
Abstract
The literature on the relationship between late acquired dual-sensory impairment (DSI) in older adults and the ability to remain independent is limited. A systematic search of the literature was conducted to assess the impact that late life acquired DSI in older adults has on their ability to remain independent within their homes. Exclusion and inclusion criteria were applied to the papers identified and eight qualified for inclusion in the review. Each selected paper was assessed using a quality rating scale. Country of origin, population studied, age, vision, and hearing criteria all varied between papers. They provide evidence that DSI affects everyday competence, and this effect is complicated by physical comorbidities, mental health, and social factors.
Keywords
Introduction
Dual-sensory impairment (DSI) is defined as the loss of vision and hearing in combination or concurrent impairment (Diehl, 1998). The term deafblindness is also frequently used to describe the combined deterioration or loss of senses, with both DSI and deafblindness used interchangeably (Wittich, Southall, Sikora, Watanabe, & Gagné, 2013): this article uses the term DSI. An individual who has difficulties with their vision and hearing can be described as having DSI if their combined vision and hearing loss causes difficulties with communication, access to information, and problems with mobility (Department of Health, 1997). As individuals age, problems may develop with both vision and hearing, and as a result, older adults are the largest group of people with DSI: they can be described as having late acquired DSI to distinguish it from congenital DSI and DSI acquired earlier in life (Swann, 2010). In the literature, little is written on late acquired DSI in comparison with congenital DSI, which was once a common consequence of congenital rubella syndrome.
A report from the Centre for Disability Research (Robertson & Emerson, 2010) estimates that there are currently between 132,000 and 356,000 people with DSI in the United Kingdom. It is estimated that this number will increase substantially to about 569,000 by 2030, and of these, about 245,000 will have severe dual impairments (the authors estimated severe impairment numbers on the basis of specific diagnoses). A large-scale survey of the opinions and circumstances of visually impaired individuals in Great Britain found that the majority were over the age of 50 years (Douglas, Corcoran, & Pavey, 2006). Similar findings were reported in the Cambridge dataset, collected in 2005: 404 of 539 participants were aged over 50 years and had acquired hearing and vision loss in later life (Bodsworth, Clare, & Simblett, 2011). Vision loss can occur as a result of eye conditions such as cataracts and macular degeneration. Hearing loss can be caused by a variety of factors, including environmental causes, such as being exposed to high levels of noise, illness, or presbycusis, a gradual decrease in the ability to hear high-pitched sounds with increasing age. The number of older individuals with DSI is expected to increase as a consequence of the ageing population: the focus of the DSI literature is often on the increasing prevalence of DSI with increasing age (Schneider et al., 2012).
For the purposes of this review, older age was defined as age 50 years and above, in line with the Cambridge dataset findings referred to earlier. Everyday competence is defined as ‘. . . one’s ability to function and live independently in the community’ (Brennan, Su, & Horowitz, 2006). Independence may be measured in terms of ability to carry out activities of daily living (ADLs) and instrumental activities of daily living (IADLs). ADLs refer to activities associated with everyday functioning, and the focus is on an individual’s ability to conduct these tasks independently. Activities that are essential in order to function independently (ADLs, for example, ability to get dressed or use the toilet) have been seen as important indicators of disability in ageing studies and clinical practice (Kingston et al., 2012). In contrast, IADLs refer to more complex and demanding tasks such as managing medication and finances, having a telephone conversation, shopping, and preparing meals: these activities are not necessary for basic functioning but enable an individual to live independently in the community.
