, ad hoc ones. The difficulty of pigeonholing professionals and situations is here a common trope. Professionals with past experience in the NHS found established interpretative schemes acquired in more traditional settings misplaced for the purpose of deriving or anticipating other’s expertise. Member O1 described the randomness of the local interpretative process: We gather bits around that, there isn’t any formal process for making people clearly aware of what working experience people have got and you just pick it up via conversations. But that’s a very hit-or-miss process, so you don’t [know]; I’m not personally aware of, you know, the vast majority of backgrounds of people in the team. (O1)
Given unstable boundary markers, team members struggle to retrieve established categories of role, and instead develop ill-defined expectations and reporting relationships about their own and others’ roles. The fuzzy nature of articulation and embodiment make it difficult for team members to anticipate others’ roles, so role attribution becomes a ‘hit-or-miss’ exercise, highly provisional and changeable. This situation is most evident to those with experience on the NHS front line.
I think in the wider NHS, if you are working in a clinical role your roles find you. So you have got to, if you say that you are a doctor or a nurse then people immediately pigeonhole you into a particular [role], and you are known as that and that is very much a part of your identity. I find that much less here [in the quango], it seems to be less relevant, less clear. (S2)
Finally, the uninstructive nature of professional boundaries at the quango does not facilitate team members to understand and generalize the task structure and subsequent allocation. Members of both teams (CommGroup and SaferGroup) unanimously perceived intragroup task coordination and allocation processes as random and undetermined. When individuals joined these teams, they were usually assigned to a general project. On top of this initial assignment, incoming daily tasks were assigned by the program heads according to fluctuating and occasionally unclear criteria (prior experience with similar projects, specific skill sets, or availability). Nine out of thirteen CommGroup members describe task allocation as ‘random’, ‘not formal’ or ‘not logical or straightforward’.
Lacking clear demarcation, complex or novel tasks are difficult to categorize into known systems. For example, meetings where CommGroup members analysed the future ‘Measuring for Improvement’ programme involved lengthy discussions about the different frameworks that should be used. We observed that initially team members quickly agreed that the goal was to improve commissioners’ understanding of measurement and methodology approaches, and connect them ‘to the science of improvement’. But then, the determination of the specifics of the programme took many meetings. Given various metrics and methodologies, and the lack of a hierarchy among them, team members unsuccessfully sought to devise a framework to organize them all. Finally, and with frustration, the team followed an additive criterion, including diverse and not necessarily aligned elements coming from management (balanced scorecard, performance management), project management (run charts), clinical governance (quality care) and statistics (statistical process control). Furthermore, the difficulty to anticipate professional ascription across team members made identification and matching of work aspects problematic, with members having to rely on multiple changing criteria to coordinate tasks.
And I think it’s also that life isn’t straightforward and logical, and things come in and you think well we need to be involved in this but it’s not obvious where it should go, so I’m going to send it to here because I have to send it to someone, but, you know, it could equally have gone to someone else and we’ll sort it out as we go. (head of the programme).
These situations generated ‘confusion’, a recurrent isotopy in the quango.
