
Abstract
The conventional and standard pharmacological approaches in the management of bipolar disorders include mood stabilizers and second-generation antipsychotics. However, renal problems owing to the gold standard mood stabilizer, lithium, is three times that of the general population. As bipolar I disorder (BPD I) is associated with overactive protein kinase C (PKC) intracellular signaling, a novel approach in the management of acute mania/mixed affective states of bipolar disorder includes the use of PKC inhibitors, such as Tamoxifen and its derivative metabolite molecule, Endoxifen. Our objective is to report two cases of bipolar disorder that presented in acute manic episodes, with preexisting renal disease, and safe use of Endoxifen as an adjunct/monotherapy for rapid control of symptoms. According to our study, Endoxifen can be used as an anti-manic agent, either as monotherapy or as an adjunct, in patients with renal disease. It can also be used as an effective cover therapy for bipolar disorder patients requiring steroids for the treatment of renal pathology, though long-term studies are needed to assess the long-term safety and efficacy.
Bipolar disorder is an episodic severe mental disorder characterized by episodes of hypomania, mania, mixed affective states, and depression. Conventional and standard pharmacological approaches include the use of mood stabilizers and second-generation antipsychotics for the management of both acute episodes and the prevention of recurrent episodes. Lithium, the gold standard mood stabilizer, increases inhibitory transmission by increasing the GABA levels. It also increases serotonin levels and reduces glutamate and dopamine levels. Further, it acts by targeting the phosphatidylinositol signaling pathway. However, as per the literature, only 30% respond well to lithium, and another 30%–55% do not benefit from it and experience adverse effects. 1 Patients on long-term lithium therapy have three times higher renal comorbidities than the general population, making it difficult for psychiatrists to continue lithium therapy for longer periods. 2
In addition, bipolar disorder is associated with another established pathophysiology of overactive protein kinase C (PKC) intracellular signaling. Isozymes of PKC are highly expressed in certain structures of the frontolimbic region, like the prefrontal cortex, hippocampus, and amygdala, which are involved in mood regulation. Thus, PKC inhibition is an additional target in the treatment of bipolar disorder. 3 Though lithium is also an indirect inhibitor of PKC, novel approaches for the poor responders of lithium in the management of acute mania/mixed affective states of bipolar disorder include the use of potent inhibitors of PKC like Tamoxifen and its derivative active metabolite molecule, Endoxifen, which is four times more potent than Tamoxifen in PKC inhibition. Further, being an active metabolite, Endoxifen is not dependent on the drug-metabolizing enzyme CYP2D6 that metabolizes Tamoxifen. 4 Our objective is to report two cases of bipolar disorder that presented in acute manic episodes, with preexisting renal disease and safe use of Endoxifen, which has level-two evidence for antimanic efficacy, 4 as an adjunct/monotherapy for rapid control of symptoms. We have obtained written informed consent from both patients, and we have received approval from the Institutional Ethics Committee. No AI was used to prepare the manuscript. The authors assume full responsibility for the entire content of the manuscript.
Case Series
Case 1
Mr. M is a 53-year-old married gentleman with nil significant family history, diagnosed with bipolar disorder at the age of 23 years, and, to date, had six episodes of mania with psychotic symptoms, one episode of mania without psychotic symptoms, and one moderate depressive episode. He was diagnosed with membranous glomerulonephritis four months back, clinically and biopsy-proven. He was diagnosed with dyslipidemia with moderate elevation of low-density lipoprotein (LDL), very low high-density lipoprotein (HDL), and severe elevation of total cholesterol and triglycerides with decreased total protein in serum. He was tried on lithium in the past with a good response, but owing to the current derangement in renal parameters, it was stopped about seven months before his current visit, and valproate was initiated by a psychiatrist elsewhere. He presented to our Department of Psychiatry with a 10-day history of overtalkativeness, overfamiliarity, increased goal-directed activities, decreased need for sleep, and hallucinatory behavior, such as talking and muttering to self and singing devotional songs to God, despite being on medication. He further reported hearing God’s voice that he has special powers to change the world. He was on valproate 300 mg/day, carbamazepine 600 mg/day, iloperidone 3 mg/day, and lorazepam 2 mg/day. He was also taking cyclophosphamide 100 mg/day for his membranous glomerulonephritis.
