
Abstract
Guided by the integrative model of behavioral prediction, we examined factors associated with more extensive mother–adolescent sexual communication. Participants were 303 mothers of young adolescents who completed a survey assessing their skills, attitudes about the outcomes of sexual health discussions, perceptions of social norms, self-efficacy, and sexual communication intentions at baseline (Time 1) and the extent of their sexual communication with their adolescent 6 months later (Time 2). A path analysis showed that, after accounting for the correlations among the four predictors and sexual communication at Time 1, intentions mediated the relationships between mothers’ skills, attitudes, and self-efficacy and the extent of their sexual communication with their adolescent. Attitudes also were related directly to mothers’ sexual communication. These results provide support for the utility of the integrative model of behavioral prediction for identifying parent characteristics that are related to more extensive parent–adolescent sexual communication and one mechanism by which these relationships may occur.
Keywords
Researchers have shown repeatedly that many parents do not communicate adequately with their children about sexuality (Boyas, Stauss, & Murphy-Erby, 2012; Morawska, Walsh, Grabski, & Fletcher, 2015; Weaver, Byers, Sears, Cohen, & Randall, 2002). That is, only a minority of parents report having in-depth discussions (Byers & Sears, 2012; Jaccard, Dittus, & Gordon, 1998; Weaver et al., 2002); and adolescents report less frequent and poorer quality sexual communication than their parents do (DiIorio, Pluhar, & Belcher, 2003; Jaccard, Dittus, & Gordon, 2000; Jaccard et al., 1998; Morawska et al., 2015). The pervasiveness and persistence of this situation is troublesome for at least two reasons. First, most parents view talking to their children about sexuality as an important way to communicate family values and prepare them for adulthood (Dyson & Smith, 2012; Wilson, Dalberth, Koo, & Gard, 2010). Second, more extensive parent–child sexual communication is associated with various positive outcomes such as delayed initiation of sexual activity and more frequent contraceptive and/or condom use (de Looze, Constantine, Jerman, Vermeulen-Smit, & ter Bogt, 2015; Hutchinson, Jemmott, Jemmott, Braverman, & Fong, 2003; Hutchinson & Montgomery, 2007; Jaccard, Dodge, & Dittus, 2002).
Our understanding of why parents are not more active in their adolescents’ sexual health education is limited. That is, researchers have not identified factors that uniquely predict the extent of parent–child sexual communication across time and/or mechanisms underlying parent–child sexual communication. Although researchers have investigated parent–adolescent sexual communication as a predictor of adolescent sexual risk behaviors longitudinally (Beckett et al., 2016; Henrich, Brookmeyer, Shrier, & Shahar, 2006; Hutchinson et al., 2003), we could find no prospective studies of factors associated with parent–child communications—that is, studies that used data collected at two or more time points. It is particularly important to conduct such research with parents of young adolescents. This is because, only a small minority of young adolescents in North America have engaged in genitally focused sexual activity such as sexual intercourse (Boyce, Gallupe, & Fergus, 2008; Byers, Sears, & Foster, 2013; Henrich et al., 2006; Saewyc, Taylor, Homma, & Ogilvie, 2008) and parent–child sexual communication appears to have more impact before youths engage in sexual activity (Dittus, Miller, Kotchick, & Forehand, 2004; Miller, Levin, Whitaker, & Xu, 1998). Yet few parents of middle school children have in-depth discussions with their adolescent on any sexual topic. For example, Weaver et al. (2002) found that only between 3% and 35% had discussed any of 10 sexual health topics (e.g., puberty, sexually transmitted infections, correct names for genitals, sexual decision making) with their child in a lot of detail; between 7% and 60% had discussed these topics not at all. When parents do communicate with their adolescent about key sexual topics, they typically do so after their adolescent has begun engaging in sexual activity (Beckett et al., 2016). Therefore, the primary goal of this study was to enhance our understanding of factors and mechanisms associated with the extent of parents’ sexual communication with their young adolescent based on the integrative model of behavioral prediction (IMBP; Fishbein, 2000; Fishbein et al., 2001). We examined mother–adolescent sexual communication only because few fathers responded to our survey.
Integrative Model of Behavioral Prediction
The IMBP (Fishbein, 2000; Fishbein et al., 2001) combines key constructs from the theory of reasoned action (Ajzen & Fishbein, 1980), the theory of planned behavior (Ajzen, 1991), the health belief model (Janz & Becker, 1984), and social cognitive theory (Bandura, 1996) to identify a limited number of variables that determine any behavior. According to the IMBP, a behavior is most likely to occur when individuals have a strong intention to engage in the behavior and the skills to perform the behavior. Intentions describe people’s motivation or plan to perform a behavior. Skills are abilities individuals need to enact a behavior. The strength of people’s intentions is determined by their attitudes, perceptions of social norms, and self-efficacy. Attitudes are positive and negative evaluations of the likely outcomes of performing the behavior. Perceptions of social norms refer to people’s perceptions of how others who are important to them would view their engagement in the behavior. Self-efficacy refers to individuals’ confidence that they could enact the behavior.
