
Abstract
The aim of this study was to investigate the impact of visual impairment (VI) on static and dynamic postural control and habitual physical activity in puberty-age children.A total of 26 children aged 10–16 years participated in the study: 13 children with VI and 13 age-matched sighted children as controls. Static and dynamic balance characteristics in eyes open (EO) and eyes closed (EC) condition were measured during standing on a dynamographic force plate. The level of habitual physical activity was evaluated with modified Baecke questionnaire scores. Associations between measured characteristics were analyzed.
Center of pressure sway in anterio-posterior and medio-lateral direction, sway radius and area in EO condition of static and dynamic tests in children with VI were greater (p < .05) in both static and dynamic exercises compared with sighted children, while postural control characteristics in EC condition did not differ between the two groups. In children with VI, characteristics of postural control were correlated to habitual physical activity in leisure time and to the age of starting sport activities in comparison with sighted children, who did not demonstrate significant associations between these characteristics. Postural control characteristics in EO condition in children with VI were greater compared with sighted children, and these data are also associated with the leisure time physical activity and the age of starting with sport activities. It is recommended to engage children with VI in sport activities earlier, especially in moderate-to-vigorous physical activity, and provide them with versatile possibilities to do so.
Introduction
Postural control (PC) is aimed at maintaining the body position and orientation in the field of gravity and maintaining balance despite perturbing effects of internal and external forces (Vaugoyeau, Viel, Assaiante, Amblard, & Azulay, 2007). Intact vision complements activities of the vestibular system (Held-Ziółkowska, 2006), thus creating a well-functioning PC system. In the case of visual impairment (VI), limitations of the use of the spatial reference system and precise correction of body alignment occur, thereby negatively affecting the maintenance of body posture and balance (Wade & Jones, 1997).
It has been noted that switching off visual and vestibular input has no significant effect on the PC of young persons (Vaugoyeau, Viel, Amblard, Azulay, & Assaiante, 2008). However, adults with VI have worse postural stability than normal-vision people in eyes closed (EC) condition (Uchiyama & Demura, 2008), on compliant surfaces and during dynamic balance tests (Tomomitsu, Alonso, Morimoto, Bobbio, & Greve, 2013; Willis, Vitale, Agrawal, & Ramulu, 2013). Another study using the Movement Assessment Battery for Children demonstrated that children with VI had lower scores in static and slow dynamic balance exercises compared with sighted children, but they had equal scores in fast dynamic exercises (Houwen, Visscher, Lemmink, & Hartman, 2008). This is explained by visual information being more important in maintaining static balance compared with dynamic balance, because performing fast movements is mostly based on the information transmitted by proprioceptive and vestibular information (Hatzitaki, Zisi, Kollias, & Kioumourtzoglou, 2002). Compared to persons with acquired VI, the congenitally blind demonstrate greater postural stability while standing on firm surface or foam pads (which decreases the somatosensory input) and with open or closed eyes (manipulating visual input) (Schwesig et al., 2011). PC depends not only on the degree of vision loss, but also on the age of the participants: 12–16-year-old children achieved significantly better results in balance tests than 6–11-year-old children; however, it was also shown that in children between 7 and 10 years emerge similarities to adults concerning balance characteristics (Cuisinier, Olivier, Vaugoyeau, Nougier, & Assiante, 2011). Static and dynamic balance definitely improves with age and reaches its maximum level at the age of 15–16 years (Steindl, Kunz, Schrott-Fischer, & Scholtz, 2006).
PC has vital importance in the motor development of young children as all further skills are based on it. Since motor skills are related to physical activity (Houwen, Hartman, & Visscher, 2009), it is important to engage children in active play and sports at an early age. Several studies have shown that motor performance of children with VI is lower compared with sighted children, and learning new skills is more difficult for them (Houwen et al., 2009; Whitall, 2003). It was found that children with VI demonstrate lower physical activity levels and poorer physical fitness participation (Augestad & Jiang, 2015), which are risk factors for health and can lead to negative adaptations in the body (World Health Organization [WHO], 2010b). There is insufficient information about the average age at which children with VI are starting sporting activities.
