
Abstract
Two concepts of identity salience are linked to different outcomes in the social psychological literature. Identity accumulation research relates identity importance (one salience concept) to physical and mental health; identity theory connects readiness to invoke an identity (another salience concept) to role enactment. A “cross-over” line of research links volunteer identity importance to frequent enactment of the volunteer role. To integrate these lines of work, I propose that both types of salience spur more frequent role enactment, which in turn benefits well-being. Rating versus ranking measures of salience are contrasted. The identity of community volunteer is the focus, specifically, the role of hospital visitor for the Mended Hearts organization (N = 458). Analyses are disconfirming, instead showing hours spent visiting links to greater visitor identity salience (of both types), which relates to better mental health. Rating measures are more predictive than the ranking measure. Identity salience seems a key mechanism that links time spent in volunteer work to greater well-being.
Individuals classify and define themselves in a variety of ways, in terms of their enduring qualities (e.g., honest, caring, intelligent), their leisure time activities (e.g., golfer, swimmer, stamp collector), their physical appearance (e.g., overweight, tall, bald), their membership in broad social groups (e.g., African American, Episcopalian, Democrat), and their social roles (e.g., spouse, parent, employee), among other attributes. Of particular interest to symbolic interactionists are people’s self-conceptions in terms of their social roles, the building blocks of society. Enacting social roles re-creates and sustains the social structure while simultaneously supplying a basis for understanding the self as a meaningful social object (McCall and Simmons 1978; Mead 1934; Stryker 1980; Stryker and Statham 1985). Society creates the self (“who I am” in terms of one’s social roles), and in turn, the enactment of normative expectations attached to one’s roles re-creates society.
Self-definitions in terms of the roles that one holds and enacts are commonly called “role identities,” or “identities” for short. They represent mergers of persons with their roles (Turner 1978). Because people typically occupy multiple roles at any one point in the life course, they possess multiple identities (e.g., “I am a daughter, sister, aunt, journalist, and community volunteer”). The question then arises: how are these many identities ordered or structured? Most symbolic interactionists argue that identities are organized by their relative salience to the person (Callero 1985; McCall and Simmons 1978; Rosenberg 1979; Stryker 1980; Thoits 2012). But conceptions of salience differ among theorists, and theorists using particular concepts typically focus on different consequences of salience. The primary purpose of this article is to bring these separate theoretical and research traditions together. A secondary goal is to contrast the predictive utility of rating versus ranking measures of role-identity salience.
Two Salience Conceptions, Two Lines of Research
Two broad understandings of identity salience can be discerned in the literature. The term can refer to the subjective importance attached by the person to each identity he or she holds or to the person’s propensity to call forth (invoke) a particular identity within and across situations. I keep these conceptions distinct from this point onward by referring to them as importance and invocation readiness versions of identity salience, reserving salience as a term encompassing both.
Some theorists who adopt the subjective importance sense of identity salience do not explicitly use the term salience. For example, McCall and Simmons (1978) describe role identities as arrayed in a hierarchy of “prominence,” which is determined by the degree to which each identity is supported by other people, the identity performance matches personal ideals, the person is committed to the identity, and extrinsic and intrinsic rewards are obtained from role-identity performance. In other words, the greater the value or rewards gained from an identity, the greater its prominence (i.e., relative importance) in the individual’s relatively stable, idealized self-structure. 1 Rosenberg (1979) instead employs the term “psychological centrality,” defining it as the importance placed by the person on some identities over others he or she holds. The implied structure for Rosenberg is a set of rings around the individual at the core; identities that are more personally important occupy an inner set of rings, whereas those less valued fall on more peripheral rings. Others such as Callero (1985) and Thoits (1992, 2012) do employ the term salience, again referring to the personal, subjective importance that individuals accord to each identity possessed. For Callero, identity salience is assessed with a set of ratings, while Thoits (1992) posits a simple “salience hierarchy” in which multiple role identities are grouped and rank ordered from most to least importance to the self.
In contrast to the value or importance notion of identity salience, Stryker (1980) argues that salience springs from the number, intensity, and density of the social ties in which an individual is involved for each role that he or she holds. The more a particular role is embedded in a large, affectively close, and dense social network (he terms this commitment), the more salient that role identity should be to the person. Salience refers to the probability of invoking a particular role identity across a wide variety of situations or when there is choice among roles to perform. Operationally, invoking an identity means describing oneself to other people in terms of a specific role and preferring to enact that particular role when there are few behavioral constraints (e.g., during free time or on weekends). For Stryker, identities that the person is readier to invoke in these ways rank high in an ordered hierarchy of salience; identities that are less likely to be called into play as self-descriptions or enactment preferences rank low. 2
These understandings of identity salience undergird two research literatures that to date have not intersected. One line of work on role-identity accumulation, grounded in traditional symbolic interactionist thought (McCall and Simmons 1978; Mead 1934; Rosenberg 1979), posits and shows a positive association between the personal importance of an identity (salience) and individuals’ emotional and physical well-being (Greenberger and O’Neil 1993; Marcussen, Ritter, and Safron 2004; Martire, Stephens, and Townsend 2000; Reitzes and Mutran 1994; Thoits 2012). The other line of work, based in Stryker’s (1980) structural identity theory, hypothesizes and finds that readiness to invoke an identity (salience) influences individuals’ choices about and degree of involvement in role-related activities (DeGarmo 2010; Merolla et al. 2012; Nuttbrock and Freudiger 1991; Stryker and Serpe 1982, 1994). (A third “cross-over” line of work that examines the effect of the importance of a volunteer identity on the frequency of volunteer role enactment [e.g., Callero 1985] will be discussed at a later point in the following.)
Identity Salience, Time in a Role, and Well-Being
Despite having spurred separate lines of research with different outcomes of interest, both concepts of salience could plausibly predict role enactment as well as mental and physical well-being, although for differing reasons. I use the role identity of community volunteer as an example here because it is the focus of this study, but the argument should apply to other conventional roles that people hold.
From a general symbolic interactionist perspective, if an individual views being a volunteer as personally important, he or she should be motivated to perform it more frequently and for longer periods of time. From an identity theory approach, the more readily a person describes himself or herself to other people as a community volunteer or indicates a preference for engaging in service work during free time, the more likely he or she is to actualize this self-definition or preference in role-related activities. In short, volunteer behavior may be performed more often because the volunteer identity is viewed as an important aspect of the self, because this identity is more readily called forth than other identities held, or for both theoretical reasons.
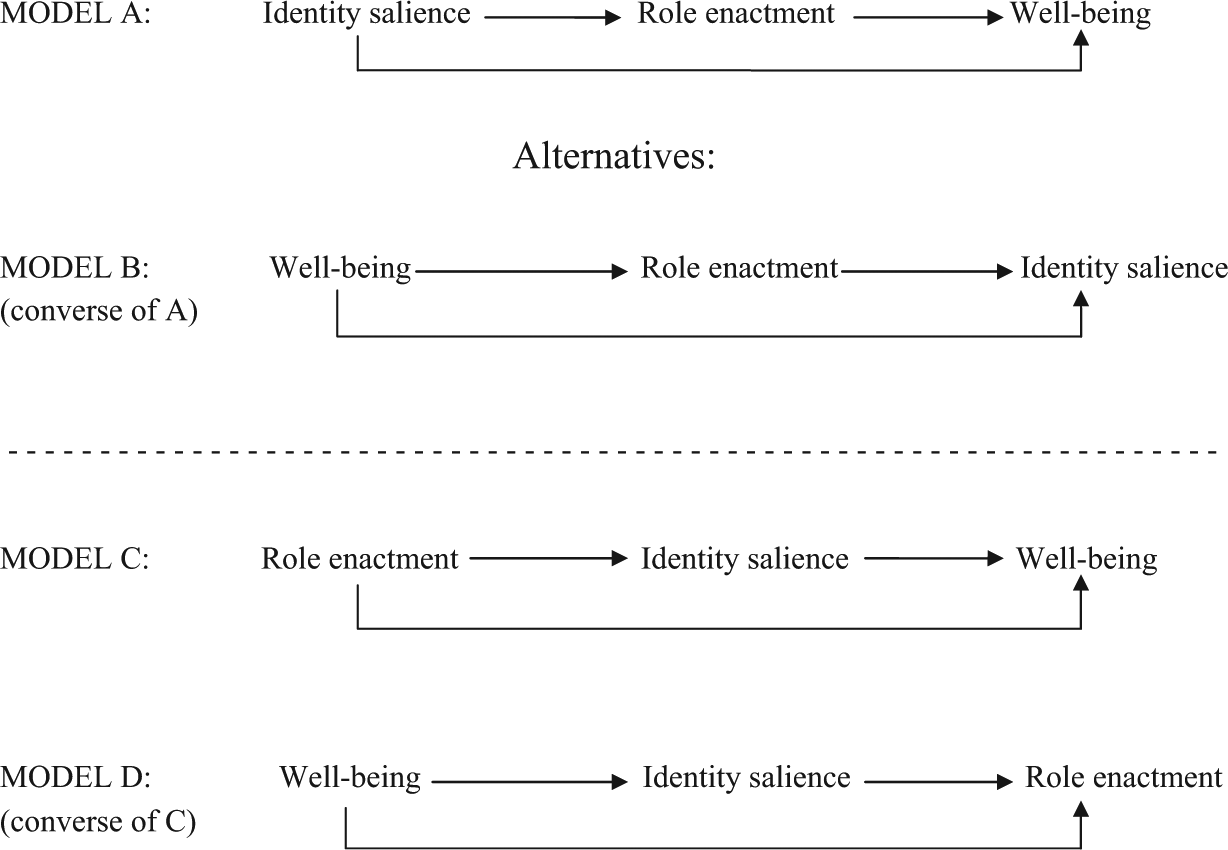
Enacting the volunteer role, in turn, should be beneficial for mental and physical health in a number of ways described in the identity accumulation literature. Role enactment provides personal gratification and social rewards (generating happiness and satisfaction), enables the development or exercise of skills and abilities (enhancing self-esteem and a sense of mastery or control), contributes to a sense of purpose and meaning in life (lessening anxiety and depression), provides normative behavioral guidance (promoting positive health behaviors), and offers opportunities for physical activity (maintaining or improving health), among other benefits (McCall and Simmons 1978; Thoits 2003, 2012; Thoits and Hewitt 2001). A salient volunteer identity (however salience is conceived and measured) thus should be connected to good mental and physical health through its influence on the frequency of role-identity enactment. In sum, these previously independent theoretical lines of argument and research easily could be spliced at the point of identity enactment, as shown in model A of Figure 1. The two concepts of salience yield identical predictions.