The IMBP model describes attitudes, perceptions of social norms, and self-efficacy as factors that shape behavior indirectly through their effects on intentions. However, in some instances, these three variables also can have direct effects on behavior (Fishbein, 2000; Fishbein et al., 2001). Similarly, skills may contribute to a behavior both directly and indirectly in that individuals without skills would not only be less likely to enact the behavior but also would be less likely to form intentions to enact the behavior. Using the IMBP model, researchers have demonstrated that the IMBP predictors are associated with intentions and behaviors related to health risk (e.g., alcohol use, condom use), health promotion (e.g., studying, exercise), and sexuality (Basen-Engquist & Parcel, 1992; Munoz-Silva, Sanchez-Garcia, Nunes, & Martins, 2007; Simms & Byers, 2013, Villarruel, Jemmott, Jemmott, & Ronis, 2004). To our knowledge, the IMBP model has not been used to study parent–adolescent sexual communication. Therefore, we assessed the direct relationships between the IMBP model variables and the extent of parents’ sexual communication with their young adolescent 6 months later as well as the indirect relationships between these variables and sexual communication mediated through parents’ sexual communication intentions.
Predictors of Parent–Adolescent Sexual Communication Behavior
There is considerable evidence that parents who report more sexual communication with their children and adolescents also report having more skills for engaging in this behavior, such as being more comfortable discussing sexuality topics (Byers, Sears, & Weaver, 2008; Guilamo-Ramos, Jaccard, Dittus, & Collins, 2008; Pluhar, DiIorio, & McCarty, 2008). They also report more positive and fewer negative attitudes about the outcomes of parent–adolescent sexual communication and more confidence in their ability to engage in these discussions (DiIorio et al., 2000; Guilamo-Ramos et al., 2008; Jaccard et al., 2000; Pluhar et al., 2008). In addition, one study found that mothers with more positive perceptions of social norms regarding parent–adolescent sexual communication engaged in more frequent conversations with their young adolescent (Guilamo-Ramos et al., 2008). However, there are at least two limitations to these studies. First, all of these researchers used cross-sectional designs in which they assessed the predictors and sexual communication behavior concurrently. This makes it impossible to evaluate whether any or all of these factors are related to sexual communication that occurs subsequently. Longitudinal research that controls for the prior level of sexual communication and shows these relationships across time would provide stronger support for the proposed connections. Second, only one study (Byers et al., 2008) has examined predictors of the depth or extent of parent–adolescent sexual communication. Given that it is unlikely that conversations in general terms only, no matter how frequent, will result in positive sexual health outcomes, it is important to identify factors associated with more extensive parent–adolescent sexual communication. We assessed mothers’ perceptions of the extent of their sexual communication with their adolescent about a range of sexual topics and evaluated whether their self-reported skills (i.e., comfort discussing a range of important sexual topics), attitudes, perceptions of social norms, and self-efficacy for having sexual health discussions at Time 1 were related directly to the extent of their sexual communication 6 months later (Time 2).
Intentions as a Mediator
According to the IMBP, individuals’ attitudes, perceptions of social norms, and self-efficacy contribute to their behavior indirectly, mediated by their intentions. We believe that parents’ skills may also shape their sexual communication behavior in this way. Mediators are variables that describe processes or mechanisms that account for the relationship between a predictor variable and an outcome variable (Hayes, 2013). There is indirect evidence that many parents have general intentions to communicate with their adolescent about sexuality in the future. For example, most parents agree that schools and parents should share the provision of sexuality education, suggesting that parents view this activity as one of their responsibilities (Weaver et al., 2002). Similarly, many mothers of school-aged children report that they plan to be proactive about sexual communication with them (Pluhar, Jennings, & DiIorio, 2006), although there may be a wide range in the ages at which they expect to have these discussions (Askelson, Campo, & Smith, 2012).
Some researchers have demonstrated that there are links between parents’ sexual communication intentions and some of the IMBP predictors. For example, Askelson et al. (2010) found that, for mothers who planned to have their daughter receive the HPV vaccine, more positive attitudes, and perceptions of social norms were associated with stronger intentions of using this event to talk to their daughter about sexuality. In addition, in our previous research (Byers & Sears, 2012), we found that mothers who did not intend to discuss sexual health topics with their adolescent scored lower on measures of sexual communication comfort, attitudes, perceptions of social norms, and self-efficacy than did mothers with these intentions and mothers who had already had these discussions. However, we could find no studies that examined the relationship between parents’ intentions to communicate with their children about sexual health topics and the extent of their subsequent sexual communication behavior or whether intentions serve as a mechanism by which predictors contribute to parents’ sexual communication. Therefore, we assessed whether parents’ Time 1 intentions to communicate about sexual topics within the next 6 months mediated the relationships between the IMBP variables (i.e., skills, attitudes, perceptions of social norms, and self-efficacy) at Time 1 and the extent of mothers’ sexual communication with their adolescent 6 months later (at Time 2).
Covariates
Jaccard et al. (2002) identified child recipient characteristics as being important for understanding variation in parent–adolescent sexual communication. Therefore, in our analyses, we controlled for two child recipient characteristics that have been linked to parent–child sexual communication—adolescent gender and adolescent pubertal timing. A number of researchers have found that mothers are more likely to talk about sexuality with their daughters than with their sons (DiIorio et al., 2003; Henrich et al., 2006; Hutchinson & Montgomery, 2007; Kapungu et al., 2010; Swain, Ackerman, & Ackerman, 2006). In addition, parents with children who are going through puberty are more likely to talk to their children about sexuality (DiIorio et al., 2003; O’Sullivan, Meyer-Bahlburg, & Watkins, 2001; Swain et al., 2006).
