
Abstract
Background:
Post-partum depression (PPD) adversely affects maternal and child health, yet evidence for integrated mother–child interventions remains limited in low-resource settings. We evaluated the impact of SPRING (Sustainable Programme Incorporating Nutrition and Games), an integrated mother–child psychosocial home-visiting intervention, on PPD outcomes in rural India.
Method:
A cluster-randomized controlled trial evaluated the intervention’s impact across 120 villages (24 clusters). Mother-infant dyads were identified through house-to-house surveillance, with PPD measured at 12 months post-partum using the Patient Health Questionnaire-9 (PHQ-9). While the intervention aimed to improve child growth and development by indirectly addressing maternal mental health, this article reports specifically on PPD outcomes.
Results:
Among 2007 mothers completing assessments, PPD prevalence was 13.1%, with no significant difference between arms (RR = 0.98, 95% CI: 0.69–1.39, p = .90). No effect of intervention was found on PPD (mean PHQ-9 score 1.8 [SD 2.68] in the intervention group and 1.9 [SD 2.79] in the control group; effect size –0.02; 95% CI: –0.11, 0.07; p = .68). Analyses were intention-to-treat.
Conclusions:
The lack of measurable impact in our study highlights two key considerations. First, integrated mother–child psychosocial interventions may require more targeted strategies to address depressive symptoms and reduce PPD. Second, implementation challenges, such as coverage and uptake, likely influence effectiveness. Notably, at least one in eight mothers in our study experienced PPD at 12 months post-partum, aligning with other Indian studies. This persistent burden, alongside unmet mental health needs, emphasizes the urgency for future integrated mother–child interventions to include PPD-specific components and critically monitor implementation, especially in rural settings.
Keywords
A cluster randomized controlled trial evaluated an integrated mother–child psychosocial home-visiting intervention for post-partum depression (PPD) in India. No impact on PPD at 12 months was observed despite addressing maternal mental well-being. Gaps in implementation, particularly in coverage and uptake, may explain the absence of effects; future mother–child interventions should more directly address depressive symptom reduction.Key Messages
Post-partum depression (PPD) is a public health challenge owing to its harmful effects on the two most vulnerable groups—women and children.1–4 Defined as a non-psychotic depressive episode, its onset period ranges from 4 to 6 weeks, 2,5 to 1 year after childbirth.2,6,7 The PPD prevalence estimates vary from approximately 10% amongst women residing in high-income countries (HICs) and about 20% and above for those living in lower- and middle-income countries (LMICs).1,8 The seriousness of PPD emanates from its considerably adverse effects on a woman’s mood and her interpersonal relationships.9–12 This can potentially restrict her capacity to nurture her child and affect their dyadic bond adversely.2,13 For the child, this may result in detrimental outcomes, including poor cognitive, emotional, behavioral, and social skills and an increased risk of psychopathology.10,11,14–17
While psychological and psychosocial interventions for maternal depression are well documented in both HICs18–26 and LMICs,26–29 few studies have investigated the impact of PPD interventions on child outcomes. 20 Conversely, interventions targeting child outcomes seldom focus on the mother’s depression as an important variable.30–32 Recent years have seen the advent of integrated interventions that aim to address both PPD and early childhood consequences.20,27,28,31,33–37 A systematic review found strong evidence supporting mother-focused interventions that combined psychological and psychosocial components to improve PPD outcomes. 38 For mother–child-focused interventions, adding strategies to help mothers manage depressive symptoms alongside techniques to enhance mother-infant interaction (e.g., responsive play) seemed vital for achieving positive changes in PPD. Mother-focused psychosocial interventions were observed to perform more effectively towards reducing depressive symptoms when these child-related components were incorporated.28,34,35,38
The SPRING (Sustainable Programme Incorporating Nutrition and Games) is one such integrated evidence-based mother–child-focused psychosocial home-visiting intervention designed to improve child growth and development by indirectly addressing maternal PPD. However, most existing studies have focused on short-term effects at 3–6 or 9 months, with limited and inconsistent evidence on their longer-term impacts, particularly at 12 months, and especially in LMICs. Given this gap, our primary objective was to evaluate the impact of the intervention on PPD at 12 months post-partum (an intermediate outcome in its hypothesized change pathway) 39 (Figure 1, Supplementary Online Material 1). This study represents one of the few cluster-randomized trials from rural India to assess the effectiveness of a community-based intervention on maternal PPD during the later post-partum period.
Methods
We adhered to the Consolidated Standards of Reporting Trials (CONSORT) guidelines (Schulz KF, Altman DG, Moher D, for the CONSORT Group. CONSORT 2010 Statement: updated guidelines for reporting parallel group randomized trials). The CONSORT checklist is uploaded as “supplementary online material 2”.
