
Abstract
Study’s purpose:
To analyze the effectiveness of telephone intervention for the nursing diagnosis of delayed surgical recovery in older persons who have undergone cataract surgery.
Design:
Blinded, randomized, and controlled trial. A total of 95 patients of both sexes who were over 60 years old and had undergone cataract surgery were divided into an intervention group (48 patients) and a control group (47 patients), allocated using BioEstat 5.3 Software.
Results:
The intervention included postoperative follow-up recovery of cataracts and prevention of complications performed on the 1st, 4th, 10th, and 20th postoperative days. After the intervention, the intervention group had a decrease in the length of surgical recovery (p = .000). The occurrence in the intervention group was 6.3%, while in the control group, it was 36.2% (odds ratio (OR) = 0.118; confidence interval (CI) = 1.02, 10.23). The number of nursing interventions nevertheless decreased during the telephone follow-up.
Conclusion:
For older persons, the telephone guidelines increase adherence to treatment, promote clinical improvement, promote surgical recovery over time, and improve independence and autonomy.
Introduction
Delayed surgical recovery (DSR) is a clinical situation in which there is an “extension of the number of postoperative days required to initiate and perform activities that maintain life, health and well-being” (Herdman & Kamitsuru, 2018). This issue is a nursing responsibility, and research on the effectiveness of DSR interventions is needed. Considering the vulnerability of elderly persons, nursing interventions can be implemented to reduce the occurrence of a DSR diagnosis in this population.
A cataract consists of partial or total opacity of the lens (Rothrock, 2014). This disease can be reversed by appropriate surgical intervention, called cataract extraction surgery. The expected recovery time to return to work is from 3 to 7 days if the work does not require great effort (Rothrock, 2014). However, the rate of postoperative complications for such surgical procedures can range from 2.0% to 14.7%. The main factors are increased intraocular pressure, corneal edema, posterior capsule opacity, inflammatory process, and endophthalmitis (Barreto, Primiano, Espíndola, Germano, & Kara, 2010).
Currently, the number of surgeries performed in the shortest transoperative period, called fast tracking, has been increasing. In these surgeries, the patient remains as short as possible in the surgical anesthetic recovery room (Barreto et al., 2010), reducing hospitalization length and available time to provide information to the patient.
In this context, some strategies are applied during postoperative follow-up, such as the monitoring of these patients to detect problems in an early and efficient way, performed through the computer for virtual consultations, the use of telephone monitoring, video conferencing, and mobile messages—short message service (SMS) (Rezende, Melo, Tavares, Santos, & Souza, 2010). The telephone follow-up is a nursing intervention involving “Providing results of testing or evaluating patient’s response and determining potential for problems as a result of previous treatment, examination, or testing over” (Dochterman & Bulechek, 2012) through nursing telephone calls, as implemented in this study.
For nurses, the modernization process of the health care, education, and nursing care is important and can increase the quality of the service provided. Thus, if used properly, the technologies can contribute to rationalize and improve the nursing communication process, helping the patient to achieve better results with the highest possible safety and improving the support of the nursing care (Cunha, Barreto, Costa, Nascimento, & Vieira, 2014; Jost, Viegas, & Caregnato, 2018).
Background
The ease of using telephones in health services allows quick access of patients to health professionals, reduced wait times for an appointment, and decreased time and cost in the locomotion of patients. In addition, it enables an increase in the frequency of contact and facilitates the return to the patient (Vasconcelos et al., 2013).
Therefore, technology requires a scientific rationale, with a structure similar to the nursing process, that is, identification of a need underlying its implementation, as well as planning for predetermined results to be achieved in the short, medium, and long term (Spiri & MacPhee, 2013).
The use of telemonitoring has been increasing, and efforts are underway to provide high-quality care, also aiming at cost-effectiveness (Rezende et al., 2010). Researchers have observed that telephone follow-up is associated with the continuity of care, offering pertinent teaching and guidance in the postoperative period according to the needs of each patient (Caljouw, Hogendorf-Burgers, 2010; Godden, 2010).
Therefore, this study aims to analyze the effectiveness of telephone intervention for the nursing diagnosis of DSR after cataract surgery in older persons.
Methods
Study design
Blinded, randomized, and controlled trial with two parallel groups.
Participants
The study was carried out in two hospitals located in the city of Niterói, Rio de Janeiro, Brazil, one public university hospital and the other, a reference in ophthalmologic surgeries. Eligible participants were older persons who were hospitalized for a cataract surgery and consented to the terms proposed by the study. The inclusion criteria were as follows: being 60 years old or older, preparing to receive cataract surgery, and having a cell phone or landline available for contact by the nurse. Patients were excluded for the following reasons: presence of dementia, auditory deficit with no accompanying person or family member who could receive the telephone interventions, and previously underwent surgeries for the treatment of prior surgical complications. The discontinuity criterion was answering fewer than 75% of telephone calls.