The Current Study
Our goal was to further our understanding of factors and mechanisms that result in more extensive parent–adolescent sexual communication. We extended previous research by studying sexual communication with young adolescents, using longitudinal data to assess relationships, controlling for the extent of sexual communication at Time 1, and using the IMBP as a theoretical framework. That is, we examined both the direct and the indirect (mediated through sexual communication intentions) relationships between the IMBP model variables and the extent of parents’ sexual communication with their young adolescent 6 months later. Specifically, we tested two hypotheses, both of which are consistent with the IMBP (see Figure 1). To consider both hypotheses, we controlled for parent–adolescent sexual communication at Time 1. This allowed for the examination of the extent to which the predictors at Time 1 were associated with change in sexual communication from Time 1 to Time 2. We predicted that:
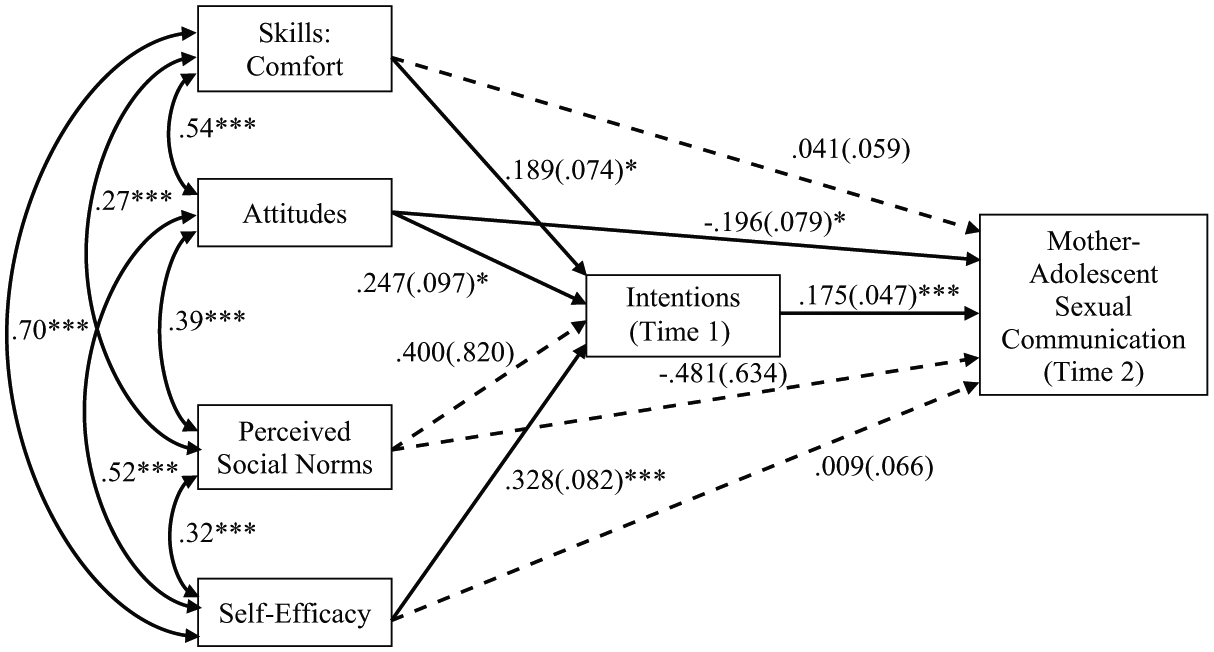
Model showing the unstandardized path estimates and their standard errors (in parentheses) as well as the significant correlations among the IMBP predictor variables.
Method
Participants and Procedure
The participants were 303 mothers of young adolescents who completed a survey at both baseline (Time 1) and 6 months later (Time 2). At Time 1, these mothers were about 40 years old, M (SD) = 40.1 (5.3), and a majority of them (81%) were living with a partner. On average, they had 2.4 children (SD = 1.0). In terms of their level of education, 27% of mothers reported that they had completed high school or less, 44% had completed postsecondary trade or technical school, and 28% had completed an undergraduate or graduate degree. Seventy-four percent of mothers were employed. Similar percentages of mothers were reporting on a daughter (53%) and on a son (47%). About half of these adolescents were in Grade 6 (54%) or in Grade 7 (46%), and two thirds of them (67%) were living with their biological parents. About half of these youths were the oldest or only child (46%) and 41% were the youngest child. Although we did not assess ethnicity specifically, in keeping with the demographic characteristics of the Canadian province in which the study was conducted, it is very likely that the sample was predominately White.
To recruit the sample, we sent survey packages for parents to 11 schools in rural and urban communities in a small Canadian province. Teachers distributed the sealed packages to students in Grades 6 and 7 and requested that they take them home to their parents. Each package contained a letter describing the study as a study of parents’ communication with their adolescents about sexual health, information about compensation for completing the survey, a copy of the survey, a contact information sheet, and a stamped addressed envelope. Parents returned their completed survey directly to the researchers by mail in the enclosed envelope, along with the contact information sheet if they wished to receive $25 as compensation for their time, a summary of the results, and/or were willing to be contacted about completing the Time 2 survey. According to the schools, 2,104 students were enrolled in the two grades at Time 1. We estimated that 1,999 surveys were distributed to students after accounting for absenteeism on the days that the survey packages were distributed. In total, 655 parents returned a survey at Time 1 for a response rate of 33% (range per school was 25% to 41%). Six months later, each of the 545 parents who agreed to be recontacted was sent a letter requesting their participation in the Time 2 data collection, a survey, and a stamped addressed envelope. Three hundred thirty-six parents (62%) returned a survey. Of these, 33 surveys were excluded: 27 because they were completed by fathers and this number was deemed too small to include them in the analyses and 6 because they were missing data on the extent of sexual communication. We compared the mothers who did and did not return surveys at Time 2 on their Time 1 responses. The two groups did not differ in terms of demographics such as age, F(1, 573) = 2.60, p = .107; marital status, χ2(5) = 4.56, p = .471; level of education, F(1, 575) = 1.95, p = .163; employment status, F(1, 575) = 0.11, p = .740; and number of children, F(1, 573) = 0.98, p = .323.They also did not differ on the predictor and control variables, F(4, 579) = 0.02, p = .889 or their intentions to discuss sexuality with their adolescent, F(1, 558) = 0.86, p = .491.
