
Abstract
Using data from the Mexican Migration Project, we evaluate the effects of documented and undocumented migration on the health of Mexican adults. Results suggest that documented and undocumented migrants are positively selected with respect to health in migrating to the United States and health status does not strongly predict selection into return migration back to Mexico. Among returned migrants, health deteriorates as the number of trips to the United States increases, with undocumented migrants experiencing an extra health penalty. While there is no continued decline on return to Mexico for undocumented migrants, they fare worse than returned documented migrants.
Keywords
In efforts to combat undocumented immigration over the past 30 years, the US government has militarized the border, heightened the internal surveillance of undocumented migrants, and assembled a complex legal infrastructure to curtail their access to rights and benefits (Massey, Durand, and Malone 2002; Nevins 2002). These punitive measures have raised questions about their influence on the well-being of undocumented migrants. Scholars have drawn attention to the traumas and abuses faced by undocumented immigrants across several dimensions, including at the border (Eschbach et al. 1999; Nevins 2002; Cornelius 2004), in the labor market (Rivera-Batiz 1999; Massey and Gentsch 2014; Passel and Cohn 2015), and in contact with the authorities (Phillips, Hagan, and Rodriguez 2006; Hagan, Rodriguez, and Castro 2011; Menjivar and Abrego 2012). Research has also detailed undocumented immigrants’ exclusion from mainstream institutions, including difficulties accessing health care (Kullgren 2003; Sullivan and Rehm 2005; Cavazos-Rehg, Zayas, and Spitznagel 2007). Owing to a scarcity of reliable data, however, less is known about their actual health outcomes.
This study examines the consequences of legal status for the health of Mexicans who have migrated to and returned from the United States. Returned migrants, the focus of this study, make up a significant, albeit selective, share of the broader Mexican migrant population. Prior to the escalation of border enforcement in the late 1980s, undocumented migration was overwhelmingly seasonal and circular. Between 1965 and 1985, an estimated 86 percent of undocumented entries were offset by departures (Massey and Singer 1995). Increased border enforcement in the 1990s and 2000s, however, reduced return migration to zero (Massey, Durand, and Pren 2015), and net migration turned sharply negative during the Great Recession of 2007–2009, when some one million immigrants left the country. Since 2009, net migration from Mexico has been zero or negative, with few migrants either departing for the United States or returning home (Gonzalez-Barrera 2015; Chort and de la Rupelle 2016).
We use data from the Mexican Migration Project (MMP), which provides unique insight into the health trajectories of Mexican migrants, both documented and undocumented, as well as nonmigrants. We build on earlier research on migrant health, including Ullman, Goldman, and Massey (2011), who used MMP data to compare the early-life and adult health of returned Mexican migrants and their nonmigrant counterparts. They found that migrants had better early-life health compared to nonmigrants but reported a greater health decline after returning from the United States. The authors, however, did not take into account legal status, cumulative migratory experience, or the total number of US trips, factors we explicitly examine here.
Our analytical strategy comprises two parts: Before being able to make claims about the impacts of migration and legal status on health, it is necessary to first account for possible health selection into both documented or undocumented migration and return migration. We address this issue by estimating an event history model to determine whether self-reported early-life health is associated with the likelihood of becoming a documented or undocumented migrant in the first place. We then estimate a series of cross-sectional models to investigate whether health reports are influenced by health selection into return migration, among other potential sources of measurement bias. After finding evidence that documented and undocumented migrants are equally positively selected with regards to early-life health into taking a first trip to the United States and finding little evidence for the return migration of sicker migrants, we then investigate the short- and long-term health effects of migration and legal status for returned migrants compared to nonmigrants. We do so by estimating a series of cross-sectional models to track changes in self-reported health across three key periods: (1) from just prior to the first migration to just after the latest return to Mexico (to measure immediate changes in health for returned migrants), (2) from just after the latest return to Mexico to the survey date (to measure continued changes in health for returned migrants), and (3) from early life at age 14 to the survey date (to measure overall changes in health, comparing returned migrants and nonmigrants).
Undocumented Status and Health
Undocumented status potentially undermines health in two ways: by creating legal barriers to the receipt of adequate health care and exposing migrants to greater health risks. With respect to legal barriers, the US government prohibits access to public social services, health insurance, and non-emergency medical care not only for undocumented immigrants but also for legal residents under certain circumstances (Kullgren 2003; Ortega et al. 2007; Wallace et al. 2013). Undocumented migrants are ineligible for government-sponsored health insurance and tax credits under the 2010 Affordable Care Act, which maintains and in some respects raises the barriers to medical care first institutionalized with the 1996 Personal Responsibility and Work Opportunity Act (Mulligan and Castañeda 2017). Although undocumented migrants are free to purchase health insurance from private venders, the cost is prohibitive for most. Furthermore, fears of apprehension and deportation discourage contact with health care providers and insurance companies. Surveys, for example, show that undocumented migrants exhibit lower rates of insurance coverage, fewer physician visits, and less access to usual care providers than documented migrants or citizens (Ortega et al. 2007; Chavez 2012; Vargas Bustamante et al. 2012; Gelatt 2016).
In addition to creating formal barriers to health care, unauthorized status undermines health by differentially channeling immigrants into hostile contexts of reception, particularly in the labor market (Portes and Rumbaut 2006). The 1986 Immigration Reform and Control Act drove the practice of undocumented hiring underground, relegating the undocumented workforce to jobs with higher risks of injury, disability, and psychological trauma (Phillips and Massey 1999; Walter, Bourgois, and Loinaz 2004; Orrenius and Zavodny 2009; Cho and Smith 2013; Hall and Greenman 2015; Passel and Cohn 2015). With no legal recourse to unfair treatment, undocumented workers are uniquely exposed to employment abuses (Fussell 2011; Bernhardt, Spiller, and Polson 2013; Lee 2014). They earn significantly lower wages than their legal counterparts, especially in sectors where undocumented workers are prevalent (Rivera-Batiz 1999; Hall, Greenman, and Farkas 2010; Gentsch and Massey 2011; Massey and Gentsch 2014).
Illegality also pushes immigrants into segregated, poorly resourced, and dangerous neighborhoods. Hall and Stringfield (2014), for instance, have shown that a greater prevalence of undocumented migrants in new destination areas predicts higher levels of Mexican segregation. Across US metropolitan areas more generally, Hispanic segregation is strongly predicted by animus against undocumented migrants (Rugh and Massey 2014).
Lastly, the everyday challenges of managing the stigmatization and risk of living without documents put considerable strain on mental health. Qualitative studies have illustrated how the specter of deportation provokes fear, uncertainty, helplessness, stress, marginality, and a diminished sense of self-worth among undocumented migrants (Coutin 2000; De Genova 2002; Chavez 2012; Menjivar and Kanstroom 2013). The repercussions of mass deportation reverberate through family and social networks, separating and traumatizing households and communities (Menjivar 2006; Brabeck and Xu 2010; Dreby 2012). Taken together, these multiple forms of exclusion and risk suggest considerable potential for undocumented immigrants to display negative health outcomes.
Implications of Migrant Health Selection
Several methodological issues complicate the task of validating the connection between undocumented status and poor health using survey data, the first of which is the likely positive selection of people into migration on the basis of health. The “healthy immigrant effect” is a common explanation for the paradox that immigrants — particularly those of Latino, and especially Mexican, origin — display lower mortality and morbidity rates than non-Hispanic whites despite lower levels of education and socioeconomic attainment. While early research found limited or no support for the healthy migrant effect (Abraido-Lanza et al. 1999; Akresh and Frank 2008; Rubalcava et al. 2008), more recent work has detected a positive association between good health and likelihood of US migration (Ullman, Goldman, and Massey 2011; Riosmena, Wong, and Palloni 2013; Martinez, Aguayo-Tellez, and Range-Gonzalez 2015; Riosmena, Kuhn, and Jochem 2017). Using the MMP’s life history data, we not only account for potential health selection into migration but also assess whether this selection differs by legal status.
A second methodological issue is potential selectivity into return migration. The “salmon bias” hypothesis, another explanation for the Hispanic mortality paradox, posits that unhealthy migrants no longer able to work are compelled to return home to receive medical treatment, seek family support, and perhaps die. Some previous research does indeed link poor health with return migration (Palloni and Arias 2004; Turra and Elo 2008; Ullman, Goldman, and Massey 2011; Riosmena, Wong, and Palloni 2013; Arenas et al. 2015). If the salmon bias were to hold true for our sample, this could result in an overestimation of any deleterious effects of migration and legal status that we might find on the health of Mexicans who returned home. We explore potential health selection in return migration, along with other potential sources of measurement bias, using cross-sectional MMP data.