Studies have suggested that everyday competence is sometimes lost in a ‘hierarchy’, that is, more complex skills are lost first beginning with the loss of competence with IADLs, for example, managing money, followed by the loss of competence with ADLs, for example, indoor mobility, dressing, and bathing. Difficulties with managing finances, medication, and using the telephone may result from impaired cognitive function, whereas difficulties with shopping, cooking, and housework, for example, may result from impaired physical function (Seidel, Brayne, & Jagger, 2011). Kingston et al. (2012) found a strong hierarchical ordering to loss of ability in older adults (over 85 years old) recruited from general practices in the North East of England in a wide range of ADL and IADL tasks. Individuals reported cutting toenails as the first activity they found difficult, followed by washing hands and face and then feeding. Women reported greater difficulty with tasks requiring strength such as shopping and heavy housework, in comparison with men who reported difficulty walking; however, women were more likely to report difficulty with each activity than men. It may be difficult to tease out the role of sensory impairments, physical illnesses, and advancing age when people have difficulties with everyday tasks in later life.
Loss of everyday competence may have a profound impact on an individual’s ability to remain functioning and safe in their own home. Research indicates that most older individuals wish to remain autonomous and in their own homes for as long as they can: it is not unusual for individuals to choose autonomy over safety (Pavey, Douglas, Hodges, Bodsworth, & Clare, 2009). Safety is an important issue: individuals with DSI may be unable to hear alarms, smoke detectors, sirens, fast moving vehicles, and other traffic noises, with consequences for their safety and security as well as daily functioning. Risks are not just physical: individuals with DSI report poorer self-rated health (Crews & Campbell, 2004), depression (Guthrie, Thériault, & Davidson, 2016), reduced quality of life (Heine & Browning, 2014), and less interaction with social networks (Gopinath et al., 2012) than those without dual impairments. Visual impairments have a greater impact on the ability to complete many daily tasks compared with hearing impairments, and this may disrupt previously established behaviours relating to physical, psychological, and social functioning (Brennan & Silverstone, 2000).
Research has demonstrated the impact of single-sensory loss on an individual’s independence and ability to carry out ADLs. There has, however, been less focus on dual loss and how that affects people’s lives. The impact of DSI is thought to be greater than single-sensory loss, as loss in one sensory modality can be compensated to some extent using other sensory modalities: however, if loss occurs in two modalities, this will compromise the person’s ability to compensate (Brennan, 2003).
Mental health is not the focus of this review, but adds further complexity to the relationship between DSI and everyday competence. Studies have started to develop an understanding of the link between sight loss and dementia in later life (Lawrence & Murray, 2010). Lin et al. (2011) found hearing loss to be strongly and independently associated with incident dementia, but more recent papers report conflicting findings (Hong, Mitchell, Burlutsky, Liew, & Wang, 2016; Taljaard, Olaithe, Brennan-Jones, Eikelboom, & Bucks, 2016). Depression (Heine & Browning, 2014; Huang, Dong, Lu, Yue, & Liu, 2010; Mener, Betz, Genther, Chen, & Lin, 2013) and loneliness (Pronk et al., 2011) add further complexities. Whether hearing loss is a marker for early stage dementia or is actually a modifiable risk factor for dementia deserves further study. Previous studies have argued that sight loss is also associated with depression (Carrière et al., 2013) and suicide (Lam, Christ, Lee, Zheng, & Arheart, 2008).
This review aims to systematically assess what is known about the effect of late life acquired DSI in older adults on their ability to remain independent and carry out everyday tasks.
Method
The systematic search was limited to scientific academic journal databases, plus bibliographies of systematic review articles published in the last 5 years. Two systematic reviews have been published recently (Heine & Browning, 2014, 2015) but neither addressed everyday competence. Initially, PubMed, PsycINFO, and CINAHL were searched for publications between 2001 and 2012 in order to identify the most recent research. The search was then re-run as far back as the electronic databases would allow. The following search terms were used (where the medical subject heading [MeSH] was used this is indicated in parentheses):
Old age. We included studies which defined old as age 50 years or above. The following terms were used: age OR ageing; aged (MeSH); elderly; and older.
Acquired DSI or late acquired DSI. The following terms were used: deafblind disorders (MeSH); deafblindness; hearing loss AND blindness (MeSH); persons with hearing impairments AND visually impaired persons (MeSH); sight loss AND hearing loss; and vision AND hearing impairment.