Measures
At Time 1 and Time 2, participants completed a survey that contained measures arranged in one of four random orders. Only the measures included in the analyses are described below. The covariates (adolescent gender and adolescent pubertal timing), predictors (comfort, attitudes, perceptions of social norms, and self-efficacy) and mediator (intentions) were assessed at Time 1. The extent of parent–adolescent sexual communication was assessed at Time 1 and Time 2.
Covariates
Participants reported their adolescent’s gender and grade at Time 1. They also described their adolescent’s pubertal development by completing four items from the Pubertal Development Scale (PDS; Petersen, Crockett, Richards, & Boxer, 1988). They rated breast growth and menarche in daughters, deepening voice and facial hair growth in sons, and body hair growth and skin changes in both daughters and sons using a 4-point scale, no (1); yes, a little (2); yes, some (3); yes, a lot (4); the menarche item for daughters was rated dichotomously, no (1); yes (4). Scores on the four PDS items were averaged within gender. Mean ratings by mothers in this sample were 3.04 (SD = 0.74) for girls and 2.05 (SD = 0.88) for boys. This suggests that their daughter’s pubertal development was underway and their son’s pubertal development had just begun. The internal consistencies were good (α = .75 for girls and α = .87 for boys). The PDS is a reliable and valid measure that has been used widely and can be completed by adolescents or parents (e.g., for the latter, see Davison, Werder, Trost, Baker, & Birch, 2007; Saxbe & Repetti, 2009). Consistent with previous work (e.g., Ge et al., 2006, Harden & Mendle, 2012), for the analyses, we standardized the PDS scores within gender and age to create a measure of pubertal timing with a mean of 0 and standard deviation of 1 for both girls and boys (pubertal timing). Higher scores indicate mothers’ perceptions of their adolescent’s earlier physical development relative to same-sex, same-age peers.
Skills (Comfort)
At Time 1, mothers reported their comfort discussing 12 sexual health topics (e.g., puberty/physical development, sexual decision making) using a 5-point scale not at all comfortable (1) to extremely comfortable (5). Ratings were summed to create a total score ranging from 12 to 60, with higher scores indicating perceptions of greater comfort. This scale was adapted from Cohen, Byers, and Sears (2012) who assessed the sexual comfort of teachers using a more extensive list of topics. These authors reported a high internal consistency and demonstrated construct validity for the scale in their sample. The internal consistency was high in the current sample of mothers (α = .95).
Attitudes
We evaluated parents’ expectations about possible outcomes of talking to their adolescent about sexuality at Time 1 with the Expected Outcomes of Parent–Child Sexual Communication Scale (Byers & Sears, 2012). Mothers responded to 13 items that describe possible positive and negative outcomes for both the parent (e.g., I would feel that I did the right thing; I would feel embarrassed) and the adolescent (e.g., my child would be less likely to have sexual intercourse as a young teen; my child would think I do not trust him or her) using a 5-point Likert-type scale, strongly disagree (1) to strongly agree (5). Summed scores ranged from 13 to 65, with higher scores reflecting more positive attitudes toward parent–adolescent sexual communication. The internal consistency of this measure was good (α = .81).
Perceived Social Norms
We assessed parents’ Time 1 perceptions of the extent to which others who are important to them would agree with and support them talking to their adolescent about sexual health using five items adapted from Yzer and van den Putte (2006). First, participants reported the extent to which they agreed that most people who are important to them think they should talk to their adolescent about sexual health topics with a 5-point scale, strongly disagree (1) to strongly agree (5). Then, they responded to four items indicating the extent to which their partner/spouse, siblings, parents, and in-laws, and most of their friends would approve of them talking to their adolescent about sexual health topics using a 5-point scale, strongly not approve (1) to strongly approve (5). They were also given the option of indicating that the item did not apply given that not all parents would have a partner/spouse, siblings, and/or living parents or in-laws. Such responses resulted in missing data for these items. Therefore, in keeping with Yzer and van den Putte (2006), responses from the five items were averaged when scores were available for at least three of them. Yzer and van den Putte (2006) reported a high internal consistency using this method (α = .84). The internal consistency in this sample was lower but acceptable (α = .75).
Self-Efficacy
At Time 1, parents reported their level of confidence that, in the following 6 months, they could talk with their adolescent about each of the 12 sexual health topics if they really wanted to. Each topic was rated using a 5-point scale ranging from not at all confident (1) to very confident (5), with higher summed scores (range = 12-60) indicating higher self-efficacy. DiIorio et al. (2001) demonstrated good reliability and validity for a similar scale (α = .97 in the current sample).
