
Abstract
Using data generated from the Global Risk Assessment Device, mental health and disrupted family processes were examined in a sample of 166 court-involved youth being raised by grandparents. Race and gender mean differences were found with regard to both mental health symptoms and disrupted family processes. Specifically, Caucasian male adolescents reported higher mental health symptoms and disrupted family processes than African American males. Also, females in the sample generally reported higher disrupted family processes than males, with African American females reporting significantly higher average disrupted family processes than African American males. Despite mean differences associated with gender and race, when entered as predictors, neither main effects nor interactions of gender or race were related to mental health symptoms. Disrupted family processes were predictive of higher mental health symptoms. Family-targeted interventions with court-involved youth being raised by grandparents would likely benefit the mental health of these adolescents.
Parenting grandchildren is a unique role that has become more common in today’s society. Approximately 5.8 million grandparents in the United States were reported to be residing with their grandchildren in 2000 (U.S. Bureau of the Census, 2000), comprising a 30% increase since 1990 (Hayslip & Kaminski, 2005a). Research related to custodial grandparenting has focused primarily on grandparental well-being, suggesting mental, physical, financial, and legal strain resulting from the custodial role (Hayslip & Kaminski, 2005a; Thomas, Sperry, & Yarbrough, 2000). Fewer studies have focused on the needs of grandchildren being raised by grandparents.
Among research that has focused on the grandchildren, risks are often identified. First, the circumstances that lead children to be raised by grandparents are often traumatic in nature, and involve the children’s parents, such as drug and alcohol use, divorce, death, HIV/AIDS, incarceration, unemployment, military deployment, and teen pregnancy (Breslin, 1992; Bunch, Eastman, & Moore, 2007; Burnette, 1997; Burnette & Kropf, 2003; Fuller-Thomson & Minkler, 2000; Grinstead, Leder, Jensen, & Bond, 2003, Ladner & Gourdine, l984; Ruiz, 2000; Pinson-Milburn et al., 1996). Despite these challenges, the children who go into grandparent custody may find themselves in more favorable circumstances than they were in prior to living with grandparents (Bell & Garner, 1996). Second, some research has indicated that children being raised by grandparents may experience more behavioral and emotional problems than their peers (e.g., Edwards, 2006). Thus, although grandchildren often benefit from living with their grandparents, they also often face great challenges.
Juvenile court involvement constitutes an additional risk for children being raised by grandparents. Involvement in the juvenile court system is an indicator of unlawful behavior. In addition, juvenile delinquent populations experience high rates of externalizing problem behaviors (Dekovic, Buist, & Reitz, 2004; Leadbeater, Kuperminc, Blatt, & Hertzog, 1999), family and other interpersonal challenges (Simons, Chao, Conger, & Elder, 2001), and serious emotional disorders (Lyons, Baerger, Quigley, & Griffin, 2001). Little is known about youth involved in the juvenile justice system that are being raised by their grandparents. Furthermore, research has indicated that approximately 45% of children of incarcerated mothers and 15% of children of incarcerated fathers live with grandparents (Glaze & Maruschak, 2008), and that these youth have increased risk for delinquent behavior (Tasca, Rodriguez, & Zatz, 2011).
Youth involved in the juvenile justice system that are being raised by grandparents constitute an at-risk group that has received relatively little attention by researchers. As such, the first objective of this study is to describe the mental health of 166 court-involved youth that are being raised by grandparents. The second objective is to explore how mental health of youth being raised by grandparents differs based on gender and race. Because the grandparent-headed family environment is primary to the youth’s mental health, the third objective is to examine links between disrupted family processes and mental health. Specifically, we explore how disrupted family processes predict the mental health of these youth. We also consider how gender and race may moderate this link.
Out of all the theories recently reviewed by Gavazzi (2011), as applied to families containing adolescent members, the link between disrupted family processes and mental health may be illuminated best by facets of attachment theory. According to Bowlby (1973), consistent nurturance from a primary caregiver leads to a “secure” internal model of attachment that becomes instrumental in how individuals cope with stress over time. Less well-adjusted individuals are represented by three other internal working models (ambivalent/preoccupied, avoidant/dismissing, and disorganized/unresolved attached styles) that are thought to be the product of disruptions in the relationship with a primary caregiver, all of which give rise to the possibility of various internalizing and externalizing disorders in adolescents (Liddle & Schwartz, 2002). In essence, secure attachments represent mutually trusting relationships between adolescents and their caregivers as certain developmental demands are met, including especially the need to balance autonomy and relatedness claims (Allen & Hauser, 1996; Cobb, 1996). In the current study, disrupted family processes represent a manifestation of poor attachment quality between court-involved youth and their grandparents. As such, we link these family processes with individual mental health.