Study Design
The SPRING intervention was evaluated by a cluster randomized controlled trial (cRCT) conducted in two settings, India and Pakistan. 39 This article only reports results from India for PPD at 12 months post-partum. In brief, 24 clusters corresponded to the catchment areas of health sub-centers at the primary healthcare system level with functioning Auxiliary Nurse Midwives (ANMs), each serving at least 8,000 people. Clusters were equally randomized to intervention or control arms using baseline data from enrolled mothers gathered via the project’s surveillance team, and a restricted randomization method to ensure balance on key variables. These included a percentage difference in child stunting (Height-for-age z-score < –2) among 18–30-month-olds, percentage of mothers with no schooling, and percentage of facility-based deliveries. The trial statistician was responsible for generating all possible allocation schemes, screening them for anomalies, and randomly selecting one using computer software. While the SPRING implementation teams were informed of cluster allocation, this information remained concealed from the trial conduct team. Surveillance field workers could not be blinded as they were based within the clusters. However, outcome assessors conducting the 12- and 18-month assessments were kept blinded to allocation. 39
The intervention was delivered to all mother–child dyads in the intervention arm, regardless of their PPD status, using a universal prevention approach. It was not explicitly targeted at women identified as high risk or already experiencing elevated depressive symptoms. Maternal depression was not assessed at baseline, and PHQ-9 scores did not inform intervention delivery. The impact of the intervention on maternal depressive symptoms was assessed at 12 months post-partum using the PHQ-9, administered uniformly across both arms. Assessment of PPD at 12 months was a planned outcome of the trial, and the sample size was calculated to ensure sufficient power to detect differences between arms. Although baseline PHQ-9 scores were not collected, the cluster-randomized design with restricted randomization ensured comparability between arms on key socio-demographic variables. These features reduce the risk of selection and measurement bias and strengthen the reliability of the findings.
For further details on the SPRING trial methodology, including randomization and masking, please refer to the earlier publications.39,40
Study Setting and Participants
This program was implemented in 120 villages within the three administrative blocks of Rewari district, Haryana, Northern India. Rewari is primarily rural with an average demographic profile. The district’s sex ratio was 898/1000 males, ranked amongst the lowest in India. Male and female literacy rates were 91.44 and 69.57, respectively. 41 Participants were mother-baby dyads reporting live births identified by the project-established house-to-house surveillance system in the trial clusters from 18 June 2015, when the program was fully implemented, till July 1, 2017, when primary outcome data collection was completed (not reported in this article). Additional mothers were recruited for PPD assessment to meet the sample size requirement. Exclusion criteria comprised any major congenital malformation, maternal death in the neonatal period, child death reported at the 12-month assessment, and mother’s incapable of answering questions.
Intervention
Designed as an innovative and scalable home-visiting intervention, SPRING was delivered by a newly developed cadre of Community-Based Agents (CBA) from pregnancy through the first two years of life, aiming to maximize child development, growth, and survival.39,40 The intervention was adapted from the World Health Organization (WHO)/United Nations Children’s Fund’s (UNICEF) Care for Development package. 42 The intervention’s change pathway 39 (Figure 1, Supplementary Online Material 1) hypo-thesized that the intervention would have a direct impact on child outcomes by improving feeding, interaction, and play behaviors while indirectly influencing maternal caregiving behaviors by improving maternal mental health, well-being, and efficacy through problem-solving techniques and family support.43–45 A supportive counselling approach adapted from cognitive behavioral therapy (CBT), previously found to be effective in a trial in Pakistan, 27 and built on the five pillars approach to maternal psychosocial well-being, 46 was used in SPRING. The intervention incorporated structured, mother-focused strategies based on CBT principles, adapted for delivery by non-specialist CBAs. While it did not directly target depressive symptoms, the intervention aimed to support maternal well-being by strengthening caregiving behaviors and family support systems. Using behavioral activation, CBAs helped mothers break down daily caregiving tasks—such as feeding, play, and stimulation—into small, achievable steps using available resources, to build a sense of mastery and improve mood. Through problem-solving, CBAs supported mothers in identifying practical barriers to these behaviors, exploring possible solutions, and involving family members in overcoming these challenges. The relationship between the mother and the CBA, often perceived as a peer, was another key source of support, helping to reduce isolation and foster trust. Regular home visits, coupled with empathic listening, created a safe space for mothers to talk, reflect, and engage in small behavioral changes. Other elements included guided discovery using counselling cards, modelling through coaching and demonstration, and praise to reinforce maternal effort. 39 Together, these strategies enhanced maternal confidence and coping, addressing psychosocial stressors that may contribute to low mood.
Treatment as Usual
Pregnant women and newborns in both intervention and control areas continued to receive treatment as usual (TAU), comprising routine maternal and child health services. In India, this included ongoing support from Accredited Social Health Activists, Anganwadi Workers, and ANMs, who delivered home- and center-based guidance and care. Participants had access to the standard maternal and child healthcare services available within the public system.
Outcome Measures
The primary outcome reported in this article is PPD at 12 months post-partum, measured using the Patient Health Questionnaire-9 (PHQ-9). The PHQ-9 is a nine-item screening instrument that assesses the severity of depressive symptoms experienced during the past two weeks.47,48 These nine items corroborate the nine diagnostic criteria from the Diagnostic and Statistical Manual-IV (American Psychiatric Association, 1994). 47 Validation and comparative studies.49–52 provide relatively strong evidence for using PHQ-9 with a perinatal population in community settings.50,53–55 Evidence indicates its equivalence with and in some cases superiority over other scales on criterion validity, operating characteristics, and specificity.48,50,53,56 In our trial, PHQ-9 was chosen because it is translated and validated in the Hindi language for use in primary care in India, 57 and required minimal linguistic changes. Short and easy to administer with illiterate women, 50 using PHQ-9 further ensured comparability between the two SPRING sites—India and Pakistan.
Sample Size
Sample size calculations for the SPRING trial are described in detail elsewhere. 39 For PPD, a sample size of 80 per cluster (40 boys and 40 girls) was determined to give 90% power at the 5% level of significance to be able to detect effect size between 0.3SD and 0.4SD based on the assumption that 38% women will be depressed in control group 8 and an intra-cluster correlation (ICC) of 0.27. 29 A 20% loss to follow-up was included from birth to 12-month assessments.
