
Abstract
The study compares levels of physical activity, body composition values, and emotional well-being of school-age children and youths with visual impairments (n = 115) in specialized schools with those of sighted children (n = 118) in mainstream schools. The methodology included pedometers, bioelectrical impedance analysis, and the WHO-Five Well-being Index. In all relevant parameters, students with visual impairments achieved results comparable to those of sighted students, and the degree of visual impairment did not correlate significantly with the parameters. The results confirm the positive effects and the importance of physical activity for students with visual impairments. High levels of physical activity are possible which provide health-related benefits for children and youths with visual impairments.
Keywords
Theoretical background
According to the World Health Organization (WHO), physical inactivity is a considerable health problem. It is regarded as one of the leading risk factors for health and can lead to negative adaptations in the body. Some proven effects are muscle atrophy, an increase in body fat and enhanced risk of sickness, an impact on overall well-being as well as deterioration in cardiovascular performance (WHO, 2010).
Lack of physical activity is especially worrisome in the case of children and youths, since patterns of lifelong physical activity are set in childhood (Barnett, van Beurden, Morgan, Brooks, & Beard, 2009; Williams, Armstrong, Eves, & Faulkner, 1996). Stuart, Lieberman, and Hand (2006) pointed out that children who are regularly physically active are more likely to have active lifestyles in adulthood. For this reason, the school and school sports environment should make a contribution and encourage students to participate in sports and activities, enabling them to lead active and self-determined lives beyond school sports (Giese, Giessing, & Eichmann, 2014). That applies to all individuals, including those with visual impairments (VI).
Research in Germany on individuals who are visually impaired or blind is limited and is concerned mostly with educational and didactic aspects and ophthalmology. Research on exercise and sports with individuals who are visually impaired or blind is particularly scarce. More research in this area is essential in order to gain further information about effects of VI on physical and psychological health. Moreover, it should be noted that in Germany the discussion of sports for children and youths with disabilities does not take place in the form of a special discipline but rather within the disciplines of sports education and sport medicine.
Current international research pertaining to children with VI has already produced some findings. Many studies have reported that children who are visually impaired have lower levels of physical activity (Augestad & Jiang, 2015; Haegele & Porretta, 2015a; Houwen, Hartman, & Visscher, 2009; Kozub & Oh, 2004). Because of these reduced physical activity patterns, children and youths with VI tend to have lower levels of health-related physical fitness and poorer body composition values compared to sighted children (Lieberman, Byrne, Mattern, Watt, & Fernández-Vivó, 2010; Lieberman & McHugh, 2001). Augestad and Jiang (2015) presented a systematic literary review of articles published between 1984 and 2014 that are related to physical activity, physical fitness, and body composition among children and youths with VI. Their general findings revealed and confirmed lower levels of physical activity, physical fitness, and body composition compared to children and youths with no VI. Their results are in accordance with Haegele and Porretta (2015a) who also reviewed published articles related to physical activity of school-aged individuals with VI. Nevertheless, studies have shown that children who are visually impaired can improve their physical health condition and obtain levels comparable to those of sighted children given equal opportunities for participation in regular physical activity (Cervantes & Porretta, 2013; Stuart et al., 2006; Williams et al., 1996).
Moreover, studies of adults with VI have shown that VI can be associated with an increased risk of emotional distress and reductions in perceived quality of life (Stelmack, 2001; Wang, Mitchell, & Smith, 2000). There also has been research on the connection between physical activity and perceived quality of life in adults with VI (Haegele, Famelia, & Lee, 2016; Holbrook, Caputo, Perry, Fuller, & Morgan, 2009; Labudzki & Tasiemski, 2013). Whereas the study by Holbrook et al. (2009) reported no significant connection between physical activity and perceived quality of life, the findings of Labudzki and Tasiemski (2013) and Haegele et al. (2016) confirmed that physical activity can impact the quality of life for adults with VI. Haegele et al. (2016) pointed out that more research is necessary which focuses on the influence of physical activity on quality of life of individuals with VI.