Outcomes. The following search terms were used: ability to remain independent; activities of daily living (MeSH); daily activities; everyday competence; and instrumental activities of daily living (IADL).
The following inclusion criteria were used for journal articles identified in the search, and only papers meeting these criteria were included:
Peer-reviewed publication;
Reports primary data;
Focus on DSI and older age (defined as age of 50 years and older);
Data on everyday competence/ADLs/IADLs.
The initial scoping search produced 134 publications across all databases. Review of titles and abstracts identified 23 potentially relevant papers. These papers were read independently by the three team members. The team met and agreed which papers fitted the inclusion criteria for the review. Disagreement/discrepancies were resolved through re-examination and discussion by the reviewers. Only eight papers met the inclusion criteria. These eight papers were quality assessed based on a modified version of the ‘Standard Quality Assessment Criteria for Evaluating Primary Research Papers from a Variety of Fields’ (Kmet, Lee, & Cook, 2004). Each paper was scored out of a total of 28 points; the score depended on the extent to which specific criteria were met (yes = 2, partial = 1, and no = 0). Items not applicable to a paper were excluded from scoring. No paper fully met the quality criteria for good design. Scores ranged from 9 to 21 with close agreement between the three reviewers (no more than 1 point difference) on five papers, which scored in the range 18–21 on the quality criteria: in analysing the papers, these were given greater weight.
The 15 papers which did not meet the study criteria are listed in Appendix 1. The main reasons for non-inclusion were as follows: nine were expository/review papers contributing no primary data; four did not address everyday competence; and two presented no primary data on DSI. We did not exclude qualitative studies, although none met the criteria for inclusion in the review. There was no formal criterion in the review for acquired DSI. One of the included studies states that the population studied had acquired DSI. One study focused on a population in contact with Deafblind UK and probably included some individuals with congenital DSI: of the 42 participants, 2 used sign language and 2 used the deafblind manual alphabet. The remaining six studies refer to age-related sensory impairments.
Results
Eight papers met the review criteria: they came from disparate geographical areas; used differing age inclusion criteria; were aimed at differing sample populations; and used various sampling strategies and different means of assessing sensory impairment. Details are set out in Table 1. Three studies assessed visual and hearing impairment objectively using audiometry and visual acuity (Deepthi & Kasthuri, 2012; Harada et al., 2008; Heyl & Wahl, 2012), and a fourth employed a practical assessment (Grue et al., 2009). The other five studies used self-reported/self-rated assessment of hearing and vision. Many of the measures used in the studies relied heavily on self-report and this limits their usefulness. Heyl and Wahl’s (2012) study focuses on the link between cognitive resources and everyday function rather than the impact of DSI. Deepthi and Kasthuri’s study is largely descriptive and omits details of ADL scores: it appears that of 65 people with DSI, 36 were ‘dependent’ but this is not operationally defined.
Comparison of core features of the eight papers which met the review criteria.