Data Collection
Mothers were assessed using PHQ-9 at 12 months post-partum within the window of -7 to +21 days from the child’s 1st birthday. Our surveillance network recruited potential mother–child dyads for participation in the trial. A separate outcome assessment team was formed, comprising workers recruited locally and trained to administer PHQ-9 and other outcome measures. To ensure data quality, routine trainings were supplemented with booster sessions, extra supportive supervision, and regular checks for the accuracy and completeness of the questionnaires.
Data Analysis
All analyses followed the intention-to-treat principle; that is, all participants allocated to the two arms were analyzed regardless of whether they received the intervention. Stata 15 was used for conducting all analyses (Stata Corp LLC: College Station, TX, USA). Mean PHQ-9 scores were calculated for the presence of PPD (Table 3) in the intervention and control arms. Overall PHQ-9 scores were obtained by adding up scores on items 1–9 [Range: Min = 0, Max = 27]. Every item was scored either 0 = Not at all; 1 = some days; 2 = more than half the days; or 3 = nearly every day. We applied mixed-effects linear regression, accounting for clustering as a random effect and allocation to trial arms as a fixed effect, to calculate the mean differences between the two arms for the overall PHQ-9 score. Effect sizes were calculated as the mean difference in outcome between the two arms divided by their pooled standard deviation.58,59 Additionally, adjusted analyses were conducted using multivariable linear regression models to account for any potential biases arising from factors (Table 1) that may be associated with PPD.8,60,61
For binary outcomes (whether a mother has PPD or not), we used mixed-effects logistic regression models. Additional analyses were done for each of the PHQ-9 depressive severity categories and suicidal tendencies. The PHQ-9 depression severity categories were (a) any depression (scores 5–27), (b) mild depression (scores 5–9), (c) moderate depression (scores 10–14), (d) moderately severe depression (scores 15–19), and (e) severe depression (scores 20–27). 62 The score range for suicidal tendencies was between 1 and 3 on Item 9 (Thoughts that you were better off dead or hurting yourself). Risk ratios were calculated post-estimation using marginals from the logistic regression model, and 95% CIs were determined using the delta method. 63 To adjust for the variables mentioned in Table 1 above, multivariable logistic regression models were applied.
Variables Known to Have an Association with PPD Were Included in the Adjusted Analysis.
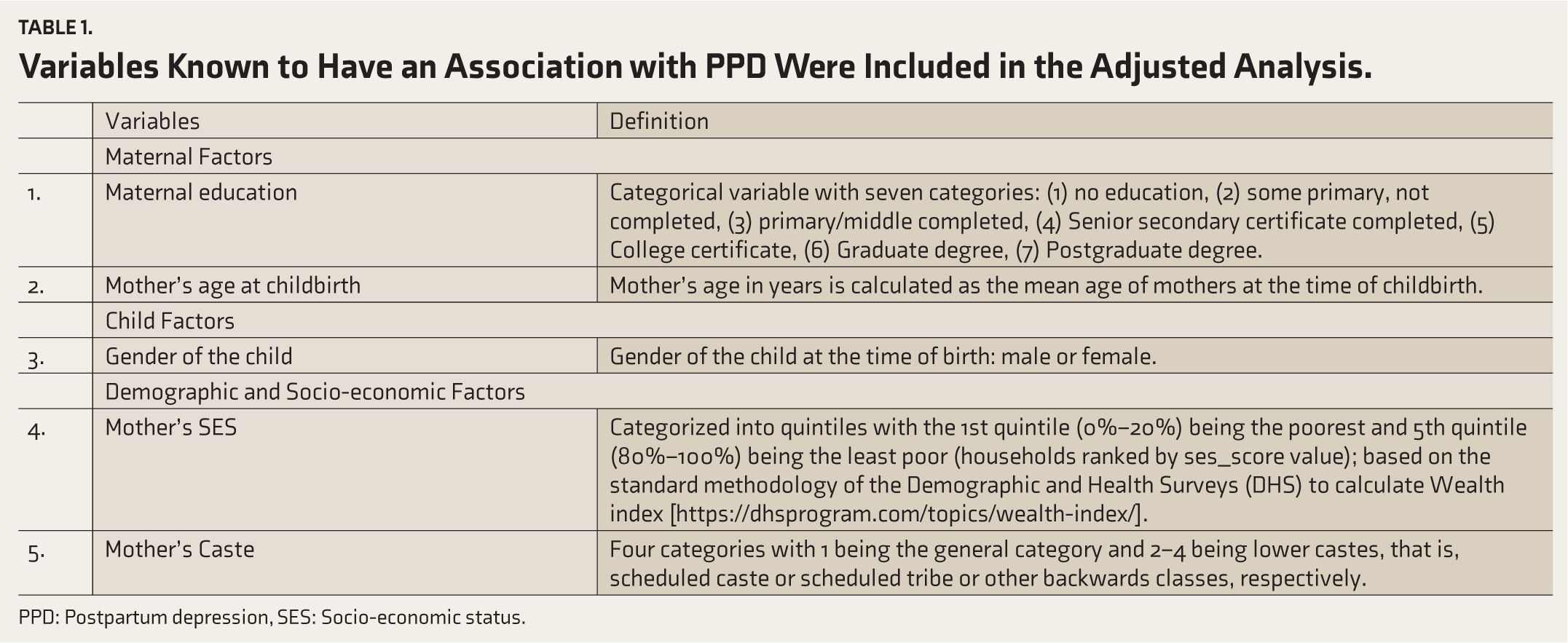
PPD: Postpartum depression, SES: Socio-economic status.
