
Abstract
This study aimed to explore the sensory processing profiles of children with the spectrum of optic nerve hypoplasia (ONH). Caregivers completed the Short Sensory Profile (SSP), the Social Communication Questionnaire (SCQ), and the Vineland Adaptive Behaviour Scale (VABS) interview. The study demonstrated that children with ONH present with sensory integration dysfunction (SID), in their intact senses, and that autistic spectrum condition (ASC) was the best predictor of SID, rather than visual loss, or level of intellectual disability in these children. The results indicate that assessment and monitoring of SID in children with ONH is crucial.
Introduction
Children with the spectrum of optic nerve hypoplasia (ONH) present with variable anatomical abnormalities and behavioural phenotype, ranging from mild visual loss to total visual loss (Lambert, Hoyt, & Narahara, 1987), intellectual disability (Garcia-Filion et al., 2008), and autistic spectrum condition (ASCs) (Jutley-Neilson, Harris, & Kirk, 2013). To date, research reporting sensory integration dysfunction (SID) (also referred to as sensory processing disorders [SPDs]) in the intact senses of children with ONH has been sparse and limited in detail (Bahar, Brody, McCann, Mendiola, & Slott, 2003). This study aimed to assess the types and incidences of SID in children with ONH, and the study also sought to identify whether visual loss, intellectual disability, or ASCs best predicted SID in this cohort of children.
The reported prevalence of ONH is 13.8 per 100,000 live births (Atapattu et al., 2012), and the aetiology of ONH is considered multifactorial with prenatal risk factors, heritability, and genetic mutations being described in research studies (Garcia-Filion & Borchert, 2013). ONH encompasses a wide clinical spectrum (Ahmad, Borchert, & Geffner, 2008), with a phenotype which is variable in its severity and symptom presentation (Signorini et al., 2012). The cardinal feature of ONH is the underdevelopment of the optic nerve, which can lead to visual function ranging from good visual acuity to no light perception (Brodsky, 2016). More commonly, ONH affects both eyes, and additional visual problems include nystagmus (more common bilaterally), and strabismus (Garcia-Filion et al., 2008; Ryabets-Lienhard, Stewart, Borchert, & Geffner, 2016). Often, associated dysgenesis of midline forebrain structures (absence or hypoplasia, of septum pellucidum and/or corpus callosum), hypothalamic–pituitary dysfunction (hypopituitarism, ranging from isolated to multiple hormone deficiencies), and developmental delay are commonly reported in children with ONH (Borchert, 2012). Reported delays include intellectual disability (Garcia-Filion et al., 2008; Margalith, Jan, McCormick, Tze, & Lapointe, 1984; Mohney, Young, & Diehl, 2013; Signorini et al., 2012), motor impairments (Tornqvist, Ericsson, & Källén, 2002; Trabacca, De Rinaldis, Gennaro, & Losito, 2012), and ASCs (Dale & Sonsken, 2002; Ek, Fernell, & Jacobson, 2005; Jutley-Neilson et al., 2013). Such behavioural problems have been reported to be more frequent in children with bilateral ONH (Teär Fahnehjelm, Dahl, Martin, & Ek, 2014).
Professionals such as occupational therapists and specialist teachers of children with visual impairments have reported that children with ONH are at an increased risk of SID in their intact senses, and SID reported in children with ONH have included extreme tactile and auditory defensiveness (Bahar et al., 2003). In support of this report in educational settings, clinical observations of SID have included hypersensitivities to certain sounds, textures, and tastes in children with ONH (Fink & Borchert, 2011).
SID encompasses impairments in responding to sensory stimuli which include the detection, modulation, and/or interpretation of external sensory stimuli (Miller, Coll, & Schoen, 2007). Children who experience these impairments show a hypersensitivity or hyposensitivity to visual information, sound, touch, taste, smell, vestibular, proprioceptive, and kinaesthetic inputs. These abnormal responses affect children’s social skills, play behaviours, motor development, emotional development, and their daily living skills (Ayres, 1972).