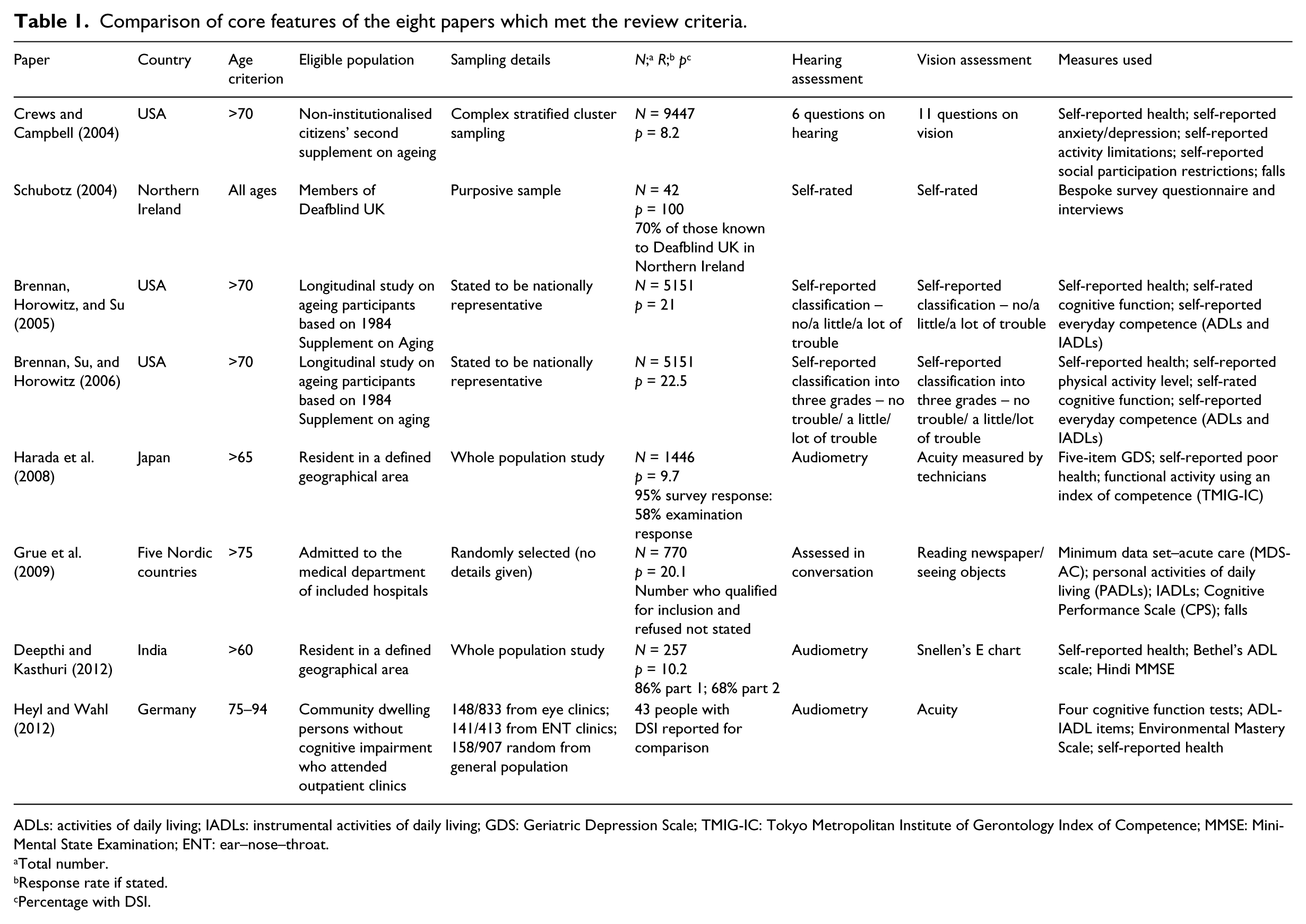
ADLs: activities of daily living; IADLs: instrumental activities of daily living; GDS: Geriatric Depression Scale; TMIG-IC: Tokyo Metropolitan Institute of Gerontology Index of Competence; MMSE: Mini-Mental State Examination; ENT: ear–nose–throat.
Total number.
Response rate if stated.
Percentage with DSI.
Population
The age criterion varied in each paper. The majority of papers recruited participants who were over the age of 60 years without an upper age cut-off. However, Heyl and Wahl (2012) had a cut-off upper age of 94 years. Schubotz involved participants of all ages as individuals themselves volunteered to take part: three quarters of participants were aged over 60 years and half aged over 80 years (Schubotz, 2004).