The Theoretical Model and Plausible Alternatives
Alternative Theoretical Predictions
The data in this study are cross-sectional so the direction of these proposed relationships plausibly could run in reverse. Individuals who are happier, more satisfied with their lives, higher in self-esteem and mastery, and mentally and physically healthier may be more willing and able to invest themselves deeply in the performance of volunteer activities, which then should lead to perceptions of greater volunteer identity salience (whether conceptualized as importance or readiness to call forth). This alternative sequence appears as model B in Figure 1; it is the converse of model A, with the independent and dependent variables reversed. Role enactment remains the lynchpin.
But other theoretical orderings are plausible. For example, the more frequently or persistently the volunteer role is performed, the greater should be the role’s salience to the individual, which then should enhance the person’s mental and physical well-being. There are two reasons why enactment frequency should affect identity salience. From a traditional symbolic interactionist perspective, the more often a role is performed, the more the role garners validation, support, and rewards from other people, reinforcing it as a valuable aspect of the self (Callero 1985; Callero, Howard, and Piliavin 1987; McCall and Simmons 1978). From an identity theory approach, frequent enactment of the volunteer role should strengthen the individual’s social ties to other people who are involved in the same service work (Serpe 1987; Serpe and Stryker 2011). The more embedded in a social network attached to the volunteer role, the more willing individuals should be to describe themselves as volunteers and to prefer to spend time in service activities (readiness to invoke). The more salience of either kind attached to the volunteer role, the more that role should provide personal validation, gratification, social rewards, self-esteem and mastery, normative guidance, and purpose and meaning in life, thus fostering positive mental and physical health, as described earlier. This theoretical sequence is illustrated as model C in Figure 1.
A final possible sequence appears as model D, the converse of model C: People in good mental and physical health should have more positive outlooks on life, predisposing them to appreciate the benefits and rewards of volunteer work and/or to cultivate and enjoy the social ties they make through those activities. Thus, the volunteer role is likely to be perceived as a more salient (valuable and/or readily descriptive) aspect of the self. The more salient the volunteer role, the more people should be motivated to spend time in service activities. In models C and D, identity salience is the mechanism tying enactment of the role to well-being.
Prior research on volunteer work suggests support for models A and B in Figure 1 over C and D. For example, a “cross-over” literature mentioned earlier has linked the subjective importance of the volunteer identity with the amount of service work that individuals perform. Callero, Piliavin, and their colleagues have shown with longitudinal data that involvement in service activities leads to the embracement of the volunteer role as an important identity at a later point in time, and the more important the volunteer identity is to the individual, the more frequently he or she enacts that role at a future time point 3 (Callero 1985; Callero et al. 1987; Chacon, Vecine, and Davila 2007; Charng, Piliavin, and Callero 1988; Grube and Piliavin 2000; Lee, Piliavin, and Call 1999). A related line of empirical research has examined the longitudinal relationship between volunteer work and well-being. The more volunteer hours worked at one point in time, the better the person’s mental and physical health at a subsequent point, and individuals in better physical and mental health at an initial period invest more hours in volunteer work in a future period (Li and Ferraro 2005, 2006; Piliavin and Siegl 2007; Thoits and Hewitt 2001; Van Willigen 2000).
For both theoretical and empirical reasons, then, I expect to find support for models A and B in Figure 1 rather than C or D. Because of cross-sectional data, one causal direction over another cannot be definitively established. I simply expect both types of identity salience to be associated positively with time spent in the role and time spent in role activities to intervene between identity salience and well-being. Although a handful of identity theory studies have shown that both types of salience correlate positively with individuals’ time spent in role performance across a number of roles (DeGarmo 2010; Nuttbrock and Freudiger 1991; Stryker and Serpe 1994), no study to date has examined associations of both types of identity salience with both types of outcomes (i.e., role enactment and personal well-being), with the expectation of similar effects. This article extends prior work, focusing on the role identity of a Mended Hearts volunteer visitor (described in the following).
The volunteer identity is advantageous for this article’s purposes because it is a role acquired by choice, and stressors in the role are low compared to those in obligatory roles (e.g., parent and employee), so the beneficial aspects of role occupancy are not counterbalanced by the strains of excessive role demands (Thoits 2003). Also, the nature of the volunteer work (visiting cardiac patients and their families in the hospital) is a constant for this study’s respondents, enabling more confident comparisons among individuals who vary primarily in the salience of the identity and the time invested in hospital visiting instead of the types of volunteer work that they do.
Ratings versus Rankings of Identity Salience
As mentioned earlier, a secondary goal is to contrast rating and ranking measures of identity salience as they relate to role behavior and well-being outcomes. There are three reasons for comparing ratings to rankings.
The first stems from an empirical observation: Evaluations of identity importance are positively associated with well-being only when people are asked for ratings of importance or subjective commitment to each social role that they hold (Greenberger and O’Neil 1993; Marcussen et al. 2004, Table 2; Martire et al. 2000; Reitzes and Mutran 1994). 4 When respondents are asked to rank order their roles by importance, their rankings are unrelated to well-being outcomes (Reitzes and Mutran 1994; Thoits 1992) or have inconsistent effects (Reitzes and Mutran 2002). Thoits (1992) speculated that respondents’ rank orderings might reflect knowledge of the relative cultural value attached to various social roles. For example, family relationships are broadly considered more important than student or work roles in American culture. Respondents’ ratings of the personal importance of each role independently of others might well diverge from such cultural consensus. When compelled to rank order his role identities, for example, a man might place his religious identity lower in his importance hierarchy than his husband and father identities, essentially taking cultural evaluations into account. But if allowed to rate the importance of each of these roles on its own, he might attach equally high value to all three or assign the highest value to his religious identity. Given such observations, personal ratings of salience (however conceived) may be more strongly connected than salience rankings to individuals’ number of volunteer work hours and well-being.
Second, a methodological observation: it is common practice among studies based in identity theory to obtain strict hierarchical rankings of identity salience from a fixed list of roles (DeGarmo 2010; Nuttbrock and Freudiger 1999; Stryker and Serpe 1982, 1994), although some studies in this tradition have utilized ratings instead (e.g., Merolla et al. 2012). Stryker and Serpe (1994), for example, compared both importance and invocation rankings of four student roles—academic, athletic, extracurricular, and friendship roles—in a college freshman sample, finding that both ranking measures contributed positively and independently to the weekly number of hours students invested in each role (although the strength of those associations varied dramatically across the four roles). But when roles are ipsatively compared, interdependence among rankings occurs: when respondents place some roles in the top spots in their hierarchies, their other roles must be placed low. Negative correlations among rankings can introduce bias.