Grandchildren Being Raised by Grandparents
Research addressing the lives of youth being raised by grandparents can be grouped into three main categories: (a) grandchild mental and emotional health, (b) gender of the child, and (c) race of the child. Regarding mental health challenges, several studies examine costs to grandparents that are raising grandchildren that have behavioral, mental, emotional, or neurological problems (Bowers & Meyers, 1999; Harrison, Richman, & Vittimberga, 2000; Sands & Goldberg-Glen, 1998), suggesting that the grandchildren often face mental health challenges. Other research indicates that the grandchildren show emotional and behavioral problems, often in school settings (Edwards, 2006; Scarcella, Ehrle, & Geen, 2003). These mental and emotional challenges could be due to the loss of attachment bonds to parents and the restructuring of emotional connections with grandparents (Poehlmann, 2003). These attachment processes are complicated by the ambiguous nature of living with grandparents, as grandchildren are often unsure of long-term living arrangements. For example, in the situation of parental incarceration, children may be unsure of their parent’s future and the future they will have together. Mental and emotional challenges may also be because of having experienced abuse, neglect, or other traumatic experiences (Smith & Dannison, 2001). Traumatic experiences have been found to affect adolescent health (Cheever & Hardin, 1999), as well as individual physical, mental, and social development (Davis & Siegel, 2000).
The effects of trauma can be influenced by the parent–child relationship. Montgomery and Foldspang (2001) found that children exposed to war-related trauma had more sleep disturbances when they did not have both parents available for support. Clinical case studies have suggested that attachment of children to parents or other adult figures are important in recovery from trauma (Mishne, 2001; Stubenbort, Greeno, Mannarino, & Cohen, 2002). Specifically, Mishne (2001) indicated from her study that the nature of the parent–child relationship was the strongest predictor of adjustment to trauma. Similarly, Stubenbort et al. (2002) linked higher attachment quality in children to better coping with trauma. Given the mental and emotional challenges, as well as the disrupted family processes that youth being raised by grandparents often face, special attention to this group seems warranted.
Despite evidence that grandchildren being raised by grandparents often face mental and emotional challenges, other research indicates more similarities than differences between children raised under various family structures (Pinson-Milburn, Fabian, Schlossberg, & Pyle, 1996). For example, in a study of 82 children referred to outpatient therapy, Harrison et al. (2000) examined parental stress and child behavior across two-parent, single-parent, and grandparent-headed households. Their findings suggested that average parental stress scores for grandparent-headed households were actually lower than those for single-parent households and not different from those for two-parent households. Also, although children from all three groups showed clinical levels of child behavior problems, there were no differences across groups. In a nonclinical sample derived from the National Health Interview Survey, Solomon and Marx (1995) reported that children from two biological-parent households were more successful in school than those in grandparent-headed households, yet those in single-parent households were more likely to misbehave in school, less likely to be obedient, and were no more successful than children in grandparent-headed households. One likely reason that children in grandparent-headed households compare well with peers in other family structures is that they benefit from living with their grandparents. Indeed, living with grandparents may provide a buffer to the stresses experienced by the grandchildren (Bell & Garner, 1996).
Gender
Research attending to gender differences of children being raised by grandparents has focused on prevalence rates and rates of behavior problems. One study suggested that boys are more likely than girls to be raised by grandparents (Shore & Hayslip, 1994). However, no nationally representative studies have examined this question. Regardless of prevalence rates, boys and girls likely have different experiences in grandparent custody. There is some evidence that boys experience more behavior problems than girls being raised by grandparents. Solomon and Marx (1995) suggested that girls being raised by grandparents are “seven times more likely to behave [appropriately] with teachers” than boys (p. 391). They also indicated that boys being raised by grandparents are twice as likely to be susceptible to illness. Consistent with these findings, Shore and Hayslip (1994) indicated that raising a granddaughter, as opposed to a grandson, was associated with “greater satisfaction in grandparenting . . ., better health, more positive relationships with a grandchild, greater well-being, and less help seeking” (p. 200). In summary, it appears that in general, raising grandsons may present more difficulties than raising granddaughters.