He was admitted for inpatient care, and mood stabilizers were optimized according to his body weight. Valproate was increased to 1000 mg/day, and carbamazepine was maintained at 600 mg/day. Iloperidone was stopped, and risperidone was started and maintained at 6 mg/day. Baseline Young’s Mania Rating Scale 5 (YMRS) was applied, and a score of 50 was recorded, which indicated moderate to severe mania. A nephrology team opinion was taken for further evaluation and management of renal pathology. Because of the persistent elevation of serum creatinine with increasing trends, lithium rechallenge was not an option. The nephrology team opined on continuing cyclophosphamide for control of worsening renal parameters with a plan to initiate steroid treatment if mood symptoms are well controlled.
The patient was continued on the same medications for one week. However, he also needed round-the-clock sedation using Haloperidol 5 mg twice a day, Promethazine 25 mg twice a day, and Olanzapine 10 mg twice a day for three days, along with frequent physical restraints for his sudden anger outbursts and aggression. YMRS scores were continuously monitored, which showed only a 12% reduction in the first six days. The patient was considered for electroconvulsive therapy (ECT), but owing to his multiple physical comorbidities and consequent cardiac safety, his nephrology team deemed him unfit for it. It was finally decided to try Endoxifen at a dose of 4 mg/day in the morning on day 7 of admission. After three days, the dose was increased to 8 mg/day. The patient showed significant improvement in the first three days on Endoxifen with a YMRS score reduction of 60% from the day of start of Endoxifen therapy and 66% from baseline. YMRS monitoring is shown in Table 1. Also, the daily dose of all medication used is shown in Table 2.
YMRS Monitoring of Case 1 During Inpatient Care.
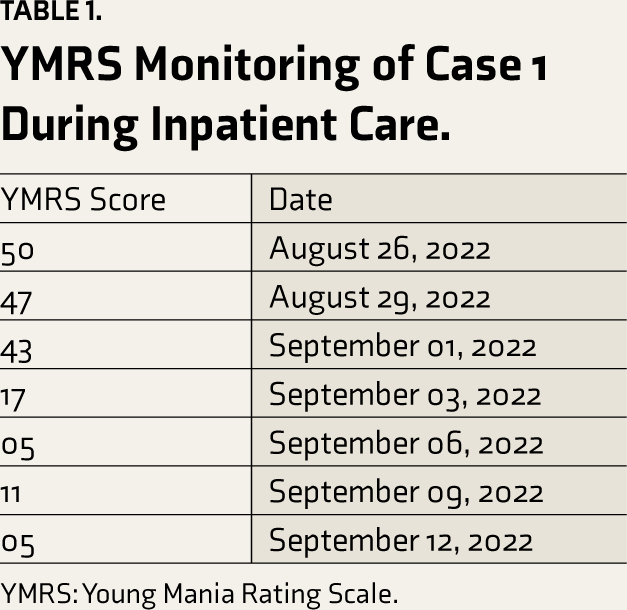
YMRS: Young Mania Rating Scale.
Daily Dose of Medication of the Two Study Subjects.
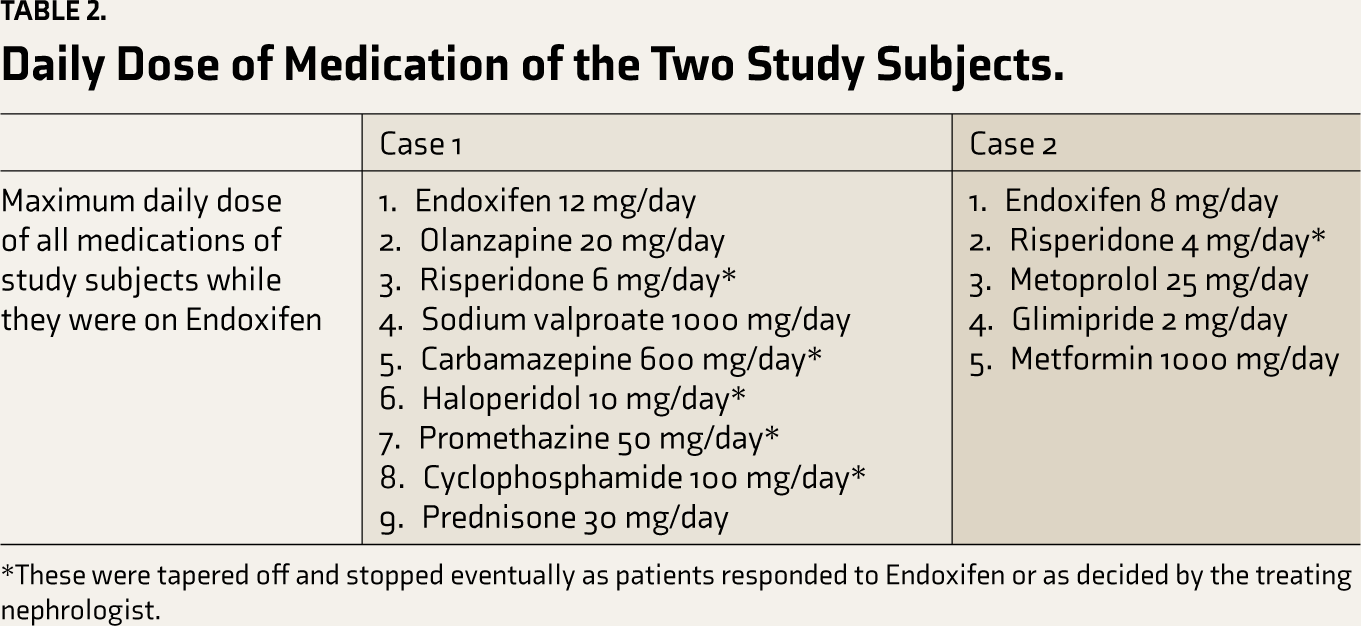
*These were tapered off and stopped eventually as patients responded to Endoxifen or as decided by the treating nephrologist.