The PC of adults with VI has been sufficiently evaluated (Tomomitsu et al., 2013; Willis et al., 2013). Although there is some evidence about disturbances of functional (Rutkowska et al., 2015) and static (De Araújo et al., 2014) balance in children with VI, there is lack of objective data on PC (dynamographic or stabilometric) related to dynamic balance without visual input. Moreover, there is no knowledge about how PC is related to habitual physical activity in children with VI. Our study is aimed at investigating the impact of VI on static and dynamic PC (in eyes open [EO] and EC condition) and habitual physical activity in children aged 10–16 years. Associations between PC characteristics and children’s habitual physical activity were also studied. We hypothesized that children with VI have considerably poorer PC characteristics in all test conditions (EO, EC, static balance, dynamic balance), but especially in EO and dynamic test conditions. The other hypothesis was that their habitual physical activity level is lower and they start practicing sports at a later age compared with sighted children and that earlier and greater physical activity is related to better PC in both the groups.
Methods
Participants
A total of 17 children aged 10–16 years with VI were recruited from the special school for the blind and visually impaired children. The following exclusion criteria were determined on the basis of medical records and interviews: blindness, any disease or disability affecting the sense of balance, and intellectual limitations. Four children who volunteered in the study were excluded from the data analysis: one child was totally blind, two children were younger than 10 years, and one child had leg length discrepancy (>1 cm).
A total of 13 children with VI (8 girls and 5 boys) and 13 randomly selected age-and-gender-matched sighted children (controls, 8 girls; 5 boys) mainstream school of the same town volunteered. All the participants and their legal representatives gave informed written consent prior to the study. The study was approved by Research Ethics Committee of the University of Tartu.
By the WHO classification, described in ICD-10 (WHO, 2010a), the VI level of the studied children with VI ranged from moderate (six subjects) to severe low vision (seven subjects). None of controls had VI. The respective assessments were based on documented data (compiled by ophthalmologists at special school, and the medical documentation compiled at mainstream school).
Assessment of PC
Postural stability was evaluated by the sway of the center of pressure (COP), which was registered standing on the dynamographic platform Kistler 9286A (Kistler Instrument AG, Switzerland) and analyzed with Elite Clinic movement analysis system SWAY® software (BTS, S.p.A, Italy). In order to standardize the body position and concentrate attention, the participants looked at a well visible mark (printed full circle with the diameter of 20 cm) on the wall at a distance of 2 m. Postural stability of the body was evaluated during the following static and dynamic exercises:
Exercise 1 (static test): standing on two legs, positioned together, arms on the sides
Exercise 2 (static test): standing on one leg, the other leg 90° flexed in the knee joint, arms on the sides.
Exercise 3 (dynamic test): standing on one leg, the contralateral straight leg swaying back and forth in the rhythm provided by metronome: one movement per second in each direction.
Standing on one leg (Exercise 2) is a very typical test for evaluation of the static balance in children, and it is used in many standardized test batteries like Movement Assessment Battery for Children-2 (MABC-2) or Bruiniks-Oseretsky Test of Motor Proficiency-2 (BOT-2; Rutkowska et al., 2015), also for investigation of pelvic girdle stability (Stork test; Hungerford, Gilleard, Moran, & Emmerson, 2007). It was shown that hip joint angle influences PC and COP sway is maximal when contralateral leg’s hip joint is flexed by 90° compared with 30° and 60° due to greater muscle force (if the length of the external moment arm is greater than the length of the internal moment arm; Cha et al., 2017). In our study, Exercise 3 assesses dynamic balance that is similar to the walking or stepping activity, where it is necessary to maintain balance on one leg while the other one is moving. Similar tests are used for assesment of posture-stabilizing mechanisms, for example, Jeté or drowing-like movements in ballet dancers (Lepelley, Thullier, Koral, & Lestienne, 2006).
