
Abstract
Maternal income increases immediate investment in children for food, child care, and health care, but whether maternal income influences longer term health and behavioral outcomes is unknown. Using data from the NICHD Study of Early Child Care and Youth Development, we examine the association between maternal income in early and later childhood on body mass index percentile, problem behaviors, and self-reported health status at age 15 among a sample of children (N = 1,283) whose mothers were employed at at least one observation time point between birth and age 15 (1991-2005). When controlling for family income (minus maternal income) and maternal employment characteristics, higher maternal income during early childhood was significantly associated with fewer adolescent problem behaviors. Maternal income during early childhood may influence adolescent behavioral outcomes. These findings suggest that increased maternal income, a positive externality of maternal employment, may increase the net benefit of maternal employment for child behavior.
Introduction
Childhood is a critical period for determining health status and behaviors in later life (Almond & Currie, 2010; Coneus, Laucht, & Reuss, 2012; Cunha & Heckman, 2007; Doyle, Harmon, Heckman, & Tremblay, 2009; Johnson & Schoeni, 2011). Parents with higher economic resources have the opportunity to use those resources to invest in child health, nutrition, and enriched home environments; these material investments are subsequently associated with improved adult health, behavior, and education outcomes (Berger, Paxson, & Waldfogel, 2009; Currie & Goodman, 2004). However, existing work has not been extended to isolate maternal income from household income to test the hypothesis that maternal income is a critical social determinant of child health. Strengthening the evidence about the effect of maternal income as distinct from household income on child health and behavior will contribute to the design of policy interventions that target critical periods in early life and may mitigate health disparities in adulthood (Almond & Currie, 2010; Coneus et al., 2012; Cunha & Heckman, 2008; Doyle et al., 2009).
To this end, this article examines the association between maternal income in childhood and adolescent outcomes. Prior research demonstrates that household income is positively associated with investments in children and contributes to child well-being over time (Berger et al., 2009; Currie & Goodman, 2004). However, it is possible that household spending decisions are driven by more than total household income. For example, the process of investing in children and the quantity and quality of those material investments may be connected to intrahousehold dynamics related to earning power and control over household resources (Duflo, 2003; Olafsson & Pagel, 2017; Thomas, 1990). In fact, research in the economics literature suggests that as a woman’s contribution to family income increases, household child-related spending patterns change (Thomas, 1990), and families are more likely to make immediate investments in their children for food (Kenney, 2008), child care (Phipps & Burton, 1998), health care (Barber & Gertler, 2010), and other goods (Attanasio & Lechene, 2002; Ward-Batts, 2008). However, there are three limitations to these prior findings. First, extant research focuses primarily on maternal employment and frames the relationship between maternal employment and child outcomes as a function of reduced maternal time allocation for children; this research has largely overlooked the positive outcomes of maternal employment, namely income. Second, despite evidence that the impact of investments in children accumulates over time (Conti, Heckman, & Urzua, 2010), most studies of female employment did not have the data available to examine how the effects of maternal income accrue from birth through adolescence (Anderson, Butcher, & Levine, 2003; Morrissey, Dunifon, & Kalil, 2011). Finally, existing studies that consider outcomes in adulthood or adolescence measure family-level characteristics (e.g., family income and education), not characteristics specific to mothers. In this article, we aim to address these limitations and address an important gap related to our limited understanding of maternal income as a distinct social determinant of child outcomes.
Theoretical Framework and Policy Implications
Microeconomic theory models the relation between maternal income and adolescent outcomes as a function of decisions regarding household-level monetary and time resource allocation (Phipps & Burton, 1998). Predictions about the direction of these effects are unclear because maternal income affects monetary and time constraints in opposite directions (Figure 1). Income generation occurs through maternal participation in the labor market; consequently, employed women may have less time to spend with children and less flexibility in their time (Anderson et al., 2003; Azier, 2004; Morrissey et al., 2011; Ruhm, 2008). At the same time, higher maternal income may enable women to offset the negative effect of reduced maternal time with children with increased investments in healthier foods, enriched environments, and health care (Apouey & Geoffard, 2013; Berger et al., 2009; Case, Lubotsky, & Paxson, 2002; Currie & Goodman, 2004; Yeung, Linver, & Brooks-Gunn, 2002).