Results
A total of 2609 mother-baby dyads were eligible for maternal assessments at 12 months post-partum. Of these, 18 dyads were excluded based on our exclusion criteria mentioned in the methods section. The trial flowchart (Figure 2, Supplementary Online Material 3) illustrates the participant flow for maternal assessments from enrolment onwards. Overall, 2007 (77.5%) mothers (n = 990 in the intervention group; n = 1017 in the control group) completed PHQ-9 assessments at 12 months post-partum (between July 6, 2016 and October 16, 2017), giving a mean of 84.5 mothers per cluster, which exceeded our sample size. Loss-to-follow-up (22.5%) was mainly due to scheduling changes and non-confirmed appointments by mothers who had initially expressed their availability for the trial.
Comparability Between Intervention and Control Groups
The mothers assessed at 12 months post-partum for PPD in the two arms showed high comparability in socio-demographic characteristics (Table 2). The proportion of mothers with a male child was also compared in the two arms, as a child’s gender has been previously reported as a predictor of PPD.8,60 While we did not observe significant differences between mothers with high and non-threshold PHQ-9 scores relevant to this article, subgroup comparisons were not part of the current analysis plan and will be reported separately.
Comparability Between Participants with Maternal PPD Assessments in the Two Trial Arms.
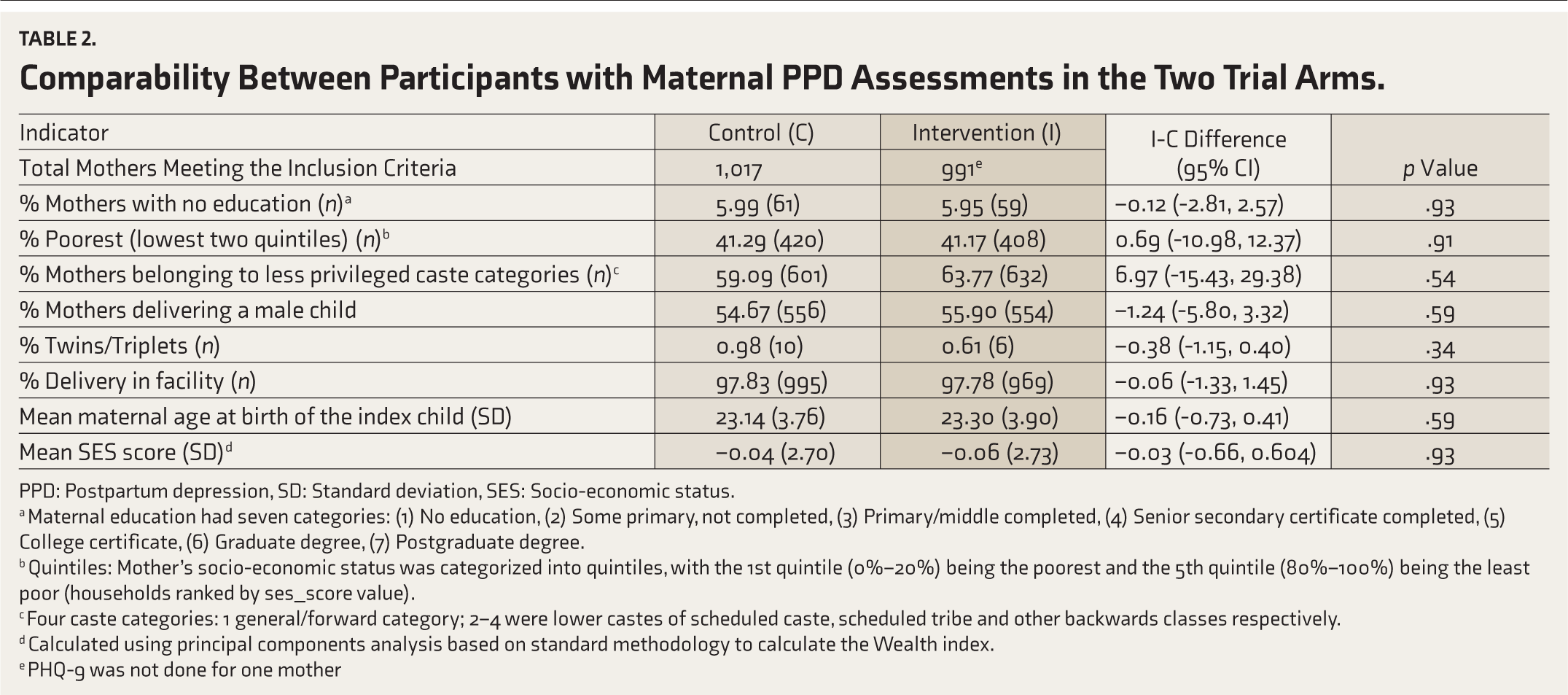
PPD: Postpartum depression, SD: Standard deviation, SES: Socio-economic status.
a Maternal education had seven categories: (1) No education, (2) Some primary, not completed, (3) Primary/middle completed, (4) Senior secondary certificate completed, (5) College certificate, (6) Graduate degree, (7) Postgraduate degree.
