
Abstract
The aim of the review was to evaluate current evidence-based knowledge about physical activity, physical fitness, and body composition among children and young adults with visual impairments. A systematic literature review of articles published between January 1984 and April 2014 inclusive was conducted. The participants were in the age range of 5–22 years. A total of 29 publications met the inclusion criteria. In general, the findings revealed lower levels of participation in physical activity, poorer physical fitness, and higher prevalence of overweight and obesity among children with visual impairments compared to children with no reported visual impairments. Lack of longitudinal observational studies and randomized clinical trials reduced the possibilities to draw cause–effect conclusions. However, the 23 cross-sectional studies confirmed that young adults with visual impairment may need more physical activity to become fitter and have a healthier body composition. Furthermore, low physical activity may influence higher prevalence of overweight and obesity among children and young adults with vision loss.
Introduction
Some authors have reported that children and young adults with visual impairments (VIs) tend to be less physically active, be less physically fit, and have a greater tendency to be overweight or obese than their sighted counterparts (Aslan, Calik, & Kitiş, 2012; Kozub & Oh, 2004; Lieberman, Byrne, Mattern, Watt, & Fernandez-Vivio, 2010; Longmuir & Bar-Or, 2000; Montero, 2005).
Lower physical activity and fitness and higher adiposity are important factors for health and well-being. Physical activity plays an important role in the promotion of children’s physical and psychological health, especially for those with disabilities (Aslan et al., 2012; Gronmo & Augestad, 2000; Lieberman, Stuart, Hand, & Robinson, 2006; Sit, McManus, McKenzie, & Lian, 2007). In addition, participation in physical activity is beneficial for healthy ageing and may also improve social involvement and quality of life in general (Chodzko-Zajko, 2014; Lieberman et al., 2010; Lieberman & McHugh, 2001).
Physical fitness is important for youths’ health and daily-life activities as well as for practising sports (Houwen, Hartman, & Visscher, 2010). Results from Lieberman and McHugh (2001) showed that up to 80% of children with VI do not reach criterion levels of health-related physical fitness. This may also increase their risk of being overweight. To reach the recommended fitness levels may be crucial for disease prevention and health promotion.
Being overweight or obese is a risk factor for good health. For example, they are important, independent components of the metabolic syndrome in young adults. Ferreira, Twisk, van Mechden, Kemper, and Stehower (2005) concluded that intervening in the period of transition from adolescence to adulthood may be a fruitful area for prevention of the metabolic syndrome. Adiposity later in life is associated with premature death and with chronic disease such as end-stage renal disease, coronary heart disease, some cancer types, and muscle skeletal disorders (Mazzocchi & Traill, 2011).
However, those with VIs may find it difficult to participate together with sighted people due to sensory impairments, psycho-social barriers, and depending on type of activities. Some countries have closed all schools for the blind and are integrating those with impairment into local schools. Physical activity programmes suited well for young people with VI may not exist in the geographical area they are living. Young people with VI may also perceive barriers related to participation in physical activity. Good appropriate opportunities are import and may be more important than vision, age, gender, and school systems.
After searching the literature, we found one systematic review published regarding motor skill performance (Houwen, Visscher, Lemmink, & Hartman, 2009) and one related to psychomotor behaviour (Skaggs & Hopper, 1996). However, we were not able to find a review regarding physical activity and fitness level among children and young adults with VIs.
Therefore, we found it of interest to conduct a systematic review. The aim of this study was to summarize the current evidence-based scientific knowledge about physical activity, physical fitness, and body composition among children and young adults with VIs. We carried out a systematic review of pre-reviewed published studies and described study characteristics and major findings.
Methods
Search strategy
We searched the PubMed and SPORTDiscus databases to identify relevant published articles. Reference lists and Google Scholar were also scrutinized for relevant studies. The searches were conducted in April 2014. The search terms used in the two databases as Medical Subject Headings terms or free text words were as follows: ‘school aged children’, ‘adolescents’, and ‘teenagers’ with combinations of ‘visual impairment’, ‘vision disorders’, ‘visually impaired’, ‘blind’, ‘blindness’, and ‘low vision’. These terms were then combined separately with ‘physical activity’, ‘inactivity’, ‘physical fitness’, ‘overweight’, ‘obesity’, and ‘body composition’. We also conducted a manual search of the reference lists of all included articles and in Google Scholar.