In contrast, the current study is focused on grandchildren that are involved in the court system. Young women involved in the court system likely have different life experiences than their female counterparts outside of the court system. For example, Chamberlain and Moore (2002) found that in a court-involved female sample (mean age = 15 years, N = 42), the girls had an average of 14 parental transitions during their lifetime. This equates to experiencing approximately one parental transition for every year of their lives. Furthermore, female juvenile offenders likely experience high rates of trauma (Brosky & Lally, 2004; Cauffman, Feldman, Waterman, & Steiner, 1998). Male juvenile offenders also often have a history of trauma exposure, PTSD symptoms, and family dysfunction (Burton, Foy, Bwanausi, Johnson, & Moore, 2006). Still, males and females likely experience different types of trauma and family problems. For example, Crimmins, Cleary, Brownstein, Spunt, and Warley (2000) found that male juvenile offenders had more often experienced accidents requiring hospitalization, whereas female youth had more often experienced or witnessed sexual trauma. Thus, although raising granddaughters, in general, may be less problematic than raising a grandson, male and female grandchildren involved in the court system may experience unique challenges.
Race/Ethnicity
Cultural trends and practices influence custodial grandparent/grandchild experiences (Goodman & Silverstein, 2002). For example, African American grandparents are more likely than other groups in the United States to provide primary care for grandchildren (Burton & Dilworth-Anderson, 1991; Hayslip & Kaminski, 2005b; U.S. Bureau of the Census, 2000). However, in their study of child outcomes among a sample of children being raised by grandparents, Solomon and Marx (1995) reported that race did not independently predict various school and health indicators, including being obedient in school, behaving with teachers, not repeating a grade, never being expelled, general health, not having asthma, not having enuresis, and having no accidents or injuries. In the United States, Hispanic grandparents provide custodial care for their grandchildren more often than Caucasian grandparents (Goodman & Silverstein, 2002). However, Hispanic families also coreside with multiple generations more often, leading to coparental care for grandchildren (Goodman & Silverstein, 2002). Each of these trends suggests higher prevalence rates of grandparental care by African American and Hispanic grandparents. Because of the increased prevalence of custodial grandparents in these cultures, the meaning that grandparents give to the custodial grandparent role may be considered as normative and as source of life satisfaction (Goodman & Rao, 2007).
Family Processes of Court-Involved Youth
A growing body of evidence has addressed both culturally sensitive and gender-specific issues in the lives of court-involved youth (Gavazzi, Yarcheck, & Chesney-Lind, 2006; Gavazzi, Yarcheck, & Lim, 2005). For example, Gavazzi (2006) explored race and gender differences in disrupted family processes using a sample of court-involved youth. Findings from that study indicated that African American females had the highest levels of disrupted family processes, followed by Caucasian females. Both Caucasian males and African American males displayed equally lower scores than both of the female groups. In that same study, male and female prior offense levels were similar when they experienced greater disrupted family processes whereas male prior offense levels were much higher than female levels among those with fewer disrupted family processes.
A second study conducted by Gavazzi, Bostic, Lim, and Yarcheck (2008) extended this literature by examining factors related to race, gender, family factors, and mental health issues in a sample of African American and Caucasian males and females coming to the attention of five different juvenile courts. In addition to reporting significant race by gender interaction effects found in the multivariate analyses on Global Risk Assessment Device (GRAD) domains associated with family processes and mental health, the results of multiple group structural equation modeling procedures generated support for the hypothesis that family environment mediates the relationship between gender and mental health problems. However, this model displayed goodness of fit only in the sample of African American youth, suggesting a strong mediating component of family environment among African American families only.
The Present Study
The present study explores the mental health and disrupted family processes of court-involved youth that are being raised by their grandparents. Although literature addresses the mental and emotional well-being of children being raised by their grandparents, involvement in the juvenile court system likely indicates greater mental distress. Thus, our first objective is to describe the mental health of court-involved youth living in grandparent-headed households. The second objective is to explore the associations of gender and race in relation to mental health and disrupted family processes of court-involved youth being raised by grandparents. As mentioned previously, research suggests higher rates of behavior problems among males, yet females involved in the juvenile court system may have more challenges than those involved in prior research. As such, gender differences are exploratory. As being raised by grandparents is more normative among African American youth, it is expected that disrupted family processes are lower for this group than among Caucasian youth in the sample. The third objective of this study was to explore how disrupted family processes among court-involved youth being raised by grandparents are linked to their mental health, and how this link may be moderated by gender and race. Findings from the literature suggest that positive family processes are linked to improved mental health treatment outcomes as well as recovery from trauma. As such, it was expected in the current study that disrupted family processes will be linked with poorer mental health. Moderating effects by gender and race are exploratory, as the literature does not point to family processes being more important for males or females or for different race groups.