Intentions
Guided by Fishbein et al. (2001), we developed a measure of parents’ intentions to communicate with their young adolescent about sexual health topics (Byers & Sears, 2012). At Time 1, participants rated the likelihood that they would discuss each of the 12 topics with their adolescent in the following 6 months using a 5-point scale, very unlikely (1) to very likely (5). A total score was computed, ranging from 12 to 60, with higher scores indicating stronger intentions to communicate. Similarly worded items have been shown to reliably predict a variety of behaviors (Armitage & Conner, 2001). The internal consistency in the current sample was high (α = .95).
Parent–Adolescent Sexual Communication
We used 12 items, based on similar items used by Byers and her colleagues (Byers et al., 2008; Weaver et al., 2002), to assess the extent of parent–adolescent sexual communication at Time 1 and Time 2. At Time 1, participants indicated the extent to which they had ever discussed each of 12 sexual health topics with their son or daughter using a 4-point scale, not at all (1), in general terms only (2), in some detail (3), in a lot of detail (4). At Time 2, participants indicated the extent to which they had discussed each of 12 sexual health topics with their son or daughter in the previous 6 months (i.e., since they completed the Time 1 survey) using the same scale. Total scores were computed, ranging from 12 to 48, with higher scores indicating more extensive communication. The authors reported evidence for the reliability and validity of an earlier version of the scale. The internal consistency was high in the current study (α = .91 at Time 1 and α = .93 at Time 2).
Results
Descriptive statistics for the variables in the study are reported in Table 1. With respect to the predictor variables, at Time 1 mothers reported, on average, that they would be moderately comfortable discussing sexual health topics with their adolescent. They also agreed, on average, that having sexual health discussions would result in positive outcomes, expected that important others would approve of such discussions, and felt confident that they could have such discussions. With respect to the mediator, mothers indicated, on average, that they were likely to talk to their adolescent about a range of sexual health topics in the next 6 months. Turning to the dependent variable, at Time 1 and Time 2, mothers, on average, reported having talked about the 12 topics between in general terms only and in some detail.
Descriptive Statistics and Correlations Among the Study Variables.
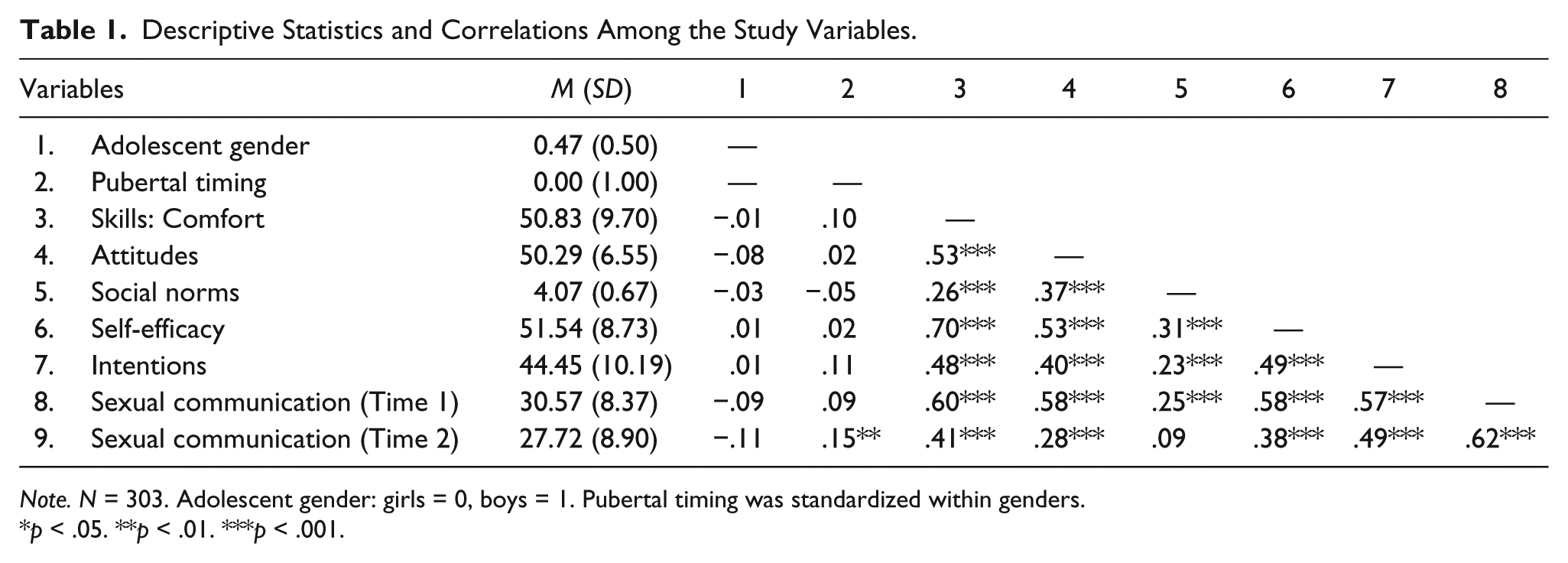
Note. N = 303. Adolescent gender: girls = 0, boys = 1. Pubertal timing was standardized within genders.
p < .05. **p < .01. ***p < .001.