b Quintiles: Mother’s socio-economic status was categorized into quintiles, with the 1st quintile (0%–20%) being the poorest and the 5th quintile (80%–100%) being the least poor (households ranked by ses_score value).
c Four caste categories: 1 general/forward category; 2–4 were lower castes of scheduled caste, scheduled tribe and other backwards classes respectively.
d Calculated using principal components analysis based on standard methodology to calculate the Wealth index.
e PHQ-9 was not done for one mother
Impact of Intervention on PPD and Prevalence
The SPRING intervention did not have an impact on overall PPD mean scores (Table 3). The results did not change substantially after adjusting for covariates, including maternal education, maternal age at childbirth, child’s gender, mother’s socioeconomic status, and caste. Additional analysis was done for PPD severity as defined by PHQ-9 scores (Table 4). Overall prevalence for any depression (PHQ-9 score range 5–27) was 13.1% (RR = 0.98; 95% CI: 0.69, 1.32; p = .90) with almost equal risk of being depressed at 12 months post-partum in the two groups. Likewise, the risk of having mild depression (PHQ-9 score range 5–9) in either of the two arms was non-significant (RR = 0.95; 95% CI = 0.63, 1.43; p = .79). For moderate depression (PHQ-9 score range 10–14), the RR estimates, though non-significant (RR = 1.25; 95% CI = 0.63, 2.45; p = .52), indicated an increased risk of PPD in those exposed to the intervention. This was similar for the moderately severe depressed group (PHQ-9 score range 15–19). None of the participants in the intervention arm scored between 20 and 27 on PHQ-9, giving us an RR of 0 for severe depression. Moreover, a lower number of mothers reported moderately severe to severe depression (PHQ-9 scores 15–27). Despite this, the percentage of women reporting thoughts of self-harm or suicidal ideation was high overall (3.4%). Separate adjusted analyses carried out for each PHQ-9 depressive severity category and suicidal tendencies did not change the estimates markedly (Table 4).
Overall Mean Scores on PHQ-9 in Control and Intervention Arms at 12 Months of Maternal Assessments.
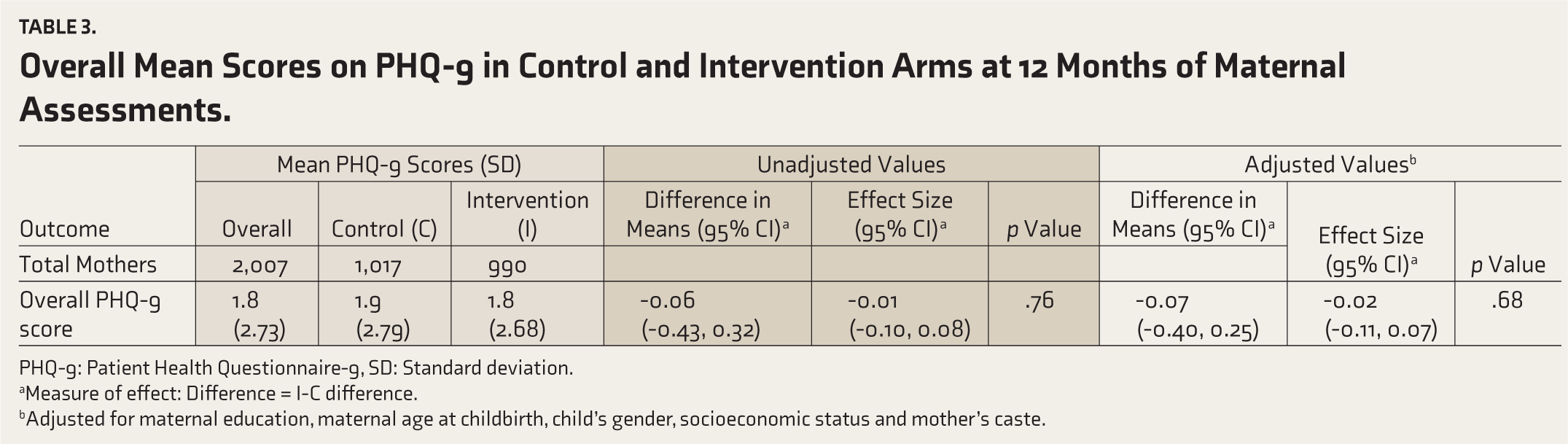
PHQ-9: Patient Health Questionnaire-9, SD: Standard deviation.
aMeasure of effect: Difference = I-C difference.
bAdjusted for maternal education, maternal age at childbirth, child’s gender, socioeconomic status and mother’s caste.
Prevalence of PPD Severity and Suicidal Tendencies in Mothers at 12 Months Postpartum in Intervention and Control Arms, Assessed by PHQ-9.