Method
Participants
Data were collected from 166 youth between the ages of 13 and 17 years (M = 15.01 years, SD = 1.3) residing with grandparents who were assessed in five Midwestern county juvenile courts. Sixty-nine percent of the sample was Caucasian and 31% African American. There were 103 males (62%) and 63 females (38%). Table 1 includes descriptive information about the sample as well as interitem correlations between study variables.
Descriptive Statistics and Correlations Among the Variables of Gender, Race, Mental Health Domain, and Disrupted Family Processes (N = 188).
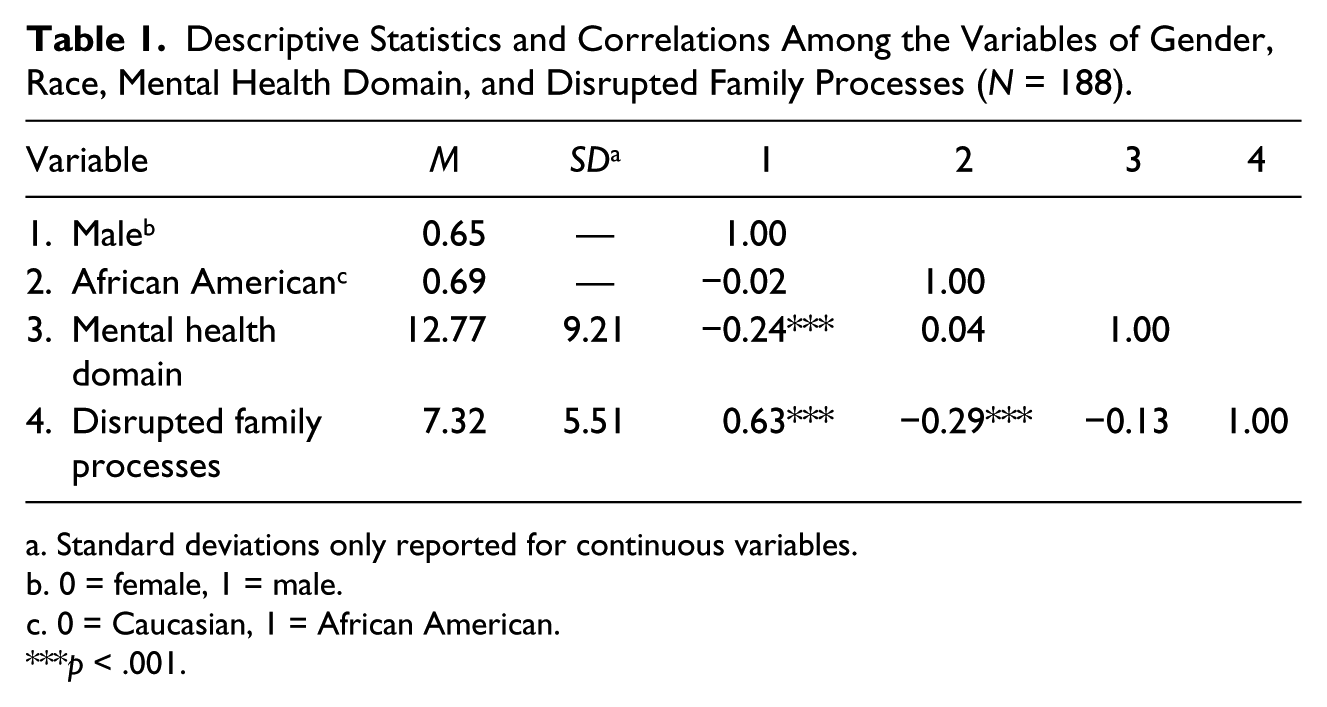
Standard deviations only reported for continuous variables.
0 = female, 1 = male.
0 = Caucasian, 1 = African American.
p < .001.
Measure
The data collection instrument used was the 132-item GRAD Version 1.0 (Gavazzi, Slade, et al., 2003), an Internet-based measure that assesses potential threats to the numerous developmental needs of adolescents who come into contact with the juvenile justice system. A number of studies have generated solid psychometric evidence regarding this assessment tool, including a solid factor structure and high internal reliability coefficients (Gavazzi, Slade, et al., 2003). Additional studies (Gavazzi & Lim, 2003) have generated concurrent validity evidence with other well-established measures of substance use (Youth Behavior Survey Questionnaire; Brener et al., 2002), mental health (Brief Symptom Inventory; Derogatis, 1993), and family environment risks and needs (Family Events Checklist; Patterson, Reid, & Dishion, 1992) and predictive validity evidence of the GRAD in terms of this tool’s use in referring youth to the most appropriate level of care (Gavazzi, Lim, Yarcheck, & Eyre, 2003). Also, the GRAD has been used to demonstrate both gender-specific and race/ethnicity differences (Gavazzi, 2006; Gavazzi et al., 2006; Gavazzi et al., 2005).