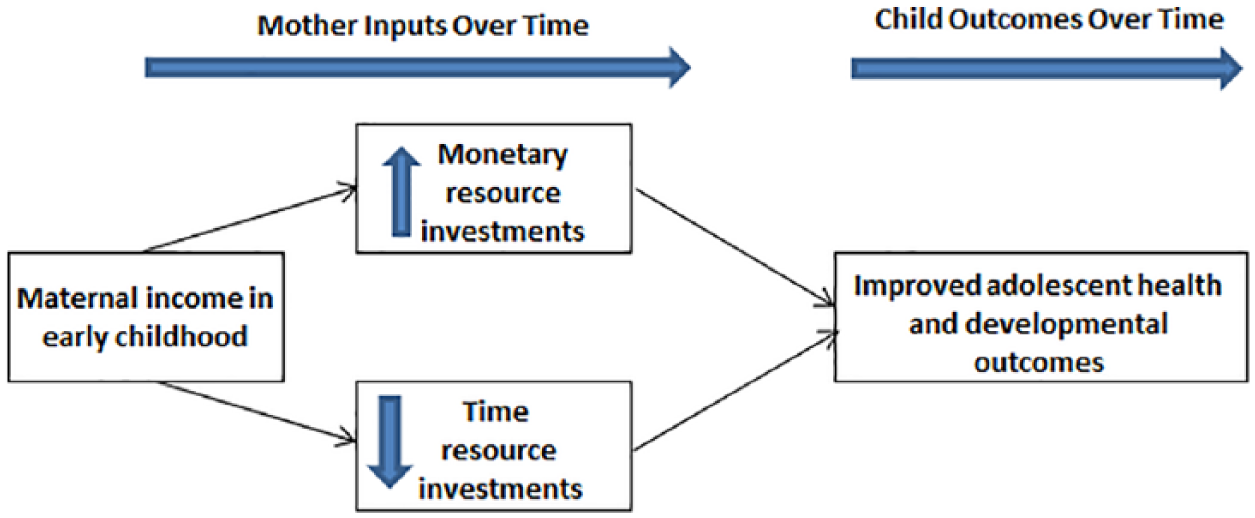
Hypothesized pathways linking maternal income and adolescent outcomes.
Furthermore, some research demonstrates that across childhood, there are specific windows of time or “sensitive periods” (Ben-Shlomo & Kuh, 2002) during which the effect of maternal income might have a stronger influence on the accumulation of risk for negative health and behavioral outcomes (Coneus et al., 2012; Cunha & Heckman, 2007; Doyle et al., 2009). Indeed, research and theory suggest that material investments in a child’s health and development during early childhood accumulate to produce advantages over time (Case et al., 2002; Cunha & Heckman, 2007; Currie & Goodman, 2004; Doyle et al., 2009). If this is the case, it is important to identify such windows so that policy interventions can target specific periods during childhood. For this reason, we examined two observational periods of maternal income: early versus late childhood.
While the primary contribution of this research is to begin to describe the association between maternal income earned throughout childhood on adolescent outcomes, specific child outcomes shown to be related to parental time and/or monetary investments are selected to explore this association, including body mass index (BMI; Anderson, 2012; Anderson et al., 2003; Morrissey et al., 2011; Ziol-Guest, Dunifon, & Kalil, 2013), behavioral problems (Azier, 2004; Ruhm, 2008), and health status (Apouey & Geoffard, 2013; Johnson & Schoeni, 2011). Furthermore, this article examines the association between maternal income earned during early childhood (infancy through first grade) and maternal income earned during later childhood (Grade 3 through adolescence) on child outcomes measured at age 15 to explore whether early versus later childhood is a sensitive period for which maternal income support might have a more important impact on child outcomes (Almond & Currie, 2010; Cunha & Heckman, 2007; Doyle et al., 2009).
