
Abstract
Using a sample of 344 dual-earner African American married couples, this study examined the effect of control over work on depressive symptoms and physical health with a dyadic model. The mediating role of personal resources capturing positive self-evaluations (i.e., self-esteem and mastery) was also examined. The association between wives’ control over work and wives’ physical and mental health was mediated by wives’ positive self. Although husbands’ control over work was not directly associated with husbands’ physical or mental health, it was associated with their sense of positive self, which influenced their level of depressive symptoms and physical health. No cross-spouse influences were found, suggesting a lack of interdependence for African American husbands and wives. The practical implications of this research include the value of work organization policies that may increase workers’ sense of control and personal resources as these variables are important to workers’ health outcomes.
Consistent with the stress-illness perspective (Pearlin, Schieman, Fazio, & Meersman, 2005; Pearlin & Skaff, 1996), research has shown that chronic stressful experiences contribute to negative health outcomes directly and indirectly through the erosion of individual psychological resources. Although lack of control at work is stressful for workers (K. A. S. Wickrama, Lorenz, Fang, Abraham, & Elder, 2005), there may be consequences for workers’ spouses as well, and little research has examined these social epidemiological pathways, particularly in African American working couples. Thus, the current study investigates how African American husbands’ and wives’ control over work (hereafter termed work control) influences their own as well as their spouses’ mental and physical health outcomes through these processes.
The few studies that have examined the associations among work conditions, personal resources, and health have primarily used Caucasian samples and have found that personal resources mediate the relationship between work conditions and individuals’ well-being (e.g., Xanthopoulou, Bakker, Demerouti, & Schaufeli, 2007). These findings are often then generalized to other ethnicities. Therefore, less is known about how these constructs operate for other racial/ethnic groups, and research, such as the current study, is needed to expand on existing knowledge and demonstrate if these models are accurate for other ethnic groups, including African Americans.
Moreover, there are reasons to believe that the associations among work conditions, personal resources, and health may be stronger for African Americans. First, it is well documented that African Americans suffer higher rates of disease and poorer health outcomes (e.g., higher rates of chronic health conditions, such as hypertension and diabetes, and health risk behaviors) than other ethnicities (House, Lantz, & Herd, 2005; Warner & Hayward, 2006). Therefore, it is important to examine psychosocial predictors, such as work control, and personal resources, such as self-esteem and mastery, that may influence these health outcomes. Second, self-evaluation, which is closely associated with ethnic pride and ethnic identity (E. P. Smith, Walker, Fields, Brookins, & Seay, 1999), may be more salient for African Americans and, thus, exert a stronger influence of their health outcomes than Caucasians. Third, compared to Caucasian couples, marital quality and marital stability are lower in African American couples (Broman, 2005). This may lead to fewer, or weaker, dyadic cross-spouse effects between African American couples than Caucasian couples. Fourth, African Americans are disproportionately employed in “blue-collar” jobs associated with lower levels of work control. Research suggests that the associations between socioeconomic conditions, well-being, and health are more pronounced among individuals who are in the lower rung of the socioeconomic status (SES) hierarchy (Marmot, 1989). Thus, extending on this argument, not only are there notable differences in the mean levels of economic conditions, self-evaluations, and physical health between African Americans and Caucasians, but there is reason to believe that the associations between these variables may be stronger for African Americans than Caucasians. However, less is known about these associations in African Americans, particularly using dyadic data.
In this study, we aim to enhance the understanding of the relationships between work control, personal resources, and physical and mental health among a sample of African American husbands and wives. Our utilization of dyadic data is an improvement on existing research and allows us to account for the interdependence between husbands and wives, examine dyadic and transactional (cross-spouse) relationships between husbands and wives, and compare the strength of effects between husbands and wives to determine potential gender differences within the same modeling framework. Figure 1 depicts this conceptual model.
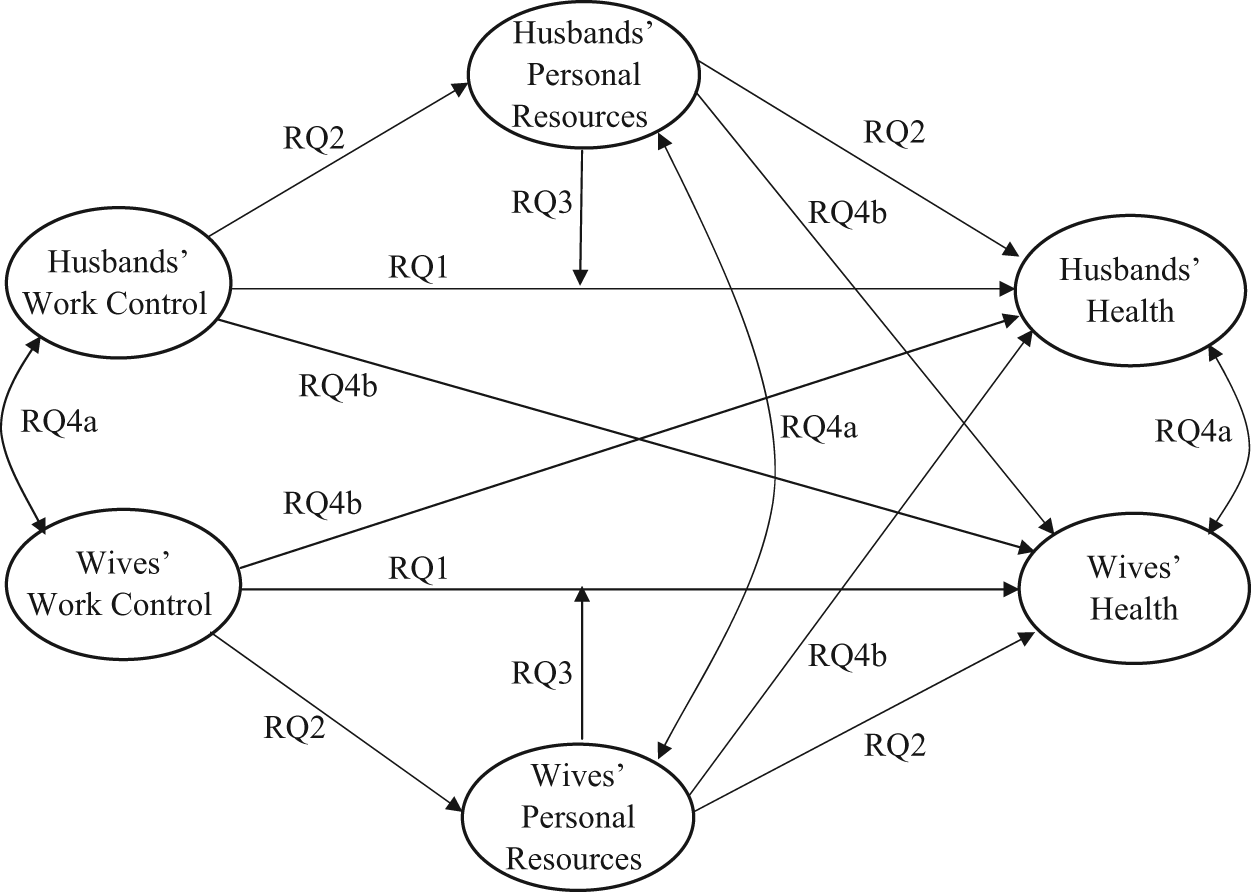
Conceptual framework: Applying the stress-illness perspective.