We used the following definition of physical fitness: Physical fitness is defined as the general fitness level of the human body, including aerobic functioning (cardiovascular), muscular strength, endurance, flexibility, speed, and balance (Aslan et al., 2012; Gronmo & Augestad, 2000). Other motor skill performances like developmental factors, posture and gait pattern are not included in this review.
Criteria for inclusion and exclusion
The search process is shown in Figure 1. The target population for the systematic review was school-age participants with VIs. Articles written in English, with original data collection and pre-reviewed publications published between January 1984 and April 2014 inclusive, were included.
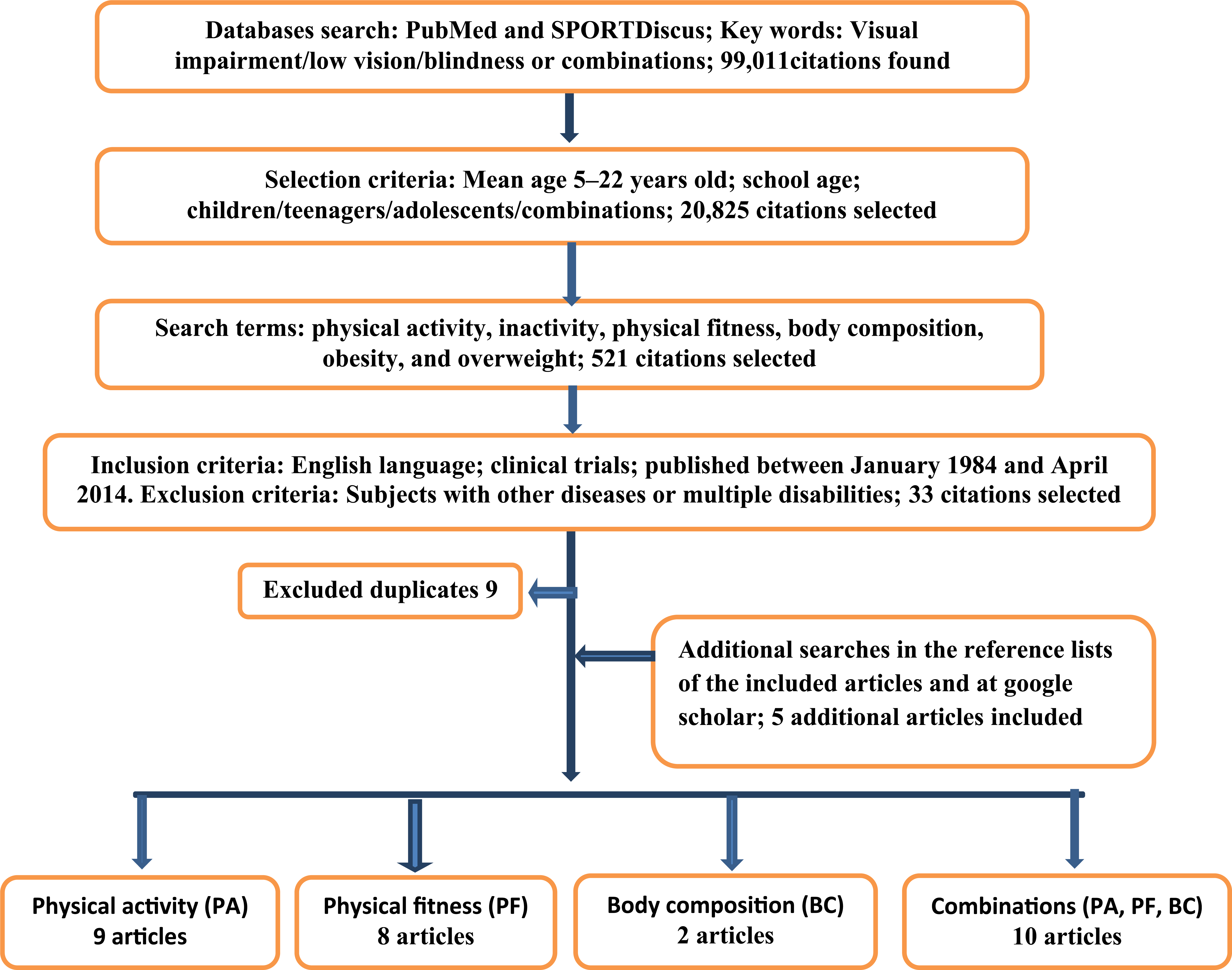
Search strategy for all relevant articles.