Third, an imposed hierarchical ranking procedure from a fixed set of roles produces orderings that may not correspond closely to respondents’ perceptions: people may not see their social roles as strictly orderable. Consider, for example, how to rank order the subjective importance or relative likelihood of describing oneself as a spouse or a parent. Individuals might prefer to group some roles into ranks rather than arraying them one by one down a ladder of salience (Thoits 1992). Given potential cultural confounding, measurement bias, and task imposition problems with strict rank orderings, free-response importance rankings are employed in this article and are compared with ratings of personal importance and readiness to invoke the volunteer identity (invocation rankings are not available in the data).
Summary
In sum, I contrast the effects of (a) identity importance ratings, (b) identity invocation ratings, and (c) identity importance free rankings on the amount of time that community volunteers spend in service work as well as their mental and physical health. I test the theoretical expectation that time spent in volunteer enactment is a key mechanism linking each identity salience construct to better well-being. 5 Given the cross-sectional nature of the data, I also explore alternative orderings of these variables, as illustrated in Figure 1.
Methods
The Mended Hearts Organization
Mended Hearts is a national, nonprofit, self-help organization founded in 1951, currently affiliated with the American College of Cardiologists. Its primary mission is to provide peer support to cardiac patients and their families (Mended Hearts, Inc. 2002). Former heart patients who themselves had cardiac procedures in the past visit current heart patients and family members in the hospital to offer support, information, and reassurance. Former caregivers to heart patients also visit and supply support to family members during hospital visits. There are roughly 250 local Mended Hearts chapters nationwide. In 2009, about 179,000 visits to patients and families were made by 2,740 Mended Hearts volunteers in 400 hospitals and rehabilitation programs across the country (Littlefield 2011).
The Visiting Chair of each local chapter trains patient and caregiver visitors in support-giving techniques. About eight to ten hours of training, including supervised visits, are required for the accreditation of new volunteers, and visitors must be formally reaccredited each year. The vast majority of volunteers are former heart patients who themselves were visited in the hospital by Mended Hearts members. Accredited visitors also give support online to current heart patients or family members through the Internet Visiting Program (Mended Hearts, Inc. 2002). Each chapter additionally holds monthly meetings that are open to all cardiac patients and families in the local area, to provide continued support and up-to-date information about heart disease, surgery, medications, nutrition, and the recovery process.
Study Design and Sampling Procedures
Design
In the first of two stages in this study, survey questionnaires assessed visitors’ degree of involvement in this volunteer work, their ratings of the importance and likelihood of mentioning their visitor role to others, and their physical and emotional well-being. Questionnaires were fielded during March to May 2011. In the second stage, those visitors who indicated in returned surveys that they were willing to participate in follow-up, in-depth telephone interviews were called and asked about their reasons for visiting, the meanings they derive from this work, and how the kinds of social support they offer differ from family and friend support. Telephone respondents were asked to rate again the importance and likelihood of mentioning their visitor role as well as to rank the importance of the Mended Hearts visitor role against other roles that they held. Interviews averaged 45 minutes in duration, were recorded with permission, and were transcribed and then de-identified to maintain confidentiality. Telephone interviews occurred in May through early July 2011. Data from both the questionnaires and the telephone interviews are used in this article.
Sampling
The national office of Mended Hearts, Incorporated (MHI) does not maintain a list of visitors; only the Visiting Chairs of local Mended Hearts chapters keep lists of their volunteers. (Visiting Chairs train volunteers, set visiting schedules, and go on hospital visits themselves.) Because of this organizational structure, Visiting Chairs of selected eligible chapters were asked to distribute questionnaires to their visitors. Eligible chapters had active visiting programs, reported their numbers of visitors to the national office in early 2010, and were located in the contiguous United States. From a list of eligible chapters, 75 were randomly drawn, seven chapters with outstanding programs were added at the request of MHI, and two pretest chapters were also added because the pilot instruments did not change appreciably, creating an initial total of 84 chapters. (Including the seven requested and two pretest chapters did not alter the proportional representation of chapters by region of the country nor the average number of visitors per chapter.)
Subsequently, five chapters were found to have ended their visiting program so they were dropped as ineligible, leaving an eligible sample of 79. From the 79, 76 Visiting Chairs were successfully contacted and all agreed to assist in distributing questionnaires. Due to illness, interrupted chapter meetings, or unknown reasons, six of the 76 Visiting Chairs did not follow through. Thus, visitors in 70 chapters were involved in the study, a total of 877 potential respondents (an average of 12.5 visitors per chapter).
Of potential respondents, 458 returned a survey, a response rate of 52 percent. With this participation rate, the study findings cannot be generalized statistically to describe the Mended Hearts visitor population as a whole. However, theoretical generalizations are still possible from hypothesis testing with these data, assuming valid measures of constructs.
Of the 458 survey respondents, 49 percent were willing to be interviewed by phone (N = 226). Telephone respondents differed from the survey sample on a number of variables, summarized in the following.
Measures
Unless otherwise noted in the text, all variables described in this section are derived from the questionnaire data.
Well-being variables
Well-being is tapped by six indicators: happiness, life satisfaction, self-esteem, a sense of mastery, psychological distress, and physical health.
Happiness and life satisfaction are considered measures of subjective well-being or quality of life (Diener et al. 1999). For happiness, respondents were asked, “When you consider everything about your present life, how would you describe yourself?” (5 = very happy, 4 = somewhat happy, 3 = neither happy nor unhappy, 2 = somewhat unhappy, and 1 = very unhappy). For life satisfaction, they were asked, “Thinking about your present life, how satisfied are you with your life in general?” with responses ranging from 5 = very satisfied, to 3 = neither satisfied nor dissatisfied, to 1 = very dissatisfied.
Self-esteem and a sense of mastery are viewed as aspects of mental health or psychological well-being (Ryff 1989). For self-esteem, Rosenberg’s (1979) well-validated 10-item scale was employed. Example items are “I feel that I have a number of good qualities” and “All in all, I’m inclined to feel like a failure” (reverse coded), with responses ranging from 4 = strongly agree to 1 = strongly disagree. To reduce missing values, each participant’s responses were summed and then divided by the number of items he or she answered to produce an average response to the scale. Thus, participants’ scores ranged from 1 to 4 in value (from low to high self-esteem). Cronbach’s alpha for the scale was .76. Pearlin’s seven-item mastery scale (Pearlin et al. 1981) assessed respondents’ sense of personal control over life. Illustrative items are “I have little control over the things that happen to me” (reverse coded) and “What happens to me in the future mostly depends on me,” with responses from 4 = strongly agree to 1 = strongly disagree. Respondents’ answers were summed and then divided by their number of answers, so scores ranged from 1 = low to 4 = high mastery with an internal consistency of .71.
Psychological distress is a state of emotional malaise consisting of symptoms of anxiety and depression. Symptoms were assessed with the anxiety and depression subscales of the Brief Symptom Inventory (Derogatis and Spencer 1982). For anxiety symptoms, respondents were asked, “In the past month, including today, how much were you distressed by: nervousness or shakiness inside, suddenly scared for no reason, feeling fearful or afraid, feeling tense or keyed up, spells of terror or panic, feeling so restless you couldn’t sit still?” Depression symptoms included: “feelings of worthlessness, thoughts of death or dying, feeling lonely, feeling blue, thoughts of ending your life, feeling no interest in things, feeling hopeless about the future.” Possible responses were 0 = not at all, 1 = a little bit, 2 = moderately, 3 = quite a bit, 4 = extremely. Respondents’ answers to all items were summed and divided by the number of valid answers, so scores ranged from 0 = low to 4 = high psychological distress, with a Cronbach’s alpha of .84.
A physical health scale consisted of four items. The first was “How would you rate your health in general?” For comparable scaling with other health items, responses were coded as 4 = excellent, 3 = very good, 2 = good, 1 = fair or poor. The second item was, “Compared to other people your age, how would you rate your health in general?” For comparable scaling, this was coded 4 = better than most people my age, 2.5 = about the same as most people my age, 1 = worse than most people my age. The third was, “How often does your health get in the way of what you want to do?” (1 = very often to 4 = never). Finally, “How satisfied are you with the current state of your health?” (4 = very satisfied to 1 = very dissatisfied). Respondents’ responses were summed and divided by their number of valid answers. Scores ranged from 1 to 4 (poor to good physical health). The internal consistency was .78.
Role enactment variables
Participants were asked two questions (at different points in the survey) about their degree of involvement in visiting activities, one objective, the other subjective. The objective item assessed weekly hours spent visiting: “About how many hours each week do you spend visiting, on average?” 6 For perceived time spent visiting, respondents were asked, “How much time do you spend being a volunteer visitor?” with responses on a 10-point scale, anchored at one end with 1 = “I spend almost no time being this” and at the other with 10 = “I spend most of my time being this.” Objective and subjective role enactment were only modestly correlated (r = .29, p < .001) so both indicators are included in the analyses.