The GRAD contains 11 domains of risk/needs: prior offenses, family/parenting issues, deviant peer relationships, substance abuse, traumatic events, mental health issues, psychopathy, sexual activity and other health-related risks, leisure activities, accountability, and education/work issues. The average time that it takes to complete the GRAD is about 25 minutes. Respondents are asked to respond to the items by indicating on a scale of 0 to 2 (where 0 indicates no/never, 1 indicates yes/a couple of times, and 2 indicates yes/a lot) how much each item applies to their life. Item scores are totaled to compute a risk score for each domain. For present purposes, the Family/Parenting domain and the Mental Health domains were employed. Previous studies have indicated that each of these domains have high reliabilities, with coefficient alphas reported at .88 and .83, respectively (Gavazzi, Bostic, et al., 2008; Gavazzi, Lim, Yarcheck, Bostic, & Scheer, 2008).
The Family/Parenting domain contains 17 items that focus attention on disrupted family processes, or those activities within the family that impede member well-being. Examples of items in this domain include “How often do you get into fights with adults who live in your home” and “How much of the time do the adults who live with you NOT know where you are?” with response options of 0 (coded as no/never), 1 (coded as yes/a couple of times), and 2 (coded as yes/often). This scale ranges from 0 to 34, with higher scores indicating greater family disruption. In the current sample, the average disrupted family processes score was 7.32 (SD = 5.51), with a Cronbach’s reliability coefficient alpha of .79. This scale is referred to as “disrupted family processes” in the current study.
The Mental Health domain contains 26 items associated with the experience of mental health issues. This scale includes items that reflect both internalizing and externalizing behavior, as well as symptoms of attention deficit hyperactivity disorder. Examples of items include “Do you ever feel sad, moody, blue or depressed?” and “Do you ever destroy things that belong to you when you get angry?” with response options of 0 (coded as no/never), 1 (coded as yes/a couple of times), and 2 (coded as yes/often). This scale ranges from 0 to 52, with higher scores indicating higher levels of mental health symptoms. In the current sample, the average mental health score was 12.77 (SD = 9.21), with a Cronbach’s reliability coefficient alpha of .90.
Procedure
The analyses were conducted on data collected by juvenile justice professionals from five Ohio counties who employed the GRAD as part of their standard and usual assessment procedure. When the administrative group of a juvenile court decides to employ the GRAD as part of their assessment practice, 6 hours of training are provided to all the juvenile justice professionals who will use the assessment tool in their daily work with youth. All such training is completed prior to the professional’s participation in the data collection process. A total of 38 professionals contributed assessments to the database employed in this study. Each of these professionals had ongoing telephone contact with their GRAD trainers and face-to-face consultation with their administrative officers as part of a quality control effort designed to ensure competence of administration. Although the GRAD was developed to capture data from three perspectives (youth, adults, and professionals), only the information gleaned directly from the court-involved youth were used in the present study.
Results
To address our first two research objectives, mental health symptoms and disrupted family processes of the grandchildren in the current sample are described in Tables 1 and 2. As seen in Table 1, the average mental health score was around 13, and the average disrupted family processes score was around 7. Associations between gender, race, disrupted family processes, and mental health symptoms were also explored through correlations (see Table 1). Findings indicated that being male was associated with lower mental health symptom scores and with higher disrupted family process scores. Being African American was associated with lower disrupted family process scores. As seen in Table 2, Caucasian male respondents had higher mental health symptom scores and higher disrupted family process scores than their African American male counterparts. African American females in the sample had similar scores as Caucasian females on both measures. Means were also compared within race but across gender (see the note in Table 2). Among these comparisons, only disrupted family process means were different between African American females and males, with females having higher disrupted family process scores.
Descriptive Statistics and Mean Difference Tests of Mental Health Domain and Disrupted Family Processes by Race and Gender (N = 188).