The nephrology team reviewed the patient, and owing to significant im-provement in manic symptoms, he was started on intravenous (IV) methylprednisolone pulse therapy (MPT) 500 mg/day for three days, followed by oral methylprednisolone 30 mg/day for membranous glomerulonephritis. During IV MPT, his mood symptoms again fluctuated, which is reflected in his YMRS score elevation from 5 to 11, but he did not require physical or chemical restraints. Endoxifen was increased to 12 mg/day. Renal parameters were reevaluated, and the nephrology team opined that the patient could be continued on oral steroids. The patient was discharged from IP care on oral steroids, Olanzapine 10 mg/day, Valproate 1000 mg/day, and Endoxifen 12 mg/day. There seems to be a temporal association between the addition of Endoxifen and rapid improvement of manic symptoms in this patient, which did not happen during the first week with multiple medications. However, the delayed effects of valproate/olanzapine cannot be completely ruled out. On a monthly follow-up on an outpatient (OPD) basis for three months, the patient reported maintaining well on the above medications and reported no side effects. He was maintaining well on Valproate 1000 mg, Olanzapine 5 mg, and Endoxifen 12 mg when he was seen seven months later on follow-up. Endoxifen was stopped subsequently, after about 11 months of initiation, as it is an off-label indication and is only for manic episodes and not prophylaxis. Renal parameters were within normal limits, and he has been receiving monthly steroid therapy with no worsening of mood symptoms. He was last seen doing well in the OPD in June 2024, that is, about one year and nine months after the last episode.
Case 2
Mr. B is a 70-year-old married gentleman with nil significant family history, diagnosed with bipolar disorder at the age of 23 years, and, to date, had multiple episodes of mania/hypomania and one moderate depressive episode. He was diagnosed with hypertension at the age of 58 years and diabetes mellitus at the age of 60 years, both under control with Metoprolol 25 mg/day, Metformin 1000 mg/day, and Glimepiride 2 mg/day. He was maintaining well on Risperidone 4 mg/day and Lithium 800 mg/day. He presented to the Department of Psychiatry with a two-week history of overtalkativeness, overfamiliarity, increased goal-directed activities, increased alcohol consumption, irritability, and reduced sleep at night. His wife reported him being compliant with medications under supervision. He was advised inpatient care. On routine baseline investigations, it was found that his serum creatinine was 1.8 mg/dL and serum lithium was 0.7 mmol/L. The physician diagnosed him with chronic kidney disease stage 3 with a renal cortical cyst in the right kidney. Owing to his renal parameters, it was decided that lithium was not a good option despite a good response to lithium in the past. He had three documented episodes of hyperammonemia with valproate in the past, and hence, that was not considered. He was started on low-dose oxcarbazepine, 150 mg/day in divided dosing, and he experienced drowsiness, difficulty in walking, frequent disorientation, and delirium-like pictures. Oxcarbazepine was stopped, and an MRI scan of the brain was done to rule out any other contributing organic etiology. It showed xanthogranulomatous changes, which were opined to be age-related by the neurologist. Serum sodium repeated twice revealed normal results. He was not rated/monitored on YMRS as he initially presented with a delirium-like picture, which persisted for a few days.