The Direct Influence of Work Control on Health
Work control is a psychosocial characteristic made up of two dimensions, including the breadth of skills one can use at work (i.e., skill discretion) and the amount of control over one’s work (i.e., decision latitude; Karasek & Theorell, 1990). Existing research has shown the distinct influence of work control beyond the influence of other work environment variables on mental health (Griffin, Fuhrer, Stansfeld, & Marmot, 2002), health behaviors (Devine, Connors, Sobal, & Bisogni, 2003), and self-assessed global health (K. A. S. Wickrama, Surjadi, Lorenz, & Elder, 2008).
Consistent with the stress-illness perspective (Pearlin et al., 2005; Pearlin & Skaff, 1996), this association can be attributed to physiological processes associated with chronic stress, which can stem from lack of control over work (K. A. S. Wickrama et al., 2005). Chronic stress associated with lack of work control has been shown to have detrimental long-term biological consequence because of various physiological stress responses, including the malfunctioning of metabolic, cardiovascular, and neurological processes (Juster, McEwen, & Lupien, 2010). In addition, there are structural constraints, such as the lack of free time and energy for exercise, stress relief, or other health-promoting behaviors, associated with low control over work that contribute to poor health (Bielby & Bielby, 1989; Nomaguchi & Bianchi, 2004). African Americans are more likely to occupy the lower rung of the SES hierarchy where the association between these stressors/structural constraints and health outcomes are stronger (Marmot, 1989). In the present study, we will examine the direct association between work control and health outcomes in African American husband and wives (Research Question 1a).
Previous work using rural Caucasian couples has found work control to exert a greater influence on men’s health than women’s health (K. A. S. Wickrama et al., 2005; K. A. S. Wickrama, Conger, Lorenz, & Matthews, 1995). However, because more African American women than Caucasian women are employed outside the home and African American wives’ income represents a sizeable amount of the family income (Mincy & Pouncy, 2003), the work role is likely to be more salient to their personal identity and, thus, related to their health outcomes. Thus, we will examine if work control influences the health outcomes of African American husbands and wives equally (Research Question 1b).
The Influence of Work Control on Personal Resources
Consistent with the stress-illness perspective (Pearlin et al., 2005; Pearlin & Skaff, 1996), lack of work control erodes individual psychological resources such as self-esteem and mastery (erosion hypothesis). Previous empirical research provides support for the link between work control and individual psychological resources, including self-esteem (Xanthopoulou et al., 2007) and mastery (K. A. S. Wickrama, Lorenz, Conger, Matthews, & Elder, 1997). Self-esteem refers to the beliefs an individual holds about their own value, whereas mastery, also known as personal control, refers to beliefs about the ability to control circumstances (Lazarus, 1966; Thompson, 1981).
Previous research provides several intra-individual mechanisms that explain the association between work control and personal resources. First, drawing from the work socialization perspective, the self-directedness hypothesis states that jobs with high work control lead to intellectual flexibility, which enhances personal resources, such as self-esteem and mastery, by maximizing feelings of empowerment and self-direction within the employee (Kohn & Schooler, 1982; Miller, Schooler, Kohn, & Miller, 1979; Schooler & Naoi, 1988). Second, an individual’s self-appraisal (e.g., self-esteem and mastery) is strongly tied to how they believe others view them (Rosenberg, 1979). Workers without skill discretion or work latitude may infer that others have a negative perception of them and their capabilities, and this external appraisal may then be adopted as an internal appraisal of their self. In addition to the potential of a more substantial association existing between work control and health for African Americans than Caucasians because of their concentration in the lower run of the SES hierarchy (Marmot, 1989), research indicates a strong link between ethnic pride and identity and personal resources (E. P. Smith et al., 1999). In the present study, we will examine the indirect association between work control and health in African American husbands and wives through their mastery and self-esteem (Research Question 2).
The Influence of Personal Resources on Health
Consistent with the stress-illness perspective (Pearlin et al., 2005; Pearlin & Skaff, 1996), eroded psychological resources increase individuals’ vulnerability to poor mental and physical health (vulnerability hypothesis). Numerous studies using Caucasian samples have provided evidence for this association (Gerstorf, Rocke, & Lachman, 2011; Lever, Pinol, & Uralde, 2005; Orth, Robins, & Roberts, 2008; Seeman & Lewis, 1995; Trzesniewski et al., 2006; Whisman & Kwon, 1993; K. A. S. Wickrama et al., 2008). Of these studies, many have focused exclusively on mental or physical health separately, which fails to account for the shared variance between physical and mental health outcomes.
Several mechanisms explain the association between these personal resources and health outcomes. First, low self-esteem is often coupled with avoiding social situations or neglecting personal relationships, thereby reducing social support that is associated with depression (Ottenbreit & Dobson, 2004). Second, substance abuse and other dangerous health-risk behaviors are more prevalent among those with low self-esteem (Donnellan, Trzesniewski, Robins, Moffitt, & Caspi, 2005), which have serious mental and physical health consequences (Goldstein et al., 2008; Umberson, Wortman, & Kessler, 1992).
Pudrovska, Schieman, Pearlin, and Nguyen (2005) highlight processes that account for the link between mastery and health outcomes. For instance, because persons with low mastery do not believe they can produce the outcomes they desire, they are unlikely to engage in anticipatory coping, such as initiating preventative health behaviors or seeking professional help to manage existing health problems. Furthermore, mastery is also associated with the use of problem-focused coping (Holahan & Moos, 1991), which helps individuals determine effective strategies for attaining or maintaining good health (Folkman, 1984; Penley, Tomaka, & Wiebe, 2002). Finally, those with high mastery are likely to focus on aspects of their health that can be improved or maintained.
Additionally, consistent with the stress-illness perspective, research has also shown that exposure to stress does not lead to poor health for those with high mastery (Pudrovska et al. 2005) or self-esteem (Corning, 2002). This moderating effect lead to the conclusion that self-esteem and mastery are coping mechanisms that act as buffers to reduce the influence of stressors on health (Thoits, 2011). Furthermore, because African Americans’ personal resources may be enhanced, or hindered, by their ethnic identity (E. P. Smith et al., 1999), we will examine if this moderating effect is present for African Americans (Research Question 3).