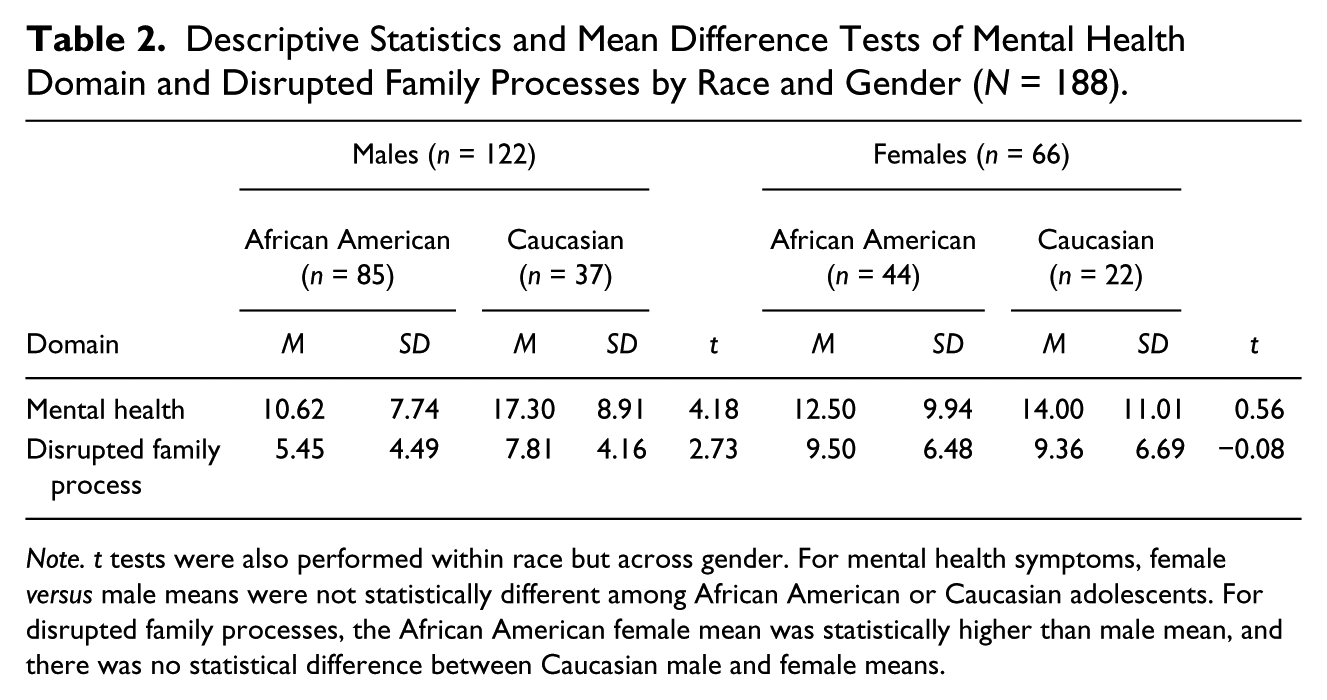
Note. t tests were also performed within race but across gender. For mental health symptoms, female versus male means were not statistically different among African American or Caucasian adolescents. For disrupted family processes, the African American female mean was statistically higher than male mean, and there was no statistical difference between Caucasian male and female means.
To address our third research objective, we used regression analyses to further explore how gender, race, and disrupted family processes were predictive of mental health symptoms as an outcome. Specifically, we used a negative binomial regression model as the count variable of mental health symptoms was positively skewed indicating that most of the sample scored on the low end of the mental health scale (skewness = 0.52; p ≤ .01). The skewness of the mental health variable violates the assumption of ordinary least squares regression of a normal distribution of the dependent variable (Land, McCall, & Nagin, 1996; Long & Freese, 2006). Poisson regression also appropriately handles skewed count data, but the assumption of the Poisson distribution is that the mean and variance of the outcome are approximately equal, and our measure of mental health symptoms violates this assumption (M = 12.77 and variance = 84.82). The likelihood ratio test, a test of the overdispersion parameter alpha, was calculated. If the overdispersion parameter (alpha) was zero, a Poisson and negative binomial distribution would yield equivalent results. The likelihood ratio test that the overdispersion parameter (alpha) was 340.87 and was significant at the p < .000 level, thus the alpha was significantly different from zero and the negative binomial distribution was the most appropriate for the mental health symptoms outcome.