Intervention
The study participants were recruited in the preoperative period by co-investigators who reported on the research and obtained written consent. The study participants were divided into two groups randomly: one experimental group and one control group. The nursing intervention was implemented as follows. The control group had access only to conventional treatment, without telephone monitoring, but masked connections were made only to inform participants of the date of the next consultation to protect groups.
The experimental group had access to telephone follow-up performed by the principal investigator and conventional treatment. The applied intervention included actions related to postoperative follow-up recovery of cataracts and prevention of complications performed at the 1st, 4th, 10th, and 20th postoperative days.
To ensure that the auxiliary investigators evaluated the outcome correctly and safely, the first step was training to diagnose DSR. All auxiliary investigators were registered nurses with experience in research and surgical nursing specialists. This training ensured a more accurate assessment of the health status of the older person and reduced the impact of the so-called imperfect gold standard. The auxiliary investigators applied an instrument to the participants in the experimental and the control groups to evaluate the outcome variables of the diagnosis.
The follow-up to identify the DSR diagnosis was performed at the ophthalmology outpatient clinic on the days of the patients’ follow-up medical appointments.
The follow-up of the participants in the outpatient clinic lasted 4 weeks, and according to the literature, the return to work usually occurs within up to 7 days (Rothrock, 2014). Therefore, participants were assessed for diagnosis at days corresponding to D1 (first postoperative day/first DSR evaluation), D7 (seventh postoperative day/second DSR evaluation), and D30 (thirtieth postoperative day/third DSR evaluation), or the day closest to these dates because of holidays and weekends (Figure 1).
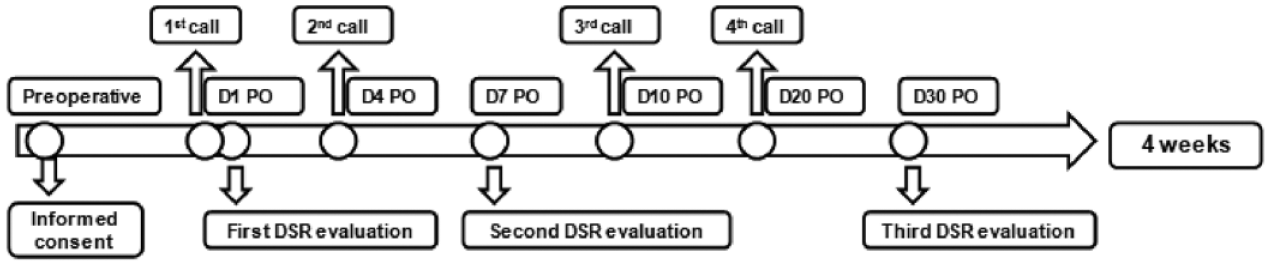
Monitoring of the intervention group (n = 48).
The principal investigator performed the telephone monitoring through a semi-structured call instrument using computerized, registered software. This follow-up occurred on D1 (first call made for initial contact), D4 (second call), D10 (third call), and D20 (fourth call).
The calls occurred during the week, from 8 am to 6 pm, in the telephone management room. On saturdays, the main researcher made the calls from her personal phone from 8 am to 12 am. At the end of the call, the researcher scheduled the next call on the participant’s preferred day and time.
Outcomes
To measure the effectiveness of the intervention, the primary outcome measure was full surgical recovery, that is, absence of a DSR nursing diagnosis. The secondary outcome measures were a decrease in the occurrence of the defining characteristics of and factors related to a DSR nursing diagnosis, such as pain, discomfort, improvement of self-care, complete healing of the surgical area, absence of surgical wound infection, and reduction of anxiety, worry, and fear.
Sample size
The sample size was determined by means of the Pocock (1983) formula: n = P1 * (100 – P1) + P2 * (100 – P2)/(P2 – P1)2 × f(α, β), where P1 = percentage of events in the experimental group, P2 = percentage of events in the control group, and f = frequency of alpha and beta errors.
For the estimation of the P1 and P2 proportions, a pilot test was performed with 16 patients (eight in each group) from May to July 2014. The analysis of the pilot test showed that among the eight patients in the experimental group, there were no DSR cases, or P1 = 0/8 = 0.0%. The control group had three cases of DSR on the seventh postoperative day, which resulted in P2 = 3/8 = 37.5%, and a 0% estimate cannot be considered for P1. In this case, the recommendation is to assume that at least one patient in the experimental group presented DSR, and P1 = 1/8 = 12.5% and P2 = 3/8 = 37.5% were considered. In addition to these pre-test parameters, a maximum significance level of 5% (α) and statistical power of 85% (1 – β) were considered. For these parameters, f (α, β) = 8.5, the minimum n value determined by expression (1) was 47 patients in each group, control and experimental, totalling 94 patients in the sample.