SID is not uncommon, and around 5% of typically developing children experience SID (Ahn, Miller, Milberger, & McIntosh, 2004), with this percentage increasing to 32%–84% for children who have a range of disabilities (Cheung & Siu, 2009; Little, Dean, Tomchek, & Dunn, 2016; Tomchek & Dunn, 2007). For example, SID has been reported in children with global developmental delays/intellectual disability (Baranek, David, Poe, Stone, & Watson, 2006; Leekam, Libby, Wing, & Gould, 2007), ASC (Baker, Lane, Angley, & Young, 2008; Little, Dunn, Tomchek, & Wilson, 2015; Wing & Gould, 1979), corpus callosum impairments (Demopoulos et al., 2015), genetic disorders which have associated intellectual disability, such as Fragile X (Rogers, Hepburn, & Wehner, 2003), Prader–Willi Syndrome (Cataletto, Angulo, Hertz, & Whitman, 2011), CHARGE syndrome (Brown, 2005), and Smith–Magenis syndrome (Hildenbrand & Smith, 2012).
The research described above has shown that SID is commonly associated with a range of clinical conditions, which share a similar symptomatology to that of ONH (e.g., intellectual disability and ASCs). Alongside these studies, research has also shown that visual loss is another vulnerability factor for SID. One of the first reports of SID in children with visual loss was reported by Wing (1969), who noted that children with autism also presented similar SID to that of blind children. In addition to these early reports, SID have been reported in case studies of blind adults with visual impairments, with tactile defensiveness and vestibular sensory impairments described (Baker-Nobles & Bink, 1979).
More recently, research has reported SID in children with heterogeneous aetiologies for their visual impairment and/or intellectual disability. Gal, Dyck, and Passmore (2010) reported that children who had a visual impairment and an intelligence quotient (IQ) lower than 70 reported higher levels of sensory processing difficulties than typically developing children and children with hearing loss, but slightly lower levels of SID than children with autism. This pattern of results was also reported for visually impaired children who had an IQ of 70 or more, which could suggest that intellectual disability did not affect SID in children with visual loss.
Visual impairments are known to impact children’s early motor development (Levtzion-Korach, Tennenbaum, Schnitzer, & Ornoy, 2000), and may influence a child’s ability to integrate information from other sensory modalities, thus resulting in SID (Gal et al., 2010). Children with visual impairments experience reduced opportunities to explore their immediate environment (Lewis, Norgate, Collis, & Reynolds, 2000; Troster & Brambring, 1994). These reduced incidences and opportunities for exploration increase the likelihood of children with visual loss engaging in stereotyped behaviours. In support of this explanation, Gal et al. (2010) reported stereotyped movements as being the best predictor of impairments in tactile sensitivity in children with varying degrees of visual loss and intellectual disability.
Early reports by Keeler (1958) and Wing (1969) noted that children with autism present with similar SID to that of blind children. These behaviours of children with visual impairments are often described as autistic-like, blindisms, or as surface similarities, which are not truly autistic in their origin. Conversely, children with visual impairments often go on to receive a formal diagnosis of ASC; therefore, the conditions are co-morbid (Hobson & Bishop, 2003; Pring, 2005; Rutter et al., 1999). Previous research has reported similar SID profiles in sighted children with ASC, and in children with visual loss. For example, in a group of sighted children with ASC, Chang et al. (2014) reported correlations with impairments in tactile and auditory processing and impaired white matter microstructural integrity. Through different methodologies, Gori, Del Viva, Sandini, and Burr (2008) also reported tactile and auditory processing impairments in a group of children with visual loss and these impairments were attributed to early visual loss disrupting intermodal calibration during the period of early perceptual development. Alternatively, adults with congenital visual loss have shown increased sensitivity in their remaining senses due to sensory compensation (e.g., touch, sound, and taste), with neural reorganisations contributing to this sensory compensation in blind individuals (Cohen, 1997; Röder et al., 1999). As such, it is unclear whether the origin of SID in children with visual loss arises due to impaired intermodal calibration or increased sensory sensitivity. In addition, for individuals with ONH or other visual pathway disorders who have functional vision, visual information which does reach the visual cortex may not integrate with other sensory modalities in a typical manner, which may also lead to impaired intermodal calibration of sensory information.
Irrespective of the origin of SID in children with visual loss, children with visual loss and/or autism may not process sensory information effectively, and sensory information may become painful and/or disorientating, thus resulting in extreme or little reaction to sensory information in their intact senses (Gense & Gense, 2005).
Taken together, it has been identified that research assessing SID in children with ONH is sparse, and also that these children are at a heightened risk for SID due to their syndrome characteristics. For these reasons, this study first assessed whether children with ONH were more likely to have SID than typically developing children. To address this, the study used the Short Sensory Profile (SSP; Dunn, 1999) which is a standardised and commonly used measure of SID. The SSP has been validated on a large population of children, which resulted in clinical diagnostic/cut-off scores for typical sensory processing performance, probable differences in sensory processing, and definite differences in sensory processing. Thus, the SSP aids in the categorisation of SID for children with ONH without the requirement of a control group.