Dyadic, Cross-Spouse Associations
Consistent with the family system perspective, interdependence is one of the defining elements of marital relationships (Thibaut & Kelley, 1959). However, researchers have only recently begun to take this interdependence into consideration by appropriately accounting for the “linked lives” of husbands and wives (Elder & Giele, 2009). There is reason to believe that dyadic and cross-spouse associations may exist in relation to individuals’ work control and their partners’ physical and mental health outcomes, making work stress a family issue. For instance, stress at work (i.e., lack of work control) can “crossover” to influence the partner’s distress, psychosomatic symptoms, and health status (Bolger, Delongis, Kessler, & Wethington, 1989; Burke, Weir, & DuWors, 1980; Eckenrode & Gore, 1981; Jackson & Maslach, 1982). Similarly, personal resources of the partner are likely to influence marital quality (Donnellan, Conger, & Bryant, 2004), which in turn is influential for both mental and physical health outcomes (Bookwala, 2005; Choi & Marks, 2006; Lincoln & Chae, 2010; K. A. S. Wickrama et al., 1995). In addition, personal resources and health outcomes of husbands and wives may be correlated (Lorenz & Hraba, 2004). Although research examining potential cross-spouse effects within African American couples is needed to advance the field’s understanding of racial minority couple relationships, the tendency of African American couples to report lower levels marital quality (Broman, 2005) may create emotional distance and separation between husbands and wives and, consequently, hinder cross-spouse influences. Thus, we will examine if dyadic (Research Question 4a) and cross-spouse (Research Question 4b) associations are present for African American husbands and wives.
Throughout the existing research, many studies have treated self-esteem and mastery as separate personal resources. This research is necessary and helpful in determining the different effects of these resources. However, self-esteem and locus of control are both broad evaluations that individuals make about themselves and have been shown to contain a common core (Judge, Erez, Bono, & Thoresen, 2002) which we refer to as positive self. Research examining positive self is needed for two reasons. First, the breadth of this concept may increase the consistency of results across studies. Second, the use of this broader concept enhances the predictive validities of the particular constructs. For these reasons, and following the work of Hatton et al. (2008), we treat global self-esteem and mastery as indicators of one core higher order construct of positive self that captures the properties of both mastery and self-esteem.
Summary of Research Questions (Figure 1)
Research Question 1: Does work control directly influence the depressive symptoms and physical health of African American husbands and wives (Research Question 1a)? Are there gender differences in this effect (Research Question 1b)?
Research Question 2: Does work control indirectly influence the depressive symptoms and physical health of African American husbands and wives through positive self?
Research Question 3: Does positive self buffer against influence of work control on health outcomes?
Research Question 4: Do dyadic (Research Question 4a) and cross-spouse (Research Question 4b) associations exist between control at work and health outcomes (depressive symptoms and subjective reports of physical health) and/or between positive self and health outcomes?
Method
Sample
The data for the present study came from a project funded by the National Institute of Child Health and Human Development, A Study of African American Marriage and Health, to study African American couples residing in rural and urban areas of the Southeast (R01-HD050045-05; Chalandra M. Bryant, Principal Investigator). Data collection began in 2005. At that time, the study area was characterized by a 20% poverty rate and a 5% unemployment rate. African Americans comprised 46% of the population in the study area (average percentages based on the 2000 Census of the United States).
Because the purpose of the initial study was to study changes in African Americans’ marriages and health over the life course, African American couples who recently married were recruited. Letters were sent to the addresses found on recent marriage license applications inviting them to participate in the study. To be eligible for the study, both partners had to be African American, at least 20 years of age, and agree to participate. Face-to-face interviews were scheduled in the homes of the participants through follow-up phone calls. Two African American interviewers visited the homes of the participants and interviewed the husband and wife separately in different rooms.
Wave one data were collected from 697 African American newlywed couples residing in the Southeast ranging in age from 20 to 79 years (wives’ M = 33.16, SD = 9.56; husbands’ M = 35.64, SD = 10.61). Wave two data were collected from 501 of these couples (72%) approximately 1 year later. An attrition analysis was conducted for all study variables and showed that husband and wife “stayers” who completed both waves reported slightly higher education and income than “attriters.” Husbands who stayed reported slightly higher self-esteem and fewer physical health complaints.
Dual-earner couples providing data at Waves one and two were used for the current analyses. The subsample included 344 (N = 688) dual-earner African American couples ranging in age from 21 to 63 years with a median age of 31 and 28 years for husbands and wives, respectively.
This was the first marriage for 74.7% of the wives and 68% of the husbands. Roughly two fifths of husbands (40.5%) and 21.5% of wives held a high school diploma or less. One third of the wives (34%) and a small portion of the husbands (16.6%) in the sample earned a college degree. At Wave 1, husbands reported a median personal earned income ranging from $30,000 to $34,999 (SD = 2.65), and 87.8% worked at least 40 hours a week. Wives reported a median personal earned income ranging from $20,000 to $24,999 (SD = 2.79) with 77.6% of wives reporting that they work 40 hours or more each week. More than 61% of couples had at least one child younger than 18 years living in their household.
Measures
Depressive symptoms
Depressive symptoms were assessed as a latent construct using 16 items of the Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977) at Wave 2. The other four items of the original 20-item scale were shown to measure positive affect and were, thus, excluded from the current analyses. The 16 items loaded onto three factors capturing behavioral, psychological, and social symptoms of depression. Respondents indicated on a 4-point scale ranging from 1 (1 day a week) to 4 (5-7 days a week) for how often in the past week they were bothered by each symptom. The five items addressing behavioral symptoms of depression included items such as “I felt like everything I did was an effort” and “I had trouble sleeping.” Items addressing social symptoms included “I felt that people were unfriendly” and “I felt that people disliked me.” Psychological symptoms were assessed using responses from nine items, such as feeling sad or lonely. For each of the three factors, mean scores were computed. Higher scores indicate the presence of more symptoms of depression. Internal consistencies for behavioral and psychological symptoms of depression were .57 and .75 for husbands and .66 and .88 for wives. Social symptoms of depression were measured by two items with a statistically significant correlation of .45 and .37 for husbands and wives, respectively.
Physical health
Physical health was assessed as a latent construct consisting of respondents’ self-assessments of global health and physical health complaints at Wave 2. Research has shown that subjective health ratings are strong predictors of morbidity among African Americans (Ferraro & Farmer, 1999) as well as mortality in many community studies using various ethnicities (Idler & Benyamini, 1997). A reduced version of three items from the Short Form 36 health survey questionnaire (SF-36) was used to assess respondents’ global health on a 5-point scale from 1 (strongly agree) to 5 (strongly disagree), including “I seem to get sick a little easier than other people I know,” “I am as healthy as anybody I know,” and “I expect my health to get worse.” Two items were reverse coded so that higher scores indicate poorer global health. Internal consistencies for the global health items were .53 for husbands and .66 for wives. Adapted from K. A. S. Wickrama, Bryant, and Wickrama (2010), respondents reported the frequency of eight physical health complaints (i.e., sore throat or sinus problems, headaches, back pain, nervousness, irregular heartbeats or chest pain, upset stomach or stomach aches, sexual dysfunction, persistent problems with teeth/gums) they experienced over the past year. These complaints were selected because they relate to five of the major anatomical systems including: skeletal, circulatory, digestive, neurological, and respiratory systems. Responses were rated on a 4-point scale ranging from 1 (not at all) to 4 (a lot), and means were computed. Higher scores reflect more physical health complaints. Although the internal consistency values indicate the items are not closely associated (α = .69 and .63 for husbands and wives, respectively), we believe the counts of complaint frequency reflect the severity of poor physical health.