The association between maternal income distinct from family income on child outcomes is a relevant policy question. If maternal income changes household spending patterns in ways that benefit children, expanding policies, including the provision of high-quality child care and after school programs (Karoly, Kilburn, & Cannon, 2005), to support more lower class and middle-class working families might offset the negative effects of reduced maternal time with children and complement the positive effects of maternal income. This study describes whether, when controlling for family socioeconomic status, health, and maternal employment characteristics, maternal income earned during childhood is correlated with subsequent adolescent health and behavioral outcomes at age 15. These results may improve our understanding of how maternal income can shape the family environment and contribute to child health.
Method
Data and Variable Definitions
Data Source and Sample
The NICHD Study of Early Child Care and Youth Development (SECCYD) is a national longitudinal study that recruited families with a target child born in 1991 from 10 sites across the United States and followed them from the child’s birth to 15 years of age (NICHD Early Child Care Research Network, 2001). Families were recruited throughout 1991 during 24-hour sampling periods in hospitals where women who had given birth were visited to assess eligibility. Participants were excluded if the mother was less than 18 years old, the mother was unable to speak English, the family planned to move, the mother delivered multiple births, the child was hospitalized for more than 7 days following birth or had obvious disabilities, the family lived too far away or in an unsafe neighborhood, or the mother had a known substance use problem. A total of 8,986 women were assessed for eligibility and 5,265 were assessed to be eligible. Randomized call lists were then generated and families were called in order from the list. Enrollment occurred during the first home visit when infants were 1 month old (N = 1,346). Data relevant for this study were collected at months 1, 6, 15, 24, 36, 54 and kindergarten, Grade 1, Grade 3, Grade 5, and age 15. The original SECCYD sample consisted of 1,364 children.
The present analysis included all children who were in the NICHD SECCYD database between 1991 and 2005 and whose mothers were employed during a minimum of one observation period between 6 months and age 15 (N = 1,283). We excluded the small number of children whose mothers who were not employed during the study to limit bias associated with selection into employment (n = 81). For example, compared with women who work, women who do not work while their children are young may face different household-level economic constraints or have other demands on their time or health that preclude them from seeking employment; therefore, between these groups we might observe different effects of maternal time and income on child outcomes. Maternal employment was measured beginning at 6 months postbirth to provide sufficient time for women to return to work after maternity leave because research shows that women in the United States take an average of 10 weeks of maternity leave (Shepherd-Banigan & Bell, 2014). The data set used is a publicly available, de-identified data set; consequently, this research was determined not to be human subjects research by the Institutional Review Board at the University of Washington and was exempt from further review.
Variable Definition and Measurement
Outcomes consist of three health and behavioral outcomes measured at age 15: age- and sex-specific BMI percentile (continuous), problem behaviors (continuous; higher score represents more behavioral problems), and self-reported health status (excellent/good health status vs. fair/poor health status). Outcomes were collected as follows:
BMI measurements were recorded by project staff during laboratory visits. BMI was calculated by weight (kg)/height2 (m2) and converted into an age- and sex-specific percentile using Centers for Disease Control and Prevention growth chart algorithms (Centers for Disease Control and Prevention, 2000).
The behavior-problem score (mother-reported) is the sum of externalizing and internalizing problem subscales and was measured using 12 items (0-2 Likert-type scale) from the Social Skills Rating System (Gresham & Elliott, 1990); internal reliability was 0.86. Higher scores represent more behavioral problems.
Health status (mother-reported) was measured on a 4-point scale (excellent to poor) and was dichotomized for this analysis as excellent/good (1) and fair/poor (0).
Predictors: Total annual maternal income from employment during early childhood and later childhood are the primary predictors of adolescent outcomes. Maternal income is defined as annual maternal income from employment aggregated between 6 months postbirth and Grade 1 (early childhood maternal income) and Grade 3 to age 15 (later childhood maternal income) averaged over the number of time periods that the woman was employed during early or later childhood. Income data were collected at months 6, 15, 24, 36, 54, kindergarten, 1st grade, 3rd grade, 5th grade, and age 15. At each time point, maternal income was adjusted to 2005 dollars using the inflation factor from the consumer price index. To improve coefficient interpretation, average maternal income was divided by 1,000.