Second, as research has reported that the vulnerability factors associated with SID include ASC, intellectual disability, and visual impairment, this study also assessed, therefore, whether or not SID in children with ONH are due to the co-morbidity of ASC, rather than due to intellectual disability or visual impairment.
Methods
Participants
Children with diagnoses of ONH were identified for recruitment by a computer database of patients, held at the Birmingham Children’s Hospital’s Endocrinology Department (UK). Invitation packs were also sent out by the national charities Focus Families, and The National Blind Children’s Society.
The total number of participants, identified for potential recruitment through the stream of Birmingham Children’s Hospital’s Endocrinology Department, was 53 with ONH. In all, 27 children were recruited in total, equal to a 51% response rate. Children with ONH were also invited to participate through the Focus Family charity conference in Oxford (UK). Invitation packs were sent out by the national charity, ‘Look’ (now merged with the National Blind Children’s Society), who identified 53 children with ONH on their national database. The National Blind Children’s Society also identified 39 children with ONH on their national database. Information packs were sent out by administration staff at the charities and in total, 14 children were recruited via these charities. Ethical approval was granted by the West Midlands NHS Research Ethics Committees (REC) in order to contact families via the hospital database and external charitable organisations.
In total, 41 children participated in the study, of whom 23 were males and 18 were females, with the mean chronological age reported as 8.5 years (standard deviation (SD) = 2.8 years; age range: 3–16 years). Of these children, 15 children reported a mild-to-moderate visual impairment, 12 children reported a severe-to-profound visual impairment, and 14 children reported near-to-total visual loss. Supplementary Table 1 reports individual participant characteristics according to children’s level of vision, diagnosis, and gender. The supplementary table further reports Vineland Adaptive Behaviour Scale (VABS), Adaptive Behaviour Composite (ABC) Standard score (SS) to provide a value of global adaptive functioning; scoring 70 or below was indicative of an intellectual disability and scoring above 70 was indicative of absence of intellectual disability. The VABS ABC SS was further classified into more detailed ability classifications of global adaptive functioning, ranging from a profound disability to a high functioning ability. Scoring above or below the cut-off point for further investigation of ASC according to the Social Communication Questionnaire (SCQ; Rutter, Bailey, & Lord, 2003) and the classification of SID according to the SSP (Dunn, 1999) are also reported in this table.
SSP classification of SID at sub-domain level for children with ONH.
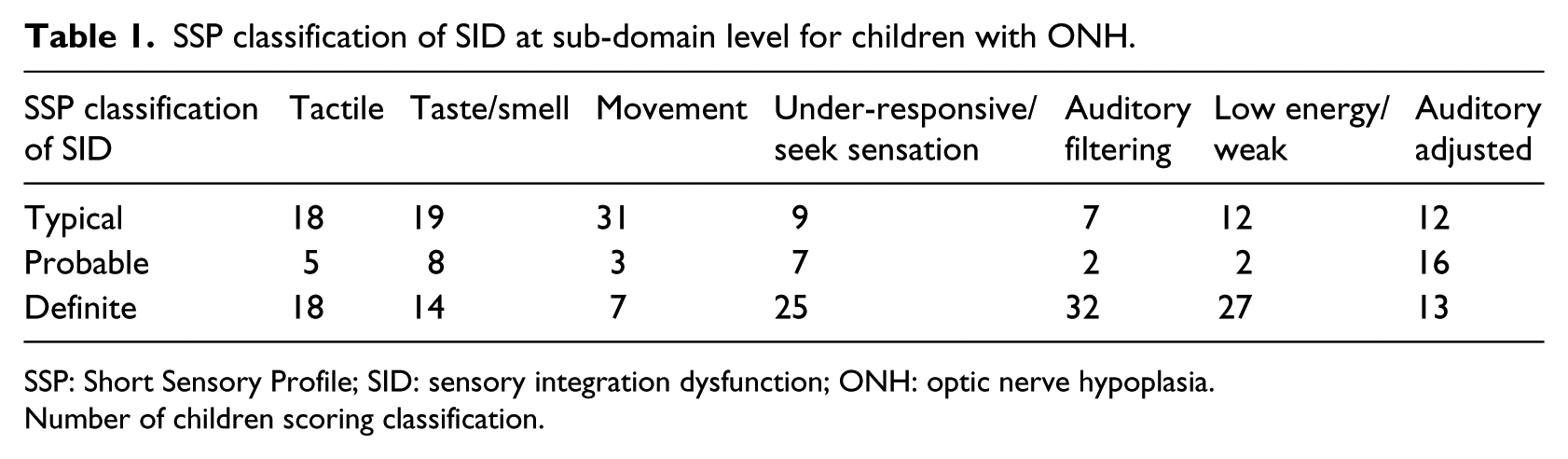
SSP: Short Sensory Profile; SID: sensory integration dysfunction; ONH: optic nerve hypoplasia.