Work control
Two latent constructs (one for wives and another for husbands) were used to assess husbands’ and wives’ work control separately at Wave 1. As shown in Figure 2, each latent construct was defined by two observed indicators: decision latitude and skill discretion. Decision latitude was assessed using four items derived from Karasek and Theorell (1990): “I have a lot to say about what happens on my job,” “I have a flexible work schedule in my job,” “In my job, I am mostly my own boss,” and “My job gives me the amount of independence I like.” Skill discretion was measured by respondents’ agreement with five items including: “My job requires that I learn new things,” “My job requires me to be creative,” “My job requires a high level of skill,” “My job matches what I like to do,” and “I have a lot of opportunities to use my ideas and imagination in my job.” All items were rated on a 5-point scale (from 1 = strongly agree to 5 = strongly disagree), and responses were averaged to create a mean score for decision latitude and skill discretion separately with higher values indicating less decision latitude and skill discretion. Internal consistencies for decision latitude were .67 and .64 for husbands and wives, respectively, and the internal consistencies for skill discretion were .76 and .77 for husbands and wives, respectively.
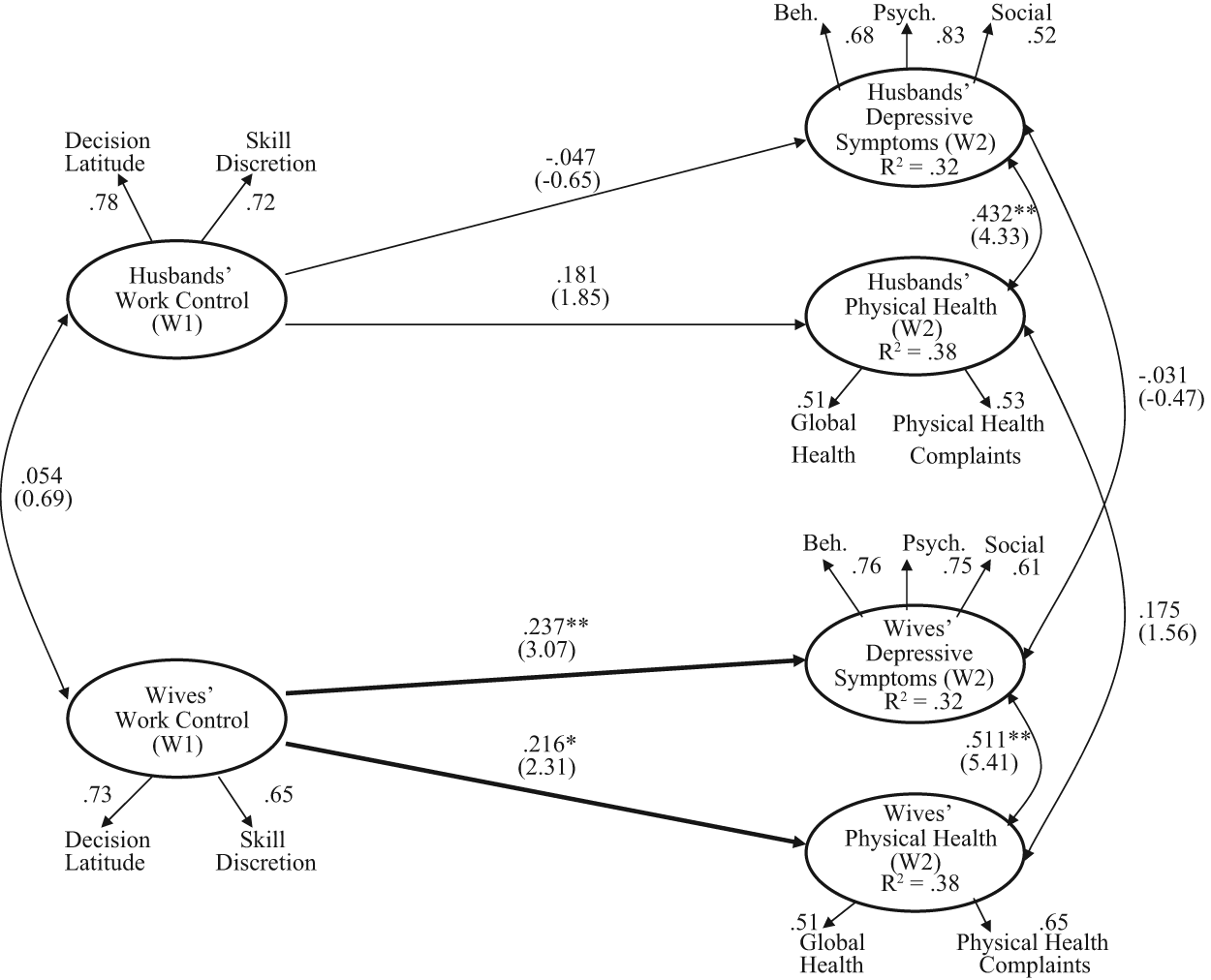
The direct influence of work control on husbands’ and wives’ depressive symptoms and physical health.
Positive self
Two latent constructs (one for wives and another for husbands) were used to assess husbands’ and wives’ sense of positive self (similar to the concept of core self-evaluations by Judge, 2009; Judge et al., 2002) at Wave 1. As shown in Figure 2, each latent construct was defined by two observed indicators: self-esteem and mastery. We believe that these two indicators adequately capture the higher level construct of positive self. Seven items from the Rosenberg (1965) self-esteem scale were used to assess self-esteem. Example items include, “I feel that I have a number of good qualities” and “I am able to do things as well as most other people.” Four items from Pearlin’s mastery scale (Pearlin, Menaghan, Lieberman, & Mullan, 1981) measured mastery. Items included the following: “There is really no way I can solve some of the problems I have,” “Sometimes I feel that I’m being pushed around in life,” “I have little control over the things that happen to me,” and “I often feel helpless in dealing with the problems of life.” Both scales were rated on a 5-point scale (from 1 = strongly agree, to 5 = strongly disagree). Three items measuring self-esteem and all four items measuring mastery were reverse coded so that lower scores indicate a more positive self-view. Mean scores were computed for self-esteem and mastery separately. Lower scores reflected more positive self-esteem and a greater sense of mastery over tasks. Internal consistencies for self-esteem and mastery were .68 and .72, respectively, for husbands and .75 and .69, respectively, for wives.