Identity salience variables
Three measures of visitor identity salience are employed: a rating of identity importance (from the survey), a rating of identity invocation (from the survey), and a ranking of the identity in the respondent’s importance hierarchy (from the telephone interview). It should be noted that the Mended Hearts visitor role was in fact considered a personal identity by an overwhelming majority of respondents; when asked in the telephone interview, “Some people say that being a parent is ‘who they are’ or that their work ‘gives them an identity.’ Do you see being a visitor this way? Is it part of who you are—an identity for you?,” 81 percent of respondents (N = 218) replied “yes.” 7
The rating of identity importance was in response to the survey question, “We know that you have many important roles such as husband/wife, parent, employee, church member, and friend. Among your various roles, how important to you is being a Mended Hearts visitor?” (1 = not at all important to 10 = extremely important). Although the stem to this question appears to request a rank ordering, participants responded in terms of the personal importance of the visitor role; 88 percent of those who gave a rating of 8, 9, or 10 (the most frequent answers to this question) responded 8, 9, or 10 to a simpler query in the follow-up interviews (conducted weeks later) that did not refer to other roles: “On a scale of 1 to 10, where 1 is not at all important and 10 is extremely important, how important to you is being a Mended Hearts visitor?” The gamma coefficient for the ordinal relationship between the two versions of the importance question (collapsed into low, moderate, and high importance) was .70 (p < .001) for respondents who answered both questions (N = 216). Responses to the survey question are used in order to take advantage of the full sample N in later analyses.
The probability of identity invocation was assessed with a survey question: “How likely is it that you would mention your role as a Mended Hearts visitor to someone you met for the first time?” (1 = not at all likely to 10 = extremely likely). A version of this question was also asked in the telephone interview: “If you were describing yourself to someone you met for the first time at a party or while on vacation, how likely is it that you would mention volunteering as a Mended Hearts visitor to this person?” Telephone participants’ open-ended responses were coded into 1 = never or very unlikely, 2 = somewhere in between or somewhat likely, 3 = very likely or almost always. When collapsed into low, moderate, and high likelihood, the survey replies were associated moderately strongly with the interview responses (gamma = .41, p < .001, N = 220). Again the responses to the survey question are used to take advantage of the full sample N in subsequent analyses.
Location in the importance hierarchy
In the telephone interview, participants were asked, “Think about the other roles you may have in your life, for example, being a spouse, a parent, a grandparent, a worker, a friend, as well as your religious, political, and leisure time activities. Which of your roles are more important than being a visitor? Which roles are less important than visiting?” Respondents were free to mention as many or as few of their roles as they wished and to order them in ways that seemed appropriate to them.
Most respondents organized their roles in a strict importance hierarchy. The following are example excerpts and how they were initially coded (all names are pseudonyms and chapter locations are identified only by broad region of the country):
Well, I guess my faith would be first, my wife would be second, my children—although they’re all adults now—would come third, and then probably Mended Hearts. [I: Okay, would anything be less important than visiting with Mended Hearts?] Less important? Uh, kind of don’t know how to relate to that. I don’t know . . . (pause) um, (laughs) . . . . (
Okay, well, definitely being a parent, you know, supersedes being that [Mended Hearts visitor], and right now, I’m a first-time grandparent, so that would supersede— [I: Congratulations.] Thank you. And so that would make it, at this point that would make it third, but I think friends—I have my [best?] friends from high school and from college, so [visitor] would fall below them [friends] needing me for some reason, and as far as—it is above religion or political identity, so it probably comes in after parent, grandparent, daughter to my mother, friends, and then it would come in fifth, I guess. (
However, some respondents grouped several roles at the same level or rank:
Oh, well, I think it’s secondary to the spousal relationship and so on. And the parent. Those have to come first, your family, I guess . . . [I: Right. So you mentioned that being a spouse and being a parent were both more important than being a visitor. Can you think of any other roles that you feel are more important than being a visitor?] Well, I, I don’t look at being a visitor as exclusive to being a good neighbor or to being able to work and do your job. It isn’t exclusive of that. You’re not sacrificing your work, I don’t think, in those cases. So you can do that [job] along with it [visitor]. (
Mm-kay. Uh, my God comes first, my family comes second, and after that, we have a level playing field. [I: Okay.] So, Mended Hearts would be in the third layer, with my friends, and I teach, but I am retired, if that makes any sense. I’m retired from one profession, and teach only two courses at the university right now, so, you know, all of it makes me who I am. And so Mended Hearts is in that third layer. (
Two considerations altered how I ultimately coded visitor importance rankings. 8 First, as evident in the previous excerpts, many respondents mentioned a variety of specific family roles (e.g., spouse, parent, grandparent, son/daughter). However, others simply cited “family” as an all-inclusive role identity. Penny provides an example:
In general? Um, [the visitor role is] important but not at the top. [I: Okay. So . . . which of your roles would you say are more important than being a visitor?] Um, my church involvement. [I: Okay. Anything else that’s more important to you?] Um, well, my family. [I: Okay. And, um, are there specific things you can think of that are less important to you than visiting?] Hmm. (pause) Gee, that’s a hard question. I don’t know. Maybe just being a housewife? (laughs) (
To increase comparability among respondents’ rankings of the visitor identity, I collapsed all specific family roles that were mentioned by a participant into one (“family”) and recoded the standing of Mended Hearts visitor and the total number of roles in each respondent’s listing.
The second issue stemmed from the free-response format of the interview questions. Unlike the fixed set of roles that are typically ranked in identity theory research, respondents spontaneously mentioned a varied number of roles, ranging from one to six after specific family roles were collapsed. It seemed reasonable to standardize the placement of the visitor identity in respondents’ hierarchical lists by the number of roles that they mentioned. To do this, I renumbered where Mended Hearts visitor was placed relative to the top of each person’s list and divided by the total number of roles he or she cited. To illustrate, consider three respondents, all of whom put visitor second from the top in their lists. Person A mentioned two roles in her list, first family and then visitor, so visitor is essentially at the bottom of her very short list. Person B mentioned three roles, so visitor is in the middle of his importance hierarchy. Person C mentioned six roles, so visitor is very high in his list of six. Dividing the placement from the top by the number of roles mentioned yields a value that varies from 0 to 1, indicating just how high up in each respondent’s importance hierarchy the visitor identity was positioned. The actual values ranged from .17 (the lowest observed location, corresponding to the bottom position among six roles) to 1.0 (the highest possible position within a respondent’s total list of roles, however long or short the list).
Control variables
Respondents’ social statuses and other aspects of their visitor role are controlled in the analyses. Female is coded 1 = female, 0 = male. Age is in years. Minority status is based on answers to two questions, “Are you of Hispanic, Latino, or Spanish origin?” (yes, no) and “What racial group or groups best describe you?” (from a list). Those who indicated that they were non-Hispanic and white were coded 0, all others were coded 1. Educational level was collapsed into 1 = high school or less, 2 = some college or associate degree, 3 = bachelor’s degree, and 4 = graduate or professional degree. Annual family income was not assessed because most respondents (86%) were retired. To indicate socioeconomic status, a scale of financial difficulties was constructed from three items, “At the present time, how much difficulty do you have in paying your bills?” (4 = a great deal to 1 = none at all), “At the end of the month, do you end up with: 4 = not enough money to make ends meet, 2.5 = just enough to make ends meet, 1 = some money left over,” and “Overall, how satisfied are you with your financial situation?” (4 = very dissatisfied to 1 = very satisfied). Responses were summed and divided by the number of items answered for each participant, so scores ranged from 1 to 4 (low to high financial difficulties). Cronbach’s alpha was .84.
Most people hold multiple roles. The more roles held, the less time participants may be able to devote to visiting and thus the lower they may rate the importance of the visitor identity or their readiness to invoke it. To control for the potential effects of multiple role occupancy, I summed the number of roles individuals held based on whether they were married or living with a partner (yes = spouse/partner), whether they had children (yes = parent), whether they had grandchildren (yes = grandparent), whether they were working full- or part-time for pay (yes = employee), whether they were attending religious services once a month or more often (yes = churchgoer), and whether they belonged to clubs or organizations other than Mended Hearts (yes = group member). The number of social roles (beyond visitor) ranged from 0 to 6.
The number of years as a volunteer visitor is controlled in the analyses as it may positively influence the salience of the visitor role-identity or the amount of time invested in that role. Years as a visitor is proxied by the respondent’s years of membership in Mended Hearts; the telephone interviews indicated that most visitors began visiting within a year of joining the organization.
Finally, whether the respondent was a patient visitor (1 = yes, 0 = no) is controlled, given that former heart patients with histories of treatment for serious heart disease may have poorer physical or mental health compared to caregiver visitors.