The zero-order correlations among the variables are also presented in Table 1. The four IMBP variables were significantly positively associated with each other as well as with mothers’ sexual communication intentions and mother–adolescent sexual communication at Time 1. With the exception of mothers’ perceptions of social norms, each of the predictors and mothers’ sexual communication intentions was significantly positively correlated with mother–adolescent sexual communication at Time 2. Adolescent gender was not related to any of the variables and adolescent pubertal timing was significantly correlated with the extent of mothers’ sexual communication at Time 2 only.
Evaluation of the Relationships Between the IMBP Variables (Time 1) and the Extent of Mothers’ Sexual Communication (Time 2)
We used path analysis to test our model of the proposed relationships between the IMBP variables and the extent to which mothers discussed sexual health topics with their young adolescent (see Figure 1). The fit indices, the path estimates, and the effects presented in Table 2 were generated using SPSS AMOS (Kline, 2011; MacCallum & Austin, 2000). Adolescent gender, adolescent pubertal timing, and sexual communication at Time 1 were controlled in the analyses. First, we examined the fit of the entire model using multiple indices including the chi-square test, the root mean square error of approximation, and the comparative fit index. This assessment indicated a good fit of the model to the data: χ2(21, n = 303) = 27.46, p = .156; root mean square error of approximation = .032, 90% confidence interval [.000, .062]; and comparative fit index = .993.
Decomposition of the Predictors of the Extent of Mother–Adolescent Sexual Communication.
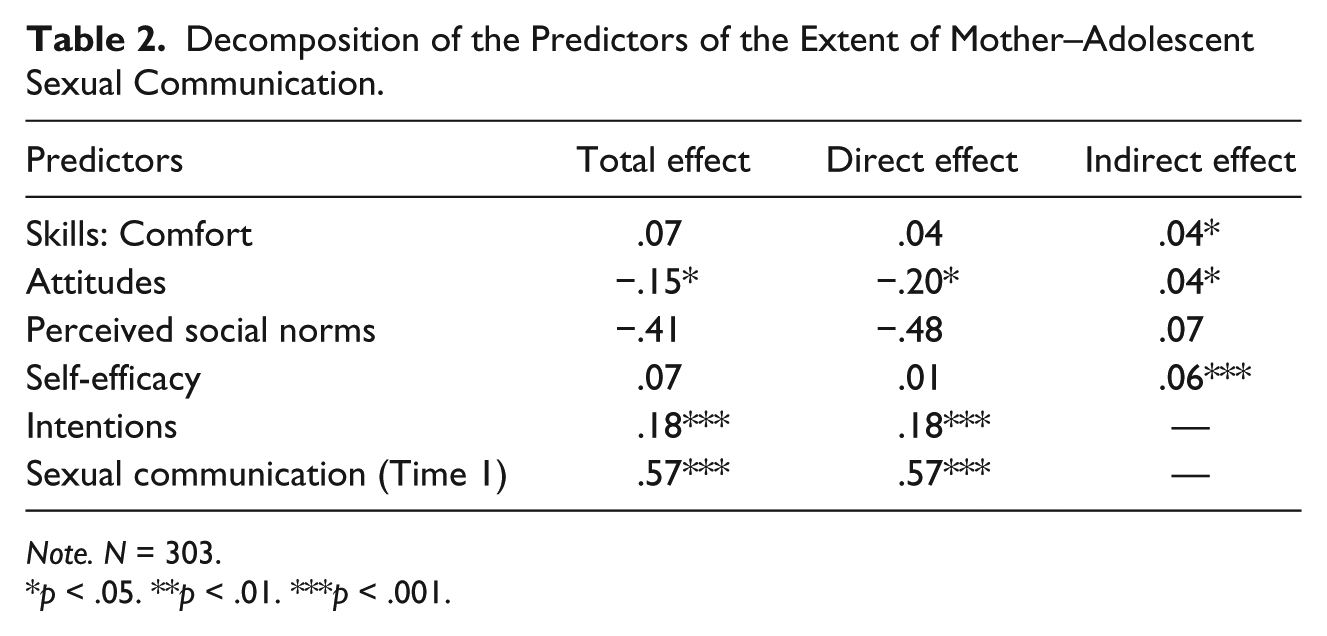
Note. N = 303.
p < .05. **p < .01. ***p < .001.
Next, we examined the estimates associated with the proposed relationships to ensure that important relationships among the constructs were reproduced. Individual paths between the variables need to be reviewed in the context of a good fit of the model because it is possible for relationships to be poorly reproduced even though the model fits well (Kline, 2011). As recommended by Kline (2011) and McDonald and Ho (2002), both the unstandardized and standardized estimates are presented. The unstandardized estimates and their standard errors are presented in Figure 1 along with the correlations among the IMBP predictor variables. The standardized estimates are reported below. The results showed a significant direct path from mothers’ attitudes to the extent of their sexual communication (−.146). However, none of the direct paths between mothers’ comfort, perceptions of social norms, and self-efficacy and the extent of their sexual communication were significant (.045, −.036, .009, respectively). Three of the four IMBP predictor variables were related indirectly to the extent of mothers’ sexual communication, however, through their significant relationships to mothers’ intentions to communicate with their adolescent about sexual health topics. That is, the paths linking mothers’ comfort, attitudes, self-efficacy to their intentions of communicating with their adolescent about sexual health topics were significant (.180, .157, .280, respectively); the path between mothers’ intentions and the extent of their sexual communication also was significant (.204). The path between sexual communication at Time 1 and sexual communication at Time 2 was significant (.545). The paths between gender (−.089), pubertal timing for girls (.094), and pubertal timing for boys (.102) were significant. The path between mothers’ perceptions of social norms and their intentions was not significant (.026).