Before the study, all participants were familiarized with PC tests and did preliminary Exercises 1–3 (1–2 trials) to prevent the learning effect (Zemková et al., 2017). All the tests lasted for 15 s and were performed in EO and EC condition with 3-min rest between the exercises, during which the participant sat on a chair with back support. Exercises 2 and 3 were performed with the participant standing initially on the right and then on the left leg. The dominant leg was identified prior to the tests with performing the task of kicking a ball. Left leg dominance emerged in three children of the VI group and in one child of the control group. It has been noted that children with VI tended to impose weight on the right side, while control group participants tended to impose weight on the left side (De et al., 2014). Considering this, we decided to present the data for the right and left leg separately.
Three postural stability parameters were analyzed in the study:
COP sway in anterioposterior (AP) and mediolateral (ML) direction
Radius of the path of COP sway (COP sway radius)
COP sway area.
The data were normalized according to the body height (m) and length of the foot (mm) of the participants (Chiari, Rocchi, & Cappello, 2002).
Assessment of habitual physical activity
Physical activity was assessed using the Baecke questionnaire (Baecke, Burema, & Frijters, 1982). This questionnaire comprises 16 questions and maps in three domains: work, leisure time, and sport participation. Individual question scores varied from 1 to 5. For the purposes of this study, and relying on the study of Deforche, De Bourdeaudhuij, and Tanghe (2006), the total score was obtained only from the sum of scores of leisure time physical activity and sport participation. In addition, participants were asked about the age of starting sports activity and its type. All children answered the questionnaire under the supervision of the member of qualified research team. Prior to the present investigation, the pilot study was performed with 10–16-year-old sighted children (n = 10) for validating the questionnaire in Estonian.
Data analysis
Data are means and standard errors (SE). One-way analysis of variance (ANOVA) followed by Fisher’s least significant difference (LSD) test was performed with SPSS software version 20 (SPSS Inc., Chicago, IL, USA). Differences between groups were considered significant at p < .05. For assessing clinical significance between groups, effect size (ES) and minimal important difference (MID) were found. Differences between groups were considered clinically significant if these conditions were met: ES ≥ 0.4 and MID was lower than the mean difference between the studied groups (Armijo-Olivo, Warren, Fuentes, & Magee, 2011). Partial correlations controlling for the vision level in children with VI and Spearman’s correlations in sighted children were calculated to evaluate associations between PC and physical activity characteristics. Pearson’s correlations were computed to investigate relations between age of starting sport activities and PC characteristics.
Results
The mean age of children with VI (13.1 ± 0.6 years) was similar to sighted children (13.2 ± 0.6 years). We found no significant differences in body height and body mass between children with VI and sighted children (158.2 ± 0.04 cm and 160.7 ± 0.03 cm, respectively, p > .05; and 50.0 ± 3.7 kg and 55.2 ± 4.2 kg, respectively, p > .05).
Static and dynamic PC characteristics in EO and EC conditions are presented in Table 1. Children with VI demonstrated greater COP sway radius (p = .023. ES = .95) and COP sway area (p = .019; ES = .98) in quiet standing on two legs in EO condition compared with sighted children. No statistically relevant (p > .05) differences emerged between groups in standing on two legs in EC condition, although COP sway in ML direction and COP sway radius was clinically different (ES = .70 and ES = .66, respectively).
Postural control characteristics (mean ± SE) in children with visual impairment (VI) and sighted children.