So (. . .) we end up with something that’s a little less formal and as a consequence has a danger of creating confusion both in their minds and also in the minds of other members of the organization looking at the team and saying, ‘who’s dealing with what’. (service improvement manager, CommGroup) [Task allocation is] a bit random, (. . .) sometimes it feels a bit arbitrary and we are left wondering why, and sometimes it does not happen in a clear-cut way, (service improvement manager & nurse, CommGroup)
Consequences on categories for acting
As professional boundaries are unspecific and blurred, quango group members were less limited by normative demands of the professional categories of their original occupational communities. The loosening of the normative grip on categories for acting was perceived by team members as positive, especially for enhancing broad team collaboration, with the perception that everyone is on an equal footing. For example, in the successive meetings to launch the ‘Triple Aim’ programme, an initiative looking at large-scale change to strengthen the commissioning of health services, we observed team members brainstorming quite freely. Regardless of whether or not they had a clinical or NHS professional background, CommGroup members tabled different implementation options, some of which could have come into conflict with their professional communities of origin. This was the more surprising as the programme was beset by a number of tensions as it aimed at improving the patient experience of health care, improving the health of the population, and securing value for money all at the same time. Yet, because of the lack of hierarchy and status among the proposed paths of actions or decisions, collaboration between professionals here involved longer processes of ‘unearthing’, ‘gathering’, ‘making sense’ and ‘negotiating’ between the different team members. The head of one of the teams suggested that having multiple non-hierarchical possible paths of action across team members not only made the process of collaboration lengthier but also less clear: They say here [that] is our ultimate goal that you need to be heading towards, but in terms of how you get there and the impact you have, well we don’t really know. And it becomes much more down to the individual perception of key people around the system, who may or may not agree with each other, and there’s often not a clear hierarchy in terms of whose opinion is more important than someone else’s. (P2, head of the programme)
Discussion and Conclusions
Our study sought to understand how professional boundaries influence interprofessional collaboration – and, specifically, whether they can enable it. We found that boundaries play a key role in enabling collaboration through a process of categorization. Professionals use boundaries and their manifestations – which we labelled boundary markers – to identify and retrieve professional categories that help anticipate other team members’ expertise and roles, as well as different aspects of team tasks. Consequently, our study expands the present conceptualization of boundaries as zones of action and conflict (Abbott, 1988; Gieryn, 1983; Manley, 1995) by elaborating on the enabling and perceptual role professional boundaries can have in delineating professional categories that then go on to influence levels of team collaboration.
In particular, we add to existing literature and theory by exploring how boundaries manifest in the workplace through three core mechanisms: materialization, articulation and embodiment, and also tracing how these mechanisms help identify and retrieve naturalized systems of professional classification. We also delve into the differentiated influences of professional boundaries on the use of categories for thinking and acting, and the implications for the existing literature on the reconfigurations of boundaries (Langley et al., 2019) and on the properties of formal organizations more broadly (Du Gay & Vikkelsø, 2016).
Boundaries ground professional categorization
One of the central ideas in the debates on professional boundaries is that they are barriers to collaboration (Allen, 2000). Consequently, boundaries need to be bridged (Bechky, 2003; Carlile, 2004), downplayed (Kellogg, 2014; Pouthier, 2017), or broken down (Bucher & Langley, 2016) in order to allow interprofessional collaboration. Instead, and distinct from this existing literature, a key finding of this study is that boundaries can provide cues for professionals’ expert judgement, such as the use of concrete boundary markers for rapidly anticipating the expertise and role of others. Accordingly, boundaries do have an enabling role, as they are inextricably related to the practice of pigeonholing (Mintzberg, 1979; Scott et al., 2000) that, as a form of categorization, is here understood as the symbolic and spatio-temporal segmentation of objects, speeches, people and tasks based on existing professional categories and schemes that serve as standards of knowledge and templates for actions (Bowker & Star, 1999). Hence, in line with more generative conceptualizations (Hernes, 2004; Quick & Feldman, 2014), we understand boundaries as socially constructed distinctions (Lamont & Molnár, 2002) that help professionals make the ambiguity and discontinuities of the world amenable to expert intervention.