Clustering Issues
Because visitors are nested within chapters, potential cluster effects must be considered, as observations with correlated errors violate an assumption of ordinary least squares (OLS). The means of the dependent variables may not only vary across individuals, they may also vary by chapter (i.e., cluster). Thus, the total variation in the dependent variables may be attributable both to within-clusters variation (individual-level variation) and to between-clusters variation (chapter-level variation). To assess cluster effects, intraclass correlation coefficients (ICCs) were calculated for each dependent variable with a random intercept model with no covariates, using Stata 11 (StataCorp 2009). The ICC, or rho, indicates the proportion of variation in the dependent variable that is attributable to between-clusters variation. For three of the outcome variables (happiness, life satisfaction, and physical health), the ICC was zero, indicating no cluster effects. Self-esteem, mastery, and distress had non-zero ICCs, but the Breusch-Pagan test indicated that between-groups variation was not significantly different from zero except for self-esteem, χ2(1) = 6.45, p < .01. Upon further exploration, the results of random effects estimation of self-esteem multivariate models were virtually identical to those using OLS estimation with robust standard errors; robust standard errors control for clustered design but do not model random intercepts. Given virtually identical results, OLS estimates are presented for self-esteem, to be consistent with models for the other five dependent variables. All models in the article are estimated in Stata with OLS using robust standard errors.
Results
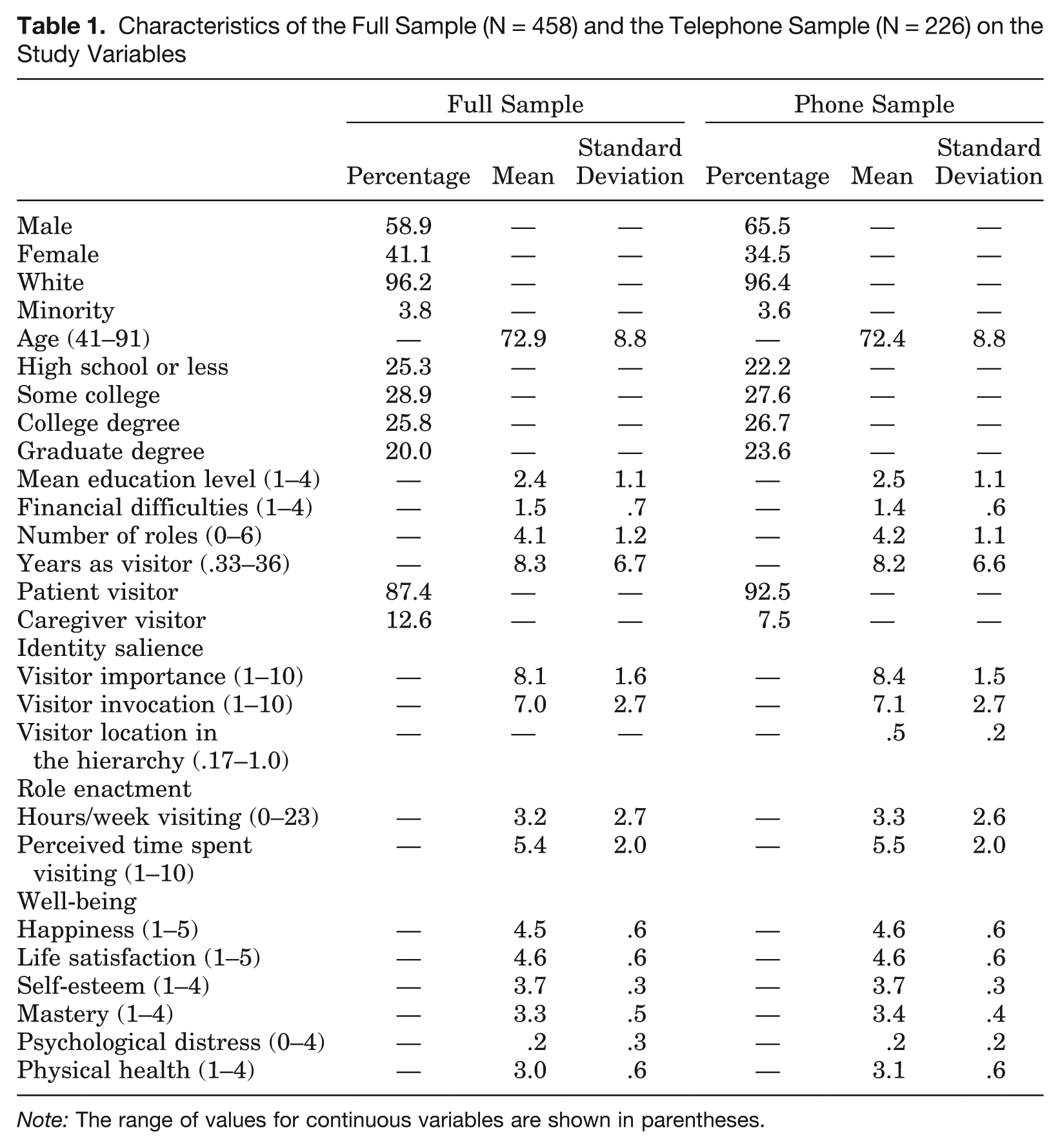
Table 1 summarizes the characteristics of the sample as a whole and of the subset of respondents who participated in the qualitative telephone interviews.
Characteristics of the Full Sample (N = 458) and the Telephone Sample (N = 226) on the Study Variables
Note: The range of values for continuous variables are shown in parentheses.
The two samples are highly similar. A majority of respondents are men, almost all respondents are white, and the average age is 73. About 75 percent of participants have some college education or more and report low levels of financial difficulties, so they are primarily middle-class in socioeconomic status. Participants hold an average of four additional roles beyond visitor so they are socially integrated. They have been visiting for Mended Hearts an appreciable number of years (a mean of eight years) and are primarily patient visitors, indicating that they are former heart patients themselves.
Respondents rate the visitor identity as highly important, with an average of 8 on a 10-point scale. Their rating of the likelihood of invoking the visitor identity is also high, a mean of 7 on a 10-point continuum. However, when participants (in the telephone sample only) rank the importance of the visitor identity against other identities that they hold, visitor is placed in the middle of the importance hierarchy, which ranges from the lowest possible ranking of .17 to the highest possible ranking of 1.0. Clearly, some role identities consistently take precedence over the visitor identity. Most frequently these were family and religious roles (not shown), while other involvements (including employee, friend, club member, neighbor, leisure time activity, and political group member) were viewed as less crucial than the visitor role (not shown).
Respondents spend about three hours per week in visiting activities. (Zero hours are possible because hospitals forbid visiting when volunteers are ill, volunteers took trips, or they had increased job demands. All study participants are active visitors but a handful had temporarily suspended their hospital visiting work for such reasons.) Subjectively, participants rate how much time they spend being a visitor midway between spending “no time” and “most of my time,” suggesting an overestimate of their actual time investment.
In terms of well-being, participants see themselves as somewhat to very happy and satisfied on average. They have very high self-esteem, a moderately strong sense of mastery over their lives, markedly low distress, and good (but not excellent) physical health. Overall, Mended Hearts participants enjoy good mental and physical health.
When respondents who completed only the questionnaire are compared to those who participated in both the survey and the telephone interview, telephone respondents differ significantly (not shown) on a number of variables but generally to small degrees: telephone respondents are more often male, have more years of education, have lower financial difficulties, have slightly more roles, accord more importance to the visitor identity, and are somewhat happier, more satisfied with life, higher in self-esteem and mastery, and healthier. These differences between the survey-only and survey-and-phone respondents are not surprising; persons who are enthusiastic about the role-identity and who are in good mental and physical health are probably more willing to talk to researchers in detail about their volunteer experiences.