Lastly, migrants who participated in the MMP are those who survived the migration experience and lived to the survey date, creating another source of potential selection bias. If we assume that the sickest migrants die earlier than others, either in the United States or at home, then returned migrants’ estimated health may be biased upward, which is in a conservative direction with respect to our hypotheses.
Data and Methods
Despite these issues, MMP data are well suited in other ways to investigating connections among migratory experience, documentation, and health over the life course since they allow for the construction of health and mobility trajectories for both legal and unauthorized migrants as well as persons who never left Mexico. Beginning with four community surveys in 1982, the MMP has since 1987 annually surveyed representative samples of three to five Mexican communities and their US branch settlements. Using semi-structured interviews, field workers gather detailed information on the characteristics and behaviors of households and their members, including data about each person’s first and last trips to the United States, and aggregate information about the community itself. While the survey is cross sectional, interviewers compile yearly life histories of household heads, which include complete international migration and border-crossing histories.
Questions about the health of household heads were incorporated into the MMP in 2007. Household heads’ health is retrospectively reported for the following points in their lives, which we use to construct the dependent variables for this analysis: early life at age 14, just prior to their first US trip (for migrants), just after their last trip to the United States (for returned migrants), and at the time of the survey (including both migrants and nonmigrants). At each timepoint, health is rated as poor, regular, good, or excellent. Owing to small frequencies, we collapse poor and regular responses into a single category henceforth labeled poor, producing a three-level ordinal rating for quality of health.
Before proceeding with our analysis, we flag three potential sources of measurement error that come with using the MMP’s retrospective health reports, the first being recall bias due to memory lapses. Several investigations into self-rated health’s merits have concluded that despite its subjective basis, it is a remarkably accurate predictor of mortality (Mossey and Shapiro 1982; Bound 1989; Idler and Benyamini 1997; DeSalvo et al. 2005; Jylha 2009; Schnittker and Bacak 2014). Retrospective evaluations, however, are vulnerable to recall error — especially among the elderly and those who migrated or returned well before the survey date (Schuman and Presser 1981). Furthermore, perceptions of past health may be endogenous to current health status.
The second potential source of error arises from relying on estimations of the household head’s health by another household member — who, in the MMP, is typically the spouse when the household head is not available to be interviewed. This is the case for 54.3 percent of the sample. Upon approaching each household, enumerators inquire as to who is the household head, with the goal of soliciting him or her to respond to the MMP questionnaire. For instances in which the household head is not available, another household member is asked to act as the informant. It is usually the wife within the household who is administered the survey when the identified head is not available since the majority (85.1%) of households in the sample are male-headed and males are more likely to be outside the house during the daytime. Ayalon and Covinsky (2009), using nationally representative longitudinal data of elderly married couples, found that spouse-rated health is just as strong a predictor of mortality as self-rated health. However, spouses could have limited purview of their partners’ health conditions in the past, particularly for couples with shorter common histories or if significant time was spent apart due to migration.
Third, migrants and nonmigrants may be evaluating their health vis-à-vis different reference populations, compromising the comparability of their health ratings. Informants with migration experience may measure health in relation to other US migrants or native-born Americans, whereas nonmigrant informants would presumably be more likely to use fellow Mexicans as their reference group. Regrettably, data limitations prevent us from conclusively determining systematic differences in standards along which health is compared or other considerations that go into the subjective process of reporting on one’s own or another person’s quality of health.
We explore how recall length and informant status may affect health ratings in a series of multinomial logistic regressions described in the following. To preview our findings, we find that recall length and informant status do appear to influence health reports and thus control for these factors in our study’s main analyses.
Our final sample consists of 8,067 household heads from 46 Mexican communities surveyed between 2007 and 2016 who migrated at the age of 15 or older between 1940 and 2015. These 8,067 household heads contribute 248,929 person-years of information to the event history file. Of these, 228,290 were contributed by 6,235 nonmigrants observed from age 15 to the survey date. An additional 16,790 person-years were contributed by 1,542 undocumented migrants and 3,849 by 290 documented migrants, both observed from age 15 up to the year of their first US trip. 1 Our cross-sectional file contains 6,235 nonmigrants, 249 returned documented migrants, 1,283 returned undocumented migrants, 41 documented migrants still in the United States, and 259 undocumented migrants still in the United States. After investigating health selection and before analyzing the health effects of migration and legal status, we restrict our sample to nonmigrants and migrants who had returned to Mexico by the survey date, thus excluding the 300 migrants still in the United States at the survey date.
Our analytical strategy comprises the following parts, the first two questions dealing with health selection and the remaining questions concerning the short- and long-term consequences of migration and legal status for health: (1) Investigating possible healthy migrant effects: Among Mexicans, is early-life health associated with initial selection into documented or undocumented migration to the United States? (2) Investigating possible salmon bias: Does health after migration predict later selection into returning to Mexico? (3) Immediate health effects of migration and legal status: Among returned migrants, is undocumented status associated with an increase in the likelihood of reporting poor or worsened health from just before the first US trip to just after the last US trip? (4) Continuing health effects of legal status: Among returned migrants, is undocumented status associated with an increase in the likelihood of reporting poor or worsened health from just after the last US trip to the survey date? (5) Overall changes in health, comparing returned migrants and nonmigrants: Holding early-life health constant, is prior documented or undocumented migration experience associated with a greater likelihood of reporting worse health at the survey date compared to nonmigrants?
To determine the degree to which respondents are selected into US migration on the basis of early-life health, we create a retrospective event history file. Drawing from the MMP life history module, we construct a longitudinal data set following each household head year by year from age 15 to the year of the first US trip or the survey year if no trips were reported. We estimate a multinomial logistic regression equation to predict whether in any given person-year a household head departed for the United States with valid documents, without valid documents, or not at all, given self-reported health at age 14 and other predictors.
We control for the health risk factors of height in centimeters, weight in kilograms, and whether the respondent ever smoked. Short height is taken to indicate poor nutrition and stunting during early childhood (Hizli et al. 2007) and is a harbinger of being overweight later in life (Popkin, Richards, and Montiero 1996), a condition that independently undermines health (Weitoft, Eliasson, and Rosén 2008). Smoking’s deleterious effects on health and mortality are widely known (US Department of Health and Human Services 2004). These variables are time-invariant and reflect the respondent’s condition at the time of the survey and thus admittedly constitute imperfect controls for health risk factors experienced over the life course. We also control for gender since despite the feminization of migration from other parts of the world, men continue to be more likely than women to migrate to the United States from Mexico (Passel, Cohn, and Gonzalez-Barrera 2012). There are also considerable gender disparities in health in Mexico, with females displaying higher life expectancies than males (79.4 versus 74.5 years of age in 2015). 2
We control for the time-varying risk factors of age, years of education, household wealth, and municipal population. The risks of morbidity and mortality vary strongly with education, with more educated people having a greater likelihood of adopting healthier behaviors and thus achieving healthier outcomes (Cutler and Lleras-Muney 2010). Home ownership, a measure of household wealth, is a dummy coded as 1 if the respondent had acquired at least one residential property during or prior to a given person-year and 0 otherwise. Urban versus rural residence is measured by the natural log of the population in the respondent’s municipality. Municipal population figures come from the decennial Mexican censuses of 1950 through 2010, with intercensal years estimated using linear interpolation. 3
Given that migrant network connections are among the strongest predictors of migration (Massey and Espinosa 1997; Massey and Aysa-Lastra 2011), we control for two measures of social capital. The US migration of at least one parent or sibling by the person-year in question is included as a dummy variable. Migration prevalence is indicated by the ratio of community members with US migrant experience to the total number of community members alive in any given person-year (Massey, Goldring, and Durand 1994). Finally, we include a dummy variable for whether the household head was the informant.
After assessing whether selection into US migration differs by early-life health, we assess whether our findings will be biased by selective return migration, among other factors that may lead to measurement error. The rest of our analyses rely on cross-sectional data from the MMP. In these analyses, we define documented migrants as those who took both their first and last US trips with valid papers, undocumented migrants as those who took either their first or last US trip without valid documentation, and nonmigrants as those who never migrated to the United States. Among undocumented migrants, 87.5 percent were undocumented on both trips or took only one trip, 10.8 percent were undocumented on their first trip but documented on their last trip, and 1.6 percent were documented on their first trip but undocumented on their last trip. Thus, the vast majority of undocumented migrants spent all their time in the United States in undocumented status, and 12.4 percent spent at least some of their time in the United States without documents. Since a portion of those who are ultimately coded as having a history of being unauthorized were at some period of time protected from illegality’s risks and harms, it is reasonable to assume that any findings about the deleterious impacts of unauthorized status in this study are conservative.