Finally, we reviewed the pattern of direct and indirect effects linking the IMBP predictor variables to the extent of mothers’ sexual communication (see Table 2). Consistent with our description of the results for the paths above, mothers’ attitudes were significantly related to the extent of their sexual communication directly and indirectly; mothers’ comfort and self-efficacy were significantly related to the extent of their sexual communication indirectly; and mothers’ perceptions of social norms were not related directly or indirectly to the extent of their sexual communication. Mothers’ intentions were directly related to their communication behavior. This model accounted for moderate amount of variance in intention (R2 = .29) and sexual communication at Time 2 (R2 = .43)
Discussion
The overwhelming majority of mothers believe that they have a responsibility to talk to their children about sexuality (Morawska et al., 2015; Pluhar et al., 2006; Weaver et al., 2002). However, consistent with previous research (Boyas et al., 2012; Morawska et al., 2015; Weaver et al., 2002), on average, the mothers in this study did not talk extensively with their young adolescent about sexual health topics, even though they evaluated their comfort, self-efficacy, attitudes, and the attitudes of others positively—that is, average scores were above the midpoint on all of these scales. This pattern highlights the importance of identifying the combination of factors as well as the mechanisms that are associated with the extent to which mothers communicate with their young adolescent about sexual health topics—the goal of this study.
There are a number of strengths to our method of furthering an understanding of factors and mechanisms that may contribute to more extensive parent–adolescent sexual communication. First, whereas most researchers have studied sexual communication with older adolescents, we examined mother’s sexual communication with their young adolescents. This is important because, such communication appears to have more impact before youths become actively involved in romantic relationships or engage in sexual activity (Dittus et al., 2004; Miller et al., 1998). Although we did not assess sexual involvement directly, in keeping with previous research (Boyce et al., 2008; Byers et al., 2013; Henrich et al., 2006; Saewyc et al., 2008), it is likely that few of the adolescents had engaged in genitally focused sexual activity such as sexual intercourse. Second, we also used longitudinal data to assess the relationships, with the predictors and mothers’ intentions to have more extensive sexual communication assessed at Time 1 and mothers’ sexual communication behavior assessed at Time 2 for the intervening 6 months. Third, we controlled for the extent of sexual communication at Time 1.
Testing the Integrative Model of Behavioral Prediction
Another strength of this study was that we used the IMBP as a theoretical framework. Our path analysis results indicate that the IMBP framework provides an effective way to conceptualize factors associated with the extent to which mothers engage in sexual communication behavior with their young adolescent. Specifically, we found that, after controlling for sexual communication at Time 1, adolescent gender, and pubertal timing, the multiple interrelated mother characteristics proposed by the IMBP were associated with the extent to which mothers engaged in sexual communication at Time 2. In addition, we found support for the mechanism proposed by the IMBP for how these relationships play out—that is, through mothers’ intentions to have these communications. As predicted, mothers’ comfort, attitudes, and self-efficacy related to having sexual communications with their adolescent at Time 1 were indirectly related to the extent of their reported sexual communication with their adolescent at Time 2, mediated by their Time 1 intentions to have sexual communications with their adolescent in the next 6 months. Furthermore, although there was a strong relationship between mothers’ reports of the extent of their communication at Time 1 and at Time 2, the IMBP variables were associated with Time 2 sexual communication over and above the extent of mothers’ previous sexual communication. This may indicate that comfort, attitudes, and self-efficacy affect the long-term patterns of the extent of mothers’ communication with their adolescents about sexual health. These findings are consistent with our proposed model that, for mothers, greater comfort talking about sexual topics, more positive attitudes about the outcomes of such communications, and higher self-efficacy about having sexual health discussions shape their immediate motivation to have discussions about sexual topics with their adolescent and this motivation, in turn, enhances the extent of their sexual communication over the next 6 months. Overall, our results extend past research that has demonstrated the utility of the IMBP for predicting behavior related to health risk (e.g., Munoz-Silva et al., 2007; Villarruel et al., 2004) by showing that it is also useful for identifying factors that contribute to other behaviors, such as parent–adolescent sexual communication.
We expected that our four predictors also would be directly related to the extent to which mothers reported having discussed sexual topics with their adolescent in the past 6 months. In keeping with this view, three predictors—mothers’ comfort, attitudes, and self-efficacy—were significantly correlated with the extent of their sexual communication with their adolescent at the bivariate level. However, after accounting for the relationships among the variables in the model and the extent of sexual communication at Time 1, attitudes was the only factor to have a significant direct effect on mothers’ sexual communication. Our results suggest that mothers’ attitudes toward the outcomes of discussing sexual topics with their adolescent contribute to their sexual communication behavior in two ways. First, it strengthens their motivation or intentions to engage in these conversations. Second, mothers with more positive outcome expectations are more likely to enact their intentions. The direct effect between attitudes and extent of sexual communication extends past research that has shown that negative outcome expectations are associated with parents having ever discussed 20 topics with their adolescent as well as with the frequency of such discussions (DiIorio et al., 2000; Guilamo-Ramos et al., 2008; Jaccard et al., 2000). These results also are consistent with the results of qualitative research that found that, despite their motivation to do so, some mothers reported that concerns about the outcomes of such conversations was a barrier to providing sexual health information to their children (Dyson & Smith, 2012; Wilson et al., 2010). It is clear that mothers’ views about the outcomes of discussing sexual health topics play a pivotal role in facilitating their sexual communication behavior. Thus, efforts to promote this behavior depend in part on our success at identifying ways to enhance positive and reduce negative outcome expectations.