He was then started on Endoxifen at 4 mg/day in the morning on the ninth day of admission and built up to 8 mg/day. The patient was discharged on the 19th day after admission, as he improved significantly. His risperidone was continued at 4 mg/day during the inpatient stay and stopped on discharge as it is also known to affect renal function. 6 Subsequently, the patient has been seen several times on an OPD basis, once in one to two months. He reported maintaining well on 8 mg/day of Endoxifen. Renal parameters were within normal limits. Endoxifen was stopped after 10 months of initiation as it is not considered a prophylactic agent. Aripiprazole 10 mg was started as he needed prophylaxis and ongoing care. Daily dose of all medication used are represented in Table 2. He came for follow-ups once in 2–3 months before he visited recently with another manic episode in April 2024, mild in severity, while on aripiprazole, about 1.5 years after the previous episode, and was admitted for five days. This time, he was discharged on Aripiprazole 20 mg/day and Quetiapine 50 mg in divided doses. As the episode was mild and the patient expressed concern over affordability, Endoxifen was not started this time.
Discussion
Novel approaches for the management of acute mania/mixed affective states of bipolar disorder include the use of PKC inhibitors like Tamoxifen and its derivative, Endoxifen. PKC activity amongst bipolar disorder patients is mostly studied in the postmortem brain sample and platelets. A study on cortical homogenates showed that patients with bipolar mood disorder have increased PKC levels and membrane-bound PKC activity when compared to healthy controls. 3 Lithium partly influences neuroplasticity through PKC-independent mechanisms. Multiple cellular-level observations suggest that valproic acid and lithium have different mechanisms of action, but they both share the same target of PKC and affect its downstream signaling. 7
Tamoxifen displays direct inhibitory activity on PKC. It is the only PKC inhibitor that crosses the blood–brain barrier. 8 Patients with bipolar disorder managed with Tamoxifen for three weeks were seen to be markedly improved in their manic symptoms as early as five days in a three-week trial.4,9 In a randomized study of six weeks, it was demonstrated that the combination of Tamoxifen and lithium was significantly better than lithium alone for the early reduction of manic symptoms. Further, monotherapy with Endoxifen, which is the metabolite of Tamoxifen and a potent inhibitor of PKC, was found to mitigate manic symptoms as effectively as 1000 mg/day of valproic acid. 10
PKC has several isozymes in humans and is divided into three subfamilies (conventional, novel, and atypical) based on second messenger requirements. Endoxifen inhibits PKCβ1 (conventional), which requires DAG and calcium ions as second messengers and thus downregulates phosphorylation. 11 Endoxifen has some advantages over lithium and valproate. It has similar efficacy as valproate, 12 without inducing thrombocytopenia. Further, there is no need for frequent drug monitoring, unlike lithium, because of its wide therapeutic index. 12 Additionally, Endoxifen crosses the blood–brain barrier, independent of CYP-2D6 metabolism. Results of its multicenter trial using an 8-mg daily dose in patients with acute manic episodes with or without mixed features found that it significantly reduced the total score on YMRS and was well tolerated.12,13
Endoxifen is benign compared to Tamoxifen with respect to side effects. Headache, vomiting, insomnia, restlessness, and somnolence are some of its common side effects. 4 There are no known severe adverse drug interactions with psychotropic medication as Endoxifen is an active metabolite. Also, it can be used safely in patients on medication for renal problems like cyclophosphamide and steroids. Studies on lipid profiles with Endoxifen therapy are mixed, showing both significant reduction and elevation of LDL and total cholesterol.10,15 Studies on Endoxifen use in bipolar disorder are scarce. Long-term follow-up studies can establish the use of Endoxifen as a safe mood stabilizer in patients with renal disease. 14
Conclusion
Endoxifen can be used as an anti-manic agent, either as monotherapy or as an adjunct, in patients with renal disease. It can also be used safely along with steroids for renal pathology in bipolar disorder, where it can prevent the worsening of mood/psychotic symptoms. Long-term studies evaluating benefits and risk are needed for establishing the sustained safety and efficacy of Endoxifen in bipolar disorder patients with chronic medical comorbidities.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
The authors assume full responsibility for the entire content of the manuscript. No parts of this manuscript were generated by any AI tool.
Ethical Approval
The Institutional Ethics Committee approved the study (Approval No. IEC1-425 dated 08/03/2024) and written informed consent was obtained from the participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Individual participants' written consent has been obtained for publishing this content.