Using the full cross-sectional data set, we estimate multinomial logistic regressions predicting health for each juncture measured in the MMP — early life at age 14, just prior to the first trip, just after the latest return (or during the latest trip for household heads still in the United States when surveyed), and at the survey date — using good health as the reference category. For the models predicting health just before the first departure to the United States, health just after return from the last trip (or during the latest trip for migrants still in the United States), and current health, we include a dummy variable for whether the respondent is still in the United States at the survey date. We also control for informant status for all models, along with the number of years that have elapsed since each timepoint for which health is measured (excluding the model for health at the survey date since recall bias is no longer a factor then). We include the same controls as the model predicting selection into migration as well as a factor variable for migrant status to compare nonmigrants (reference group) with documented and undocumented migrants. In preliminary analyses, we estimated annual aggregate probabilities of taking a first undocumented US trip and returning from a last undocumented trip and included them as time-varying covariates to control for possible changes in the selectivity and nature of undocumented migration over time, but these variables proved to be insignificant and were dropped from subsequent analyses.
As we elaborate on in the results section, we find little evidence of the salmon bias and therefore restrict subsequent analyses to the impacts of migration and legal status for returned documented and undocumented migrants versus nonmigrants. However, we do find evidence that recall length and informant status have an influence on health reports.
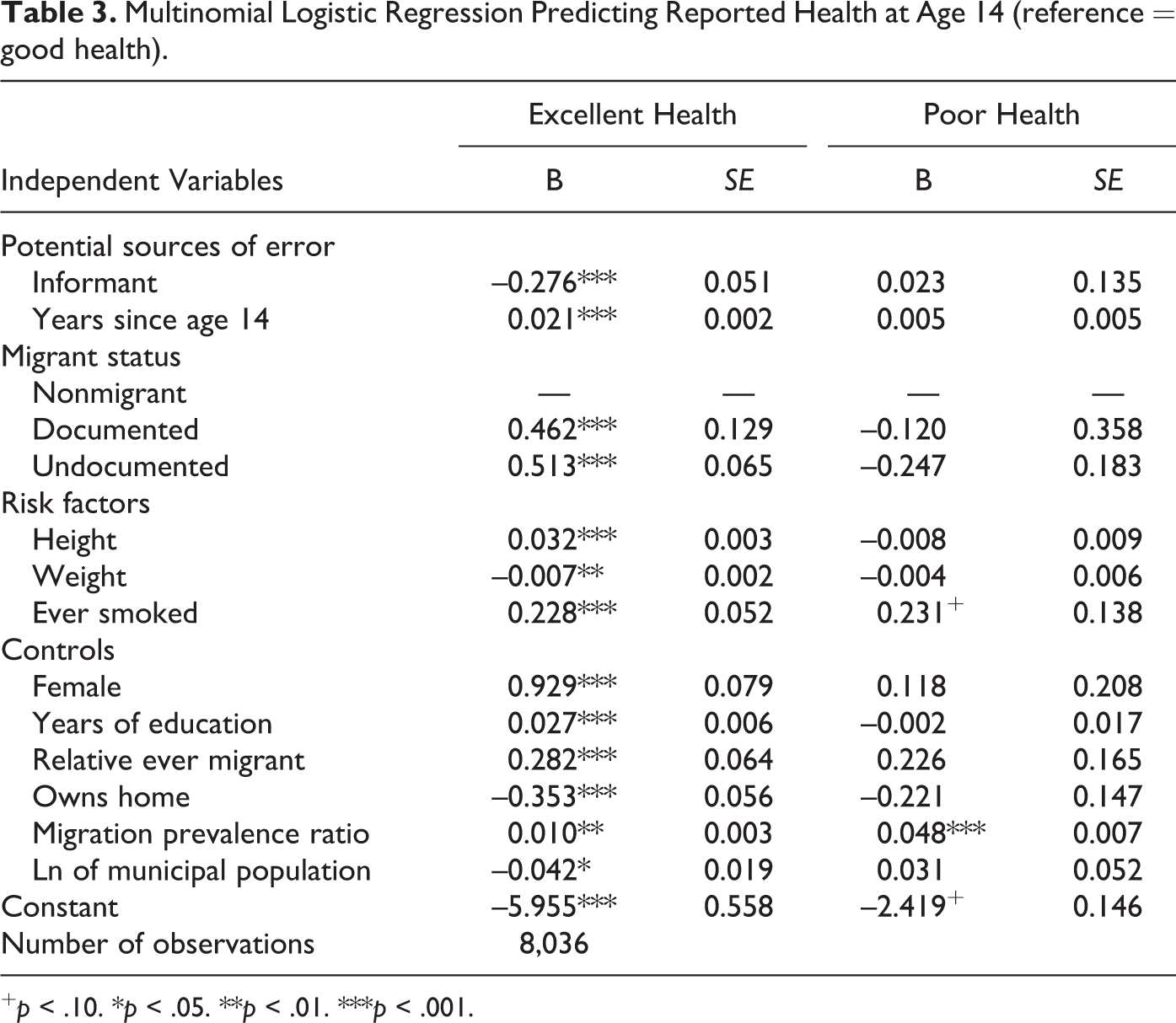
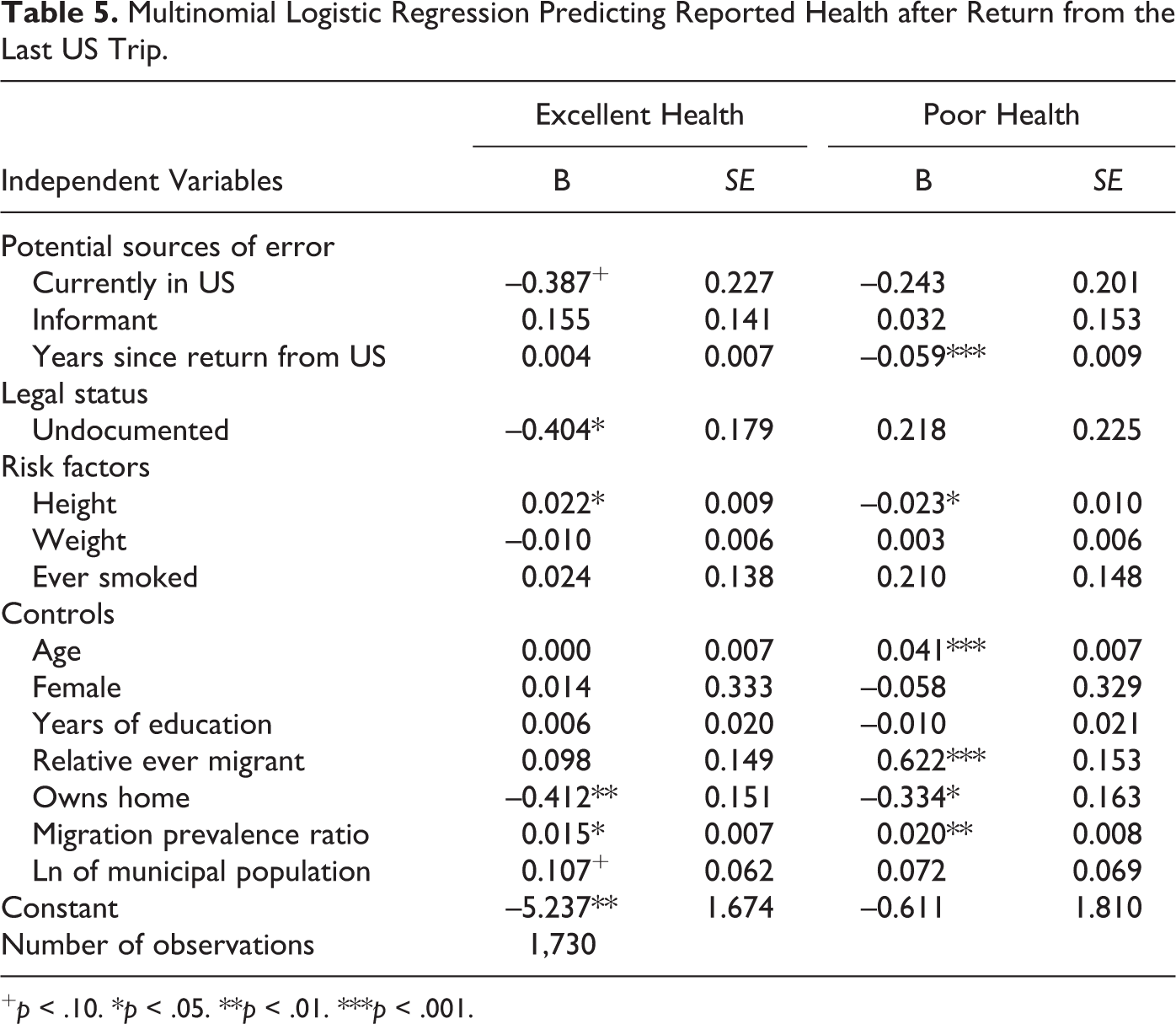
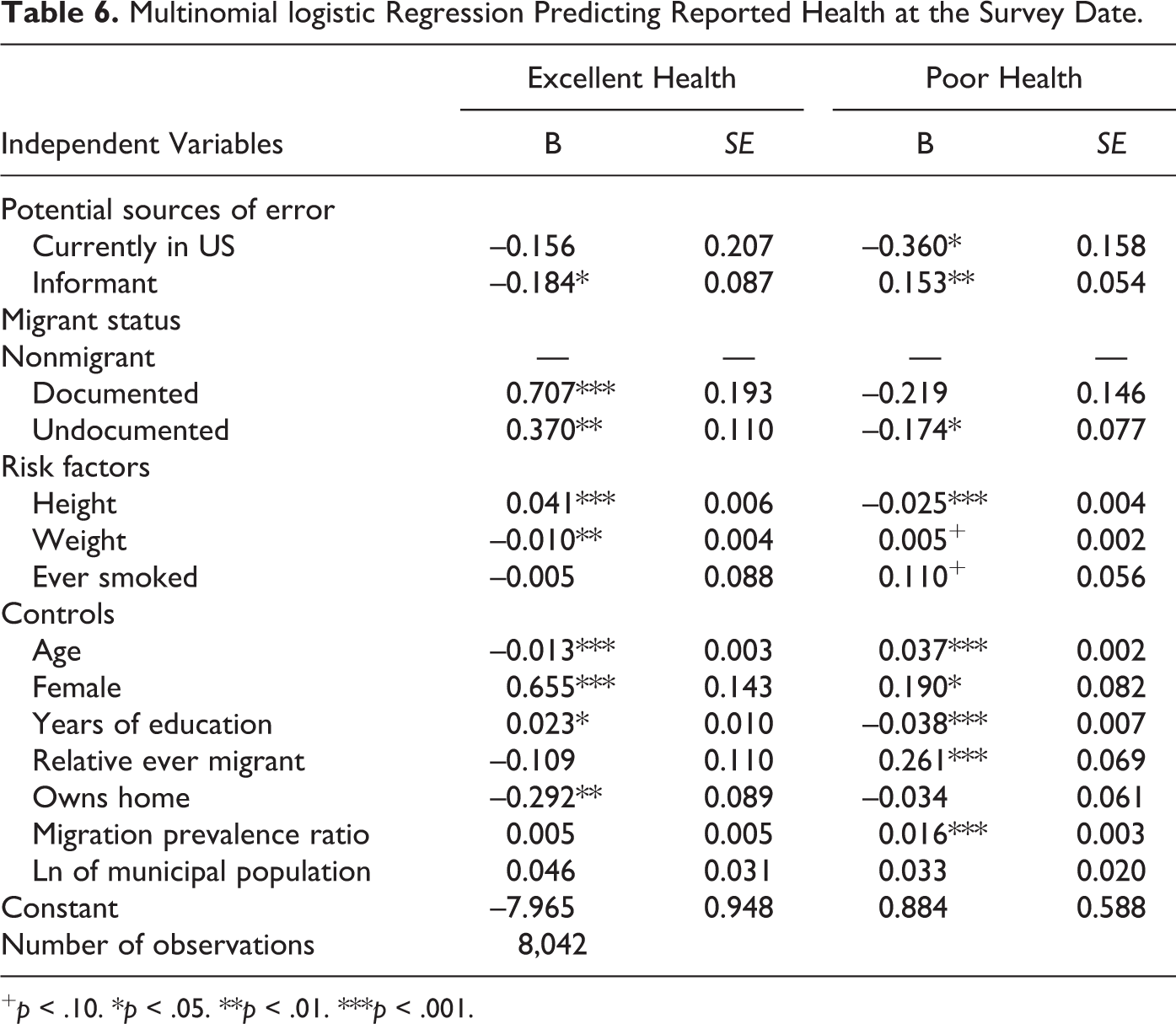
Concerning informant status, self-rated reports of health at age 14 and at the survey date are more conservative than other-rated health reports, with household head informants being less likely to report excellent as opposed to good early-life and current health (Tables 3 and 6). Conversely, being an informant is associated with a higher likelihood of reporting excellent health before migration (Table 4) but is not a significant predictor of health status after migration (Table 5). As for recall length, number of years since the time interval in question is associated with more favorable health reports. Likelihood of reporting excellent early-life health increases with years elapsed since age 14 (Table 3). Likelihood of reporting excellent pre-migration health increases with years since departure to the United States, which corresponds with a decrease in the likelihood of reporting poor health prior to migration (Table 4). A similar trend persists for health after migration, with years since return predicting a lower likelihood of reporting poor health (Table 5). We therefore control for informant status and years elapsed since the timepoint in question in our models controls for these sources of measurement error.