We did not find support for our predictions that mothers’ perceptions of social norms would be related directly and indirectly to their sexual communication behavior. In keeping with the IMBP, our measure of perceptions of social norms assessed mothers’ perceptions of the views of significant others in their lives about parent–adolescent sexual communication. Thus, these results suggest that mothers who have formed intentions to discuss sexual topics with their adolescent (related, in part, to their comfort, outcome expectations, and self-efficacy for engaging in these discussions) will enact these intentions regardless of their perceptions of the views of their families and friends. It may be that mothers’ behavior is shaped more by their beliefs about the views of other parents of similar-aged adolescents, their adolescent’s teachers, and/or the school curriculum than by the views of significant others. Research using a more comprehensive measure of parents’ perceptions of social norms is needed to assess this possibility. Alternately, it may be that mothers’ perceptions of social norms are less important for understanding parent–adolescent sexual communication than are the other IMBP predictors (i.e., comfort, self-efficacy, outcome expectations). According to the IMBP, the extent to which each of the predictors influences intentions and behavior is affected by both the behavior and population being studied (Fishbein & Ajzen, 2010).
Limitations and Conclusion
The results must be interpreted in keeping with some limitations of the study. First, only 33% of parents completed the survey at Time 1 and only 62% of them completed it at Time 2. In addition, because so few fathers returned our surveys, this research was limited to mothers only. Furthermore, because parents were informed that the study was about sexual communication, it may be that mothers with low perceived comfort and self-efficacy related to sexual communication and/or with conservative sexual attitudes were underrepresented in the sample (Bogaert, 1996; Morokoff, 1986; Wiederman, 1999). Thus, the extent to which the findings are generalizable to all parents of young adolescents is not known. Second, we evaluated a model that depicted a one-way direction of effect from four IMBP factors to mothers’ sexual communication behavior. Although this model was derived from the IMBP framework, alternative models that are equivalent or nonequivalent may fit the data equally well (Kline, 2011; MacCallum & Austin, 2000). Likely mothers’ characteristics and their sexual communication intentions and behavior interact in a reciprocal way over time. In addition, we assessed our variables at only two, rather than three or more time points. Although mediation can be evaluated using two time points (Kline, 2015), measurement of all of these variables at multiple points is needed to clarify how they operate in relation to one another. Third, it is possible that mothers’ sexual communication behavior between Time 1 and Time 2 was affected by their awareness that there was a follow-up component to the study. If so, this effect was not a strong one in that even at Time 2 mothers on average reported that they had not talked with their adolescent about the sexual health topics in detail. Nonetheless, research is needed which includes a control group at Time 2 to assess the impact of study participation on mothers’ behavior. Finally, we collected information about mother–adolescent sexual communication from mothers and not also from their adolescents. Research has shown that adolescents tend to perceive more limited communication about sexual health topics than their parents do (Jaccard et al., 1998, 2000; King & Larusso, 1997). Thus, research is needed that evaluates more complex longitudinal models that incorporate, in addition to the current predictors, adolescent characteristics (e.g., their willingness to be responsive when their parents initiate such discussions) that are expected to contribute to these interactions as well both parents’ and adolescents’ perceptions of the extent of their sexual communication discussions.
Nonetheless, the results of this study provide support for the utility of the IMBP for understanding parents’ sexual communication with their young adolescent from the mother’s perspective. Research is needed to determine the extent to which the IMBP variables as well as their influence on parent–adolescent sexual communication changes over time. Because comfort, attitudes, and self-efficacy are modifiable personal characteristics, our findings have important implications for increasing mothers’ sexual communication with their young adolescents, something that mothers (and fathers) want for themselves and their family (Dyson & Smith, 2012; Morawska et al., 2015; Weaver et al., 2002). Our finding that attitudes were strongly associated with both the extent of communication and intentions to communicate suggests that it is important to develop initiatives aimed at making parents aware that early and on-going sexual communication with their adolescent has been linked to positive sexual health outcomes for young people (de Looze et al., 2015; DiIorio et al., 2006; Evans, Blitstein, & Davis, 2011; Villarruel, Loveland-Cherry, & Ronis, 2010). For example, educational agencies and government could assist with the development of parental guides that would have wide reach to more families. Our finding that self-efficacy and comfort were strongly associated with the extent of sexual communication through their influence on intentions demonstrates the importance of educational initiatives aimed at enhancing these parental characteristics. Such initiatives could include workshops or other experiential activity that include skill building and role-play activities designed not only to enhance perceptions of social norms and outcome expectations but also to increase comfort and self-efficacy. Finally, as social norms toward sexual health education become more progressive, the development of interactive social media tools such as parenting blogs or Facebook groups may also assist with improving mothers’ outcome expectations, comfort, and self-efficacy.
Footnotes
Acknowledgements
The authors would like to thank Susan Voyer, Erin Atkinson, and Sara Thornton for their assistance with this project.
Authors’ Note
Research materials related to this study can be obtained by e-mail from the first author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the Social Sciences and Humanities Research Council of Canada to the first and second authors.