Coefficients from stepwise negative binomial models are found in the first column of each model in Table 3, with exponentiated coefficients or incidence-rate ratios (interpreted similarly to odds ratios yielded from logistic regressions) in the second column of each model in the table. The incidence-rate ratios are interpreted as risk for an additional mental health symptom. As seen in the first model, African American respondents had 30% lower odds of reporting a mental health symptom. After the race by gender interaction is added in Model 2, the main effect of race is no longer different from zero. In Model 3, after the addition of disrupted family process to the model, men have 69% greater odds of reporting an additional mental health symptom than do women, and for each additional disrupted family process, the odds of a youth reporting an added mental health symptom increased by 11%. As seen in Models 4 and 5 of Table 3, disrupted family processes did not interact significantly with gender or race. The model fit statistics of the final model (chi-square) indicated appropriate model fit (see Table 3). Also, the pseudo r squared indicated that approximately 6% of the variance in mental health was accounted for by the predictors in the model.
Coefficients (Standard Errors in Parentheses) From Stepwise Negative Binomial Regression of the Association Between Gender, Race, and Disrupted Family Process With Mental Health in Grandparent-Headed Households (N = 188).
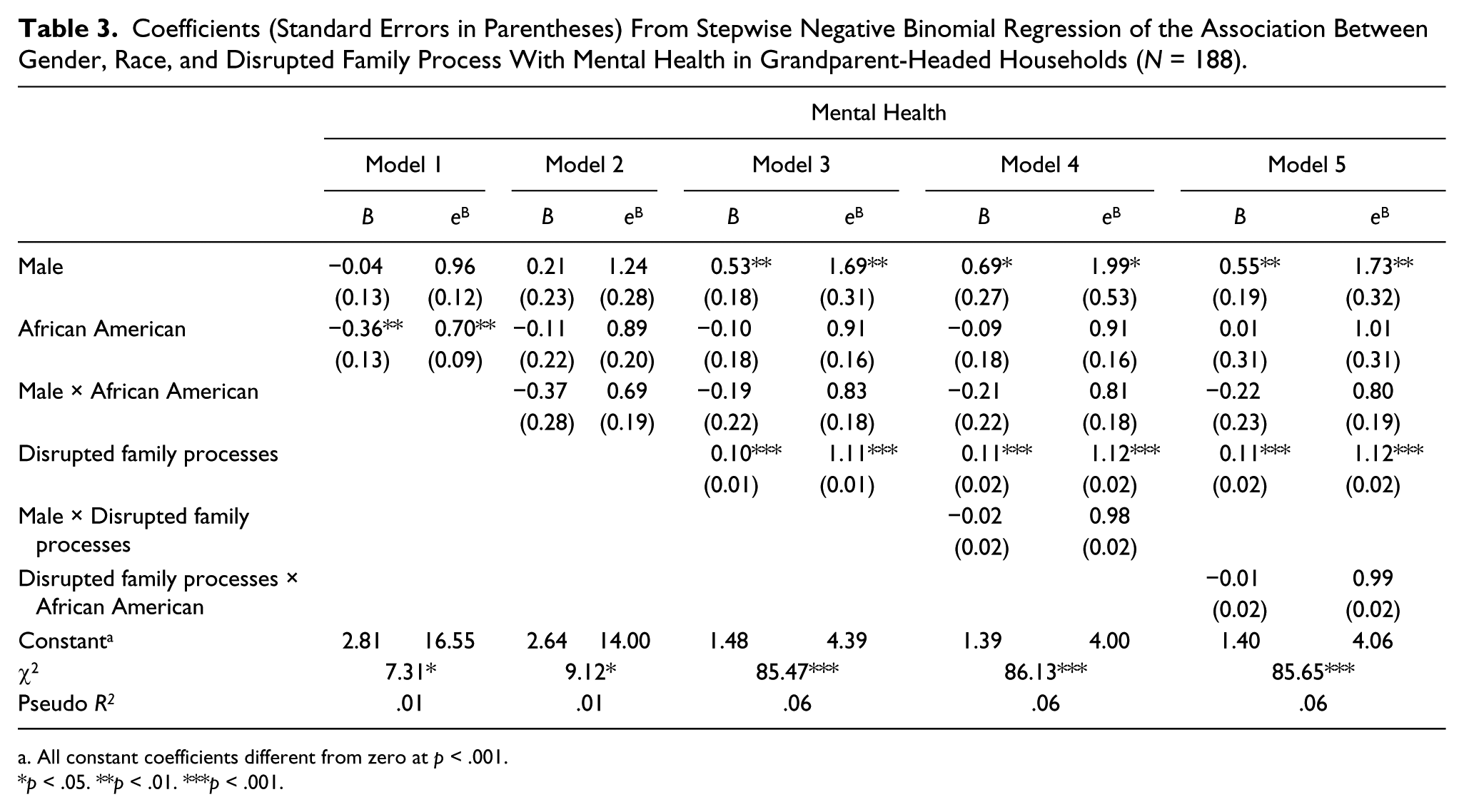
All constant coefficients different from zero at p < .001.
p < .05. **p < .01. ***p < .001.