After inquiring into potential selection and measurement biases, we turn to our main inquiry into the links between migration, legal status, and health, based on cross-sectional MMP data that are limited to nonmigrants and migrants back in Mexico at the survey date. To examine the links between undocumented status and health from pre- to post-migration (immediate effects) and from post-migration to the survey date (continuing effects), we estimate two models for each time interval: a simple logistic regression equation predicting whether reported health worsened over time and an ordered logistic regression model predicting health at the end of the interval given health status at its beginning. The latter model enables us to infer the directionality and size of migration’s effect on health by observing changes in health relative to a clear baseline. Finally, we estimate an ordered logistic regression model for all respondents to predict health at the survey date given health at age 14 to assess overall changes in health.
As in the event history analysis, the cross-sectional models control for the risk factors of height, weight, smoking, age at the end of the time interval, gender, education, and the natural log of the municipal population. We also control for the total number of US trips taken and cumulative years of US experience to estimate the degree to which different “dosages” of migration yield divergent health outcomes. These variables, which are moderately collinear (r 2 = .50), assess two distinct risks to migrant health: exposure to the specific health risks of undocumented border crossing and exposure to the more general health risks of life in the United States.
Models predicting health at the time of the survey include three indices of material well-being at the survey date, which are likely strongly influenced by savings and remittances generated through migration. The first is a zero to 14 count of the following amenities or goods present in the household: a non-dirt floor, running water, sewage facilities, stove, refrigerator, washing machine, sewing machine, radio, television, stereo, telephone, cellphone, Internet, and computer. The second is a dummy variable indicating whether or not the household’s current dwelling is owned. As a measure of household density or crowding, we include the ratio of the number of household members to the number of rooms in the home.
Finally, in addition to controlling for informant status for all models, we adjust for recall bias by controlling for the number of years that have elapsed since both the first departure and latest return for models investigating the period from before to after migration and for the number of years since the latest return for the models investigating the period from after migration to the survey date.
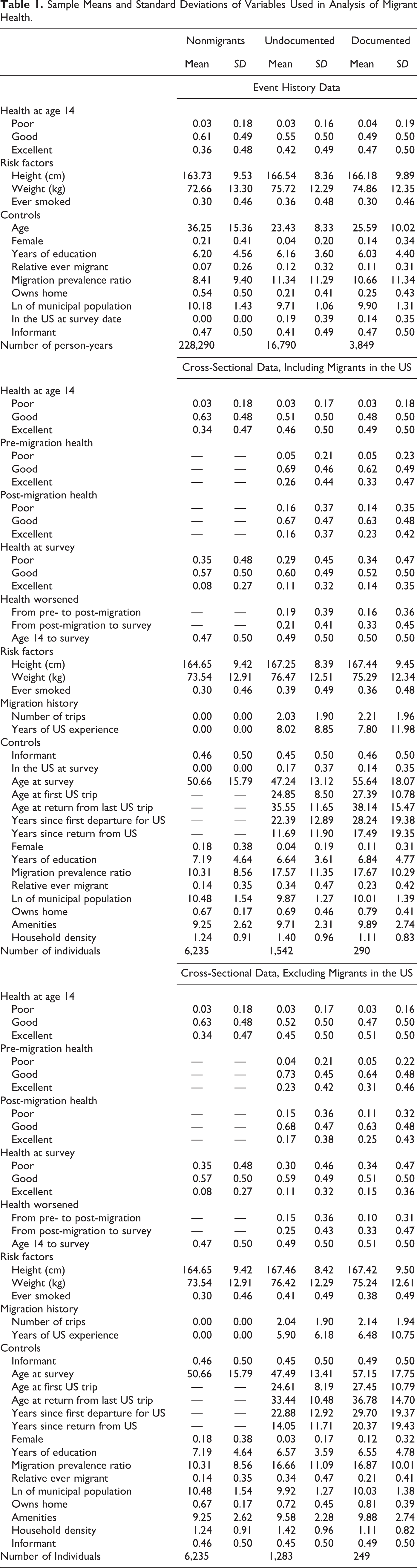
Means and standard deviations for event history and cross-sectional data sets (both including and excluding migrants still in the United States at the survey date) are presented in Table 1. We use the Amelia II package in R to multiply impute missing values (Honaker, King, and Blackwell 2011). Information about the frequency of missing data for each variable is provided in the Appendix. Compared with list-wise deletion, multiple imputation produces results with less biased estimates and smaller standard errors. We create 10 complete data sets across which observed values are held constant, with missing values imputed using the “expectation-maximization with boot-strapping” algorithm developed by Honaker and King (2010), thereby generating distributions that reflect uncertainty with respect to missing data.