Shapiro, Moffett, Lieberman, and Dummer (2005) and Stuart et al. (2006) stated that children and youths with VI generally have fewer incentives and opportunities to participate in activities, which provide the amounts and kinds of physical stimulation needed, and which are common for sighted children. There has also been research on barriers to physical activity for children and youths with VI (Haegele & Porretta, 2015a; Shields, Synnot, & Barr, 2012; Stuart et al., 2006). In a recent review, Shields et al. (2012) identified various barriers and facilitators to physical activity for children and youths with disabilities such as personal, social, environmental, and policy restrictions which aggravate their limited engagement in physical activities. More precisely, the barriers included a lack of skills and knowledge, the child’s preferences, fear, negative attitudes to disability, parental behavior, inadequate facilities, cost, and a lack of transport, appropriate programs, and staff capacity (Shields et al., 2012). The facilitators included the child’s desire to be fit and active, practicing skills, family support, involvement of peers, accessibility and proximity of facilities, better opportunities, skilled staff, and information dissemination (Shields et al., 2012). According to Shields et al. (2012), these barriers and facilitators can influence the amount of physical activity of children with disabilities.
Skaggs and Hopper (1996) also noted that physical fitness levels of children in specialized schools for children and youths with VI are higher than those of children in mainstream schools and may be explained by less effective sports programs and sports environments for individuals with VI in mainstream schools. Recent research has revealed no differences in physical activity between children with VI educated in specialized and integrated school settings (Gronmo & Augestad, 2000; Haegele & Porretta, 2015a). According to Haegele and Porretta (2015a), low physical activity levels of school children with VI may be connected with perceived barriers to participation such as the non-availability of appropriate opportunities, rather than educational setting. However, these implications cannot be ignored in the current debate about the inclusion of students with disabilities in general education classes (Lieberman & McHugh, 2001). Lieberman and McHugh (2001) stated that it is important to promote the implementation of appropriate physical activity programs and incentives in all educational settings. The implications are especially relevant for the school situation in Germany where children with VI are being schooled both in special schools and also in general schools.
The purpose of this study was to investigate (1) the physical activity, (2) body composition, and (3) emotional well-being of children and youths of a specialized school who are blind and visually impaired. The study also examined whether the degree of the VI does in fact affect the parameters in question as is generally assumed.
The educational system of the visually impaired in Germany
One of the peculiarities of the German-speaking inclusion controversy and its connection to the special schools’ right to exist is its discussion primarily as a school infrastructure debate (Herz, 2014). This national peculiarity is based among other things on the fact that Germany relies on a very differentiated school system. In the special school system alone, for example, there are eight distinct school types for different forms of impairment. Whereas a high degree of special educational expertise could arise out of this differentiated system, the German school system finds itself in the cross-fire of the criticism in international educational reporting due to its selective and structured nature (Muñoz, 2007). So far, no unified interpretation of the United Nations Convention on the Rights of Persons with Disabilities (CRPD) could be established in this complex interchange in Germany and the school context is generally more concerned with teaching more pupils together, be it with or without impairment.
Whereas 31.4% of all pupils needing special education in Germany during school year 2013/2014 were schooled inclusively in their local schools with able bodied peers, in the category of VI it was a high as 37.9% (Klemm, 2015). It should be noted, however, that this value varies greatly depending on the state and age of the child. In Schleswig-Holstein, for example, 100% of all students with VI are schooled inclusively, in the state of Hesse, it is only 21.4%.
Methods
Study design and participants
The cross-sectional study assessed 115 children and youths who are visually impaired and blind attending a specialized school for children who are visually impaired and blind (M age = 16.0; standard deviation [SD] = 3.1) in Germany. The participants did not have other cognitive impairments and the group consisted of 67 male and 48 female students. Criteria for VI of this group of school children and youths are based on German law. VI is defined as a visual acuity of 0.3 or less in the better eye with best possible correction. In German law, severe VI is defined as a visual acuity of 0.05 or less in the better eye with best possible correction. Blindness is defined as best corrected visual acuity of 0.02 or less in the better eye or a visual field restriction to no more than the central 5°. In order to identify deficits in physical activity, body composition, and emotional well-being, the results were compared with a control group of sighted children and youths (n = 118) who attended a mainstream school in Germany. Of the 118 sighted school children and youths (M age = 13.8; SD = 2.5), 63 were males and 55 females. The specialized school and the mainstream school are located in different federal states and in different geographical areas of Germany. In both schools, the specialized school for children with VI and the mainstream school of the sighted control group, students can obtain the general secondary school-leaving qualification for university matriculation. The children and youths of both schools strive for the highest schooling degree in Germany. Besides, the curriculums of the mainstream school and the specialized school for children and youths with VI are similar and comparable. The schools’ curriculums follow the guidelines of their federal state in all types of schools. The specialized school does not have an adapted curriculum for their students with VI.