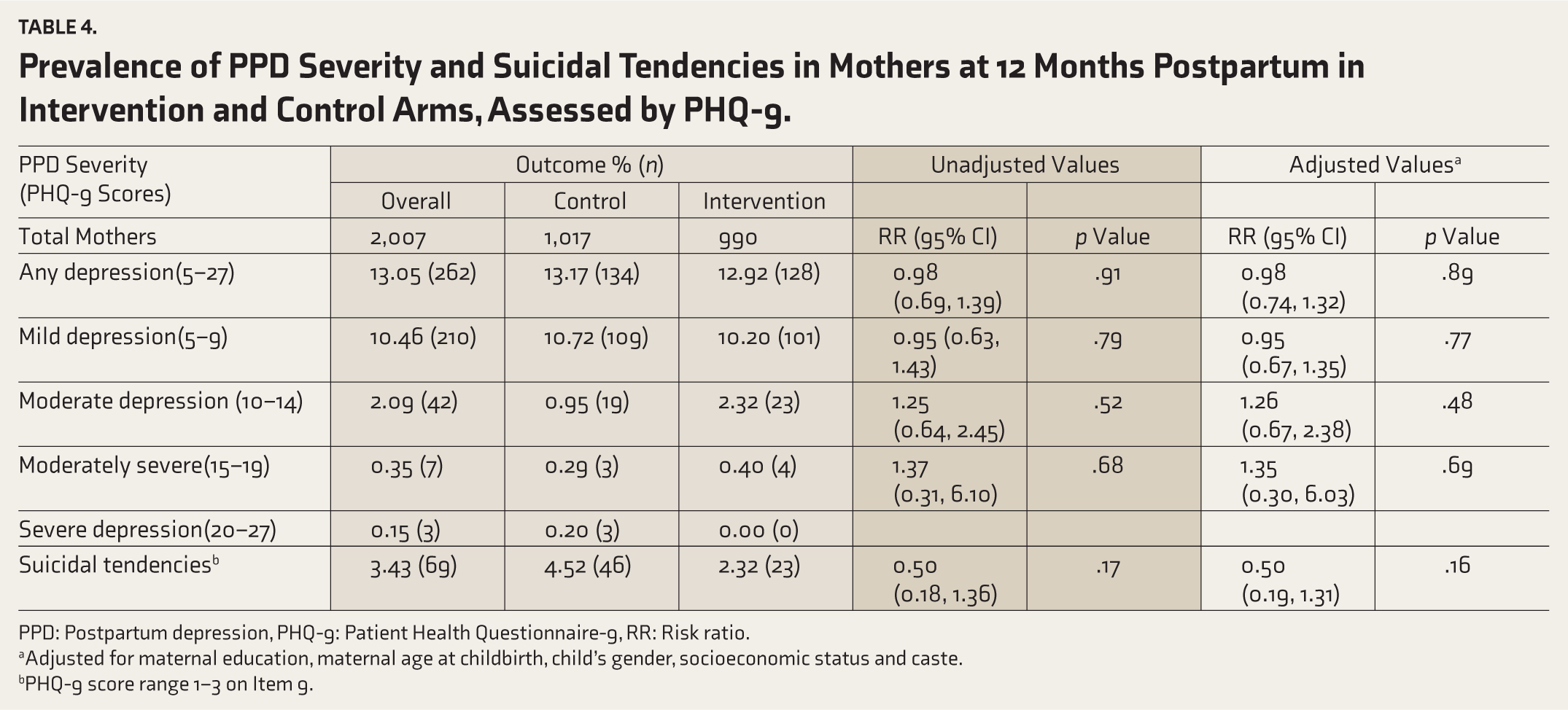
PPD: Postpartum depression, PHQ-9: Patient Health Questionnaire-9, RR: Risk ratio.
aAdjusted for maternal education, maternal age at childbirth, child’s gender, socioeconomic status and caste.
bPHQ-9 score range 1–3 on Item 9.
Discussion
The strength of the SPRING intervention lies in its evidence-based design drawing on best practices from the scientific literature to simultaneously address maternal and child health outcomes while giving careful attention to cultural practices and beliefs. Two key findings emerged: first, there was no measurable impact on PPD; and second, the prevalence of PPD (PHQ-9 score: 5–27) at 12 months post-partum was 13.1%, with no difference between the intervention and control arms.
This lack of observed impact can be summarized under two broad themes:
Intervention design and focus: The approach focused on promoting positive maternal behaviors, enhancing mother–child interaction, and strengthening family support, rather than targeting symptoms of PPD.
Delivery and implementation: Lower-than-expected coverage, variable uptake, and possible misinterpretation of the intervention’s core messages by caregivers may have affected its ability to influence maternal depressive symptoms.
These themes are explored in the sections that follow.