Sample Means and Standard Deviations of Variables Used in Analysis of Migrant Health.
In our analyses of health outcomes, we exclude observations for which the dependent variable was missing. Although all health variables are included in the imputation model, we do not use imputed Y values at the analysis stage. This practice produces more efficient point estimates, smaller standard errors, and smaller confidence intervals than if observations with imputed Y values were included in the model (Von Hippel 2007). As indicated in the Appendix, only 0.3 percent of cases were missing health at the survey date, 1.4 percent were missing pre-migration health, and 1.3 percent were missing post-migration health values. The exclusion of cases with missing dependent variables explains the small differences in sample size across the cross-sectional models. The post-imputation deletion step is not necessary in the event history model because we observed no missing values in the dependent variable. We produce our analyses using the Zelig package in R, which estimates results within each of the 10 imputed data sets and then combines them according to Rubin’s rules (Rubin 1987).
As shown in Table 1, the cross-sectional summary statistics (including migrants in the United States at the survey date) offer prima facie evidence that migrants are indeed self-selected on the basis of health. Whereas only 34 percent of nonmigrants reported their health at age 14 to be excellent, the figure was 46 percent for undocumented migrants and 49 percent for documented migrants, χ2(4, N = 8,067) = 94.966, p < .001. In addition, migrants were taller on average than nonmigrants, with respective heights of 167.3 cm and 167.4 cm for undocumented and documented migrants, compared with 164.7 cm for nonmigrants. However, this apparent initial health advantage is offset somewhat by the cumulative effects of smoking over the life course, as around 39 percent of undocumented and 36 percent of documented migrants reported having ever smoked, compared to just 30 percent of nonmigrants.
Focusing on returned migrants, the cross-sectional data also offer prima facie evidence for a greater decline in health among undocumented compared to documented migrants after having lived and worked in the United States. For returned undocumented migrants, the share reporting excellent health falls from 45 percent at age 14 to 17 percent post-migration. In contrast, the share reporting excellent health among documented migrants fell from 51 percent to 25 percent over this interval. At the survey date, around one-third of respondents in each group reported poor health, though documented migrants evinced the highest proportion, reporting excellent health at 15 percent, compared to undocumented migrants at 11 percent and nonmigrants at 8 percent. Chi-square values for cross-tabulations between migration status and each health measure are statistically significant.
The greater decline in health among returned undocumented migrants occurred despite their having accumulated 0.6 years fewer years living in the United States, on average, than those who had valid documents (around 5.9 versus 6.5). Both returned documented and undocumented migrants had accumulated just over 6.5 years of education, lower than nonmigrants who reported 7.2 years on average. Nonmigrants were more likely than migrants to live in urban areas, with a mean municipal population size of 143,366. In contrast, documented migrants’ municipalities had a mean population size of 81,453, while undocumented migrants were most likely to come from smaller communities, with a mean population size of 49,530. At the survey date, returned documented migrants were older (57.2 years) than returned undocumented migrants (47.5 years) and nonmigrants (50.7 years).
In terms of material well-being, returned migrants were much more likely to be homeowners than nonmigrants, as one would expect given their greater earning power. Whereas only 67 percent of nonmigrants owned homes at the time of the survey, the figures were 81 percent and 72 percent for returned documented and undocumented migrants, respectively. Likewise, the average number of consumer goods and amenities possessed at the time of the survey was greatest for returned documented migrants (9.9), followed by returned undocumented migrants (9.6) and nonmigrants (9.3). Household density was greatest for returned undocumented migrants (an average of 1.4 persons per room) compared with nonmigrants (1.2 persons per room) and returned documented migrants (1.1 persons per room).
Means computed across person-years in the event history file generally replicate the patterns observed at the survey date while providing additional information about respondents’ migration-facilitating social capital. Unsurprisingly, both documented and undocumented migrants reported greater access to migrant networks than nonmigrants. Whereas in the average person-year only 7 percent of nonmigrants reported having a parent or sibling with US experience, the figure was 12 percent for undocumented and 11 percent for documented migrants. Similarly, across person-years, the average nonmigrant lived in a community in which only 8.4 percent of all persons had been to the United States, while 11.3 percent of undocumented migrants’ community members had been north of the border, compared with 10.7 percent for documented migrants.
Health Selectivity, Potential Bias, and Migration
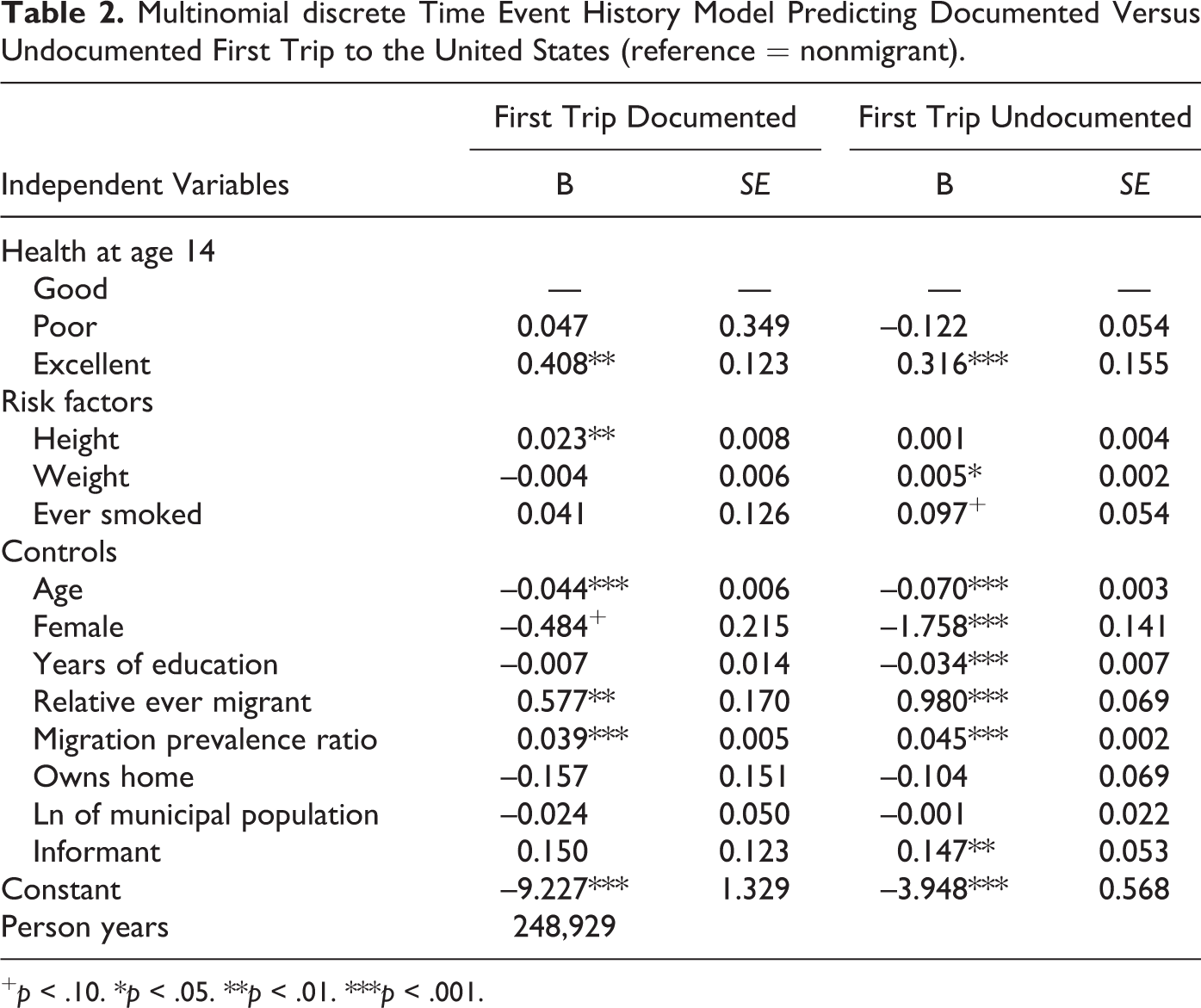
We first assess whether migrants and nonmigrants systematically differ with regard to early-life health and whether there is differential selectivity by legal status among migrants. Table 2 presents the results of a discrete time event history analysis that used multinomial regression to predict the likelihood of departing for the United States in documented or undocumented status given health at age 14, health risk factors, and other controls. Consistent with prior research (Akresh and Frank 2008; Ullman, Goldman, and Massey 2011), our estimates indicate that US migrants are positively selected with respect to health. Reporting excellent health at age 14 increases the odds of a documented departure by 50 percent (exp(0.408) = 1.503) compared to those reporting good or poor health at that age (p < .01). Likewise, excellent early-life health increases the odds of undocumented departure by 37 percent (exp(0.316)=1.362, p < .001). These two values are not statistically different from one another, suggesting that documented and undocumented migrants are equally well selected with respect to health.