School for children and youths who are visually impaired and blind
The children and youths with VI who participated in the study attended a specialized school, a state-recognized private special school with emphasis on “visual impairment.” It is combined with a boarding school where students can, but need not, board. However, it is often necessary because the catchment area of this specialized school encompasses the entire German-speaking region. The school is the only basic secondary school institution in the German-speaking geographic area for students with VI and also includes a counseling center for students included in mainstream schools. Instruction follows the guidelines of its federal state in all types of schools and leads to the federal state’s school-leaving certificate. The acceptance criteria for the school are based on the German Law for the Visually Impaired and Blind. Moreover, the specialized school sets priorities in physical activities and sport programs. Students can experience physical activities in physical education and extracurricular sports. The school creates opportunities for achieving various exercise skills by offering a variety of physical activities which include the classic sports as well as trend or outdoor sports (Giese & Zink, 2015). Male and female students of the school’s classes 5–13 took part in the study. In general, students of the school’s classes 5–10 have two physical education classes a week (90 and 45 min). The same applies to the control group of sighted students in the mainstream school. The amount of physical education varies in the schools’ classes 11–13 depending on whether students make physical education a priority in their school schedule. The minimum amount of physical education is 90 min a week. Moreover, extracurricular sports is optional in both schools.
Instruments
The methodology included various analytical instruments. The test procedures were performed by researchers who are experienced with children with VI and with the help of teachers of the special school facility for children and youths with VI.
Pedometer
OMRON Walking Style Pro Pedometers were employed in the study which allow for different carrying methods such as in trouser pockets or on shoes. The pedometers were easy to use since they are constantly active and automatically begin counting steps. The pedometers measured the number of steps of 7 week days. The children and youths with VI carried the pedometers an average of 6.8 days. The control group of sighted children and youths carried the pedometers an average of 6.6 days. The participants with VI used the same contemporary pedometers as the control group. The pedometers have not been validated for children with VI.
Bioelectrical impedance analysis
A bioelectrical impedance analysis (BIA) was performed to measure body composition. BIA is a commonly used method of measuring various components of the body’s constitution. Different components of the human body such as muscle mass, body fat mass, fat-free mass, bone mass and percentage of body fat, muscle fat, and body fluids can be determined. The amount of visceral (organic) fat and the basic metabolism of the body can also be ascertained. BIA makes physical contact by means of measuring electrodes on hands and feet. The test persons are measured while standing with their feet placed on designated areas and holding special grips in their hands. The technology is non-invasive and quick since the measurement results for body components are displayed with minimal delay.
The professional body composition analyzer (TANITA MC-180MA) used in the study is employed in the medical field as an accredited analysis device. According to the manufacturer, it can be used with children aged 5 years and above. Two parameters were considered in this study – the percentages of body fat and muscle mass.
WHO-Five Well-being Index
The WHO-Five Well-being Index (WHO-5) is a short, self-administered questionnaire that measures current emotional well-being. It includes five positively worded statements relating to positive mood (good spirits, relaxation), vitality (being active and waking up fresh and rested), and general interest (being interested in things) (Diabetes Attitudes, Wishes, and Needs [DAWN], 2006; WHO, 1998). Each item is rated on a 6-point Likert scale from 0 to 5. The raw score is calculated by summing the scores (ranging from 0 to 25) and multiplying by 4 to obtain a percentage score (ranging from 0 to 100). A percentage score of 0 represents worst possible and a score of 100 best possible well-being. A score of 50 or below indicates low mood and a score of 28 or below indicates likely depression. A 10% difference can be regarded as a significant difference in emotional well-being (DAWN, 2006; WHO, 1998).