Analyses
A latent-variable structural equation model with full information maximum likelihood was used to examine the proposed associations between constructs. Structural equation model was chosen because it facilitates the analysis of actor and partner effects concurrently. This is an improvement over multiple regression analyses, which fail to simultaneously analyze the effects that wives and husbands have on each other. Estimates were obtained using the AMOS 17.0 software package (Arbuckle, 2006). Goodness of fit was assessed using multiple fit indices, including the chi-square statistic, comparative fit index (CFI), and root mean square error of approximately (RMSEA). CFI values greater than .93 (Byrne, 1994) and RMSEA values less than .05 are thought to indicate a good model fit (Browne & Cudeck, 1993). Additionally, the chi-square statistic divided by the model’s degrees of freedom was examined as an estimate of the overall model fit. Values less than 3.0 suggest a good model fit (Carmines & McIver, 1981). Following existing research (e.g., Cox et al., 2004; T. Wickrama & Bryant, 2011), the moderation hypothesis was analyzed using mean splits to determine if the association between husbands’ and wives’ work control and health outcomes varied for those with high and low positive self.
Results
Correlations and Descriptive Statistics
Descriptive statistics are shown in Table 1, and bivariate zero-order correlations among the latent constructs are shown in Table 2. Most of the correlations among latent constructs were as expected. On average, husbands’ and wives’ work control were not significantly correlated (r = .054, p > .05), but sense of positive self for husbands and wives was significantly correlated (r = .208, p < .01). Husbands’ and wives’ self-assessed physical health were significantly correlated (r = .238, p < .05), but depressive symptoms were not significantly correlated (r = .030, p > .05).
Descriptive Statistics of Study Variables.
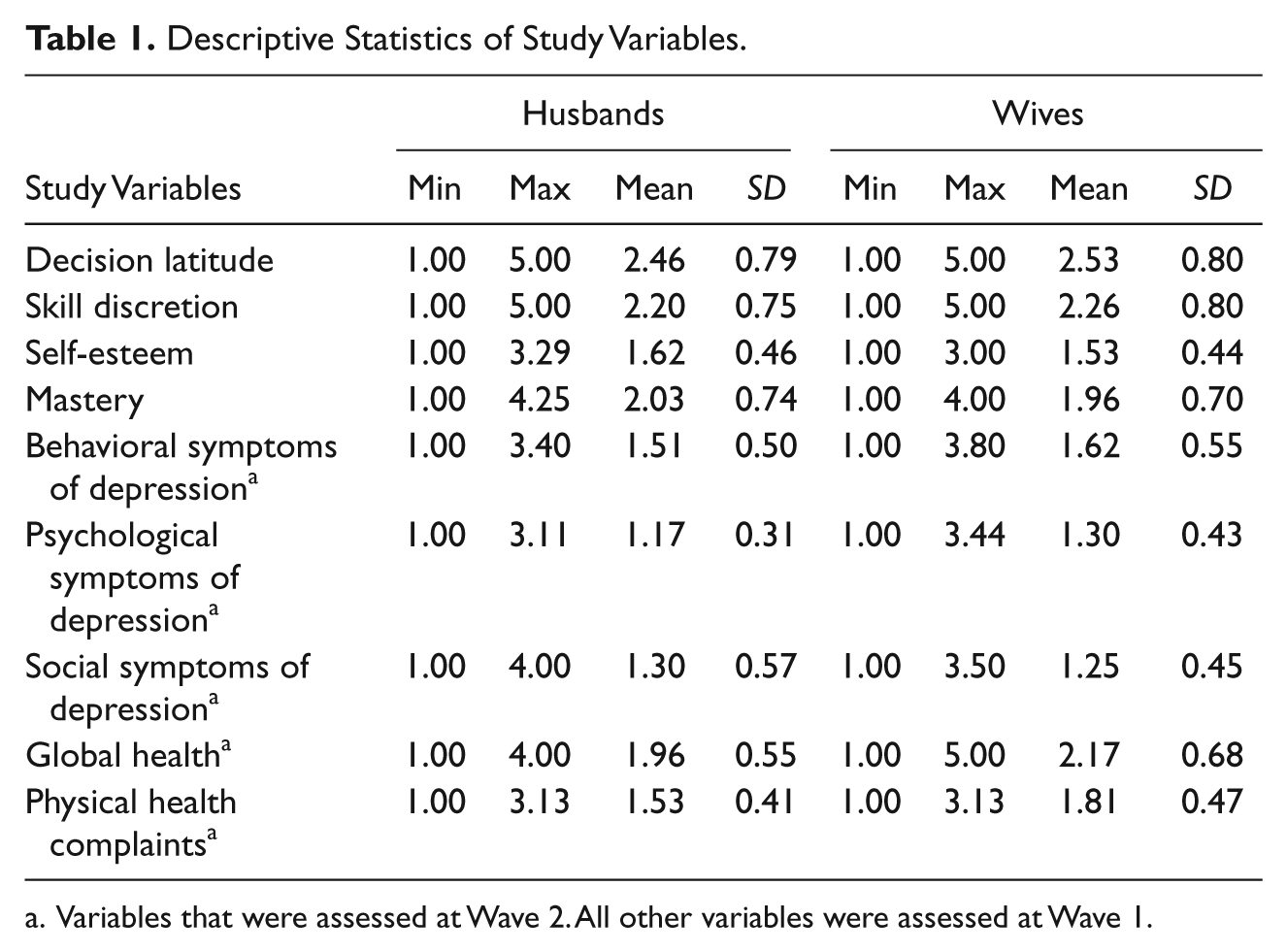
Variables that were assessed at Wave 2. All other variables were assessed at Wave 1.
Zero-Order Correlations Among Latent Constructs.