Discussion
The current study addressed the mental health and disrupted family processes of court-involved youth being raised by their grandparents. While the literature has explored the emotional well-being of youth being raised by their grandparents, children involved in the juvenile court system are potentially different from their peers and therefore exploring their mental health is important. Furthermore, it is important to investigate the associations between race and gender in regards to the mental health in these youth, as these factors may play an important role in their lived experiences. Finally, the study addressed the association between disrupted family processes and mental health, as moderated by gender and race.
In general, youth in the court system who were being raised by their grandparents showed similar mental health and disrupted family process scores displayed in previous samples of court-involved adolescents that were being raised in differing forms of two-parent and single parent–headed households (cf., Gavazzi, Russell, & Khurana, 2009 and Gavazzi, Lim, et al., 2008). The resemblance of these average risks among differing family forms would suggest that it is not structure per se but rather the interaction of family factors and mental health symptoms with certain demographic variables (i.e., gender and race) that create important differences in the lives of these youth (Gavazzi, 2011). Indeed, results from the current study indicated significant mean differences in these constructs across gender and race.
Specifically, with regards to gender and race associations with mental health, Caucasian males were found to have higher mental health symptoms than both African American males and Caucasian and African American females; this supports of the finding of Solomon and Marx (1995), which claimed that adolescent females being raised by their grandparents experience fewer behavioral problems. In contrast, both African American and Caucasian females reported more frequent disrupted family processes than males (this difference was statistically different for African American females). This disparity in disrupted family processes experienced by female youth in the court system being raised by their grandparents suggests that these females may have uniquely challenging family circumstances.
Furthermore, male African American youth experienced less disrupted family process than their male Caucasian counterparts. This may be because of the fact that residing with a grandparent is relatively normative for African American youth (Burton & Dilworth-Anderson, 1991; Hayslip & Kaminski, 2005b; U.S. Bureau of the Census, 2000). Because of this trend, male African American youth may be more likely to reside with their grandparents from a younger age and continue to reside with them into adolescence, without additional custodial transitions. Fewer transitions may be linked with fewer disrupted family processes. On the other hand, the increased frequency for which custodial grandparenting may occur for African American youth may not necessarily negate the challenges common to these circumstances.
Finally, regardless of gender or race, each disrupted family process led to a significant increase in mental health symptoms for youth in the court system being raised by their grandparents. It is clear from these findings that disrupted family processes are detrimental to adolescent well-being and emotional health. Given the parenting difficulties that custodial grandparents often face (see Hayslip and Kaminski, 2005b), disrupted family processes may be greater in grandparent-headed households. Thus, family processes of grandparent-headed households may be an ideal point of intervention, especially for youth involved in the juvenile justice system.
While the current study addresses a research breach in the field, there were some limitations. The current study only examined the mental health and disrupted family process of youth in the juvenile justice system raised by their grandparents. Future research should address disrupted family process and mental health of youth from a variety of family backgrounds and structures including low risk youth, and those raised by single-parent versus two-parent families. Furthermore, as the current study is cross-sectional in nature, it is possible that it is not only disrupted family processes that led to mental health symptoms, but that mental health symptoms in adolescents lead to or influence disrupted family processes. Because only a relatively small percentage of youth are raised by grandparents, the current sample was drawn from various sites where various assessment administrators collected the data. Steps were taken in the study protocol to ensure systematic procedures, yet holding these constant would give greater confidence to the current results. Longitudinal research is needed to examine adolescent outcomes before, during, and after residing with grandparents.
Despite limitations, the current study provides an investigation into an underresearched area. Grandparents are raising more youth today than ever before and this trend seems to only be increasing with the passing of time (Hayslip & Kaminski, 2005a). In certain ethnic groups, grandparents are often primary caregivers for adolescents (Goodman & Silverstein, 2002). Though researchers have begun to address the mental and emotional well-being associated with being raised by a grandparent, few if any studies have addressed these issues in a court-involved population, which may be at greater risk. Overall, court-involved youth who were living with their grandparents saw increases in mental health problems as the number of disrupted family processes increased. These findings held true regardless of gender or race. Intervention efforts addressing family processes in grandparent-headed families may be particularly fruitful for the long-term mental health benefit of adolescents in these families.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by National Institute of Child Health and Human Development, 1K01HD056238-01, awarded to the third author.