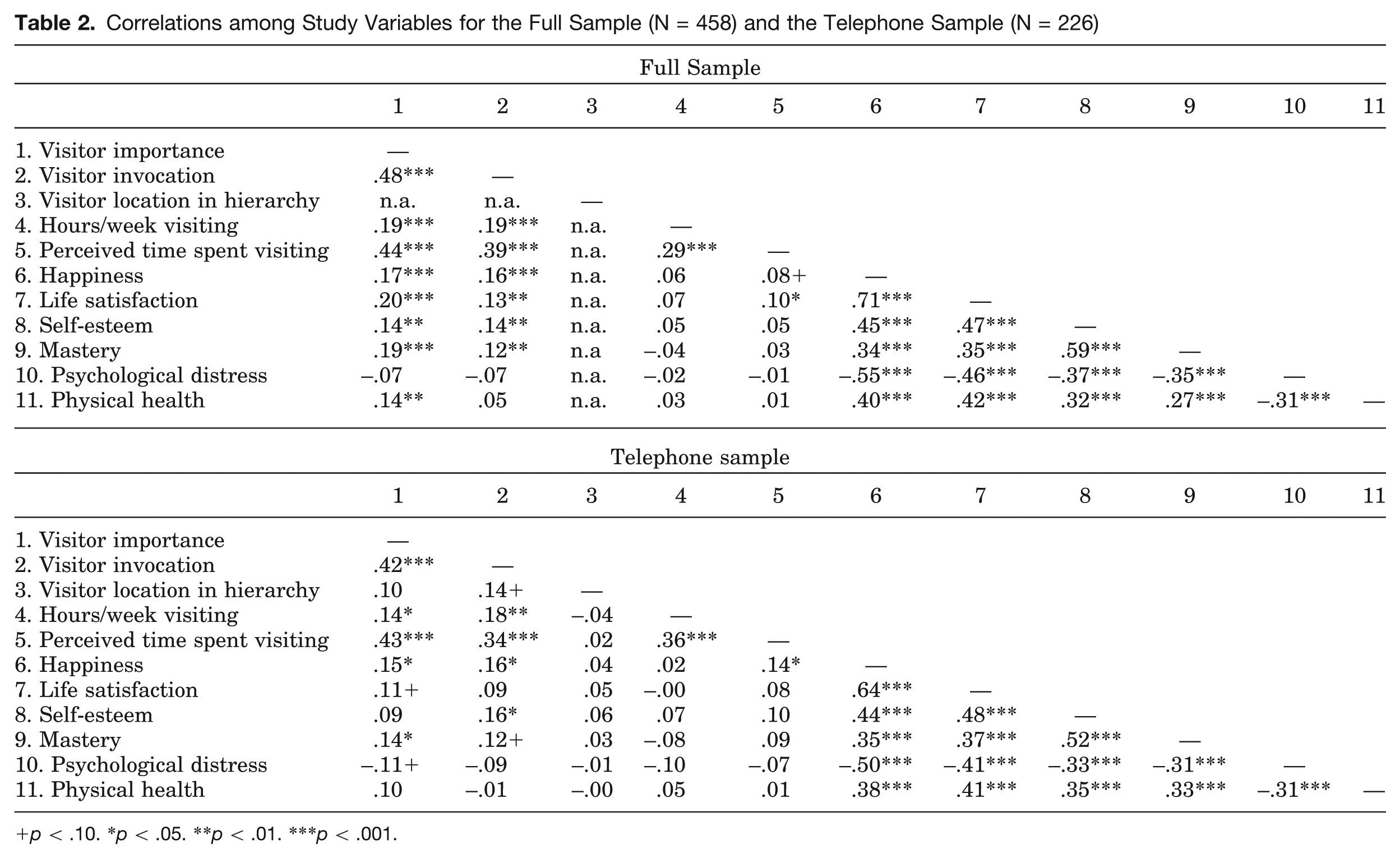
Table 2 presents correlations among the main independent and dependent variables in the two samples. The correlations are very similar across the two groups, so only general patterns will be described. First, note that ratings of visitor identity importance and the likelihood of visitor invocation are correlated moderately strongly and positively with one another (.48 and .42, p < .001, in the two samples, respectively). However, the ranked location of Mended Hearts visitor in respondents’ importance hierarchies (see the telephone sample) is unrelated to identity importance and weakly and only marginally associated with the probability of identity invocation, suggesting that these three salience variables are tapping different aspects of the construct of salience.
Correlations among Study Variables for the Full Sample (N = 458) and the Telephone Sample (N = 226)
p < .10. *p < .05. **p < .01. ***p < .001.
Second, only identity importance and identity invocation ratings are positively and significantly linked with role enactment variables. The relative ranking of the visitor role in the importance hierarchy (in the telephone sample) has no relationship with hours spent visiting or perceived time spent in the role.
Third, only identity importance and identity invocation ratings are linked to the well-being variables (with exceptions with respect to life satisfaction, distress, and physical health). The relative importance ranking of the visitor identity is unrelated to all well-being outcomes.
Finally and unexpectedly, role enactment variables generally are not linked to mental and physical health. Weekly hours spent visiting does not correlate with any well-being outcome, while perceived time spent visiting is positively associated only with happiness and life satisfaction.
Overall, the most striking pattern in Table 2 is the total lack of relationship of respondents’ identity importance rankings (i.e., location of Mended Hearts visitor in the importance hierarchy) with role performance or well-being variables. Regressions (not shown) of role enactment and well-being variables on identity importance rankings with control variables held constant confirmed that respondents’ rankings of visitor identity importance were unrelated to subjective or actual time spent in role or to the six mental and physical health indicators. 9 With respect to a Mended Hearts volunteer identity, importance rankings do not seem to be useful measures of identity salience.
Given this finding, I focus the remaining analyses only on comparisons of importance versus invocation ratings of salience, taking advantage of the greater number of respondents in the full sample. (All findings discussed in the following were replicated in the smaller telephone sample.)
Role Enactment as a Mediator of the Identity Salience–Well-Being Relationship (Models A and B)
I hypothesized that time spent in visitor role performance would be the mechanism through which identity importance and/or identity invocation would be related to well-being (model A in Figure 1). To test this hypothesis, I first regressed each well-being measure on visitor importance and the probability of invoking the visitor identity, holding constant the control variables. In a second step, I added hours of visiting and perceived time spent visiting. If role enactment intervenes in the identity salience–well-being relationship, then significant salience coefficients should become smaller and nonsignificant after role enactment indicators are controlled.
The results of these analyses are not shown, as the findings were clear and unambiguous: although both types of visitor identity salience were positively linked to good mental and physical health as expected (as will be seen in other analyses in the following), this relationship was not forged through frequent performance of the visitor role-identity. When the time investment variables were entered into the analyses, their coefficients were near zero in size and nonsignificant in every equation estimated. In short, model A (Figure 1) was not supported.
Given these findings, model B, which reverses the independent and dependent variables in model A, also should be unconfirmed. Analyses verified this (not shown); significant positive effects of well-being variables on the visitor identity salience measures were somewhat reduced in size but never eliminated when role enactment variables were controlled in a second analytical step.
In sum, time spent in visiting activities did not connect the salience of the Mended Hearts visitor identity to participants’ emotional or physical well-being, contrary to expectations.
Identity Salience as a Mediator of the Role Enactment–Well-Being Relationship (Model C)
As noted earlier, the relationships posed in model A plausibly could occur in alternative theoretical orders. One possibility, shown as model C in Figure 1, was that the more time spent in role performance, the more salient the visitor role-identity should be, which in turn should reinforce emotional and bodily well-being. To test this alternative model, the well-being variables were regressed first on the role enactment measures, with control variables included in the equations. In the next steps, the identity salience indicators were added singly and then together. The results of these analyses are reported in Table 3.