In fact, professionals actively use such distinctions – as they materialize in boundary markers – to retrieve and assess the appropriateness of existing professional categories, indicating productive links between the literature on boundaries and that on the micro-foundations of categorization (Coslor, Crawford, & Leyshon, 2020). More specifically, as our study shows, professional boundaries become evident for team members through three mechanisms: materialization, articulation and embodiment. Boundaries materialize in concrete objects that symbolize professional affiliations, membership and spaces. They not only convey differential status between professionals, as traditional and recent work on symbolic objects in professional contexts argues (Siebert, 2020), but also ground the use of professional categories in each specific situation. Also, boundaries are manifestly articulated in professional languages (concepts, utterances and discourses). Again, while the use of language in relation to borders has been studied as a way of expressing normative and ideological aspects of the competitive dynamics of the professions (Finn, 2008), or as a response to jurisdictional challenges (Gieryn, 1983), we found that at the team level, the use of categories is elicited by speech acts, discourse, or other features of professional communities’ different languages. Finally, boundaries are embodied in concrete professionals, who not only hold identities but also show these professional identities by putting on specific performances (Hodgson, 2005). The stability of these embodied markers helps team members discern the subtle differences between professional displays.
Theorizing around these empirical observations, we suggest that boundaries and their markers are not only interlaced with the practice of categorization but also, and more substantially, ground it in three distinctive ways. First, professional categories are embedded in the material and symbolic spaces delimited by professional boundaries, and consequently the associated process of pigeonholing is built into boundary markers (such as objects, utterances and even into the embodiment of professional conducts). Second, the practice of categorization is dynamic and situated (see Mäkitalo & Säljö, 2002), and its enactment is anchored in the distinctions provided by professional boundaries. Professionals assess and categorize concrete situations and individuals with reference to such distinctions. Yet, discerning the subtle differences between boundary markers (such as different jargons or gestures) presupposes that the grounding of categorization in boundaries is a dynamic and context-specific process. The comparative evidence between the cases studied provides further empirical support to this notion, as the absence or breaking of boundaries forces professionals to ‘readjust’ (O2) their categories-in-use. Professionals feel that existing categories are displaced and/or ‘out of context’, not only generating confusion and paralysis in their use but also compromising the ‘reading’ and ‘anticipation’ that categorizing may bring. Finally, pigeonholing, especially as it refers to interprofessional dynamics, is enacted upon a system of justification (Hall & Slembrouck, 2009). Boundary markers allow professionals to assess whether the categories-in-use are appropriate and justify them. The absence or blurring of these markers force professionals to engage in lengthier assessment and justification processes, as we found in the quango.
Multiple influences of boundaries on collaboration
Another key finding of this article is that professionals not only use boundaries to ground category use, but that boundaries have differential influences on the identification and use of thinking and acting categories. In one form or another, distinctions between templates for understanding and for doing have been recently drawn upon to study professional routines and interactions (Bucher & Langley, 2016; Feldman & Pentland, 2003) and professional roles (Bechky, 2006). By comparatively exploring this distinction within the practice of pigeonholing, it is possible to discover an original way to start addressing two current puzzles in the literature. Namely, while the definition of boundaries as barriers that must be overcome to enable collaboration is widely acknowledged (Bechky, 2003; Carlile, 2004), collaboration and coordination between professions occurs much more frequently and efficiently than this conceptualization would predict. Furthermore, as recent studies highlight, broken or fuzzy boundaries paradoxically show negative consequences for professional collaboration and coordination, to the extent that some authors argue for the need to restore professional boundaries (Wolbers et al., 2018) or to set up substitutes (Valentine & Edmondson, 2015) to sustain interprofessional collaboration. In the remaining part of this section, we conceptually delve into the multiple and differentiated influences of professional boundaries on collaboration through their distinctive consequences on the retrieval and use of categories for thinking and acting, suggesting some answers to these puzzles.
Influences on categories for thinking
We argue that for categories for thinking, and under established conditions – where well-established and recognizable professional boundaries are in place – materialization, articulation and embodiment help professionals to more easily categorize other team members’ expertise and roles, as well as aspects of tasks. Consequently, boundaries and their markers provide the basic clues that allow for an intuitive judgement of whether someone – or something – belongs to a particular professional group, based on their resemblance to a typical group member. Boundaries ground, speed up and simplify processes of identification and coordination of others’ expertise, responsibilities and roles. This is not to say that each team member understands all the expertise and skills held by others; rather, they understand, at a minimum, the basic constitutive elements that the members of a specific professional category have in common.