Grue et al.’s (2009) participants were randomly selected for inclusion from those admitted to medical departments in acute hospitals in five Nordic countries: participants who were discharged within 24 hr, critically ill, or transferred to a surgical unit within 48 hr were excluded. Participants in Crews & Campbell’s (2004) study were US non-institutionalised citizens included in the 1994 Second Supplement on Ageing. The only inclusion criterion in Schubotz’s (2004) study (carried out in Northern Ireland) was to be a member of Deafblind UK, and this study probably included some individuals with congenital DSI. Harada et al. and Deepthi and Kasthuri’s participants included all residents of a defined geographical area: in the first case (Harada et al., 2008), a rural Japanese town, and in the second (Deepthi & Kasthuri, 2012), two villages in South India. Heyl and Wahl’s (2012) participants were community dwelling individuals without cognitive impairment who attended regional outpatient clinics in Germany. Brennan et al.’s (2005, 2006) two US-based studies involved data obtained from the Longitudinal Study of Ageing (LSOA) participants based on 1984 Supplement on Aging.
Measures employed
Participant self-report was commonly used, but in addition, most studies employed some standardised measures. The studies varied in terms of the training/qualifications of persons carrying out the research. Grue et al. used assessments carried out by a geriatrician or a specifically trained nurse, including the Minimum Data Set–Acute Care Canadian version 1.1, which is validated and tested for reliability; the Cognitive Performance Scale; and ratings of personal activities of daily living (PADLs) and IADLs (Grue et al., 2009). Harada et al.’s (2008) study involved interviews carried out by trained public health nurses and local welfare commissioners using a structured questionnaire together with the five-item Geriatric Depression Scale and the Tokyo Metropolitan Institute of Gerontology Index of Competence (TMIG-IC), a 13-item functional activity scale. Deepthi and Kasthuri (2012) used Bethel’s ADL scale and the Hindi Mini-Mental State Examination. Heyl and Wahl (2012) used four cognitive function tests, plus what they described as ‘a selection of 10 items from classic ADL-IADL scales’ and an Environmental Mastery Scale. Brennan et al.’s (2005, 2006) two studies used self-reported everyday competence on ADL and IADL scales. Schubotz (2004) used an unstandardised survey questionnaire and interview, and Crews and Campbell (2004) reported a secondary data analysis.
Impact on everyday competence
In terms of the impact of DSI on everyday competence, this was directly addressed in one paper (Brennan et al., 2005), which found that compared with loss of hearing or vision alone, DSI was associated with greater impairment of IADL tasks than ADL tasks. Preparing meals, shopping, and using the telephone became increasingly difficult as levels of DSI increased. A second paper (Brennan et al., 2006) reported a 2-year follow-up interview on the same sample and found that the strength of the relationship between DSI and high levels of functional restrictions decreased over time. However, the study relied on self-report of sensory impairment at baseline and did not take account of changes in hearing and vision over time. Schubotz (2004) reports findings related to mobility, getting out of the house, and leisure activities: his sample had high levels of dependence on others and found access to public areas difficult, but his findings relate to a tightly defined small group of people in contact with Deafblind UK. Grue et al. (2009) found that DSI was associated with loss of IADLs but not with falls.
Two other papers have additional information on this area. Crews and Campbell (2004) found that people with DSI reported increased difficulty in mobility (in terms of walking, getting outside, and getting into or out of bed/chair); in meal preparation; and medication management as well as restrictions in social participation. Harada et al. (2008) found that DSI was linked with a threefold increase in the likelihood of having depression in both men and women, and along with visual impairment alone, DSI was associated with a more than threefold increase in the likelihood of ‘reduced functional activity’ as measured using the TMIG-IC. Table 2 compares the findings reported in three of the papers (Crews & Campbell, 2004; Harada et al., 2008; Heyl & Wahl, 2012) and shows that there is a gradient of increasing difficulty with people with DSI reporting more difficulty in relation to ADLs and IADLs than people with visual impairment alone, who in turn report more difficulty than those with hearing impairment alone.
Comparison of ADL and IADL results from Crews and Campbell (2004), Harada et al. (2008), and Heyl and Wahl (2012).