The WHO-5 has been validated in various studies with regard to its clinical and psychometric relevance (http://who-5.org). The WHO-5 can be applied ad hoc to obtain information on individuals’ mood and has already been successfully employed with children and in educational institutions (Allgaier et al., 2012; DAWN, 2006; Wang & Bian, 2011). The WHO-5 questionnaire has not been validated for children and youths with VI.
Statistical analysis
A statistical analysis was performed using the analytics software SPSS (22.0). The independent t-test was used to determine whether there were statistical differences in the means of physical activity, body composition (percentages of body fat and muscle mass), and emotional well-being between children with and without VI. Also, the non-parametric Mann–Whitney test was used to analyze the group differences because not all data were normally distributed. Correlation analyses were performed to examine associations between the parameters. In particular, the correlation between the degree of VI (%) and physical activity, body composition, and well-being among children with VI was analyzed. The Spearman rank correlation was included here to investigate relationships. The significance level was set to .05.
Results
Descriptive and inferential statistics
There were no significant differences in the parameters physical activity, body composition, and emotional well-being. The results are displayed in Table 1. Results confirm comparable physical activity in everyday movement of children with VI to sighted children (p = .213). Also, children and youths with VI showed none of the expected adaptations such as low muscle substance ratio and increased body fat percentages. There were no significant differences in the components of body composition. Body fat percentages and muscle mass percentages of female (p = .672; p = .667) and male (p = .578; p = .570) children and youths with VI were comparable to sighted children. The same applies to the results of the WHO Well-being Index. The WHO Index scores of the children and youths with VI compared favorably with their sighted counterparts (p = .328).
Mean values and p-values of physical activity, body composition, and emotional well-being for children and youths with and without visual impairment (VI).

SD: standard deviation; WHO-5: WHO-Five Well-being Index.
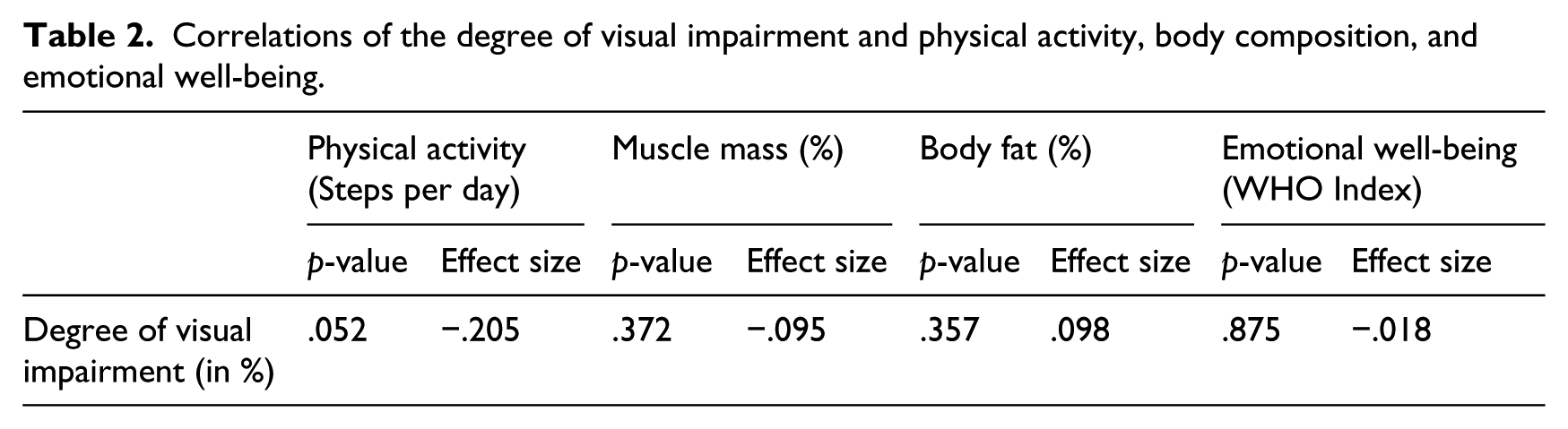
The results of further analyses confirm no significant correlation between the percentage degree of VI and the average number of steps (per day) (r = −.205; p = .052), body composition (muscle mass: r = −.095, p = .372; body fat: r = .098, p = .357), and emotional well-being (r = −.018; p = .875). The results are displayed in Table 2.