Conversely, we pose that fuzzy professional boundaries provide little information about what is being delimited by them, making the practice of categorization unstable (see Hernes, 2004), a ‘hit-or-miss’ process. In contrast to the economy of perception and understanding associated with boundaries in more established conditions, any mental representation of a collective professional category and its ‘typical’ members is seriously limited and, more importantly, potentially inadequate. Our findings suggest that ill-defined boundaries trigger categorical confusion (Zuckerman, 1999) as professionals in the quango can be flummoxed by categorical ambiguity not only because it makes it difficult to identify and elicit specific professional categories for thinking, but also because it opens up to a large number of ad-hoc and idiosyncratic interpretations. In other words, boundaries grounding categories of thinking are important not only because they help anticipate and categorize a number of relevant aspects related to role, expertise and team tasks, but also because they help disregard an almost infinite number of aspects that might not be relevant.
Influences on categories for acting
As for the influences of professional boundaries on the retrieval of categories for acting, under established conditions – like the ones found in hospital settings – boundaries reinforce notions of ‘rightness’ and ‘appropriateness’ (Llewellyn, 2001). In our CD cases, we specifically found that while boundaries enabled and facilitated mutual awareness and even helped collectively anticipate paths of action or decision, under conflicting paths among group members or when tasks exceeded the established demarcated responsibilities, members from higher-status groups imposed their views and overruled other team members. Boundary markers and the mechanisms identified (especially through embodiment) serve as a reminder of the obligations with each respective professional community. In contrast, normative grip and the inherent tenacity of professional categories for acting are softened under hybrid professional conditions. Rather than drawing on clear and defined collective categories, group members seem to develop more sui generis types of epistemology to draw situated interpretations and value attributions of the different decisions and actions. This is a more intuitive epistemic practice that lacks clear boundaries and more definite contents. Therefore, existing professional patterns of actions seem to lose their normative grip, relaxing the need for consistency between new beliefs and any prior collective beliefs.
Boundaries and formal organizations
Finally, our findings enrich the recent literature that calls for a revisiting of the roles of formality and bureaucracy and their merits (Du Gay & Vikkelsø, 2016). Many recent public sector reforms have been conducted with the aim of dismantling ‘pigeonholes’ and professional autonomies under the assumption that greater collaboration and integration can only be achieved if professional boundaries and jurisdictions are radically altered (Martin et al., 2009). On the contrary, our findings provide insight into how boundary-breaking strategies have differentiated consequences on categories for thinking and acting, and suggest that interprofessional collaboration severely declines in extreme situations of boundary breaking. We hence argue that it is not enough to focus on informal relations as ‘the substance’ of these reforms; instead, the formal aspects that professional boundaries bring about in the coordination of work need to be considered if interprofessional collaboration is to be achieved.
Conclusions
Our study of different initiatives that aim at softening or breaking down professional boundaries in health care teams shows that these initiatives can hinder rather than facilitate interprofessional collaboration. We empirically found that professionals in cross-occupational groups use boundary markers to anticipate and retrieve professional categories and so enable interprofessional collaboration. We theoretically elaborate on these findings proposing that boundaries manifest in the workplace through three mechanisms (materialization, articulation and embodiment) that help professionals to ground the use of their professional categories for both thinking and acting.
Footnotes
Acknowledgements
We would like to thank Editor-in-Chief Trish Reay and the three anonymous reviewers for their guidance and thoughtful comments. For valuable feedback on multiple versions of the paper we would like to thank Daniel Menchik, Tim Morris, Paul Carlile, Roy Suddaby and Marc Ventresca. We have benefited from the insights of seminar audiences at the IAE Business School, Saïd Business School University of Oxford, Warwick Business School, and AOM. An earlier version of this paper appeared in the Proceedings of the Annual Meetings of the Academy of Management.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.