Confounders were chosen a priori based on a review of the literature and include variables that are related to maternal income during childhood and adolescent outcomes at age 15. Of note, variables that were hypothesized to mediate the association of interest, such as the Home Observation for Measurement of the Environment score (HOME), which examines the relation between aspects of the home environment and child development (Caldwell & Bradley, 2003) or child care quality, were not included in the analytical models. The early family environment, defined as parental and family characteristics from prebirth to 15 years, exerts an important influence on health in later childhood and adulthood (Johnson & Schoeni, 2011). As our observation periods of maternal income spanned many years, time varying confounders were also averaged over time in an attempt to reflect some change. Therefore, following were controlled for in the statistical analyses:
Family demographic characteristics included the following:
Average household income in early childhood and later childhood: All sources of household income not attributable to maternal income from employment were aggregated and averaged over all observation periods during early childhood (age 6 months through Grade 1) and all observations periods during late childhood (Grade 3 through age 15). Prior to aggregation, nonmaternal household income was adjusted to 2005 dollars using the inflation factor from the consumer price index. Sources of income encompass husband/partner’s income from employment, if the individual lived at home during the observation time period, and other sources of income, such as alimony, income from a rental property, food stamps, and Women, Infants, and Children. The specific sources of income comprised in “other sources” were not specified in the data and could not be disaggregated from one another.
Total family income during pregnancy: Includes mother’s income from employment, other sources of income, and husband/partner’s income from employment if that individual lived at home during the pregnancy; adjusted to 2005 dollars.
Average number of dependent children during early childhood and later childhood: Total number of full-time children living in the house averaged across each observation period of early childhood and later childhood.
Proportion of data collection periods that the mother-reported being married in early childhood and later childhood: Categorized as married/not married; mother’s marital status was averaged over the number of observation periods in early childhood and later childhood.
Mother’s race/ethnicity: Categorized as non-Hispanic White; non-Hispanic Black, Hispanic, Other (reference).
Mother’s educational attainment at child birth: Categorized as “less than high school” (reference), “completed high school,” and “completed more than high school.”
Maternal age at child’s birth included as a continuous variable.
Maternal employment characteristics during early and later childhood included the following:
Total number of observation periods that the woman was employed in early childhood (age 6 months to Grade 1) and in later childhood (Grade 3 to age 15).
Annual hours worked per week divided by the total number of observation periods that the woman was employed in early childhood (age 6 months to Grade 1) and in later childhood (Grade 3 to age 15). Annual hours worked per week was included as a proxy for work role, job demands, and flexibility. Both maternal employment variables were significantly correlated with maternal income (proportion of time employed ρ = ~0.55; average hours worked ρ = ~0.70).
Child health endowment during early life, an important predictor of health disparities in adulthood (Conti et al., 2010), is represented by maternal health status, paternal health status, maternal depressive symptoms, and the child’s birth weight. Note that data for mother and father health were only collected during the time periods reported below.
Paternal health is measured as the average of self-reported father’s health measured on a 4-point scale (poor to excellent) over months 1, 6, 15, 24, 36, and 54.
Maternal health is measured as the average of self-reported mother’s health measured on a 4-point scale (poor to excellent) over months 1, 6, 15, 24, 36, and 54.
Average maternal depressive symptoms score during early and late childhood. Maternal depressive symptoms were assessed using the Center for Epidemiological Studies Depression Scale (Radloff, 1977).
Child birth weight was measured in grams categorized as normal (2,500-4,000g; reference), high (>4,000g) and low (<2,500g).