First, we consider one of SPRING’s hypothesized change pathways, which aimed to improve child development and growth by indirectly enhancing maternal mental well-being (Figure 1, Supplementary Online Material 1). 39 Accordingly, each home visit was designed to deliver key messages around mother–child interaction and responsive stimulation while encouraging the adoption of recommended infant feeding practices. 39 The CBT techniques were directed more towards guiding mothers in infant management and less towards managing depressive symptoms. The intervention followed a universal approach—it was delivered to all mothers in the intervention arm regardless of their PPD risk or symptom profile. Recent systematic reviews support this approach, showing strong evidence for psychological and psychosocial interventions, particularly CBT, as effective in preventing PPD among both asymptomatic and at-risk women.64,65 Unlike programs specifically targeting PPD, SPRING aimed to enhance maternal caregiving behaviors and strengthen family support systems. While improvements in maternal well-being were anticipated as a secondary benefit, they were not a primary objective or direct focus of the intervention. This broader, non-targeted approach may have contributed to the observed lack of measurable impact on PPD symptoms. A recent systematic review comparing mother-focused and mother–child-focused interventions for PPD found that those not primarily targeting depressive symptom reduction, but instead aiming to enhance mother–child interactions by improving maternal knowledge and caregiving, did not significantly reduce PPD.38,66–68 The authors further noted that psychosocial interventions incorporating child-related components appeared more effective in alleviating depressive symptoms. 38 However, this was not observed in our intervention. Similar findings were reported from a mother–child-focused health visitor intervention in South Africa that benefited the mother-infant dynamics significantly but did not improve maternal mood. 35 In India, a group-based participatory intervention significantly lowered neonatal mortality with no effect on maternal depression until year three of the study.38,69 Likewise, a psychosocial stimulation plus food supplementation intervention in Bangladesh reported beneficial growth and development outcomes for malnourished children with no reductions in the mother’s PPD six months later. 68
In contrast to our intervention, the mother–child-focused psychosocial Learning Through Play (LTP) Plus intervention in Pakistan reduced depressive symptoms significantly, though the child growth outcomes remained unaffected.28,38 However, LTP Plus targeted only women with depression, while our intervention targeted all women. Similar integrated home-visiting intervention packages, such as the early stimulation intervention in Jamaica, 34 the psychotherapy trial in the United Kingdom, 31 and the Thinking Healthy Program in Pakistan, 27 substantially reduced maternal PPD. At the same time, results for child outcomes were mixed. 38 These interventions differed from ours in that they focused directly on addressing PPD by using specific strategies for symptom relief. Furthermore, our intervention lacked a direct focus on PPD. It did not include cognitive restructuring (modifying unhelpful thinking patterns), a core cognitive component that helps address one’s depressive thoughts and emotions.34,70 Supporting our observation further, the LTP program in rural Pakistan that did not use CBT strategies for depressive symptom reduction failed to have an impact on maternal mood. At the same time, it significantly improved maternal knowledge and childcare behaviours. 71 These aspects that were missing from the SPRING intervention may have contributed to its lack of impact on PPD outcomes. However, child feeding practices improved, 39 indicating behavioral change in mothers in favor of the child despite no improvements in maternal mental health, an observation similar to those reported above. Somewhat similar to SPRING, a community-based, peer-led parenting intervention in rural Uganda treated maternal depression as a secondary outcome, yet prevented the worsening of PPD symptoms.72,73 It differed from SPRING in the inclusion of psychological components focused on maternal relationships, conflict resolution, and father involvement. These elements, especially the heightened support, may explain its positive impact. 72 The findings support evidence that mixed interventions with mother-focused components are more effective for treating PPD than psychosocial strategies alone, 38 and also suggest that implementation factors may play an equally important role in improving PPD outcomes.
Findings published from the SPRING trial’s process evaluation reported on key aspects of implementation, such as reach, visit coverage, caregiver coaching, and uptake, that are essential to an intervention’s effectiveness and fidelity. 40 The evaluation attributed the absence of impact to lower-than-expected coverage and uptake of the intervention despite high-quality home visits. They further highlight that the way the CBAs coached the mothers on skill development may have led participants to interpret the central theme of the intervention to be play activities rather than responsive stimulation and mother–child interaction. This perception may have weakened the intended behavioral change mechanisms and affected the overall impact.39,40 In addition, low visit coverage may have affected the intervention’s hypothesized causal pathway (Figure 1, Supplementary Online Material 1), 39 of indirectly improving maternal mental well-being by decreasing the chances of involving family and strengthening mothers’ social support systems. Moreover, TAU, comprising home- and facility-based maternal and child health services, was available to participants in both the trial and control arms. The SPRING psychosocial home-visiting CBT-based intervention was delivered alongside these existing services to mother–child dyads in the intervention arm. However, no additional benefits were observed in maternal depressive symptoms.
Our overall PPD prevalence was 13.1% at 12 months post-partum. Different assessment tools, time points, and cut-off scores across studies make direct comparisons difficult. However, we found two studies from India reporting comparable prevalence estimates at the same assessment time point as ours, one from an urban setting (11.67%) and one from a rural setting (12.5%).74,75 A meta-analysis of 38 studies from the Indian sub-continent reported PPD prevalence ranging from 10.9% to 26.3% in rural settings and an overall pooled prevalence of 22% highlighting varying estimates within the country. It also reported differences in prevalence between rural and urban settings, with lower rates, though non-significant, in the former setting. 76 The largest global meta-analysis of 565 studies to date estimated a PPD prevalence of 17.22% (95% CI: 16.00–18.51); their sub-group analysis of 14 Indian studies found a slightly higher pooled prevalence of 18.81% (95% CI: 13.59–25.44), reflecting the influence of income setting and geographic region. 77 Our findings on PPD prevalence are consistent with both national and global reviews, which highlight substantial variation depending on contextual factors and methodological differences. Many etiological theories of depression point to spontaneous remission, meaning that the natural course taken by the PPD condition comprises a reduction or disappearance of symptoms without any external cause over time, and more so during 6–9 months after childbirth.31,78-81 The psychotherapy trial in the UK attributed no positive treatment effects by 9 months post-partum to spontaneous remission. 31 Similarly, a review of 143 studies from 40 HICs and LMICs, 82 a study from Sudan, 83 and a meta-analysis from India, 76 found a higher prevalence of depression closer to birth, especially around the initial three months, than periods further away. 38 The theory and evidence stated here partly explain our PPD prevalence estimates that are relatively lower than our baseline assumption of 38% depression in control groups. 8 Considering such wide-ranging prevalence rates reported within countries and in existing literature, our setting may have had a lower PPD prevalence initially, which may or may not have changed over time.