The Effects of Visitor Role Performance and Visitor Identity Salience on Well-Being (Model C)
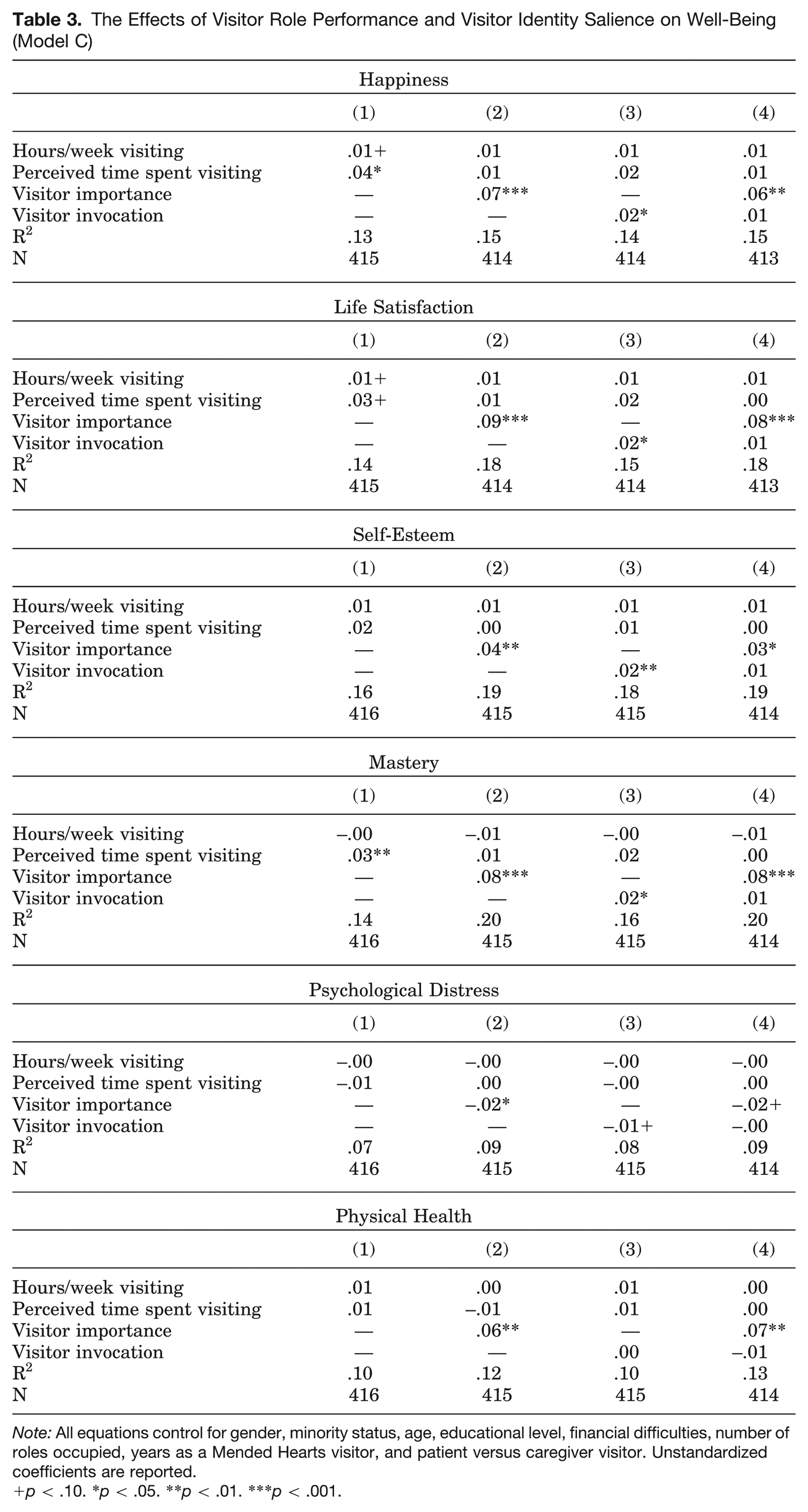
Note: All equations control for gender, minority status, age, educational level, financial difficulties, number of roles occupied, years as a Mended Hearts visitor, and patient versus caregiver visitor. Unstandardized coefficients are reported.
p < .10. *p < .05. **p < .01. ***p < .001.
Scanning down the column for the first equations in Table 3, we see that the more frequent the respondent’s performance of the visitor role, the greater his or her happiness, life satisfaction, and sense of mastery. Specifically, perceived time spent visiting is positively associated with all three well-being variables; actual hours invested in visiting links marginally to more happiness and life satisfaction only. 10 Equations 2 and 3 show that ratings of the importance of the visitor identity and the likelihood of identity invocation are each significantly associated with all six well-being variables in expected directions (e.g., greater happiness, lower distress). If identity salience mediates the role enactment–well-being relationship, we should see significant coefficients for weekly hours and for perceived time spent visiting in the first equations become nonsignificant and near-zero in equations 2 and 3. This indeed happens in both equations 2 and 3 for happiness, life satisfaction, and mastery, indicating that the salience of the visitor identity (however measured) does mediate these three associations. Model C is supported for three of the six well-being indicators.
One additional pattern is of note in Table 3. The significant coefficients for identity invocation in each equation 3 become nonsignificant and almost zero when ratings of visitor importance are controlled in each equation 4 for happiness, life satisfaction, self-esteem, sense of mastery, and psychological distress. This pattern suggests that visitor identity importance mediates the effect of the respondent’s readiness to invoke the visitor identity on well-being. In other words, a process is implied: the more time invested in enacting the visitor identity, the greater the participant’s likelihood of mentioning it to other people. The more ready he or she is to call out the identity, the more the respondent perceives the identity to be important, which in turn is associated with better mental health. However, it is also possible that rather than mediating the influence of identity invocation on well-being, identity importance subsumes it; readiness to invoke the visitor identity may be an aspect of viewing the visitor identity as personally important.
Reverse Causality: Identity Salience as a Mediator of the Well-Being–Role Enactment Relationship (Model D)
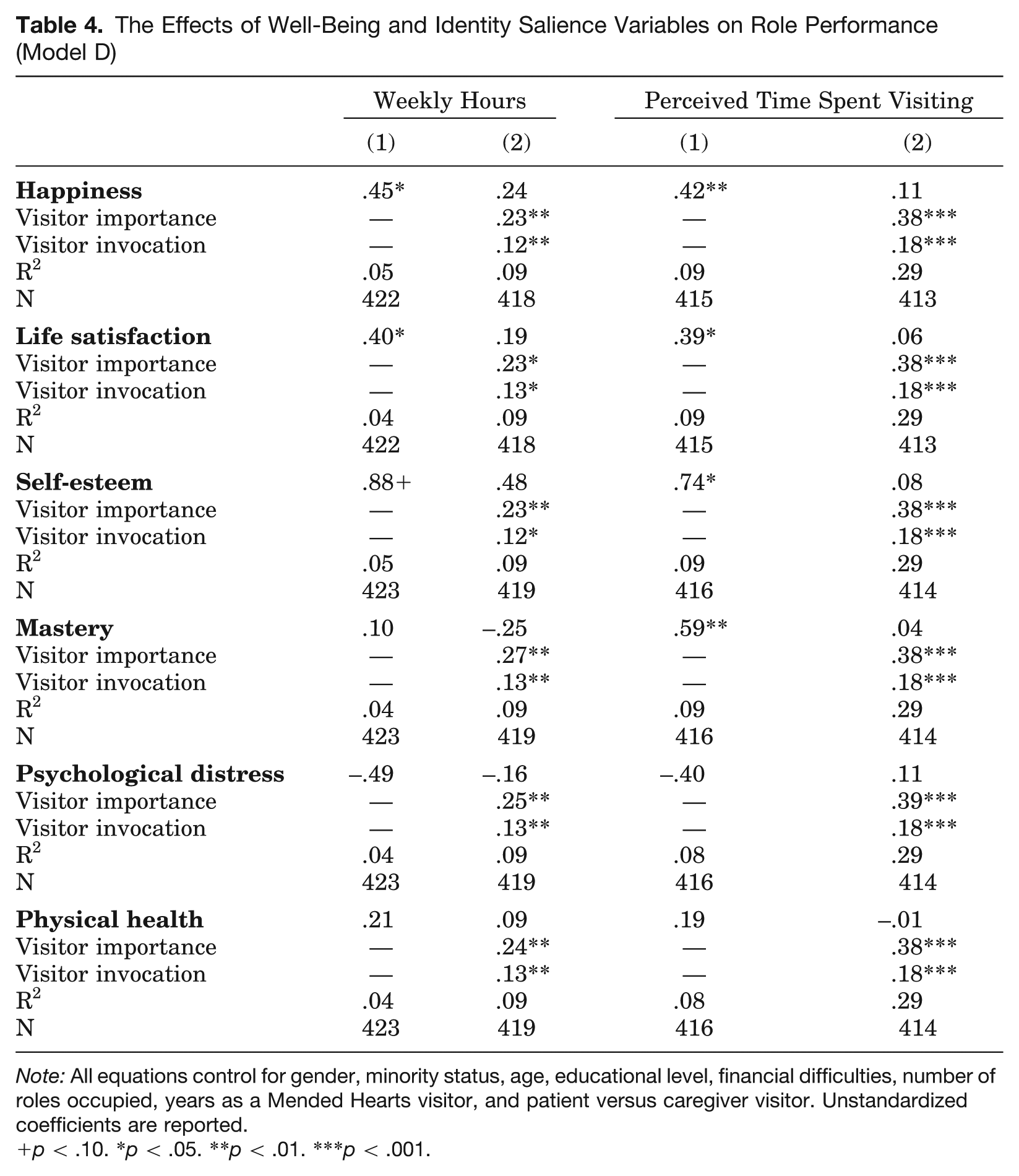
Given the findings in Table 3, Model D, the causal reverse of model C, is also likely to find support. To examine model D, role performance indicators were regressed on each well-being indicator first, with control variables held constant. In the next step, the two identity salience measures were introduced together, with results summarized in Table 4.
The Effects of Well-Being and Identity Salience Variables on Role Performance (Model D)
Note: All equations control for gender, minority status, age, educational level, financial difficulties, number of roles occupied, years as a Mended Hearts visitor, and patient versus caregiver visitor. Unstandardized coefficients are reported.
p < .10. *p < .05. **p < .01. ***p < .001.