Most of the missing data were related to attrition; by age 15, 25% of the families were lost to follow-up. Attrition was associated with fewer periods of employment, lower income, higher maternal depressive symptoms, higher likelihood of being married, and younger maternal age at the child’s birth. Missing observations beyond attrition were largely concentrated in the outcome variables, particularly in BMI percentile. Missing an outcome variable was associated with lower maternal age, but no other demographic variables. To address missing data due to loss to follow up and other causes, analytic models were run with data sets imputed using the MICE system of chained equations (imputed data sets n = 15; Royston, 2009). Imputation in later time periods relied heavily on within-person data from baseline data (almost 100% complete) and data from prior time periods. Prior to running the analytical models, missing data models were examined to compare the value of the observed, complete, and imputed data. While the assumption of missing data model validity is untestable, examining graphical depictions of missing data model performance can highlight potential problems.
Analytical Models
Descriptive analyses were performed; proportions/means and standard deviations were computed for all variables. All variables were examined for skewness, kurtosis, and missing patterns. Bivariate distributions were examined for outliers and deviations from normality.
Generalized linear regression models were used to describe the association between maternal income and adolescent outcomes controlling for all covariates. Ordinary least squares regression was used for linear outcomes and logistic regression was used for binary outcomes. Robust standard errors were applied. Given the high correlation between maternal income and maternal employment characteristics and the potential for reciprocal influences over time on income and family health, we present results from each stage of model building. The first-stage model regressed the child outcomes on maternal income in early and later childhood, the total number of observation periods a woman was employed in early and later childhood, and the socioeconomic variables: mothers age and education at birth, mother’s race, total household income at birth, the proportion of periods that the mother was married during early childhood and later childhood, and the child’s birth weight. The second-stage model regressed the child outcomes on maternal income in early and later childhood, the total number of observation periods a mother was employed during early and later childhood, the socioeconomic variables, all other sources of household income not related to maternal employment in early and later childhood, and the number of dependent children living in the house full-time in early and later childhood. The third-stage model built on the second-stage model by adding the average number of hours the mother worked per week during early and later childhood. The fourth-stage model built on the third-stage model by adding the parental health variables (maternal and paternal health status and maternal depression score). Models included covariates averaged across time during early childhood (infancy to Grade 1) and later childhood (Grade 3 to age 15) to assess whether the association between maternal income in early childhood and child outcomes persisted into later childhood and whether maternal income in early childhood had a greater association than maternal income in later childhood with adolescent outcomes. The focus of this analysis will be the findings from the Stage 4 models. To assess the validity of the imputation models, results using the imputed data sets, complete case analysis, and analysis that excluded families that were loss to follow up by age 15 were compared. Analyses were performed using STATA IC 13 (College Station, TX).
Several sensitivity analyses were conducted. Analytical models were run to compare results among the imputed data set, the complete observations data set, and a data set that included all families in the SECCYD sample, including families in which mothers never worked.
Results
Descriptive statistics, including sample proportions/means and standard deviations, are reported in Table 1. Women in this sample were primarily non-Hispanic White, educated, and from middle- to high-income families. Average annual maternal income in early childhood was approximately $13,500 and was close to $27,000 in later childhood. Women were employed, on average, during 75% of the observation time points and worked, on average, 31 hours per week during early childhood and 34 hours per week during later childhood. Only 6% of women in the sample (n = 81) reported never having worked since the study child was born. The sample for this analysis likely contained a lower proportion of minority, single-parent families, and more high-income families than might have been be present in the study population catchment areas during recruitment. Maternal employment during the 15-year study period was associated with fewer maternal depressive symptoms and a lower likelihood of being married. Consistent with the prevalence of overweight among children in the United States during 2005 (Dehghan, Akhtar-Danesh, & Merchant, 2005), 25% of adolescents in this sample were overweight in 2005 (not reported in table). The adolescents in the sample were otherwise generally healthy and mothers reported few problem behaviors. The descriptive characteristics between the complete and imputed sample were substantively similar; differences in means and proportions between the observed and imputed samples means are presented in Table 1.
Participant Characteristics (N = 1,283).

Note. BMI = body mass index; CES-D = Center for Epidemiological Studies Depression Scale.
The descriptive statistics do not include values for the missing observations.
The results from the adjusted linear regression models are shown in Table 2 and represent the change in adolescent health and behavioral outcomes associated with a $1,000 increase in the mother’s average annual income. Mean change in the outcome (for linear models) and log odds (for binary models), 95% confidence intervals, and significance levels (cutoffs defined at α < .001 and α < .05) are displayed. Analyses run with imputed data sets, imputed with loss to follow-up families removed, and complete cases produced similar findings.