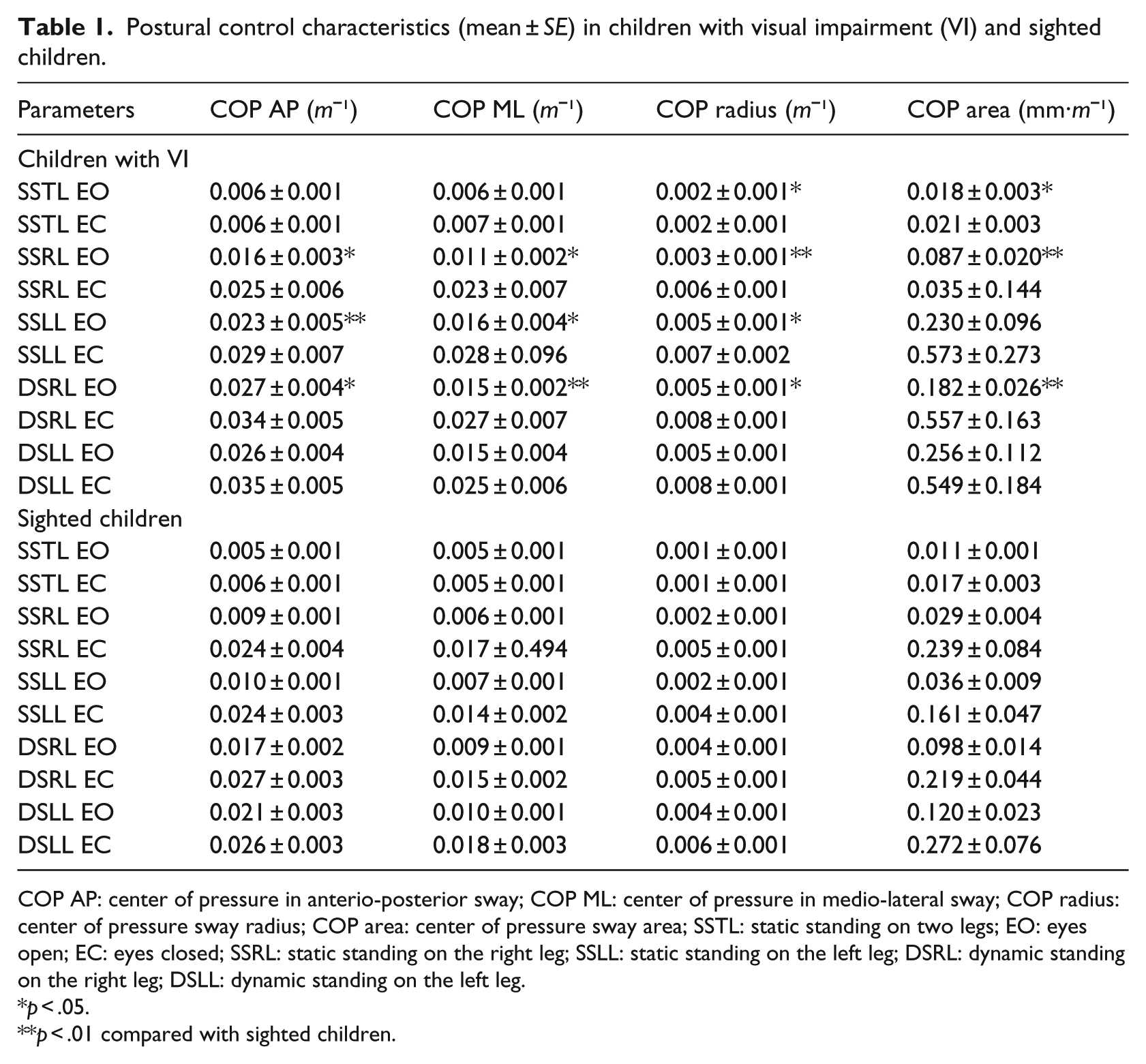
COP AP: center of pressure in anterio-posterior sway; COP ML: center of pressure in medio-lateral sway; COP radius: center of pressure sway radius; COP area: center of pressure sway area; SSTL: static standing on two legs; EO: eyes open; EC: eyes closed; SSRL: static standing on the right leg; SSLL: static standing on the left leg; DSRL: dynamic standing on the right leg; DSLL: dynamic standing on the left leg.
p < .05.
p < .01 compared with sighted children.
During static standing on one leg in EO condition, children with VI had greater COP sway in AP (on right leg p = .051, ES = .81; on left leg p = .015, ES = 1.03) and ML (on right leg p = .045, ES = .83; on left leg p = .025, ES = .94) directions as well as COP sway radius (on right leg p = .002, ES = 1.34; on left leg p = .017, ES = 1.01). COP sway area was greater in children with VI compared with sighted children only in standing on the right leg (p = .009, ES = 1.11), in standing on left leg the difference was at level p = .56, but clinically different (ES = .79). We did not find statistically significant (p > .05) differences between groups in standing EC on the right or on the left leg, although clinically significant difference was found for COP sway in ML direction (ES = .56) and COP sway radius (ES = .49) and area (ES = 0.58) at standing on left leg.