Interestingly, despite the low PPD severity in our mothers, we observed somewhat higher-than-expected estimates for suicidal tendencies. At the same time, evidence suggests the risk of suicide is lower in the first year after childbirth, as motherhood can be a protective factor.84,85 Second, suicide is perceived to be associated with increased depressive severity. 86 However, recently, mild to moderate depression has been reported to result in significant suicidal tendencies. 87 Other psychiatric disorders also have suicidality as a symptom, including personality disorders, anxiety, bipolar disorders, and schizophrenia, 88 which could not have been detected by the PHQ-9. 62 Moreover, about 10% of those committing suicide have no evidence of psychiatric illness, indicating non-psychological factors at play in suicidality.89,90 All these may have contributed to our estimates.
Limitations
First, SPRING’s main limitation was low coverage and sub-optimal coaching of carers, which may have led them to perceive the intervention to be play-focused rather than responsiveness-focused, thereby affecting uptake and impact. Second, while PHQ-9 is a well-established screening tool for assessing depression severity, ideally, it should be followed by a clinician-performed interview for confirming the diagnosis. Recognizing this, the WHO recommends the use of validated screening tools such as the PHQ-9 by frontline workers in community settings to identify potential cases and allow for early intervention, including psychosocial support and referrals. In our study, we adhered to all key quality assurance procedures; however, this two-step approach of clinical confirmation of PPD diagnosis following PHQ-9 screening would have further strengthened the study’s overall validity. Third, the PHQ-9 assessment was conducted at a single time point, that is, at 12 months post-partum, which may have prevented us from observing changes to PPD prevalence and severity over time or developing a deeper understanding of the workings of the intervention’s change pathway of improving mothers’ depression. Fourth, we were unable to adjust for family history of psychiatric illness and history of mood or psychiatric disorders, as data on these variables were not collected during the trial. This limits our ability to account for potential underlying risk factors for PPD adequately.
Conclusions
Our analysis found that the SPRING intervention did not significantly impact PPD outcomes, aligning with growing evidence showing that mother–child-focused psychosocial interventions alone are often insufficient to improve maternal depression. These findings highlight two critical lessons: First, integrated programs require specific, evidence-based strategies directly targeting PPD symptom reduction, alongside components supporting mother–child interactions and child-rearing practices. Second, implementation challenges—particularly in coverage and uptake—appear to affect the effectiveness of even well-designed evidence-based interventions. Moreover, with at least one in eight mothers affected by PPD at 12 months post-partum in our study, a persistent burden consistent with other Indian evidence, the need for more effective interventions is urgent. As one of few rigorous evaluations of a community-based intervention in rural India, our study points to three key requirements for future program design and delivery: (a) explicit inclusion of components for PPD reduction alongside mother–child interaction strategies, (b) strengthened implementation procedures to ensure high coverage, uptake, and consistent delivery quality, and (c) multiple PPD assessment timepoints (including baseline) to better understand symptom trajectories and intervention timing effects through the first year after childbirth. Furthermore, interventions sensitive to the changes in PPD (including prevalence, severity, and remission patterns) during the post-partum period may give us a chance to achieve better uptake and effectiveness. These adaptations, with careful implementation and monitoring, could lead to tangible mental health improvements for mothers in LMIC settings.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Acknowledgements
We would like to thank Lu Gram, Seeba Amenga-Etego and Satya Narayan Panchal for designing and managing data management software for surveillance data. We extend our thanks to the National Health Mission, Haryana, Ministry of Health and Family Welfare, for allowing access to their team working at the ground level. We would also like to acknowledge the important role played by the Sangath NGO as the implementing organization for SPRING in India. Furthermore, this work would not have been possible without the outcome assessors who put in sincere efforts to collect high-quality data regardless of unfavorable weather conditions at times or long distances; the data management team who were diligent in entering and processing collected data; and the CBAs who delivered the intervention. Lastly, we were able to complete our research with the support of the mothers who agreed to participate and cooperated with us despite their busy schedules.
Consent to Participate and Publish
Participating SPRING mothers provided informed consent twice—at the enrolment stage and the beginning of the outcome assessment phase.
Data Availability Statement
The study datasets presented in this study are available in these online repositories. Their names and accession number(s) can be found at: World Bank International Household Survey Network (IHSN) microdata catalogue (
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
This study involving human participants was performed in line with the principles of the Declaration of Helsinki, 1964. Ethical approval was granted by the London School of Hygiene & Tropical Medicine research ethics committee, UK (for SPRING: 23 June 2011, approval number 5983; for secondary analysis of the SPRING data: November 14, 2017, approval number 14445)—and from Sangath Institutional Review Board, India (SPRING: February 19, 2014). The study also received approval from the Indian Council of Medical Research’s Health Ministry Screening Committee (HMSC) (SPRING: 24 November 2014).
We adhered to the Consolidated Standards of Reporting Trials (CONSORT) guidelines (Schulz KF, Altman DG, Moher D, for the CONSORT Group. CONSORT 2010 Statement: updated guidelines for reporting parallel group randomized trials). The CONSORT checklist is uploaded as “supplementary online material 2.”
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A Wellcome Trust Programme Grant (Award No: 093615) funded SPRING. Supplementary funding was received from the World Bank Strategic Impact Evaluation Fund (SIEF; Contract No: 7180224).
Prior Presentations
None.
Simultaneous Submission to Another Journal or Resource
None.
Trial Registration
Trial registry: Clinicaltrials.gov; Registration number: NCT02059863; URL:
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.