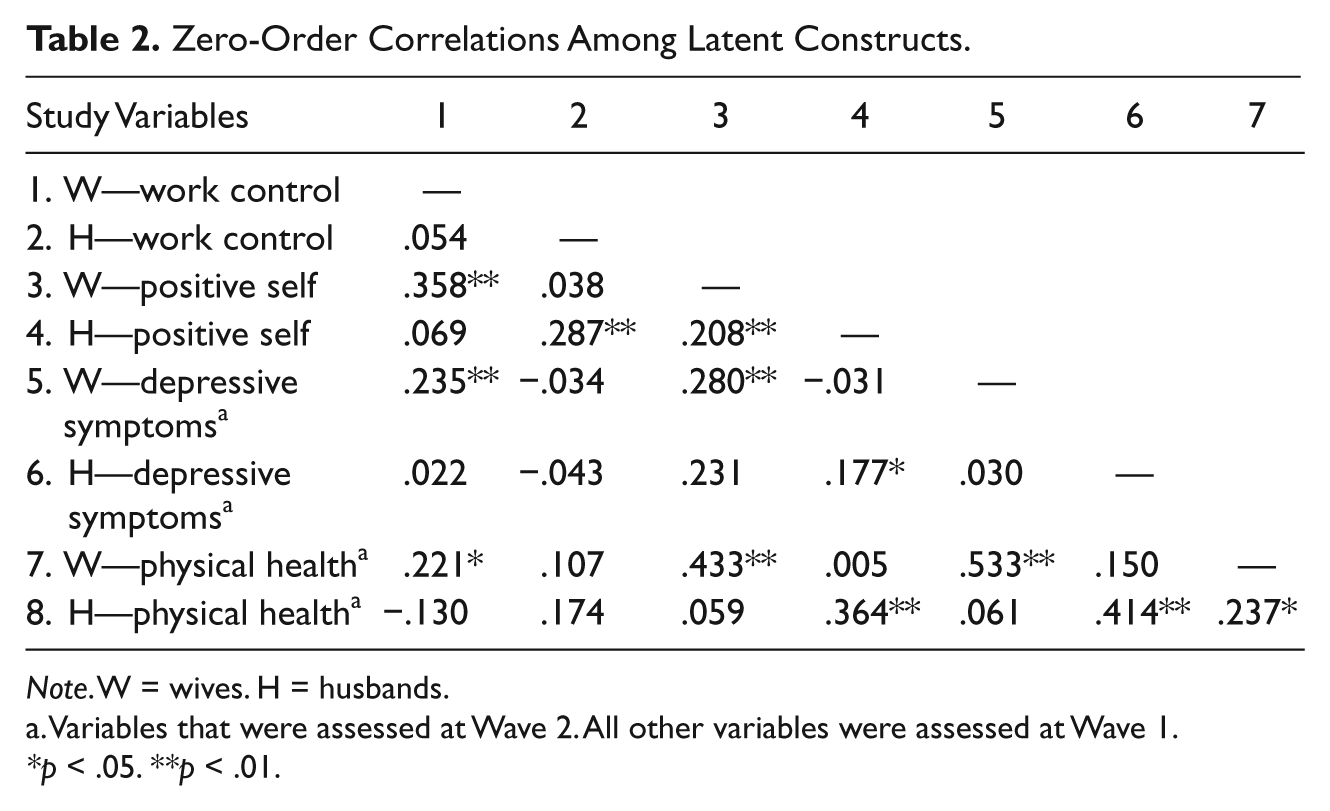
Note. W = wives. H = husbands.
Variables that were assessed at Wave 2. All other variables were assessed at Wave 1.
p < .05. **p < .01.
Although correlations among the observed variables are not shown, skill discretion and work latitude were correlated for wives (r = .477, p < .01) and husbands (r = .562, p < .01), and self-esteem and mastery, the two indicators of positive self, were significantly correlated for wives (r = .545, p < .01) and husbands (r = .568, p < .01). The two self-assessed indicators of physical health (global health assessment and physical health complaints) and the three indicators of depressive symptoms (behavioral, psychological, and social symptoms) were also significantly correlated with each other (p < .01).
Testing the Hypothesized Structural Equation Model
Figure 2 displays the structural equation model examining the influence of work control at Wave 1 on husbands’ and wives’ depressive symptoms and physical health 1 year later. Wives’ control over work was directly related to wives’ depressive symptoms and physical health (β = .237, p < .01 and β = .216, p < .05, respectively). Husbands’ control over work was not directly related to husbands’ depressive symptoms (β = −.047, p > .05) and was only marginally related to husbands’ physical health (β = .181, p < .10). Cross-spouse effects between work control and health outcomes were not statistically significant.
Next, both work control and positive self at Wave 1 were included in the model as predictors of depressive symptoms and physical health 1 year later (see Figure 3). With the inclusion of positive self, work control was no longer significantly related to mental or physical health for either spouse. Husbands’ control over work significantly predicted husbands’ positive self (β = .284, p < .01), and wives’ control over work significantly predicted wives’ positive self (β = .352, p < .01). Husbands’ and wives’ positive selves were, in turn, significant predictors of their own level of depressive symptoms (βhusband = .207, p < .01 and βwife = .242, p < .01) and physical health (βhusband = .354, p < .01 and βwife = .411, p < .01). There were no significant transactional effects between husbands’ and wives’ positive selves and their partners’ health outcomes. Husbands’ and wives’ work control, depressive symptoms, and physical health were not associated with each other. Husbands’ positive self was moderately correlated with wives’ positive self (r = .206, p < .01). Cross-spouse effects between work control, positive self, and health outcomes were not statistically significant. Overall, this model fit the data well (CFI = .94, RMSEA < .04, and χ2/df ratio of 1.60).
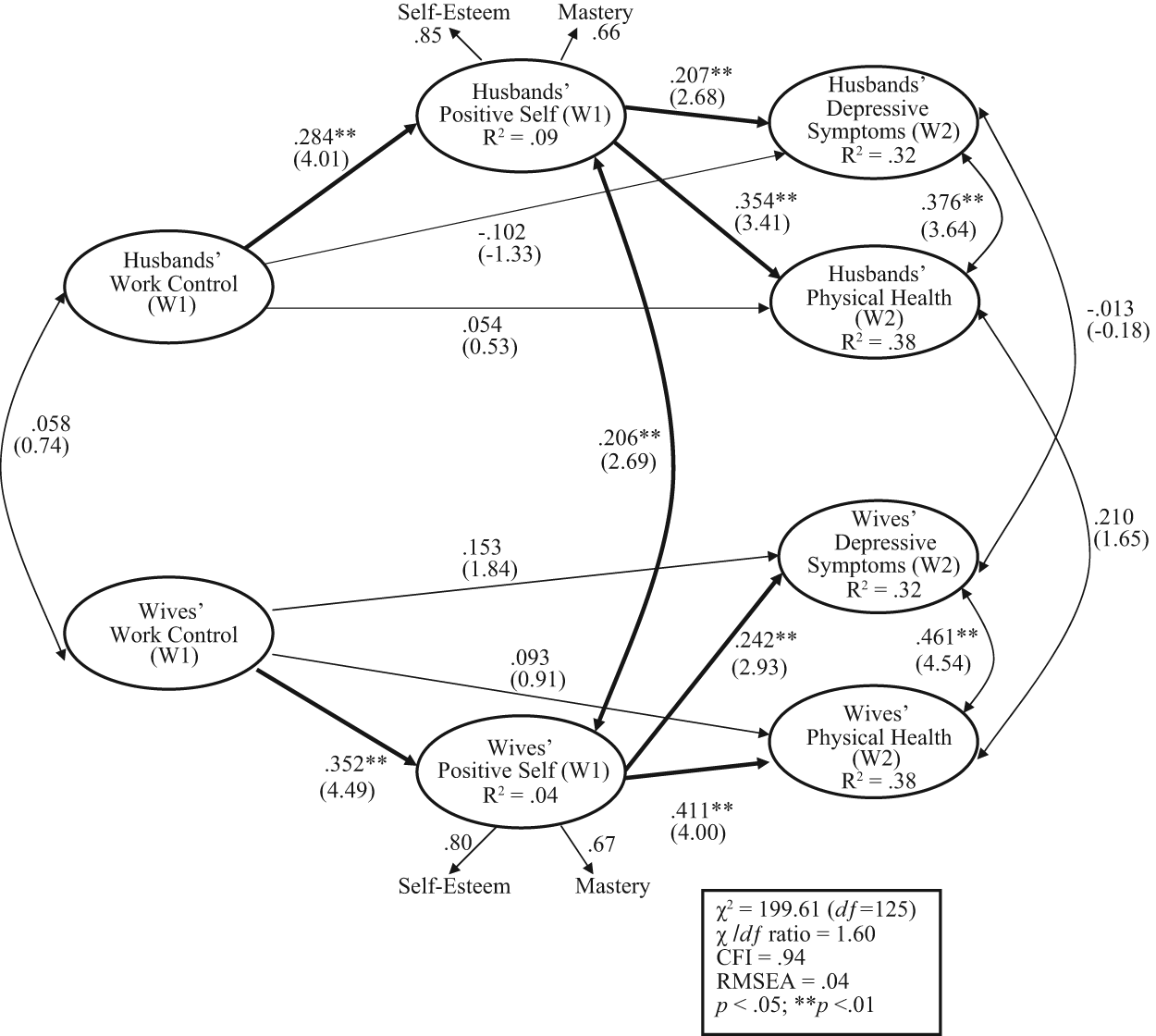
The mediating effect of positive self on the influence of work control on husbands’ and wives’ depressive symptoms and physical health.