Multinomial discrete Time Event History Model Predicting Documented Versus Undocumented First Trip to the United States (reference = nonmigrant).
+ p < .10. *p < .05. **p < .01. ***p < .001.
As other studies have found (Massey and Espinosa 1997; Massey and Aysa-Lastra 2011), migrants to the United States are negatively selected with respect to age and positively selected with respect to social capital from kinship ties to migrants and a high prevalence of migrants in the community. However, whereas education is negatively associated with taking a first undocumented trip (in keeping with prior studies — see Massey and Espinosa 1997), it does not predict the likelihood of taking a first documented trip.
Having determined that documented and undocumented migrants are equally selected into migration on the basis of health, we turn to assess potential sources of bias in the reporting of health itself. As shown in Table 3, in reporting health at age 14, there are two potential sources of error: misreporting by informants and recall bias from memory lapses. While the likelihood of poor as opposed to good health is unaffected by who provided the health assessment or time since the assessment’s target date, we see that reporting excellent health is significantly less likely when the assessment was made by an informant rather than by the household head and that it grows significantly more likely as the amount of time since the target date of 14 increases, suggesting the potential for both informant bias and recall bias.
Multinomial Logistic Regression Predicting Reported Health at Age 14 (reference = good health).
+ p < .10. *p < .05. **p < .01. ***p < .001.
Among US migrants, reports of health prior to the first trip likewise may be biased owing to informant error and recall error. As shown in Table 4, we see that informants are indeed more likely to report excellent health before the first trip than household heads, indicating potential informant bias. In addition, the likelihood of reporting excellent health rises with years since the date of departure, and the likelihood of reporting poor health falls with years since this date, again suggesting possible recall bias. Reports on health by migrants may also be influenced by the salmon bias. If migrants with poor health are more likely to return to Mexico, we might expect those still in the United States to report systematically better health than those who have returned. Although migrants still in the United States at the time of the survey are in fact more likely to predict excellent as opposed to good health, they are also significantly more likely to report poor as opposed to good health. Moreover, the sizes of the two coefficients are not significantly different from each other. Thus, we do not see systematic evidence for the salmon bias in reports of pre-migration health.
Multinomial Logistic Regression Predicting Reported Health Prior to the First US Trip.

+ p < .10. *p < .05. **p < .01. ***p < .001.
Reports of post-migration health are likewise potentially influenced by informant bias, recall bias, and salmon bias. As shown in Table 5, however, we do not see any evidence of informant bias in assessments of post-migration health. Moreover, being in the United States at the time of the survey is unrelated to the likelihood of reporting poor post-migration health and only marginally related to the likelihood of reporting excellent post-migration health (p < .10). In addition, the effect is in the opposite direction (negative) than one would expect if a salmon bias were influencing health assessments. Thus, we do not see much evidence of informant bias or salmon bias. We do see, however, that the likelihood of reporting poor post-migration health significantly decreases with time since the date of the return trip, suggesting the potential existence of recall bias.
Multinomial Logistic Regression Predicting Reported Health after Return from the Last US Trip.
+ p < .10. *p < .05. **p < .01. ***p < .001.
Finally, reports of health at the survey date are obviously not threatened by recall bias but might be subject to either informant bias or salmon bias. As shown in Table 6, we do find evidence for the former, as informants are more likely to report poor health and less likely to report excellent health than household heads. The evidence for salmon bias is mixed. Although those migrants still in the United States are neither more nor less likely to report excellent health (and the effect is negative, contrary to the salmon bias hypothesis), they are significantly less likely to report poor health (p < .05), which is consistent with the potential existence of a salmon bias.
Multinomial logistic Regression Predicting Reported Health at the Survey Date.
+ p < .10. *p < .05. **p < .01. ***p < .001.
In summary, we have shown that documented and undocumented migrants are equally positively selected into migration on the basis of excellent health at age 14 and that health reports at different times in the past are potentially influenced by informant bias and recall bias, prompting us to include controls for informant status and time since health assessment in subsequent models. Evidence for the influence of salmon bias brought about by the selective return of migrants with poor health and the selective US settlement of migrants with excellent health is less compelling, however. The health status of migrants who are still in the United States on their last trip is not significantly different from the health status of those who have returned from their last trip (p > .05). We therefore move forward with our assessments of changes in health before and after migration to the United States among migrants who have returned to Mexico, which is the subject of the next section.
Health Effects of US Migration by Legal Status
The left columns of Table 7 present the results of a logistic regression equation predicting whether a decline in health occurred from just before the first US trip to just after the last trip given migrant status, total number of trips, cumulative years of US experience, and relevant controls. Like Ullmann, Goldman, and Massey (2011), we find that migration to the United States is bad for one’s health, but we also detect a dosage effect in which more US trips and years of US experience increase the likelihood of a decline in health from pre- to post-migration. With each successive trip, the odds of a decline in health rise by around 12.7 percent (determined here and thereafter by taking the exponent of the regression coefficient). Each year of US experience is associated with a 5.4 percent increase in odds of experiencing worsened health during this interval.
Logistic Regression Models Predicting Decline in Health Pre- to Post-migration and Health Just After Last US Trip.a
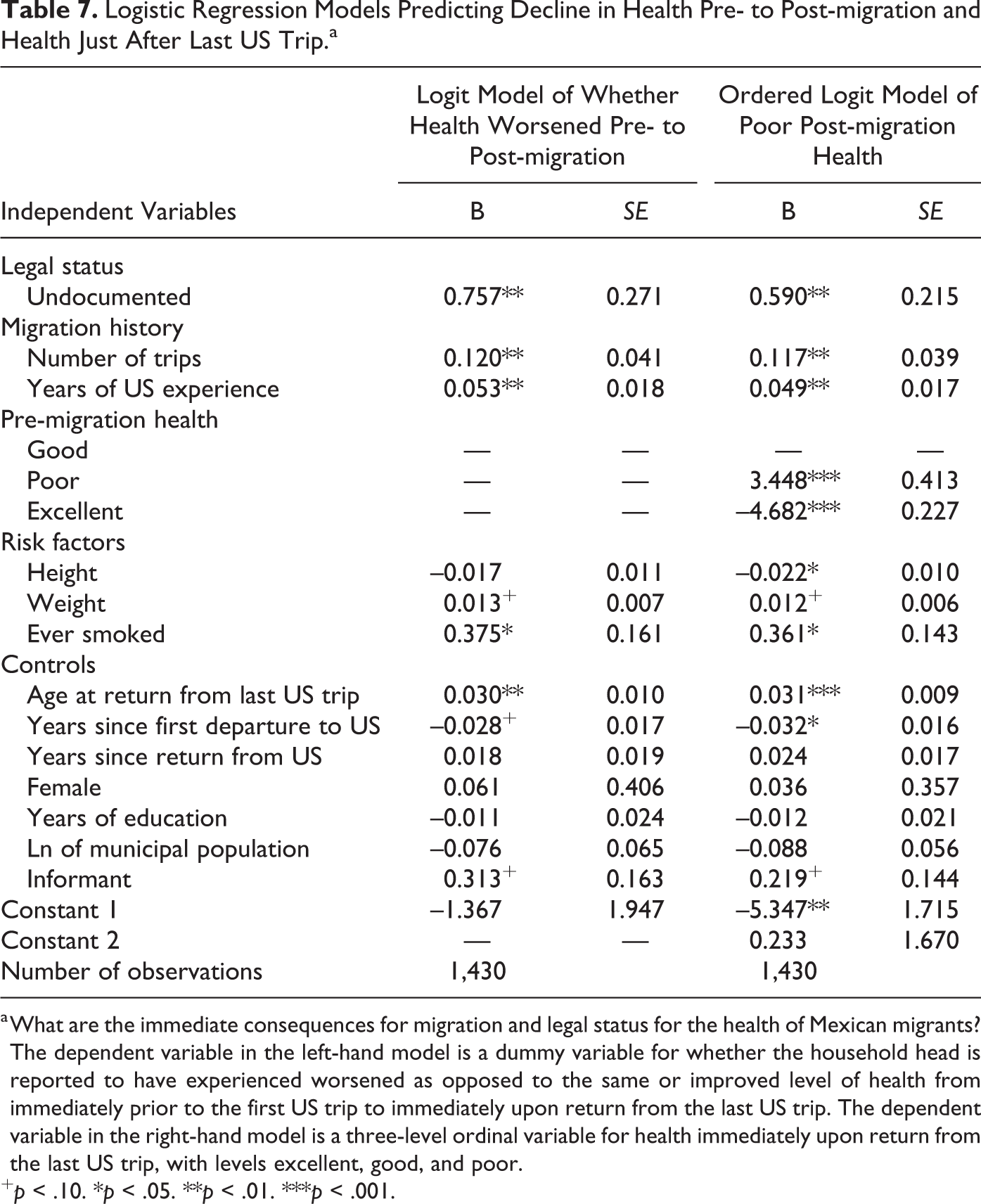
a What are the immediate consequences for migration and legal status for the health of Mexican migrants? The dependent variable in the left-hand model is a dummy variable for whether the household head is reported to have experienced worsened as opposed to the same or improved level of health from immediately prior to the first US trip to immediately upon return from the last US trip. The dependent variable in the right-hand model is a three-level ordinal variable for health immediately upon return from the last US trip, with levels excellent, good, and poor.