We excluded articles related to children with VIs and additional co-morbidity and multiple disabilities. Articles that had the main focus on motor skills, movement therapy, movement education, motivation, or building social skills were not included.
The two authors independently reviewed citations and abstract, assessed full text articles, and extracted the data from each publication. We also used the ancestry method, where we looked up articles by subject headings and by authors’ previous publications that were cited by articles that were more recent. A total of 29 studies were included in the review.
Data extraction
We used a standardized protocol and reporting form to abstract the following data from each publication: the first author’s name, the year of publication, the country in which the study was conducted, the age and number of persons of the study population, number visually impaired and sighted in each study, test measurement of physical activity and physical fitness, definition of VI, school type, and each publication’s main results.
Evaluation of the studies
We used the Quality Assessment Tool for Studies with Divers Design (QATSDD) to evaluate the studies in the review (Sirriyeh, Lawton, Gardner, & Armitage, 2011). The tool was developed according to Moher, Liberati, Tetzlaff, Altman, and PRISMA Group (2009) to indicate preferred reporting items for systematic reviews. We used the 14 QATSDD items related to quantitative studies. Each item was rated on a 4-point scale from not at all (0), very slightly (1), moderate (2), and complete (3), with a maximum score of 42. The percentage score was calculated by dividing the actual score by the maximum score 42. Papers scoring over 75% were considered ‘high’ quality, those between 50% and 75% ‘good’, and below 25% ‘poor’. The quality ratings are presented in Tables 1 to 3.
Characteristics of the studies of physical activity (PA) among children with vision impairments.

QATSDD: Quality Assessment Tool for Studies with Divers Design; USABA: United States Association for Blind Athletes; LBIA: leg-to-leg bioelectrical impedance analysis; WHO: World Health Organization; SOFIT: system for observing fitness instruction time; BPFT: Brockport Physical Fitness Test; FTMS-A: free-time motivation scale for adolescents; HSPPA: Harter’s self-perception profile for adolescents; VI: visual impairment; PA: physical activity.
Interventional studies (all other studies were observational studies with a cross-sectional design.
ActiGraph device.
Triaxial Accelerometers.
European Test of Physical Fitness.
Characteristics of the studies of physical fitness (PF) among children with vision impairment.

QATSDD: Quality Assessment Tool for Studies with Divers Design; BPFT: Brockport Physical Fitness Test; USABA: United States Association for Blind Athletes; LBIA: leg-to-leg bioelectrical impedance analysis; WHO: World Health Organization; FHRF: Fitnessgram Health-related Fitness Test; VO2: oxygen uptake; IBSC: International Blind Sports Classification; VO2max: maximal oxygen uptake; CMI: Cornell Medical Index; VI: visual impairment; PF: physical fitness; PA: physical activity.
Interventional studies (all other studies were observational studies with a cross-sectional design.
European Test of Physical Fitness.
The Project UNIQUE physical fitness test.
Characteristics of the studies of nutrition related to obesity or overweight among children with vision impairment.