Scanning down the equation 1 columns in Table 4 we see that happiness, life satisfaction, and self-esteem are significantly associated with investing more hours weekly and perceiving more time spent in hospital visiting. Respondents with a greater sense of mastery over life also perceive that they spend more time in the visitor role. Symptoms of psychological distress and degree of physical health, however, do not influence the role enactment variables.
In the equation 2 columns, ratings of visitor importance and the probability of visitor invocation are significantly and positively associated with role performance outcomes. (Each measure of salience was directly and significantly related to the role enactment variables when entered separately into each equation 2, not shown.) Respondents who rate the visitor identity as highly important and who are very ready to mention the role in describing themselves to other people donate significantly more hours per week to hospital visiting and perceive themselves as spending a good deal of time in visiting activities.
Once the identity salience measures are controlled in each equation 2, well-being coefficients that were significant in each equation 1 become nonsignificant and dramatically reduced in size, indicating that identity salience mediates the well-being–time in role relationship, consistent with model D in Figure 1. It should be noted that when the identity salience measures were added singly to the second equations of Table 4 (not shown), each measure fully mediated the positive influences of happiness, life satisfaction, self-esteem, and mastery on role enactment outcomes.
In sum, the analyses generally support models C and D, rather than models A and B, of Figure 1.
Discussion and Conclusions
The primary purpose of this article was to bring together two previously independent lines of theorizing and research on the consequences of role-identity salience, one line linking the subjective importance of a role identity to better mental and physical health, the other connecting readiness to invoke an identity with more frequent role enactment. I argued that both salience conceptions should positively affect the amount of time people invest in role-related activities, which in turn should generate greater psychological and physical health benefits.
The analyses did not support my argument (model A in Figure 1) or its theoretical reverse (model B): role enactment did not connect identity salience to well-being nor well-being to salience. Instead, the salience of the volunteer identity was the mechanism connecting time invested in service work with individuals’ well-being in both theoretical directions (models C and D). Individuals who spent more of their time visiting patients and their families in the hospital rated their visitor identity as more important and said they were more likely to mention it to other people. Viewing the visitor identity as salient in these ways was associated with several aspects of mental health (happiness, satisfaction, mastery), but not physical health. Conversely, Mended Hearts visitors in good mental health saw their visitor role as more important and were readier to call it up when describing themselves to other people; the more salient the visitor identity in these ways, the more time participants spent performing Mended Hearts volunteer activities. The findings for models C and D thus hint at an unfolding, cyclical process over time: high rates of role enactment foster a strong sense of role-identity salience, which in turn benefits psychological well-being; greater well-being strengthens identity salience, which in turn motivates further role-identity performance. These results also are consistent with the idea of a reciprocal causal relationship between identity invocation and role enactment raised as a possibility by identity theorists (Serpe 1987; Serpe and Stryker 2011) and explored in one study (DeGarmo 2010). Additional longitudinal research will be necessary to confirm or refute actual directions of these effects and the process implied by the findings.
Although both types of identity salience were expected to behave similarly in the analyses (for different theoretical reasons), their influences on time spent in volunteer activities and on well-being diverged in an unanticipated way. As expected, both the personal importance of the visitor identity and participants’ readiness to mention this identity predicted greater perceived and actual time invested in hospital visiting (Table 4). In contrast, although both salience constructs were significant predictors of well-being on their own, when entered together in the analyses, only identity importance retained its significance (Table 3). This unexpected effect suggested that the personal value placed on the visitor identity might intervene between invocation readiness and well-being or, alternatively, that personal importance is a broader, more inclusive construct that simply subsumes invocation readiness as a component. I am more inclined toward the former interpretation than the latter for two reasons.
First, if identity importance did encompass identity readiness, then importance and readiness to invoke should not have had simultaneous, independent, significant effects on time spent in performing the visitor role (Table 4). Second, for conceptual reasons, the two constructs should relate differently to role behaviors than to physical and psychological well-being. Volunteers do service work for a variety of reasons, in part because it is who they are in their own and others’ eyes (i.e., the role comes to mind readily as self-descriptive) and in part because they attach personal value to the volunteer role (i.e., it is important to them), among other motivations. In contrast, performing the volunteer role should affect well-being less because it is a ready way to describe oneself (or preferred as a free time activity) and more because volunteer work is viewed as valuable and personally meaningful (Thoits 2012). Individuals derive meaning and both intrinsic and extrinsic rewards from performing a valued role identity (McCall and Simmons 1978), including positive emotions that constitute aspects of psychological well-being (happiness, satisfaction, pride in oneself and one’s abilities), which can also bolster physical health (Fredrickson et al. 2008). It seems theoretically plausible that the volunteer role takes on importance over time because it has been grounded in numerous and dense social ties and becomes readily accessible as a self-description, as described in identity theory. In turn, the importance attached to the role determines the degree to which positive benefits are reaped from its enactment. Of course, these observations are speculative and require further research on relations between the two identity constructs as well as how they are associated with other substantive outcomes.
A secondary goal of this study was to compare the predictive utility of the two identity salience concepts when measured with ratings versus rankings, with the expectation that ratings might be more powerfully linked to individuals’ role performances and well-being than rankings; this was indeed the case. The ranking measure of identity importance was completely uncorrelated with time spent in visitor role performance or with any aspect of well-being. This may be because importance rankings capture broad cultural consensus about the relative value of the volunteer role rather than individuals’ own views of its personal significance. Supporting this possibility, respondents’ personal importance ratings were unrelated to their rankings of visitor importance (Table 2, telephone sample). Telephone respondents also were in considerable agreement about which roles ranked higher in importance than Mended Hearts visitor (family and religious roles), again suggesting cultural consensus. Their views echo patterns reported by Thoits (1992), wherein close family roles were ranked as “first most important to me” on average, church was in the “second most important to me” rank, while the volunteer identity fell below the “third most important to me” rank for married and unmarried men and women. In sum, the results here suggest that ratings of identity salience (both importance and invocation readiness) may be more powerful than rankings. The jury will remain out, however, until there are additional comparisons of salience ratings with rankings.
There are a number of limitations of this study that must be acknowledged. That the data are cross-sectional, leading to uncertainty regarding causal direction, has already been discussed. A clear limitation is the lack of a ranked measure of visitor invocation for comparison to the other three salience measures. Also, the three salience measures are based on single item indicators, which can be unreliable. An additional problem is that only one role identity is examined in this study. One could argue, however, that this is advantageous, given that everyone in the sample held, was trained for, and performed the same Mended Hearts volunteer role, thus reducing ambiguity due to variations among the types of service work a random sample of community volunteers might do. Finally, the sample is overwhelmingly older, white, middle class, and retired in its social composition, and respondents have volunteered for this organization an impressive number of years. Whether the relationships documented in the study would be replicated in more diverse samples of volunteers with shorter durations of service remains an empirical question.
Stepping back, the findings support research that has documented a reciprocal relationship between enacting a volunteer role and the personal importance attached to that role (Callero 1985; Callero et al. 1987; Charng et al. 1988; Grube and Piliavin 2000; Lee et al. 1999). Much of that literature has focused on a volunteer activity that is relatively undemanding, occasional, and brief: donating blood. Visiting cardiac patients and their families in the hospital every week to provide reassurance and support is a much more time- and effort-intensive service activity than periodic blood donation. It is significant that the positive associations in the blood donation literature between donor role enactment and donor identity importance are also seen for a far more demanding volunteer involvement, hospital visiting (see also Grube and Piliavin 2000; Lee et al. 1999).
This article pushes work on the volunteer identity one step further by connecting it not only to the frequency of service activities but to volunteers’ well-being. Frequent volunteer activity not only strengthens the salience of the volunteer role (which leads to more service) but the salience of the volunteer role enhances individuals’ psychological well-being. Such findings suggest that service organizations in need of committed, active workers would find it useful to attend to conditions that encourage identity salience: fostering strong social ties to other volunteers in the organization and highlighting the value and meaning volunteers can derive from their service. Closer researcher attention to the processes that influence individuals’ selection of specific roles for self-description and performance will likely suggest other strategies (e.g., Lee et al. 1999; McCall and Simmons 1978; Serpe 1991). Exploring a wider range of determinants of volunteer identity salience seems a compelling new direction for both theoretical and practical reasons.
Footnotes
Acknowledgements
I am grateful for the generous assistance of Tim Elsner, former Executive Director of Mended Hearts, Incorporated (MHI); Marcia Baker, Field Director, MHI; Don Arvay, National Visiting Chair, MHI; and the Mended Hearts visitors who participated in this study. I appreciate the valuable work of Sociological Research Practicum Assistants: Christy Erving, Eric Grollman, Sarah Hatteberg, Amy Irby, Jaime Kucinskas, and Kody Steffy. Shawna Rohrman provided helpful statistical advice.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported with funds from Indiana University and the Department of Sociology.