+ p < .10. *p < .05. **p < .01. ***p < .001.
Holding constant the number of trips and years of US experience, we find that returned undocumented migrants are more likely than returned documented migrants to experience worsened health, with the odds of reporting poorer health after migration being 2.1 times greater for the former compared to the latter. Thus, not only does health decline as a result of migration to the United States generally, worsening with each successive trip, but the odds of experiencing a decline in health are greater for the undocumented. Beyond these effects, a decline in health is also predicted by greater age upon returning from the United States and having a history of smoking.
The right columns show results of an ordered logit model predicting migrants’ health on returning from the last trip, given pre-migration health, legal status, number of trips, US experience, and controls. Consistent with the prior model, the likelihood of poorer health is significantly predicted for all migrants depending on the number of total trips taken, with worsened health significantly more likely for undocumented migrants. The odds of experiencing poorer health increase by 12.4 percent with each successive US trip and by 5.0 percent with each successive year spent in the United States and are 80 percent greater for undocumented than documented migrants. As one would expect, worsened health is also predicted by greater age upon return from the United States, ever having smoked, and marginally by greater weight, and worsened health is negatively predicted by greater height and years of education.
We now investigate whether legal status continues to have a negative effect on migrants’ health between coming back to Mexico and the survey date. The left columns of Table 8 show results of a logistic regression predicting the likelihood of a decline in health from just after the final US trip to the survey date, controlling for height, weight, smoking, gender, age, education, and the natural log of the municipal population size. This model additionally controls for home ownership, amenities, household density, years since return from the United States, and informant status. Unlike the prior regressions, this model reveals no significant effects of legal status on the likelihood of a decline in health once migration has ended, and the number of trips is only marginally related to worsened health (p < .10). The likelihood of reporting a decline in health increases with age as well as with the number of years since returning from the United States. Greater number of amenities, an indicator of material wealth, is negatively related to a decline in health.
Logistic Regression Models Predicting Decline in Health from Just After Last Trip to Survey Date and Health at Time of Survey.a
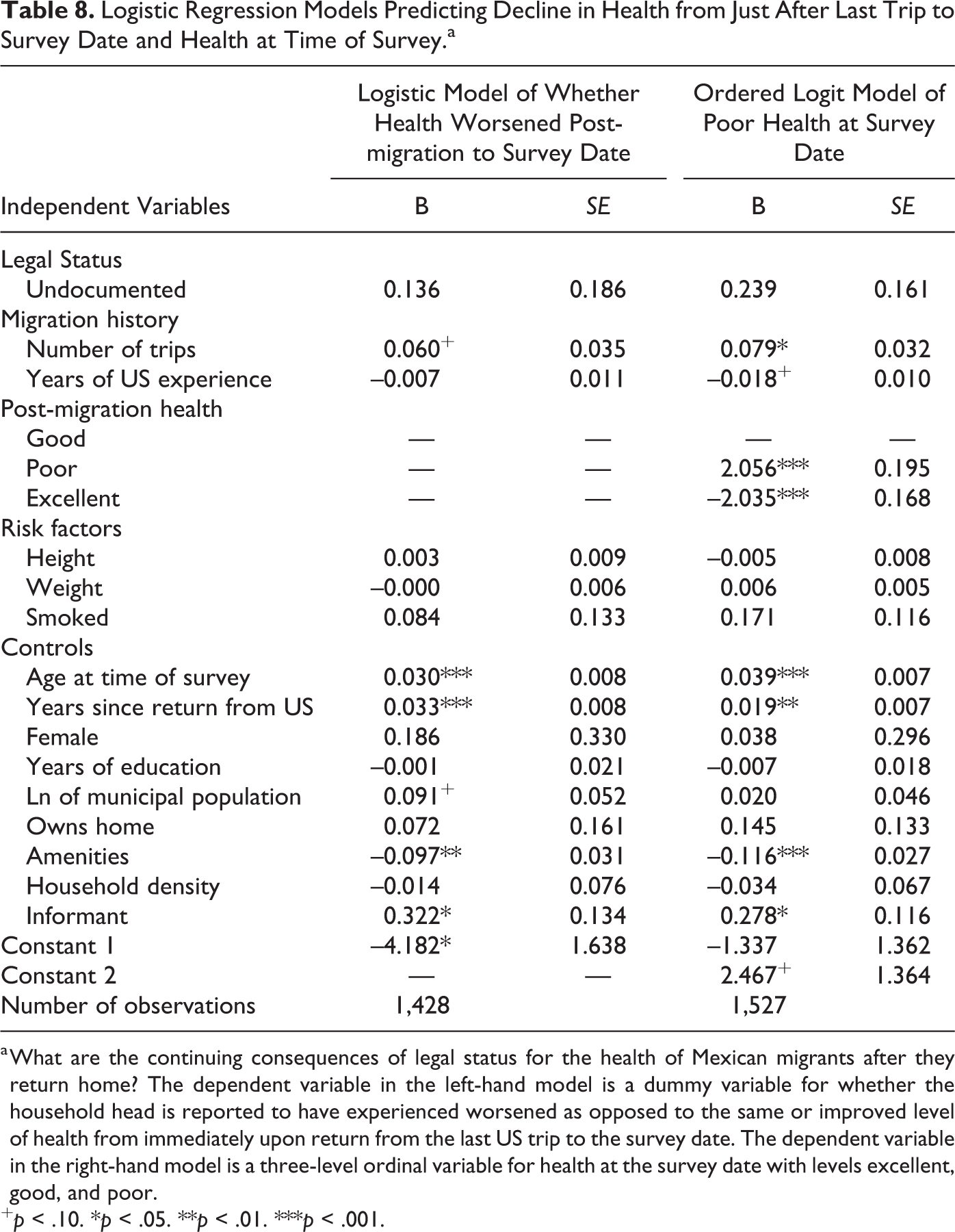
a What are the continuing consequences of legal status for the health of Mexican migrants after they return home? The dependent variable in the left-hand model is a dummy variable for whether the household head is reported to have experienced worsened as opposed to the same or improved level of health from immediately upon return from the last US trip to the survey date. The dependent variable in the right-hand model is a three-level ordinal variable for health at the survey date with levels excellent, good, and poor.
+ p < .10. *p < .05. **p < .01. ***p < .001.
The right columns of Table 8 present an ordered logistic model predicting health at the survey date among returned migrants given health immediately after the last US trip, legal status, total number of trips, total US experience, and controls. In accordance with the previous model, returned undocumented migrants are no more likely to be in poor health at the survey date compared to documented returned migrants. In contrast to the previous model, however, years of US experience are negatively related to poorer health, with the likelihood of experiencing worse health decreasing by 1.8 percent with each additional year spent in the United States, though the effect is only marginally significant (p < .10). A negative effect of US experience on health is not entirely unexpected. In earlier work, Kanaiaupuni and Donato (1999) found that the immediate effect of US migration was to worsen health but that over the long term, it increased household resources in ways that improved health. Consistent with the suggestion that US migration might improve long-term health by providing additional resources to support health, the ordered logit equation shows that the odds of experiencing worse health decrease by 11.0 percent with each increment in the number of household amenities owned. As before, age and greater number of years since returning from the United States are also associated with a higher likelihood of reporting poor health at the survey date.
Table 9 completes our analysis by showing results from an ordered logistic regression assessing the health of returned documented and undocumented migrants relative to nonmigrants at the survey date. The likelihood of experiencing a shift toward poor health between age 14 and the time of the survey is significantly lower for returned documented migrants than returned undocumented migrants and nonmigrants. For all migrants, health is more likely to worsen as trips increase, rising by 9.6 percent for migrants with each trip taken. Consistent with the prior set of models, there is suggestive evidence that greater US experience lowers the likelihood of being in poor health at the survey date by improving the material well-being of households. In addition, the likelihood of reporting poor health at the survey date is greater for women and smokers and rises with increasing weight and age. The odds of poor health fall with increasing height, years of education, municipal population size, and number of amenities.