Number of children scoring classification.
Materials and procedure
Parents or guardians of the children completed the questionnaire packs, including the SSP (Dunn, 1999), the SCQ (Rutter et al., 2003), and background demographic information. Following the completion of the questionnaire pack, the VABS (Sparrow, Balla, & Cicchetti, 1984) was completed via a face-to-face interview with parents or guardians.
The definition of visual impairment was adapted from the International Classification of Diseases-10 (ICD-10; World Health Organisation, 2006) standardised definitions. Children were grouped according to their level of visual acuity as; (1) mild to moderate visual loss, (2) severe visual loss (including astigmatism) and, (3) profound visual loss (complete visual loss or light perception).
The SSP (Dunn, 1999) was designed as a screening tool to determine how well children process sensory information in everyday situations. It consists of 38 questions about children’s tactile sensitivity, taste/smell sensitivity, movement sensitivity, under-responsiveness/sensation seeking, auditory filtering, low energy/weak, and visual/auditory sensitivity.
The SSP allows for the classification of sensory scores into three categories: ‘typical performance’, ‘probable difference’, and ‘definite differences’ in sensory processing. Children who score between 190 and 155 are described as ‘typical’, scores between 154 and 142 indicate a ‘probable difference’, and scores below 141 indicate a ‘definite difference’ in children’s processing of sensory information. For this study, three questions, which assessed visual sensitivity, were omitted for all children. The omission of these questions was required due to the levels of visual loss, which are often observed in children with ONH. The adjusted classification of SSPs scores for all children in the study was as follows: scores between 175 and 140 for children who showed ‘typical’ sensory profiles, scores between 139 and 127 indicated a probable difference’, and scores below 126 indicated a ‘definite difference’ in children’s processing of sensory information.
Caregivers were asked to tick the box that best described the frequency with which the subject engages in the listed behaviours, and choices were as follows: never (five points), seldom (four points), occasionally (three points), frequently (two points), and always (one point). On the SSP, lower scores indicate a greater symptoms severity. The SSP includes high- and low-threshold items. High-threshold items measure an individual’s lack of response or need for more intense stimuli, and low-threshold items measure a person’s notice of, or annoyance with, sensory stimuli.
The SCQ (Rutter et al., 2003) was used to evaluate the communication skills and social functioning in children. The SCQ is used to screen for behaviours which characteristic of autism or ASC. It is completed by a parent, or other primary caregiver, in less than 10 min, and consists of 40 yes-or-no questions. If parents were unable to respond to a question due to their child’s visual loss, they responded with ‘not applicable’ and a score of zero was given. The SCQ has good levels of validity, with good sensitivity at .85 and specificity at .75, when the cut-off of ≥15 was used to differentiate between ASC and non-ASC. Although, in our previous study, the SCQ lost some of its sensitivity and specificity in a group of children with profound visual loss which highlighted further the need for a standardised measure for autistic behaviours in children with varying degrees of visual impairment this (for further discussion, see Jutley-Neilson et al., 2013 and see Mukaddes, Kilincaslan, Kucukyazici, Sevketoglu, & Tuncer, 2007 and Kancherla, Braun, & Yeargin-Allsopp, 2013 for further discussion on the absence of diagnostic assessment for ASC in children with visual loss). Therefore, based on the findings of the above study, and the suggested use of the SCQ (Rutter et al., 2003), this study will use the SCQ to compare overall levels of ASC symptomatology across different groups of children and not as for proxy ASC.
The VABS (Sparrow et al., 1984) examines the abilities of individuals from birth to the age of 18 years. The VABS measures the three domains of Adaptive Behaviour: (1) the domain of Communication, with the sub-domains of Receptive, Expressive, and Written Skills; (2) the domain of Daily Living Skills, with the further sub-domains of Personal, Domestic, and Community; (3) the domain of Socialisation, which includes the sub-domains of Interpersonal Relationships, Play and Leisure, and Coping Skills. Standard scores (SS) are available for each behaviour domain, and, once added together, make up the individual’s ABC, which gives a value to global adaptive functioning.