The sample selection process was developed during the period from August 2015 to December 2016.
Randomization
A total of 95 patients were randomized into two groups (experiment and control) by simple randomization of the sample. BioEstat 5.3 Software was used for randomized allocation, which selected 48 participants for the experimental group and 47 participants for the control group. The principal investigator elaborated and applied the randomized sequence of allocation to the study participants to carry out the intervention and maintained exclusive possession during the research.
Blinding
The examiners with diagnosis training who collected the data were unaware which patients would receive the intervention or conventional follow-up. To ensure masking, the experimental and control groups received reminder calls for 4 weeks to confirm the date of return to the outpatient clinic. Thus, even if the participants said they had received calls, the researchers would not know who received the intervention.
Statistical methods
The following tests were performed for inferential analysis of the incidence of DSR diagnosis at a significance level of .05 or less: For association analysis between qualitative variables and the diagnosis of DSR, a Fisher’s exact test or a chi-square test was used. The measure used to assess risk was the odds ratio (OR). For numeric data, the Kolmogorov–Smirnov test, Student’s t-test, Levene’s test, the non-parametric Mann–Whitney test, and Wilcoxon’s test were performed based on normality assumptions. When there was a need to compare more than two repeated measures, analysis of variance (ANOVA) was performed for repeated measures if the variables were normal, and the Friedman test was used if the variables did not follow normal distribution.
Ethical considerations
Ethical approval was obtained from the Research Ethics Committee of the Hospital, under a certificate of ethical appreciation. Volunteers were informed about the research and about the right not to participate or withdraw from the study at any time without causing any harm to their care. Participants who agreed to participate in the study signed a written consent form.
Results
Flow of participants
The total number of participants approached to carry out this study was 264. From this total, 76 participants who had their surgery canceled, and 93 participants who did not meet the inclusion criteria were subtracted: 18 refused to participate in the study, 47 were under 60 years old, 13 did not have a contact telephone, 7 had complications before the surgical procedure, and 8 were in readmission. The study did not observe over-recruiting or potential loss to follow-up. The follow-up presented, thus, a randomized sample of 95 participants, 48 in the experimental group, and 47 in the control group. There was no loss to follow-up in either group. Figure 2 presents a flow diagram of the participants throughout the study.
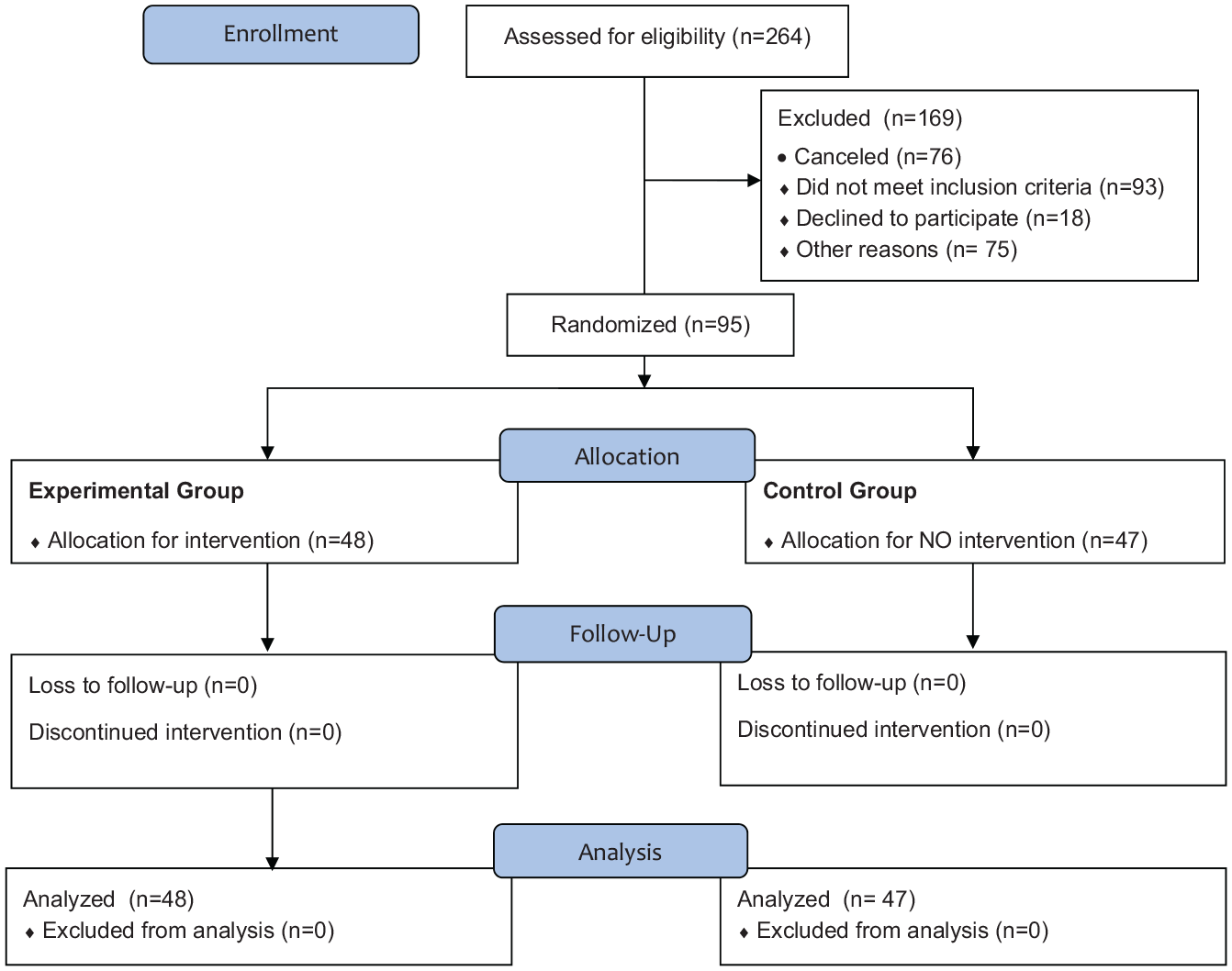
CONSORT flow diagram.
Sample homogeneity
To verify whether the sample was homogeneous, the characteristic profile of the participants was traced. The control and experimental groups had the same formation characteristics, that is, the same baseline initial conditions. There were no significant differences in the distribution of patients between the control and experimental groups with respect to gender (p-value = .436), marital status (p-value = .672) and comorbidities: hypertension (p-value = .296) and cancer (p-value = .617).