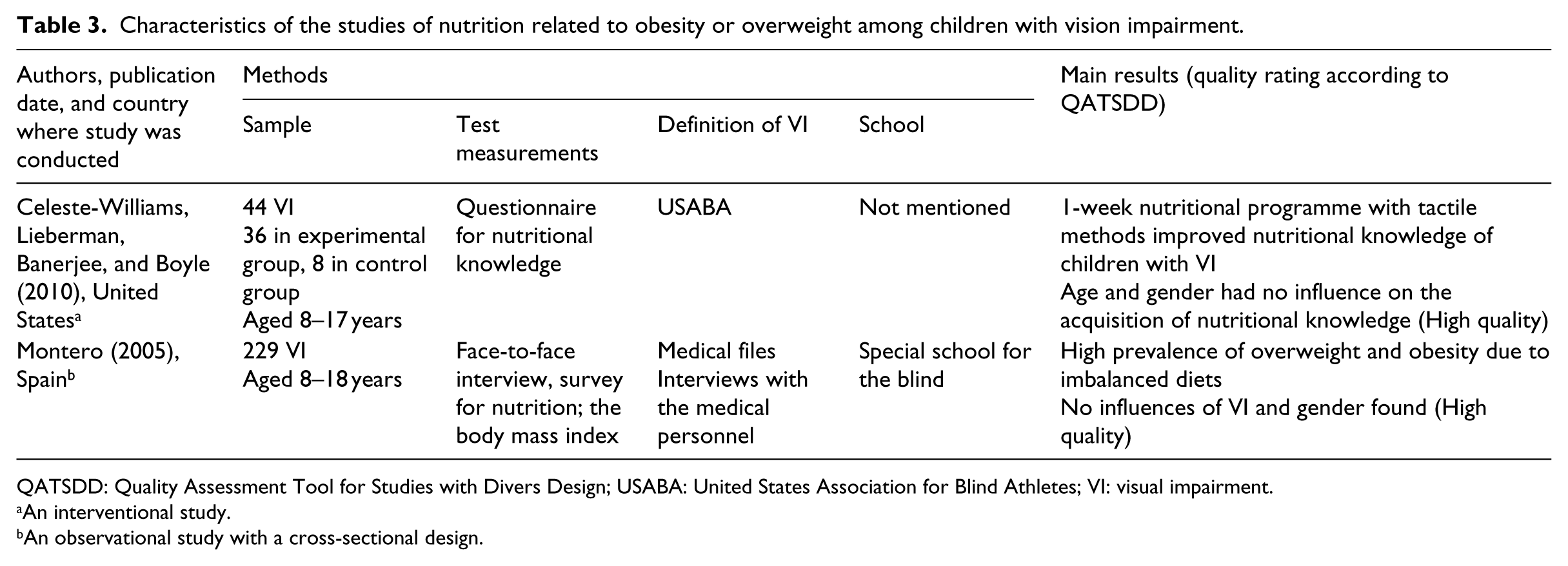
QATSDD: Quality Assessment Tool for Studies with Divers Design; USABA: United States Association for Blind Athletes; VI: visual impairment.
An interventional study.
An observational study with a cross-sectional design.
Results
Study characteristics
Six articles report interventional studies (Celeste-Williams et al., 2010; Cervantes & Porretta, 2013; Chen & Lin, 2011; Lieberman et al., 2006; Morelli et al., 2011; Shindo et al., 1987), and the remaining 23 articles report observational studies with a cross-sectional design. The studies represented 14 countries, and 10 out of 29 studies were conducted in the United States. The sample size was small in most studies, and only five studies had more than 100 participants (Colak et al., 2004; Lieberman et al., 2010; Montero, 2005; Short & Winnick, 1986; Suzuki et al., 1991). The authors used different age ranges, different measurements for physical activity, physical fitness, and body composition, different definitions of VI, and different school types.
Participation in physical activity
Five of the articles listed in Table 1 report that children and young adults with VIs participated less in physical activity than their sighted peers (Gronmo & Augestad, 2000; Hopkins et al., 1987; Houwen et al., 2009a; Kozub & Oh, 2004; Kroksmark & Nordell, 2001). Two studies report that children with VIs seldom participated in moderate to vigorous physical activity (Aslan et al., 2012; Houwen et al., 2009a).
Four studies assessed the effect of level of vision on physical activity among children with VIs (Aslan et al., 2012; Hopkins et al., 1987; Houwen et al., 2009a; Kozub & Oh, 2004). Aslan et al. (2012) and Hopkins et al. (1987) found that the level of participation in physical activity differed between children with low vision and blindness, while Houwen et al. (2009b) found that decreased levels of physical activity were associated with increased levels of VI among children with low vision. Kozub and Oh (2004) did not find any relationship between vision and participation in physical activity.
The studies revealed inconsistent results regarding the influence of age on participation in physical activity. Ayvazoglu et al. (2006) and Kozub and Oh (2004) found that older children with VIs were more inactive than younger children with VIs. However, Longmuir and Bar-Or (2000) did not find any age-specific differences among children with VIs related to participation in physical activity.
There were also inconsistent results concerning the influence of gender on participation in physical activity among children with VIs. Aslan et al. (2012) found different physical activity levels between boys and girls with VIs, whereas Longmuir and Bar-Or (2000) did not find any gender differences in participation in physical activity by children with VIs.