During dynamic standing on the left leg and moving the right one, children with VI demonstrated greater COP sway in AP and ML directions (p = .034, ES = .88; and p = .005, ES = 1.20, respectively), COP sway radius (p = .022, ES = .96) and COP sway area (p = .009, ES = 1.11) in EO condition compared with sighted children. Dynamic PC parameters in standing on the right leg and moving the left one with EO, or standing in dynamic condition with EC did not differ (p > .05) between the groups. However, COP sway radius values were clinically different during standing on right leg and moving the left one with EO (ES = .56) and with EC (ES = .55). We noted similar trend for COP sway radius and area during standing on left leg and moving the right one with EC (ES = 0.79 for both characteristics).
Characteristics of physical activity are presented in Table 2. Children with VI demonstrated lower (p < .001) sports participation scores, as well as total physical activity score (p < .001) and they had started practicing sports at considerably later age (p < .014) than sighted children. Also, they were practicing mostly low-to-moderate intensity sports, like bowling or sailing (average energy expenditure 0.76 MJ/hr, according to Baecke et al., 1982), compared with sighted children, who mostly practiced moderate-to-vigorous intensity sports, like track and field, soccer or basketball (average energy expenditure 1.26 MJ/hr, according to Baecke et al., 1982).
Physical activity scores assessed by modified Baecke questionnaire and the age of starting sport activities (mean ± SE) in children with visual impairment (VI) and sighted children.

p < .01.
p < .001 compared with sighted children.
In children with VI, we found significant negative correlations (r = −.58; r = −.85, p < .05) between leisure time activity score and static PC parameters in EC condition and between leisure time activity score and dynamic PC parameters in EO condition (Table 3). Higher leisure time physical activity level correlated with smaller body sway during quiet standing. In children with VI, characteristics of PC positively associated (r = .56; r = .62, p < .05) to the age of starting with sport activities (Table 4). In children without VI, we noted significant correlations between PC characteristics and leisure time physical activity level, as well as the age of starting sport activities, only in static standing on the right leg and dynamic standing on left leg, both with EO (r = .61; r = .70, p < .05).
Associations between leisure-time activity and PC characteristics in children with VI and sighted children.

PC: postural control; VI: visual impairment; EO: eyes open; EC: eyes closed; SSTL: static standing on two legs; SSRL: static standing on the right leg; SSLL: static standing on the left leg; DSRL: dynamic standing on the right leg; DSLL: dynamic standing on the left leg; COP AP: center of pressure in anterio-posterior sway; COP ML: center of pressure in medio-lateral sway; COP radius: center of pressure sway radius; COP area: center of pressure sway area.
Partial correlations controlling for vision level in children with VI and Spearman’s correlations in sighted children are presented.
Significant correlations between age of starting sport activities and PC characteristics in children with VI and sighted children.

PC: postural control; VI: visual impairment; EO: eyes open; EC: eyes closed; SSRL: static standing on the right leg; DSRL: dynamic standing on the right leg; DSLL: dynamic standing on the left leg; COP AP: center of pressure in anterio-posterior sway; COP ML: center of pressure in medio-lateral sway; COP radius: center of pressure sway radius; COP area: center of pressure sway area.
Partial correlations controlling for vision level in children with VI and Pearson’s correlations in sighted children are presented.
Discussion
This study was undertaken to compare PC and habitual physical activity characteristics in static and dynamic test conditions with EO and EC, as well as establish associations between these characteristics in children with VI and their sighted peers. Previous studies have indicated that children between 7 and 10 years begin to demonstrate similarities of body balance to adults (Cuisinier et al., 2011) and their ability to maintain balance does not depend on gender (Rutkowska et al., 2015). For this reason, children for our study were selected in the age bracket of 10–16 years, irrespective of gender.