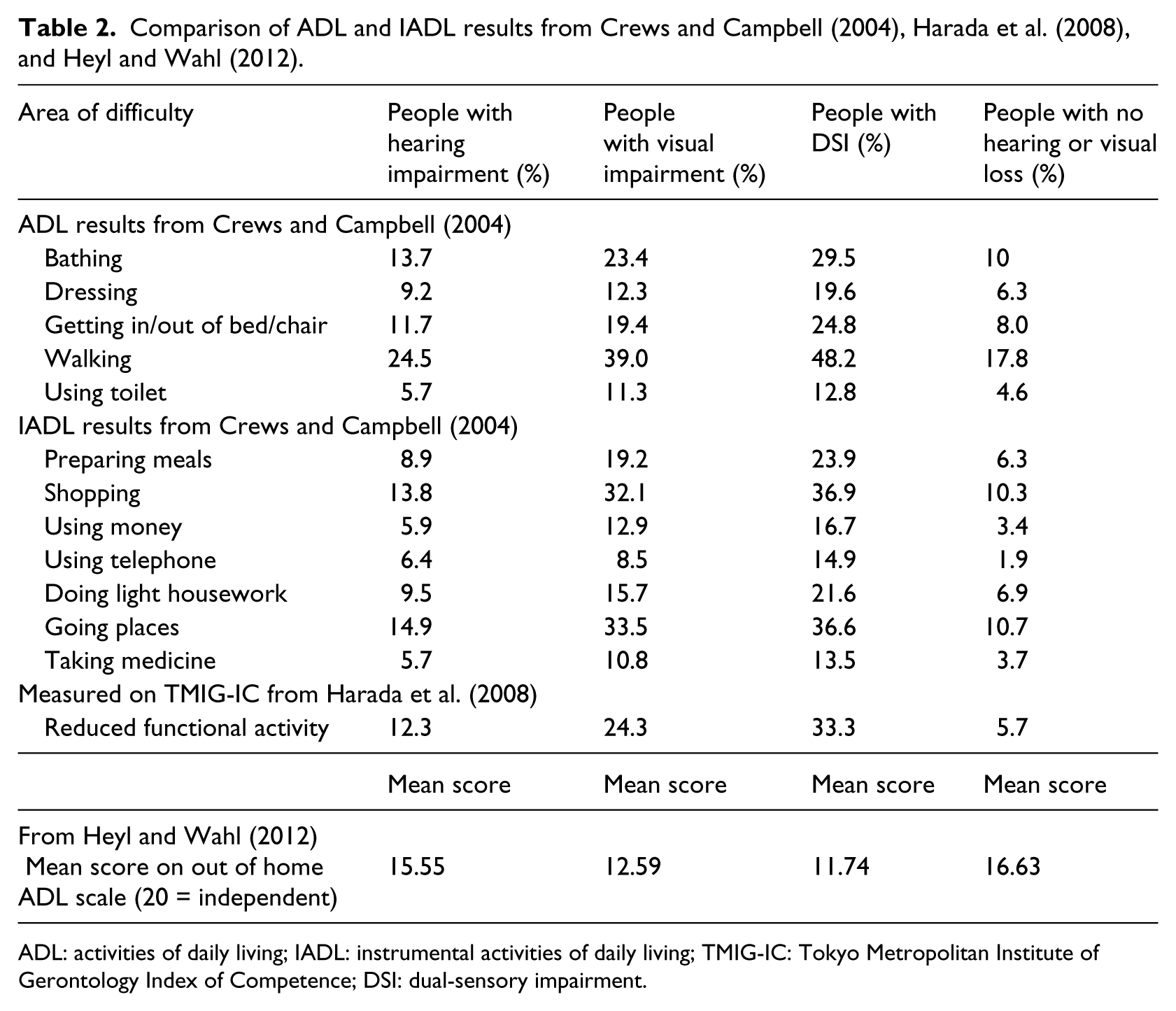
ADL: activities of daily living; IADL: instrumental activities of daily living; TMIG-IC: Tokyo Metropolitan Institute of Gerontology Index of Competence; DSI: dual-sensory impairment.