Lack of motivation and limited ability to participate in physical activity were two important reasons for children with VIs becoming inactive (Ayvazoglu et al., 2006; Kozub, 2006; Longmuir & Bar-Or, 2000). School type did not seem to affect physical activity level, while the context of physical education and teachers’ behaviour seemed to be more important for whether children with VIs participated in physical activity (Kozub, 2006; Sit et al., 2007). Furthermore, Ayvazoglu et al. (2006) found that families’ and siblings’ involvement in moderate to vigorous physical activity was an important determinant for participation in physical activity by children with VIs. Furthermore, children with VIs were able to engage in suitable sports when they were motivated and given proper opportunities to participate in activities (Cervantes & Porretta, 2013; Lieberman et al., 2006; Morelli et al., 2011).
Physical fitness
Table 2 shows that those with VIs were found to have lower levels of physical fitness than their sighted peers (Hopkins et al., 1987; Houwen et al., 2010; Kobberling et al., 1989; Meek & Maguire, 1996; Short & Winnick, 1986; Wyatt & Ng, 1997). However, Williams and Armstrong (1996) did not find any statistical significant differences between aerobic fitness among 10 girls with VI and 10 sighted girls. Colak et al. (2004) concluded that goalball may be considered as an effective option to improve fitness among children with VI.
Different results were found regarding the relationship between the degree of vision loss and physical fitness among children with VIs. Seven studies found that children who were blind were most unfit compared to children with some vision or normal vision (Hopkins et al., 1987; Kobberling et al., 1989; Lieberman & McHugh, 2001; Meek & Maguire, 1996; Shindo et al., 1987; Short & Winnick, 1986; Wyatt & Ng, 1997), while two other studies showed that the degree of vision loss did not affect physical fitness (Houwen et al., 2010; Lieberman et al., 2010).
There were also inconsistent results regarding the influence of gender on physical fitness for children with VIs. Lieberman and McHugh (2001) report more differences in arm and abdominal strength between boys with and without VIs compared to girls with and without VIs. By contrast, a study by Lieberman et al. (2010) showed no association between gender and physical fitness among children with VIs.
Two studies had results related to fitness level and educational settings. Short and Winnick (1988) claimed that children in inclusive schools had better physical fitness, while Gronmo and Augestad (2000) did not find differences in physical fitness between children with VI in inclusive schools in Norway and children in special schools for the blind in France.
Three studies found that unhealthy body composition was associated with lower level of physical education among children with VIs (Hopkins et al., 1987; Karakaya et al., 2009; Wyatt & Ng, 1997). A further two studies suggested that exercise training could improve fitness levels among children with VIs (Chen & Lin, 2011; Shindo et al., 1987).
Overweight and obesity
Children with VIs were shown to have a more unhealthy body composition and higher rates of overweight and obesity than sighted (Gronmo & Augestad, 2000; Hopkins et al., 1987; Houwen et al., 2009a, 2010; Kozub, 2006; Suzuki et al., 1991; Wyatt & Ng, 1997). The researchers claimed that the main reasons were inactivity and imbalanced diet (Montero, 2005). Also, poor physical fitness was associated with higher rates of overweight and obesity among children with VIs than sighted peers (Lieberman et al., 2010; Wyatt & Ng, 1997).
Hopkins et al. (1987) found that greater skinfold thickness was associated with increased degrees of VI. However, Lieberman et al. (2010) and Montero (2005) found no significant difference in body mass index (BMI) among children with different severity of VI. From a study conducted in Japan, Suzuki et al. (1991) found low excesses of body fat among blind girls in the age group 4–14 years compared to high excesses among blind girls in the age group 13–22 years, whereas there were no differences between blind boys in the age groups 4–12 years and 13–22 years. By contrast, Montero (2005) found no gender differences in the prevalence of overweight and obesity among Spanish children with VIs. Only one study reported the effect of school type on body composition, and no differences were found between inclusive schools and special schools for the blind (Gronmo & Augestad, 2000).
Montero (2005) found a high prevalence of overweight and obesity due to imbalanced diet among 229 children with VI. However, a 1-week nutritional programme with tactile methods was found to improve the nutritional knowledge acquired by children with VIs (Celeste-Williams et al., 2010). The results from the two studies did not show any effect by gender or the degree of VI according to imbalance in diet or nutritional knowledge (Table 3).