The main results of our study included the following observations. Children with VI had greater COP sway parameters during EO stance and lower habitual physical activity level, and they were also older when starting sport activities. Lower leisure time activity in children with VI correlated with greater body sway during static and dynamic standing. Similarly, higher age when starting sport activity correlated with greater body sway during dynamic standing. Interestingly, in sighted children such clear relations between the age of starting sport activity or leisure time activity and PC were absent. It has been shown that participation in physical education and sports lessons is similar in adolescents with VI and their sighted peers (Demirturk & Kaya, 2015). However, Houwen et al. (2009) noted that participation in moderate-to-vigorous physical activity in children with VI is significantly lower than in sighted children. They found that participation in sport lessons that are adapted to children with VI is not sufficient for fulfilling modern requirements for daily physical activity or the development of basic motor skills. Why do children with VI have poorer PC despite practicing sport? The possible reason is that they are frequently recommended to go in for sports involving light physical activity levels or less demands on motor skills (Ponchillia, Armbruster, & Wiebold, 2005), and that is not sufficient for promoting adequate development of body balance. According to our experience, this also applies for Estonia. The opportunities to practice sports and availability of qualified specialists to manage trainings of children with disabilities being limited in Estonia, as well as overprotection by parents are reasons why the versatility and training loads of children with VI differ greatly from the related possibilities open for sighted children. However, the leisure time activity level of the measured groups was similar, the PC characteristics of children with VI was strongly related to their physical activity in leisure time. This can be explained by the different nature and limited diversity of the activities practiced by children with VI in leisure time, but unfortunately the questionnaire applied in our study did not cover that aspect very thoroughly.
Practicing sports is very important to children with VI, because it bolsters the sense of independence and autonomy, generating multiple benefits of physiological, sociological, and psychological nature (Çolak, Bamaç, Aydin, Meriç, & Özbek, 2004). We agree with the above statement. Since several motor skills are based on PC, the poorer balance can jeopardize or limit engagement in sporting, as well as in leisure time physical activity, and therefore decrease independence in everyday activities.
The information about the environment and the localization of the body segments that children with VI receive does not enable them to create adequate compensatory proprioceptive reactions, which in turn increases body sway (Juodžbaliené & Muckus, 2006). Previously, Brambring (2006) reported that maintaining balance in dynamic conditions is far more difficult for blind children than maintaining static balance. It has also been shown in other studies that the static PC of blind adults is significantly poorer than of people without VI in EO condition and does not differ from them in EC condition (Ozdemir, Pourmoghaddam, & Paloski, 2013; Sobry, Badin, Cernaianu, Agnani, & Toussaint, 2014). In our study, the PC of children with VI was poorer in static as well as in dynamic conditions compared to controls. The main differential determinants were PC values in EO condition that are in agreement with several studies (Juodžbaliené & Muckus, 2006; Ozdemir et al., 2013; Sorby et al., 2014). None of our visually impaired participants were totally blind, so we can claim that the impaired vision did disrupt their balance mostly in EO condition, but intact vestibular and proprioceptive functions provided better postural reactions in EC condition.
Conclusion
The results of the study indicated that static and dynamic PC characteristics with open eyes in children with VI aged 10–16 years were greater compared with sighted children. On one hand, children with VI demonstrated lower habitual physical activity level and they started sport activities later. In children with VI, the lower leisure time activity associated with the greater body sway during static and dynamic standing. On the other hand, the age at which sport activity is begun, plays a significant role—the later the sport activity was started, the greater was the body sway during dynamic standing. This refers to the need to widen the possibilities to practice sports and to be physically active during leisure time for children with VI.
Limitations
The limitations of this study are the small sample size and the usage of questionnaires for reporting physical activity. Nevertheless, the participants’ groups were sufficiently homogeneous in baseline characteristics to support the value of our study.
Footnotes
Acknowledgements
We are grateful to the subjects who participated in this study. We thank Kristo Ringas and Karin Länts for their contribution to the study. I.M. conceived the idea of the study, participated in its design, performed the statistical analysis and wrote the final version of the manuscript, R.K. and H.G. participated in the design of the study, carried out the assessments and helped to draft the manuscript. J.E. performed the part of statistical analysis. M.P. helped to draft the manuscript. All the authors read and approved of the final manuscript.
Availability of data and materials
Please contact the corresponding author for data requests.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was partially supported by Republic of Estonia Ministry of Education and Research, Institutional project IUT20-58.