Each item within the set is scored as 0 (never), 1 (sometimes; partially), or 2 (usually), according to criteria detailed in the VABS. If unable to answer an interview question (due to visual loss), caregivers can respond with ‘don’t know’.
Research design
A cross-sectional design was undertaken to establish the prevalence of SID in children with ONH. Participants were recruited between 2005 and 2010, and the participants in this study were also utilised for the Jutley-Neilson et al., study published in 2013.
Experimental manipulations
The percentage and number of participants who reported ‘definite differences’, ‘probable differences’, and ‘typical sensory profiles’ on the SSPs are reported in Table 1. Table 2 shows the SSP classification of SID according to children’s level of visual impairment, whether they were classified as having a VABS ABC score of 70 or below (presence of intellectual disability), or 70 or above (no intellectual disability) and their SCQ classification according to scoring above or below the cut-off point of 15 for further investigation of ASC; this table identifies how the degree of visual impairment, level of intellectual disability and ASC affected SSPs classification.
SSP classification of SID for children with ONH according to level of vision, intellectual disability, and ASC classification.
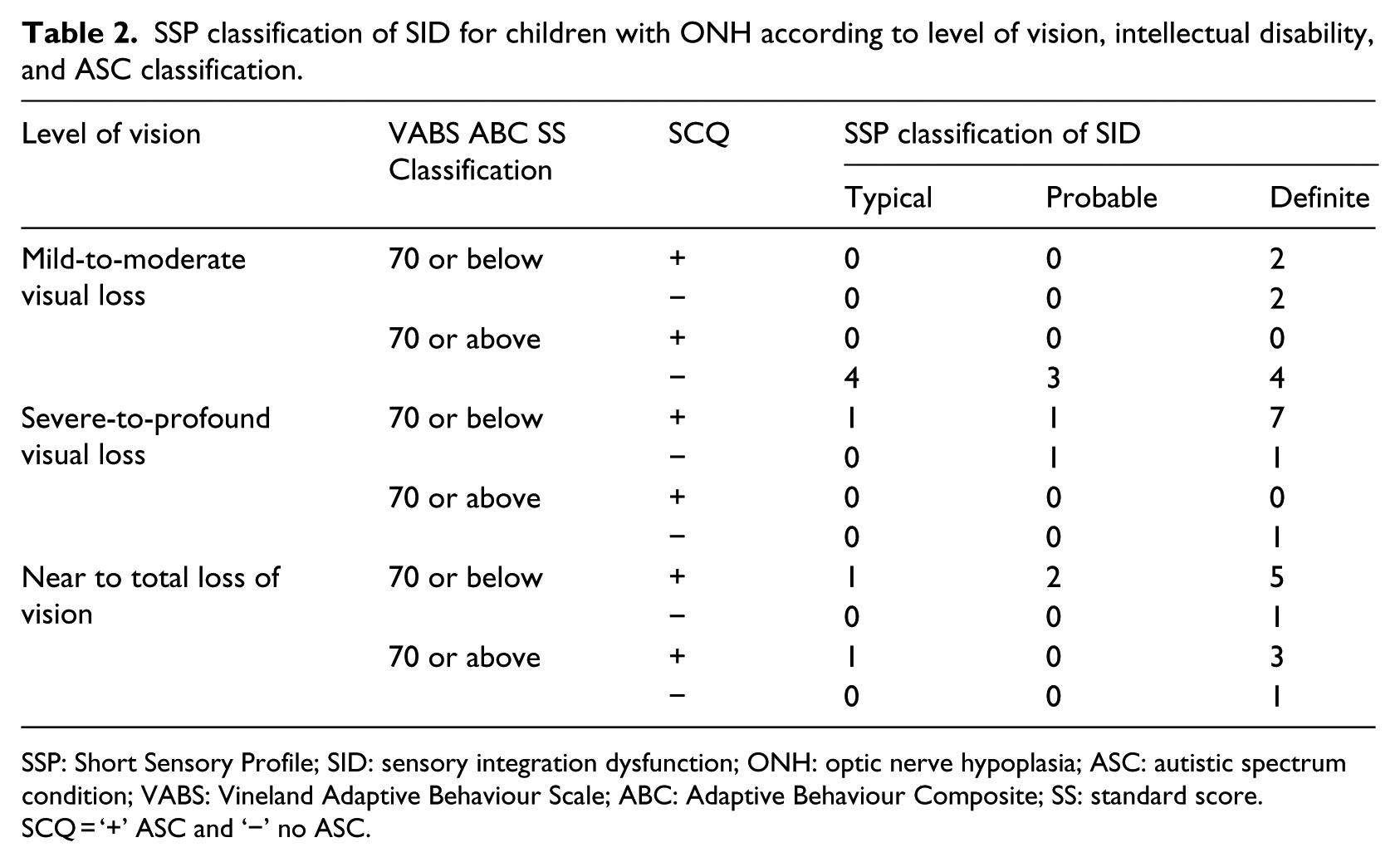
SSP: Short Sensory Profile; SID: sensory integration dysfunction; ONH: optic nerve hypoplasia; ASC: autistic spectrum condition; VABS: Vineland Adaptive Behaviour Scale; ABC: Adaptive Behaviour Composite; SS: standard score.