Correlations of the degree of visual impairment and physical activity, body composition, and emotional well-being.
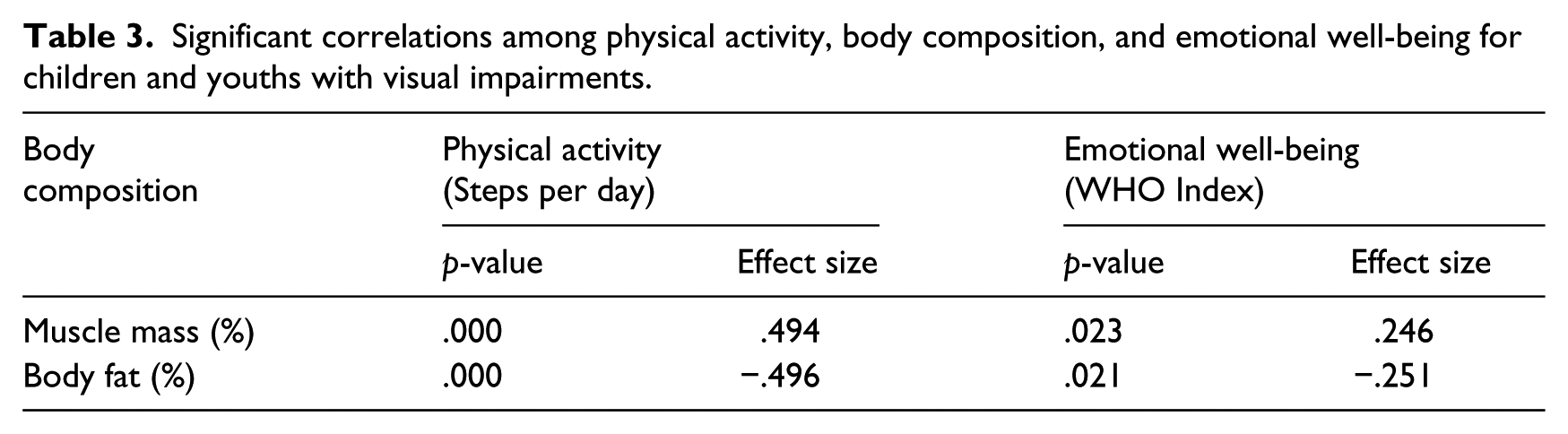
In addition, the results show a positive connection between the average number of steps (per day) and body composition values of children and youths with VI. For children with VI, there were significant correlations between the percentages of body fat (r = −.496; p = .000) and muscle mass (r = .494; p = .000) with the average number of steps (per day). The more physically active, the better body composition values of children with VI (and vice versa). Also, a significant association between body composition and well-being was found (r = .246, p = .023; r = −.251, p = .021). Children and youths who are visually impaired or blind with good body composition values were likely to have high WHO scores (and vice versa). The results are displayed in Table 3.
Significant correlations among physical activity, body composition, and emotional well-being for children and youths with visual impairments.
Discussion
As mentioned earlier, research in Germany related to exercise and sports with individuals who are visually impaired or blind is scarce. To our knowledge, this is the first investigation which documents physical activity, body composition, and emotional well-being in children and youths with VI in Germany.
The goal of the pilot study was to show initial trends. In all relevant parameters, students with VI achieved results comparable to those of sighted students. The results showed no insufficiencies in the profiles of physical activity of students who are visually impaired and blind. Additionally, children with VI did not have lower body composition values than sighted children. Moreover, the results have no connection with the percentage degree of VI. The study results reveal that VI do not necessarily lead to insufficiencies in physical activity, body composition, or emotional well-being. The results therefore contrast the results of the studies previously mentioned.
It has to be noted that the children and youths with VI were provided with a curriculum that has the same expectations as their sighted peers. Moreover, the specialized school provides not only a curriculum with high expectations but also opportunities and incentives to engage in physical activity through physical education and extracurricular sports. This leads to the assumption that children and youths with VI can perform equally in physical activity measures when provided with the same curriculum as sighted peers and equal opportunities for participation. The study’s results would go along with previous studies that have reported improvements in the physical health condition of children with VI and physical activity levels comparable to those of sighted children when equal opportunities for participation in regular physical activity are given (Cervantes & Porretta, 2013; Stuart et al., 2006; Williams et al., 1996).