Association Between Maternal Income and Adolescent Outcomes.

Note. BMI = body mass index; CI = confidence interval. The coefficient is defined as a one-unit change in the outcome for every $1,000 increase in maternal income. Maternal income defined as maternal total annual income divided by number of periods employed during (a) early childhood (6 months through Grade 2) and (b) later childhood (Grade 3 through age 15) divided by 1,000. Sociodemographic variables include mother age, mother race/ethnicity, mother education level at birth, and total family income from all sources at birth. Family income/need variables include (a) average number of full-time dependent children living in the household from birth through first grade during early childhood (6 months through Grade 1) and later childhood (Grade 3 through age 15) and (b) total annual household income from all sources except maternal income from employment during early childhood (6 months through Grade 1) and later childhood (Grade 3 through age 15). Maternal hours worked is defined as the total number of hours worked per week divided by the total number of periods the woman was employed during early childhood (6 months through Grade 1) and later childhood (Grade 3 through age 15). Family health variables include maternal health status, paternal health status, and average maternal depression score divided by the number of observation time points.
p < .05. **p < .001.
Results discussed are those from the Stage 4 models, as these models contained all covariates identified a priori. Controlling for family demographics, maternal employment characteristics, and other family variables, maternal income in early childhood was associated with a statistically significant 0.05 decrease in the number of mother-reported problem behaviors at age 15. This result was consistent across all model stages. A similar association was not observed between maternal income in later childhood and problem behaviors at age 15. Maternal income in early or later childhood was not associated with BMI sex-and-gender percentile or child health status.
Discussion
The present study is the first that we know of to use data from the United States to consider the role of maternal income as a social determinant of child health by describing the association between maternal income during early and later childhood and adolescent outcomes. In the full model, controlling for family socioeconomic status, parental health, and maternal employment, maternal income in early childhood was associated with a slight decrease in the number of mother-reported behavior problems; maternal income in later childhood was not related to changes in the number of mother-reported behavior problems. These associations persisted despite the additional covariates included in the models. Also, no association was observed between maternal income in early or later childhood and adolescent BMI percentile and health status. Taken together, these findings suggest that maternal income during early childhood may be an important factor for positive adolescent behavioral outcomes, above and beyond the effects of maternal employment, which have been shown to have a detrimental impact on child behavior (Jacobson & Crockett, 2000).
Research suggests that higher maternal income might improve children’s health and development outcomes through increased household investments in children (Attanasio & Lechene, 2002; Azier, 2004; Berger et al., 2009; Currie & Goodman, 2004; Yeung et al., 2002). Specifically, studies from developing countries have shown that income generating programs for women, such as microcredit and cash transfers, improve the health outcomes of their children because women use these resources to invest in basic health and nutrition for their families (Duflo, 2003; Rubalcava, Teruel, & Thomas, 2009). Our results do not suggest a similar association between maternal income and adolescent health outcomes in the United States. The health and developmental needs of children in the United States versus children in developing countries are very different. For instance, the baseline population health status of U.S. children is higher and the majority of children have medical insurance and reasonable access to vital clinical care, including immunizations. Therefore, U.S. children may benefit less from parental investments in fundamental health inputs (e.g., immunizations, basic medical care, and basic nutrition), but more from parental investments in social and emotional development which might exert a stronger influence on behavioral outcomes.