Discussion
In general, the findings revealed lower levels of participation in physical activity, poorer physical fitness, and higher prevalence of overweight and obesity among children with VIs compared to children with no reported VIs. Lack of longitudinal observational studies and randomized clinical trials (RCTs) reduced the possibilities to draw cause–effect conclusions. However, the cross-sectional studies confirmed that children with VI may need more physical activity to increase their fitness levels and to have a healthier body composition. Our results are in accordance with Furtado, Allums-Featherston, Lieberman, & Gutierrez (2015) and Haegele & Porretta (2015).
Physical activity may have a positive influence on the physical and mental health of children with VIs and may improve their quality of life (Lieberman et al., 2001). It is suggested that children with VIs are less fit mainly because of inactivity (Hopkins et al., 1987; Longmuir & Bar-Or, 2000; Wyatt & Ng, 1997). It is also suggested that both inactivity (Hopkins et al., 1987) and high calorie intake (Montero, 2005) might lead to overweight and obesity among children with VIs.
Some studies’ results showed that children with VIs might perform as well as their sighted peers in physical activity (Cervantes & Porretta, 2013; Lieberman et al., 2006; Morelli et al., 2011). In order to reduce the weight and improve the physical fitness of children with VIs, the results showed the importance of motivation and providing adequate opportunity to participate in proper programmes for physical activity (Celeste-Williams et al., 2010; Colak et al., 2004; Shindo et al., 1987; Williams & Armstrong, 1996). Satisfactory eating habits and nutritional knowledge may also be important to achieve good health for children with VIs (Celeste-Williams et al., 2010).
Furthermore, it is suggested that physical education teachers, parents, and significant others lack enough knowledge regarding how best to educate children with VIs in physical activity (Lieberman, Ponchillia, & Ponchillia, 2013). This could, in part, explain the possibly limited programmes, inadequate teaching, and increased sedentary behaviour of children with VIs. Appropriate physical education programmes may increase the involvement of children with VIs in physical activity (Lieberman et al., 2013). However, families and significant others may play an important role in encouraging children with VI to participate in physical activity and sports (Ayvazoglu et al., 2006).
Due to differences in culture, school organization, and healthcare systems, the context of physical education differs between countries, and such differences were found to affect participation in physical activity by children with VIs (Gronmo & Augestad, 2000; Sit et al., 2007). Lack of friendships in later childhood may result in less motivation to participate in physical activity and reduced social involvement for children with VIs (Ayvazoglu et al., 2006).
The scientific evidence is limited and there are inconsistent results on the influences of the degree of VI, gender, age, and school types (Lieberman & McHugh, 2001; Meek & Maguire, 1996; Short & Winnick, 1986; Wyatt & Ng, 1997).
Limitations
Relatively few studies of physical activity, physical fitness, and body composition among children and young adults with VIs were published between January 1984 and April 2014 inclusive. The aims, study design, participants, and measures of outcomes differed to some extent between the reviewed studies. The studies differed in the reported degree of vision loss, definition of VI, age of the participants, time and geographic disparities, and measurements of physical activity and physical fitness, and thus complicated the comparison. The diagnosis, cause, progression of the disease or vision loss, and onset-time of VI varied greatly between the studies. Most articles do not mention the causes and onset-time of blindness, although different eye conditions might correspond to different levels of physical activity, physical fitness, and body composition. In addition, most studies had small sample sizes and a cross-sectional study design. Therefore, the data were not synthesized in a meta-analysis because of the small number and heterogeneity of the included studies. In addition, we suggest that selection bias occur in at least some studies (Ayvazoglu et al., 2006; Karakaya et al., 2009; Kozub, 2004; Kozub & Oh, 2006; Kroksmark & Nordell, 2001; Morelli et al., 2011). The selection bias may special refer to the studies with that no proper randomization and therefore the samples may not be representative of the population to be analysed. Some conclusions of studies may not be accurate because selection bias has not been taken into account.
Conclusion
Lack of longitudinal observational studies and RCTs reduced the possibilities to draw cause–effect conclusions. However, the 23 cross-sectional studies confirmed that young adults with VI may need more physical activity to become fitter and have a healthier body composition. Furthermore, low physical activity may influence higher prevalence of overweight and obesity among children and young adults with vision loss.
Participation in physical activity and adequate nutrition knowledge may be important for children with VIs to improve their physical health and quality of life. More longitudinal intervention studies are required.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.