According to Baron and Kenny’s (1986) steps for determining mediation, these results showed that positive self fully mediated the direct association between work control and health outcomes (including depressive symptoms and physical health) for wives but not for husbands. Based on Baron and Kenny’s (1986) prerequisites, mediation was not present for husbands because in the model examining only the direct effect of husbands’ work control on husbands’ depressive symptoms and physical health, these paths were either not significant or only marginally significant (t values were marginally significant for physical health and nonsignificant for depressive symptoms). However, recent research has demonstrated flaws in Baron and Kenny’s (1986) method (Zhao, Lynch, & Chen, 2010). In reference to the current findings, Hayes (2009) has suggested that Baron and Kenny’s (1986) causal steps approach overemphasizes the importance of the X–Y test (i.e., work control predicting health in our study) for several reasons. First, this step has the least power to detect significant differences, thereby increasing the chance of not finding existing statistically significant differences (c.f. Fritz & MacKinnon, 2007). Second, placing excessive importance on the test of the direct effect ignores the very indirect effect that the research is attempting to clarify (Hayes, 2009).
Thus, on further review, the results showed that positive self mediates the association between work control and depressive symptoms and physical health for both sexes, although traditional complementary mediation was present for wives and indirect-only mediation, where a mediated effect (a × b) is present but a direct effect is not, was detected for husbands (Zhao et al., 2010). Furthermore, the significance of the indirect paths between work control and depressive symptoms and physical health were significant for husbands and wives (p < .05, Sobel test). That is, for both genders, work control is indirectly associated with depressive symptoms and physical health.
Using a dyadic model allowed us to employ equality constraint tests (K. A. S. Wickrama et al., 1995) to determine if the strength of paths differed for husbands and wives. These tests are conducted by constraining the path of interest to be equal for husbands and wives and comparing model fit between this alternative model and the original model. Several notable paths were significantly different for husbands and wives, including the paths between work control and positive self, Δχ2(1) = 116.79, positive self and depressive symptoms, Δχ2(1) = 146.09, and positive self and physical health, Δχ2(1) = 106.49. The equality constraint test showed that the association between wives’ work control and wives’ sense of positive self was stronger than the association between husbands’ work control and husbands’ positive self. Likewise, wives’ positive self exerted a stronger influence on wives’ health outcomes than the influence of husbands’ positive self on husbands’ health outcomes.
The model failed to converge when each partner’s age, education, and income were included as controls. Therefore, we tested models with controls for depressive symptoms and physical health separately to determine if the inclusion of controls altered the results. These models provided essentially the same results suggesting that the exclusion of control variables does not appear to limit the validity of these results.
Analyses examining the moderating role of positive self (Research Question 3) revealed the same pattern of results for husbands and wives with high and low positive self (not shown). Thus, for dual-earner African American couples, positive self does not appear to moderate the influence of work control on physical and mental health outcomes.
Discussion
This study investigated whether African American husbands’ and wives’ work control was longitudinally associated with depressive symptoms and physical health directly and indirectly through their sense of positive self using structural equation models. The dyadic model allowed us to account for the interdependence between husbands and wives by including associations between husbands’ and wives’ work control, positive self, depressive symptoms, and physical health as well as transactional (cross-spouse) associations between (a) work control and health outcomes and (b) positive self and health outcomes.
In general, the results supported the stress-illness perspective (Pearlin et al., 2005; Pearlin & Skaff, 1996) and work socialization perspective (Karasek & Theorell, 1990). The results call attention to the observed social epidemiological pathway leading African Americans to experience relatively poor health and the role of work experiences and personal resources in shaping African American husbands’ and wives’ mental and physical health outcomes. The results provide evidence that work control is directly associated with wives’, but not husbands’, depressive symptoms and physical health. However, for both husbands and wives, work control is indirectly associated with depressive symptoms and physical health through the influence of work control on individuals’ positive self. These basic mediation findings are similar to existing research. For instance, Xanthopoulou et al. (2007) found that personal resources (i.e., self-efficacy, organizational-based self-esteem, and optimism) mediate the relationship between job characteristics and individual well-being. However, comparisons between these findings and previous research are limited because of the lack of studies examining African American health outcomes.
Interestingly, our results revealed no significant cross-spouse influences between husbands and wives, and the only significant correlation between husbands and wives was found for positive self. The lack of dyadic influence indicates that these processes occur independently for African American husbands and wives. The nonsignificant contemporaneous association between husbands’ and wives’ depressive symptoms is particularly notable because existing research with other minority ethnicities, Czech and Argentinean couples, has found husbands’ and wives’ depressive symptoms to be highly correlated (Falconier, 2010; Lorenz & Hraba, 2004). This suggests that, on average, unlike couples from other ethnicities, depressive symptoms are less likely to be interdependent for African American couples. Pinderhughes (2002) argues that the ties between African American spouses are generally weaker than the ties between blood or adopted kin. Thus, rather than examining cross-spouse interdependence, transactional effects may be more likely between other family members (e.g., parent/child or siblings) for African Americans. The stronger ties between African Americans and their families of origin (including extended family) than African American marital spouses may be because of the culture’s tendency to embrace a strong sense of familial obligation leading some to speculate that this familial support may come at the cost of reduced marital well-being and closeness (Bryant et al., 2010). Thus, individuals may be more invested (e.g., finances and time) and emotionally connected to their family of origin than their marital partner, which may create distance within the marital relationship and, consequently, make African Americans’ family of origin the primary source of stress crossover. Future research should examine these cross-spouse associations for other life domains (e.g., health behaviors and other dimensions of work or life stress).