SCQ = ‘+’ ASC and ‘−’ no ASC.
A multiple regression analysis was conducted to assess which of the variables of visual loss (dummy coding was utilised to ensure data were dichotomous), adaptive behaviours, or autistic phenomenology best predicted SID in children with ONH. In addition, previous research has reported that repetitive behaviours are strongly associated with SID (Gal et el., 2010) and are also a diagnostic feature of ASC. To assess for any associations in the current cohort, a Pearson correlation was used to assess the relationship between the total and sub-domain scores of the SCQ and SSP (Table 3).
Pearson correlation coefficients results between the SCQ and SSP total score and sub-domains for children with ONH.
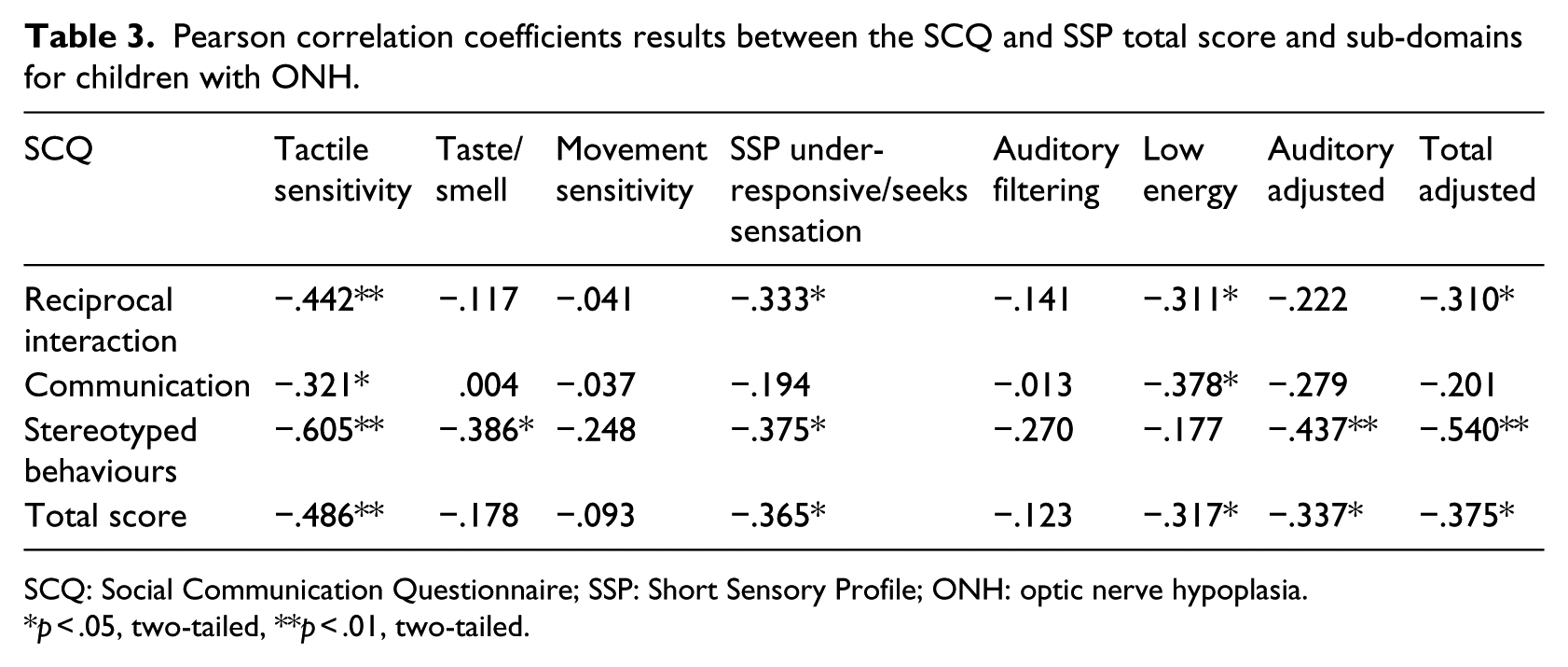
SCQ: Social Communication Questionnaire; SSP: Short Sensory Profile; ONH: optic nerve hypoplasia.