Ordered Logistic Regression Predicting Health at Time of Survey.a
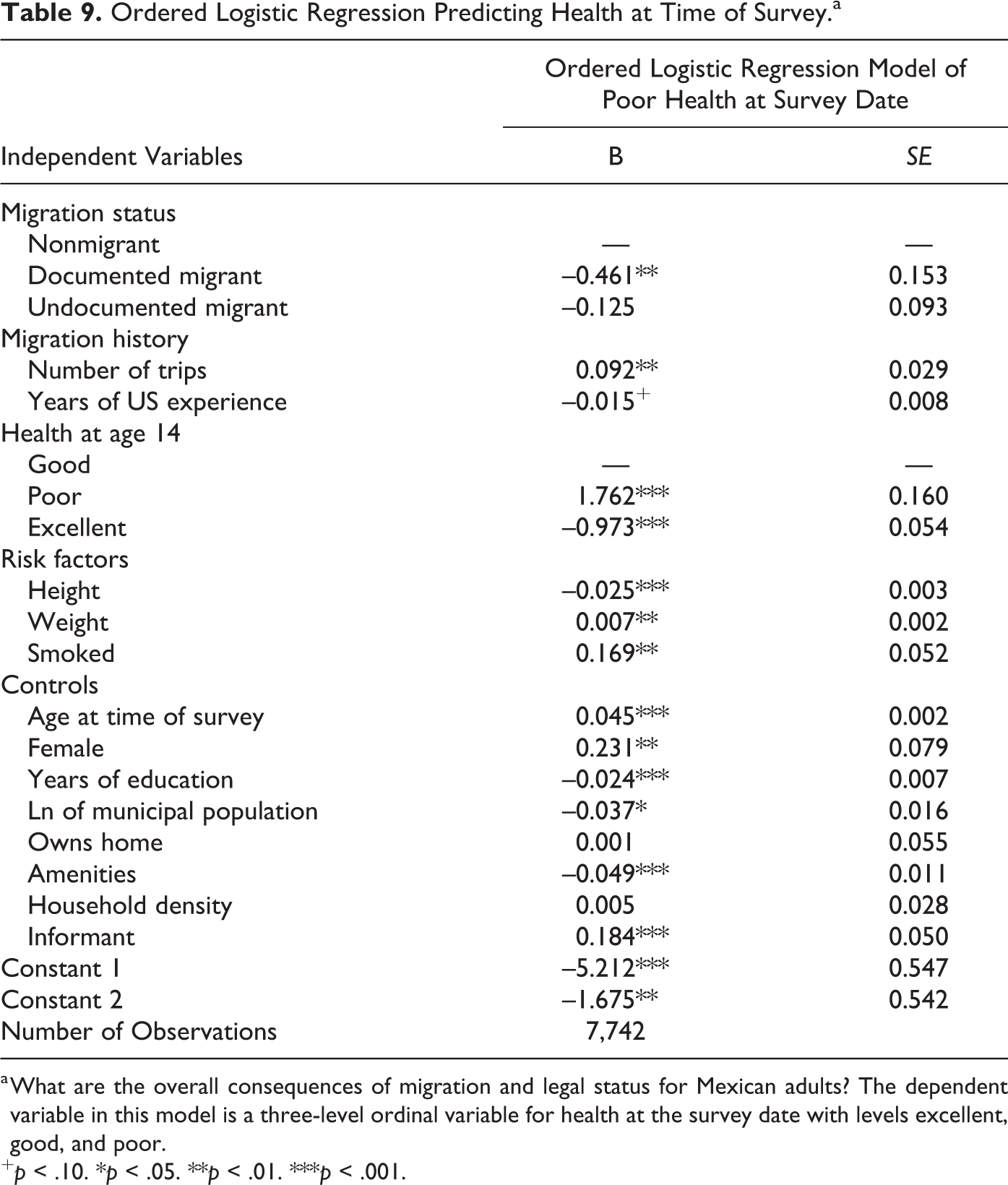
a What are the overall consequences of migration and legal status for Mexican adults? The dependent variable in this model is a three-level ordinal variable for health at the survey date with levels excellent, good, and poor.
+ p < .10. *p < .05. **p < .01. ***p < .001.
Summary and Conclusion
Unauthorized status relegates migrants to the most disadvantaged segments of the US social structure, within which they face exclusion from most public social services and heightened risks of discrimination, arrest, and deportation. Our analyses suggest that unauthorized status has strong negative consequences for migrants’ health as well. After controlling for possible informant bias and recall error in our data and discounting the possibility of a significant salmon bias among returned migrants, our analysis yields the following key conclusions: Mexican migrants to the United States are positively selected on the basis of health, and the degree of health selectivity does not vary by legal status. Over the course of a migratory career, health steadily deteriorates, declining with each successive US trip and each additional year spent in the United States. The decline in health is greater for undocumented than documented migrants, holding constant the number of trips and years of US experience, suggesting that a lack of legal status itself increases the risks to health. After retiring from active migration, migrants’ health continues to deteriorate depending on the number of US trips taken, but neither the likelihood nor amount of the health decline differs by legal status. When the health of documented and undocumented migrants is compared with that of nonmigrants at the survey date, we find that the health of migrants is worse than that of nonmigrants and grows worse with each successive US trip. The negative health effects of US migration are less for documented than undocumented migrants and are mitigated by the accumulation of household assets financed by US earnings.
In sum, our work shows that migrating to the United States is bad for one’s health and that it is especially bad for migrants who lack legal documents, worsening as migratory careers lengthen and trips accumulate. No analysis is perfect, however, and ours carries several caveats. First, our findings are estimated for returned migrants and cannot necessarily be generalized to the broader population of undocumented migrants still in the United States. Second, the MMP’s method of soliciting health reports are vulnerable to multiple sources of measurement error, including relying on proxy informants, recall bias due to memory lapses, and possible differences in standards to which migrants and nonmigrants are comparing health. Third, reports on past health may be influenced by perceptions of current health, leading to endogeneity bias. Fourth, while we find little support for the salmon bias, it is possible that the MMP does not fully capture the mortality of sick migrants.
Although we cannot identify the specific mechanisms by which poor migrant health is generated, the 2016 US elections validated political positions in favor of fortifying physical and legal barriers to integration and augmenting the hostile context of reception for immigrants. This study reinforces the need for recognition of the direct public health consequences of immigration policy (Castañeda et al. 2015). The deterioration of immigrants’ health — especially among those who are undocumented — represents yet another indication of the disjunctures of the United States’ restrictive and exclusionary immigration policies. Measures such as lowering the legal and financial barriers to health insurance for migrants and other policy changes informed by the recognition of access to health care as a basic human right regardless of legal status will be needed to safeguard the welfare of undocumented immigrants and their children, a growing fraction of whom are native-born US citizens.
Footnotes
Appendix
Percentage of Data Missing before Multiple Imputation.
| Variable | Cross Sectional | Event History |
|---|---|---|
| Health at 14 | 0.003 | 0.004 |
| Pre-migration health | 0.014 | — |
| Post-migration health | 0.013 | — |
| Current health | 0.003 | — |
| Health worsened pre- to post-migration | 0.014 | — |
| Health worsened post-migration to survey date | 0.013 | — |
| Health worsened age 14 to survey date | 0.004 | — |
| Migrant status | 0.000 | — |
| Whether a trip was taken in the person-year | — | 0.000 |
| Number of trips | 0.000 | — |
| Years of US experience | 0.000 | — |
| Height | 0.012 | 0.013 |
| Weight | 0.040 | 0.043 |
| Ever smoked | 0.002 | 0.001 |
| Amenities | 0.018 | — |
| Household density ratio | 0.004 | — |
| Owned home | 0.003 | 0.000 |
| Municipal population | 0.000 | 0.001 |
| Age at survey date | 0.000 | — |
| Age of first trip | 0.000 | — |
| Age of return from last trip | 0.000 | — |
| Years since first departure to US | 0.000 | — |
| Years since return from US | 0.000 | — |
| Currently in US | — | 0.000 |
| Informant | 0.000 | — |
| Age in person-year | — | 0.000 |
| Female | 0.000 | |
| Years of education | 0.006 | 0.007 |
| Relative ever migrant | — | 0.000 |
| Community migration prevalence | — | 0.000 |
| Observations after list-wise deletion | 7,374 | 234,750 |
| Observations after multiple imputation | 8,067 | 248,929 |
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development of the National Institutes of Health under Award Number P2CHD047879.