Additionally, the stress-illness perspective (Pearlin et al., 2005; Pearlin & Skaff, 1996) contends that personal resources can also operate as moderators in the relationship between stressful experiences and health outcomes. Our results did not support the moderating hypotheses, suggesting that work control influences African Americans’ health outcomes regardless of their level of personal resources. However, there may be a threshold level of personal resources that is necessary for this buffering effect, and perhaps our sample of African American dual-earner couples did not have the high levels of personal resources necessary for this to occur. It should also be noted that our use of mean splits to test for moderation involved analyzing the baseline model after dividing the sample into two groups (high and low). Although no cases are lost, simply divided, this does create a reduced sample, which could have lacked the necessary statistical power.
This research suggests that the work role and personal resources are highly salient among African American couples. Moreover, personal resources may be particularly salient for African Americans couples, because it is strongly tied to their ethnic identity (E. P. Smith et al., 1999). We hypothesized that work control and personal resources, or lack thereof, may have a particularly strong impact on African Americans’ health outcomes because African Americans are disproportionately exposed to adverse conditions, including occupations associated with low control and limited resources (R. A. Smith & Elliott, 2002), and the detrimental influences of these adverse conditions are more pronounced among individuals in the lower levels of the SES hierarchy (Marmot, 1989). Furthermore, although existing research using Caucasian samples has concluded work control is more salient for husbands than their wives (K. A. S. Wickrama et al., 1995; K. A. S. Wickrama et al., 2005), we expected that African American wives would be as responsive to their work conditions as their husbands because African American wives are more likely than Caucasian wives to be employed outside the home and provide a larger proportion of the family income (Mincy & Pouncy, 2003). Our results were consistent with this hypothesis. In fact, the work role was more salient for African American wives than their husbands. The equality constraint tests revealed that, on average, the indirect effects of work control on mental and physical health outcomes were stronger for wives than husbands. This is also seen in the weaker correlations between work control and depressive symptoms and work control and physical health among husbands relative to wives.
Perhaps this gender difference is related to the educational discrepancy between African American men and women. Like the national average, the mean level of education in our sample was higher for African American women than African American men (U.S. Census Bureau, 2010), yet a paired-samples t test (not shown) indicated no gender difference in work control within the current sample. Although work control is generally thought to be greater for those with advanced degrees because of the nature of the jobs that they are likely to hold, these findings suggest that African American women with advanced educational attainment may not have greater work control than those with little formal education. Thus, future research should examine if educational attainment moderates the influence of work control on mental and physical health outcomes, particularly for African American women as they are subject to both racism and sexism, which may increase their risk of workplace discrimination and subsequent lack of work control even when holding advanced degrees (Cole, 2009).
In addition to elucidating a mechanism explaining the connection between work control and health outcomes, several methodological aspects of this study contribute to existing literature. First, the use of dyadic data allowed us to account for the associations between husbands’ and wives’ responses. That is, correlations were included between husbands’ and wives’ variables and transactional paths between positive self and both health outcomes were included to account for interdependency between spouses. Second, all concepts (i.e., work control, personal resources, depressive symptoms, and physical health) were measured as latent constructs, which often provide more accurate path estimates because latent constructs take into consideration the measurement error that is common in observed indicator variables. Third, the two personal resources (i.e., mastery and self-esteem) examined as indicators of positive self were chosen based on existing theoretical and empirical work that has shown these resources contain a common core self-evaluation component (Hatton et al., 2008; Judge, 2009). Thus, this research provides more evidence supporting the validity of this concept. Fourth, physical and mental health was examined simultaneously within the same model to eliminate shared variance, which can overestimate the amount of variance explained for each construct. Finally, using a sample of African American couples permitted the evaluation of constructs within a racial group that is often poorly represented in existing datasets. This is particularly important because, as previously discussed, there is reason to believe the association studied (i.e., work control and health) may be stronger for African Americans than Caucasians.
As with any study, there are limitations to this study that should be noted. First, constructs were defined using individual self-reports. Because previous research has demonstrated the validity of self-assessed health outcomes (Ferraro & Farmer, 1999) and personal resources are primarily introspective, the use of self-report data is primarily a concern for the variable work control. Future studies using more objective measures of work control may arrive at different conclusions. Another limitation is the marginal or moderate internal consistency values of some of the measures (e.g., husbands’ behavioral symptoms of depression and physical health complaints) used in the current study. However, some research suggests that, when using latent constructs, associations between constructs with low internal consistency remain accurate (Little, Lindenberger, & Nesselroade, 1999). Furthermore, although the items used to assess physical complaints were not strongly associated with each other, as indicated by Cronbach’s alpha, we believe the measure assesses the accumulation of complaints, which may reflect the severity of health condition. It is also important to note that although this research is longitudinal because we assessed health outcomes 1 year after our measurement of work control and positive self, we were not able to control for health status at Wave 1 because of the high stability between the two measurement points with only 1 year in between measurements. Future studies controlling for previous health status can rule out this possibility. Of course, the restricted scope of the sample (i.e., African American newly married couples) limits the generalizability of these findings. Although the sample was fairly diverse in age and, thus, likely includes individuals at a variety of life course stages (e.g., various parental, work, and family roles), newly married couples may report low levels of depression because of the “honeymoon period,” thereby creating a potential ceiling effect of positive emotions and making associations between work control and depressive symptoms and personal resources and depressive symptoms difficult to detect with statistical analyses. Or newly married couples may have less cross-spouse associations than other couples who have a longer history of “linked lives” together (Elder & Giele, 2009). Future studies may also improve on these findings by analyzing racial discrimination and work control simultaneously as there is some evidence that jobs with low work control may coexist with more institutional discrimination within the workplace (Hughes & Dodge, 1997).
Despite these limitations, the findings from this study contribute important information. Whereas existing research has examined fragments of this model (e.g., the influence of work control on personal resources), our study is novel in its analysis of a model combining several previously tested associations using an African American sample, a racial group that is largely absent from existing literature in this area. By examining depressive symptoms and physical health within the same model, our study provides important new evidence concerning the unique influence of work control and positive self on each of these health outcomes after accounting for the shared variance between these constructs. Furthermore, this study illustrates the value of examining individual personal resources as observed indicators of a larger core construct of self-evaluation, or positive self. These findings also illustrate the value of work organization policies aimed at increasing workers’ decision latitude and sense of positive self. For instance, self-enhancing programs that provide a variety of instrumental and immaterial rewards such as verbal recognition may facilitate workers’ positive self, which our research suggests may have a positive influence on health outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Grant R01-HD050045-05 from the National Institute of Child Health and Human Development (Chalandra M. Bryant, Principal Investigator).