p < .05, two-tailed, **p < .01, two-tailed.
Results
In our cohort, using the total adjusted cut-off score of the SSP, 17.1% (n = 7) of children were rated in the ‘typical performance’ category, 24.4% (n = 10) had scores which fell into the ‘probable differences’ category, and 58.5% (n = 24) reported in the ‘definite differences’ category, indicating possible sensory processing difficulties. Table 1 shows the number of participants’ categorisation for sensory processing differences for the sub-domains of the SSP.
Table 1 shows that children with ONH often demonstrated definite sensory differences, but it is unclear whether visual loss and/or intellectual disability (as measured by VABS ABC SS) best predicted sensory processing difficulties in such children. Initial exploratory data in Table 2 show that children who reported greater levels of visual loss, scored above the cut-off point for possible ASC according to the SCQ and had VABS ABC SS of 70 or below were at greater risk of showing definite differences in the processing of sensory information according the SSP.
However, it was unclear which of these symptomatologies best explained SID in children with ONH. In order to assess the impact of visual loss, intellectual disability, and ASC on SID in children with ONH, a multiple regression analysis was conducted. The results of the multiple regression analysis indicated that the three predictors explained 52% of the variance, and the overall relationship was significant (F (4, 37) = 3.59, p = .014). With other variables held constant, autistic phenomenology (SCQ scores) was negatively related to sensory integration difficulties (SSP scores), decreasing by 1.29 for every one score increase on the SCQ. Only autistic phenomenology (SCQ scores) was a significant predictor of sensory processing difficulties (t (37) = −2.92, p < .05).
To further explore the relationship between SID and autistic phenomenology in children with ONH, a Pearson’s correlation was carried out on the total scores and sub-domain scores of the SSP and SCQ; the results are reported in Table 3.
Statistically significant correlations were found in the following; SCQ reciprocal interaction sub-domain and the SSP sub-domains of tactile sensitivity, under-responsive/seeks sensation, low energy, and the adjusted total scores. The SCQ stereotyped behaviours domain and SSP sub-domains of tactile sensitivity, taste/smell, under-responsive/seeks sensation, auditory adjusted, and adjusted total score also showed statistically significant correlations. Furthermore, statistically significant correlations between the SCQ communication domain and the SSP sub-domains of tactile sensitivity and low energy were observed. All, but two of the SSP sub-domains (auditory filtering and movement sensitivity) showed statistically significant correlations with the SCQ total score. These findings indicate that lower level SSP scores are related to higher levels of SCQ sub-domain and SCQ total scores.
Discussion
In this cohort of children with ONH, 58% reported ‘definite differences’ in their processing of sensory information in their intact senses. This percentage is considerably higher than reported SID for typically developing children (Ahn et al., 2004), but within the range of reported percentages for children who present with a similar symptomatology to children with ONH, and in particular, ASC and/or intellectual disability (Cheung & Siu, 2009; Little, Tomchek, & Dunn, 2016; Tomchek & Dunn, 2007).