Moreover, it is important to mention that the special school facility offers intensive student support which focuses on the needs of students with VI. The school includes teachers with special educational expertise, specific didactic concepts, small class sizes, and additional qualified teachers in classes if needed. This information is relevant with regard to Shields et al. (2012) and the previously mentioned barriers to physical activity for children with disabilities. It can be noted that environmental and policy or program barriers such as inadequate facilities and the lack of appropriate physical activity programs, staff capacity, and opportunities (relating to the amount, variety, and quality of opportunities) are not likely to exist in the special school facility. This goes along with Haegele and Porretta (2015a) who stated that low physical activity levels of school children with VI may be connected with perceived participation barriers such as the availability of appropriate opportunities.
Limitations
It must be considered that study methods bring only limited insight into the discussion. The amount of activity, for example, is only one view of activity. Intensity of activity is equally important and could not be captured by the study methodology. The pedometers used also could not capture certain type of motion or sports activities such as swimming, weightlifting, horseback riding, and rowing. For this reason, further studies are needed to obtain comprehensive insights.
Also, the pedometers used in this study are not valid for children with VI. The pedometers display the user’s accumulated step count on a small screen and could not provide feedback for the participants with VI. Talking pedometers, which also have been validated for step-count accuracy, could provide auditory feedback here and motivate individuals with VI to increase daily physical activity (Beets, Foley, Tindall, & Lieberman, 2007; Haegele & Porretta, 2015b; Lieberman, Stuart, Hand, & Robinson, 2006). Moreover, the WHO-5 has not been validated for children and youths who are visually impaired. Previous authors have pointed out that it is difficult to assess health-related quality of life of individuals with VI (de Boer et al., 2004; Margolis et al., 2002; Stelmack, 2001). For example, the manifestation, stability, and progression of VI and the occurrence of additional impairments can influence an individual’s quality of life, and they are often not considered in questionnaires (Holbrook et al., 2009; Margolis et al., 2002). These issues have not been addressed in this study as well.
More limitations need to be taken into account. In the context of this study, we must consider that all children and youths who participated in the study came from a school for the blind and visually impaired. As stated previously, not all children and youths with VI in Germany are educated in this type of school. The results are therefore not representative for all children and youths with VI in Germany and raise the question as to how they would look in an inclusive setting. Further studies would be needed to shed light on this subject and its components as related to the type of schooling, including a comparison of mainstream schooling versus specialized schooling. This topic must also be reviewed in the light of study results from other countries where students with VI are for the most part schooled inclusively.
It must also be noted that the specialized school for children and youths with VI sets priorities for sports. The students may experience physical activity in school through physical education and extracurricular sports. They are given opportunities and incentives to engage in physical activity and to lead active lifestyles which provide the amounts and kinds of physical stimulation needed. This may have an impact on the study results. It is likely that they are related to the type of schooling. That would support the conclusions of Skaggs and Hopper (1996) who maintained that the types of schools may differ in the efficiency of their sports education.
Conclusion
The findings demonstrate the importance of physical activity in influencing body composition and emotional well-being of children and youths with VI. The results confirm the positive effects and the importance of physical activity for students who are visually impaired and blind. The findings of our study could be connected to the results of Labudzki and Tasiemski (2013) and Haegele et al. (2016) who reported a significant connection between physical activity and perceived quality of life in adults with VI.
Moreover, the results reveal no association between VI and physical activity. High physical activity levels of school children with VI may be connected with the availability of opportunities for participation in regular physical activity, a curriculum with high expectations and intensive student support which focuses on the student’s needs, rather than the severity of VI. The results reveal that higher levels of physical activity are possible which provide health-related benefits for children and youths. They make a considerable contribution to the understanding and validation of school physical activity programs for children and youths with VI. It is important to promote the implementation of effective physical activity programs in all educational settings, both in specialized schools and in mainstream schools. Students with VI can achieve comparable activity levels if given the opportunity. Considering that active lifestyles for children and youths form the foundation for present and future physical activity, the results are promising.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.