Discussion
Research into acquired DSI is limited, and research focusing on its effect on everyday competence is even more restricted. We identified only a small number of papers from different areas of the world. One paper reported UK-based research, four American-based research studies, two northern European studies, and one conducted in India. The differences between these countries in terms of the health and social care contexts complicate comparison of the findings, although taken together the papers suggest a gradient of increasing difficulty in that those with visual impairment appear to experience more difficulty than those with hearing impairment and those with DSI report more than those with single-sensory impairment.
Limitations of the studies identified include differences in how they defined DSI, in how they assessed DSI, and in the age eligibility criterion used: this complicates analysis of their findings and makes it difficult to draw firm conclusions. Further research is clearly needed, and future studies might benefit from researchers using clear entry criteria with an agreed definition of DSI and an agreed age cut-off. One question is whether objective measurement of vision and hearing should be carried out to determine whether people have DSI: is it sufficient to rely on potential participants’ accounts of how their vision and hearing impairments affect their daily lives? Is it appropriate to use an age cut-off for age eligibility? The studies included in the review variously used 65, 70, and 75 years. Similarly, the studies reviewed here used differing approaches to assess ADLs and IADLs. Standardised assessments have much to commend them, but it is likely that combining qualitative and quantitative measures would add to our understanding of the impact DSI has on people’s everyday lives and how they cope with the challenges they face.
With regard to physical health, falls are an obvious area of risk in people with DSI. Grue et al. (2009) found a complex relationship between falls and sensory loss and reported that falls were common among their participants. Recently, a link between DSI and ‘all cause’ mortality has been found (Fisher et al., 2013): older men with DSI had a greater risk of dying from any cause, and particularly cardiovascular disease, when followed in a 5-year study.
If, as this review suggests, IADLs, getting about, and social participation are affected earlier than ADLs in older people with DSI, early recognition of DSI combined with measures to support IADLs might be of benefit in maintaining independence. A multi-facetted approach to intervention is likely to be helpful and might be a fruitful area for future research, combining holistic assessment with access to acceptable non-stigmatising aids and adaptations to assist with both sensory impairments and physical comorbidities. Alongside this there is a public health message about the importance of physical, mental, and social activity contributing to health in later life. The Foresight Project proposed five ways to mental well-being: connect, be active, take notice, keep learning, and give (The Government Office for Science, 2008). These five areas could offer a structure for supporting everyday competence in older people with DSI.
Finally, is age the key issue in whether people can live independently or alternatively is the key issue DSI? Or should we understand the impact on everyday competence as resulting from an interaction between age and DSI? The papers reviewed here confirm a relationship between age and DSI and perhaps an attempt to distinguish between the two in terms of impact on everyday competence misses the point. As people age, they tend to accumulate illnesses (World Health Organization, 2011), and age-related changes that impact on their ability to live independently may restrict their activities and may have an impact on their mental health. Social isolation (Gopinath et al., 2012), loneliness (Heine & Browning, 2002), economic constraints (Brennan & Bally, 2007), and mental health challenges (in terms of both mood (Heine & Browning, 2014) and cognitive impairment (Hong et al., 2016)) are some of the challenges that may accompany ageing and add further complexity to the relationship between DSI and everyday competence. Sensory changes are part of this accumulation, and the question as to which is more important, age or sensory impairment, is irrelevant. For older adults living with DSI, a more important question is how might they be supported to maintain their independence and competence in ADLs and IADLs. In conclusion, the evidence suggests that DSI impacts on day-to-day activities and lifestyle, alongside the possibility of mental health impact, increased falls, and increased mortality.
Footnotes
Appendix 1
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Sense, the national charity supporting and campaigning for deafblind people.