Out of the 22 children who were suspected of ASC, 19 children showed ‘probable’ or ‘definite’ differences in their processing of sensory information, and these children were more likely to present with a severe to profound, or near to total loss of vision, and greater levels of intellectual disability (Table 2). To assess which of these symptoms best predicted SID in children with ONH, multiple regression analyses were used, which showed that ASC symptomatology was the best predictor of SID. Looking more closely at ASC symptomatology and SID for this current cohort of children, Pearson’s correlations reported the strongest statistically significant associations between the stereotyped behaviours sub-domain of the SCQ and the sub-domain of tactile sensitivity and the adjusted total score on the SSP. This finding is similar to research assessing SID in children with ASC, which has reported that tactile over-responsivity is associated with more rigid stereotyped behaviours (Baranek et al., 2006). Similarly, Gal et al. (2010) reported statistically significant relationships between stereotyped movements and tactile sensitivity in a group of children with visual impairments and intellectual disability. However, what is not known from previous research or from this study is the origin of the relationship between SID and stereotyped behaviours in children with ONH. These behaviours could be a result of either ASC or autistic-like behaviours due to children’s visual loss, or both. For example, it is proposed that reduced incidences and opportunities for exploration due to visual loss increase the likelihood that children may engage in stereotyped behaviours, and Lowenfeld (1973) postulates that this could lead to autistic-like phenomenology in visually impaired children. The reported SID in this study may be explained by the constraints that visual loss poses on the types of activities that a blind individual can engage in, and, in-turn, they may appear to lack typical responses to processing of sensory information (Lewis et al., 2000) and thus they present with a range of SID in their intact senses.
Finally, this study is the first to identify the uneven profile of SID in children with ONH. All sub-domains of the SSP reported ‘probable’ and ‘definite’ sensory processing difficulties although the number of children who reported SID differed across the sub-domains of the SSP. The highest percentage of ‘definite differences’ was reported on the sub-domain of auditory filtering (78%), under half of the children showed ‘definite differences’ in their tactile sensitivity and a third reported ‘definite differences’ in their taste/smell sensitivity on the SSP. These present findings are line with previous observations of SID in children with ONH (Bahar et al., 2003). Importantly, this study now adds new findings to research literature that children with ONH show the high percentages of ‘definite differences’ on the sub-domains of under-responsiveness/seeks sensation (61%) and low energy/weak (66%) on the SSP.
Children with ONH present with a varied clinical profile of visual impairment and intellectual disability, and the rarity of the condition can pose problems for statistical analysis. In this study, we experienced these problems, but it was important to present a complete clinical picture of SID in a cohort of children with ONH, which best reflects this population of children; however, this did limit the statistical exploration of data at times.
Children with ONH show varying degrees of neurologic impairments, which include the agenesis of the corpus callosum, and previous research has identified that corpus callosum abnormalities are associated with SID (Demopoulos et al., 2015). Additionally, it is widely accepted that children with ONH present with abnormalities in their taste, smell (anosmia), and an increased appetite due to associated hormonal deficiencies due to hypothalamic–pituitary axis abnormalities (Webb & Dattani, 2010). These neurologic abnormalities could explain why a third of our cohort showed ‘definite differences’ in their sensory processing of taste and smell. However, as some of our current cohorts were recruited from charities, magnetic resonance imaging (MRI) findings were not accessible for all of these cohorts of children. In light of these findings, future research could consider exploring the relationship between SID, hypothalamic–pituitary axis abnormalities, and corpus callosum abnormalities.
Additionally, a detailed analysis of spatial exploration, fine and gross motor skills, and SID could explain how interactions with the environment contribute to SID in children with visual impairments. Importantly, further research needs to explore the high incidences of children reporting with under-responsiveness/seeking sensation and low energy/weak on the SSP. This research would need to consider whether these reports are due to reduced incidences and opportunities for exploration, sleep disturbances, or associated hormonal deficiencies, which are known to cause fatigue in children with ONH (Webb & Dattani, 2010).
A limitation of this study is that it is unknown whether SID is specific to children with ONH, or generalisable to other conditions which lead to visual impairment. To better understand the impact of intellectual disability and/or visual deficits upon SID, we will undertake future research with the inclusion of children with visual impairment who have no associated or known involvement of the central nervous system, and a group of children who are sighted and have an intellectual disability.
The results above indicate the importance of professionals considering that many children with ONH display varied SID in their intact senses, which are related to their syndrome characteristics. Sensory hyposensitivities or hypersensitivities impact children immensely in their daily lives; therefore, awareness among professionals in educational and clinical settings is essential in ensuring that intervention and identification of SID occur at the earliest opportunity (Gense & Gense, 2005; Jordon, 2005). Early educational programmes need to include methods to help children to integrate, and effectively use their intact senses, in order to reduce some of their hyposensitivity and hypersensitivity to sensory information.
Footnotes
Acknowledgements
The authors wish to thank the children and their families for their participation in the study. The authors would like to thank Professor Linda Pring and Professor Chris Oliver for their professional advice and support for the development of this work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by a PhD grant from the Endocrinology trustees at the Birmingham Children’s Hospital and the University of Birmingham, School of Psychology.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.