Maternal income, however, is an externality of maternal work; and higher maternal work intensity has been shown to negatively affect child outcomes, such as obesity (Anderson et al., 2003) and problem behaviors (Jacobson & Crockett, 2000) because of limited supervision and family time promoting health (Anderson, 2012; Anderson et al., 2003; Azier, 2004). Yet our findings suggest that, for some outcomes, the negative time-related effects of maternal employment might be offset by the net benefit of maternal income. Our findings may have implications for how to strengthen policy interventions for low-income families by targeting families that are the most vulnerable, perhaps because of low maternal income, and directly addressing the source of those vulnerabilities. For example, programs that improve skills, access to employment, and other opportunities for low-income female wage earners could increase maternal income. On the other hand, policy interventions to improve the quality of nonmaternal care, such as publicly funded child care subsidies for all families (Azier, 2004) and more stringent state-level child care regulations, may complement maternal time with children, help women maintain their income, and free up family resources for additional investments in children that maximize adolescent outcomes. Specifically, our results suggest that related investments in children between birth and first grade might be especially beneficial for reducing problem behaviors.
Several limitations must be considered. First, despite the ability to control for a variety of family demographic and health characteristics, it is likely that sample selection and unobserved heterogeneity are present. A woman’s income is based on selection into employment, choice of occupation, and work intensity over time; these decisions may be influenced by unobserved factors, such as motivations, values, needs of the child, emotional climate of the family, parenting style, peer influences, and so on, that are related to child health and development over time and not captured in this data set; our inability to capture such variables may have led to spurious findings. Relatedly, we included average hours worked as a proxy for aspects of maternal availability, such as work role, job demands, and flexibility; however, it is possible that hours worked does not capture this construct in which case we may have induced some measurement bias into our analytical models. Second, as the analytical sample is composed of families in which women were employed during at least one data collection period, the results can be not generalized to families in which women never worked. However, sensitivity analyses that included all families regardless of maternal employment, the associations did not change between maternal employment and child outcomes. Third, the NICHD SECCYD data set comprises a somewhat homogeneous sample that might have limited the ability to detect associations. This sample is not nationally representative and therefore the results are not generalizable to the full U.S. population. For example, families who participate in a 15-year longitudinal study may have had the personal motivation and economic means to invest in their children thereby blunting the potential impact of maternal income in this sample. The observed effect of maternal income may have also been biased toward the null because sample attrition was associated with some indicators of lower socioeconomic status (i.e., lower income and younger maternal age) and poor maternal health; therefore, families who remained in the study over time may have had even more resources to invest in their children than those who were lost to follow-up. Fourth, the database did not categorize sources of “other family income” and thus we were unable to account for maternal income beyond income earned through employment; that being said, grouping these other sources of income as part of household income would have biased our estimates toward the null. Fifth, the data is fairly dated; however, we argue that the underlying mechanisms linking the hypothesized association between maternal income and adolescent outcomes, such as gender roles related to financial decision making, have likely not changed enough to render our results irrelevant for families in the United States today. Finally, the data set did not include information about parental supervision, time use, or specific investments in children, and thus we were unable to assess causal mechanisms.
Examining the association between maternal income and adolescent outcomes is plagued by methodological challenges, but the study was designed to enhance internal validity to the extent possible. At the same time, the methodological challenges limited our ability to conduct a confirmatory analysis. Despite these limitations, these findings contribute to an important social and economic question that has not been addressed in the extant scholarly literature among U.S. children.
Conclusions
This study contributes emerging evidence about the independent effects of maternal income on adolescent health and behavior in the United States. These results suggest that higher maternal income in early childhood, could have implications for improved behavioral outcomes at age 15. Ideally, the results will stimulate other scholars to generate new evidence to help shape public policies that support working families. In particular, longitudinal prospective studies are needed to address the limitations of unobserved bias and disentangle relations between maternal income, maternal employment, and child outcomes and to provide guidance for policy interventions that best support the well-being of U.S. families across the life-course.
Footnotes
Acknowledgements
The authors would like to acknowledge Courtney Van Houvten, Virginia Wang, Matthew Maciejewski, Santanu Datta, and Hollis Weidenbacher for their review and comments that greatly improved this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Grant Number 1 T42 OH008433 from the National Institute for Occupational Safety and Health (OSHA), Grant Number TL1 TR0042 from the National Institutes of Health, National Center for Advancing Translational Sciences (NCATS), and by a VA OAA HSR&D PhD Fellowship TPP 21-000. The funders of this work had no involvement in study design, data collection, analysis and interpretation, in writing the article, or in the decision to submit this article for publication.