Both groups presented a prevalence of women, typical of the older population (60.4% in the experimental group and 68.1% in the control group), as well as a prevalence of married participants (43.8% in the experimental group and 51.1% in the control group). Important data related to the effectiveness and importance of the systematization of the tested intervention refer to education, as approximately 50% (47 participants) did not complete elementary school.
Therefore, these participants need continuity in post-discharge care to ensure their understanding of information and care related to recovery. In all these cases, the distribution of men and women in the control and experimental groups did not present significant differences.
The patients who had cataract surgery presented a mean age of approximately 71 years were married (47.4%), did not complete elementary school (49.5%), systemic arterial hypertension (69.5%), and presented KATZ classification A (68.4%) and an average LAWTON of approximately 19. The distribution of KATZ, LAWTON, Mini-Mental State Examination, and Nutritional Assessment scores in the control and experimental groups did not present significant differences. Both groups of participants, control and experimental, differed significantly in the incidence of diabetes (p-value = .038), which was higher in the control group. Therefore, they were groups with similar characteristics containing patients with the same baseline initial conditions, indicating the random allocation of the patients of the control and experimental groups.
Comparison of the nursing diagnosis in the experimental and control groups
Table 1 shows the distribution of the defining characteristics, related factors, and nursing diagnosis of DSR during the three assessments according to group (experimental or control) and the respective chi-square or Fisher’s exact test results.
Distribution of the defining characteristics, related factors, and nursing diagnosis of DSR during the three assessments (D1, D7, and D30) (n = 95).

DSR: delayed surgical recovery.
χ2 or Fisher’s exact test.
The defining characteristics “postponed resumption of work” and “loss of appetite without nausea” were not identified during the three assessments (n = 0, percentage = 0, p-value = 1.000). The same was true for the related factors of postoperative feelings of fear, insecurity, guilt or loss, hopelessness, decreased self-esteem, and extensive surgical procedure.
Statistical analysis indicated that the DSR diagnosis was present in the second and third evaluations, performed on the 7th and 30th postoperative days, with significant differences between the two groups, as shown in Table 2. The diagnosis was not present in any patient in the control or experimental group at the first evaluation (first postoperative day).
Nursing interventions performed in the telephone follow-up (n = 48).

PO: postoperative.
The OR in the second evaluation was equal to 0.118, with a confidence interval (CI = 1.02, 10.23). Patients who received the telephone follow-up intervention had a significantly reduced chance of presenting DSR. In other words, the chance of a patient who did not receive the telephone intervention receiving a DSR diagnosis was 1/0.118 = 8.5 times greater than the chance of a patient who did receive the telephone follow-up being diagnosed with DSR.
Patients who did not receive the intervention were more likely to have evidence of interrupted healing of the surgical area (OR = 10.8; CI = 2.84, 14.07), discomfort (OR = 7.0; CI = 2.79, 18.53), pain (OR = 6.4; CI = 2.04, 9.89), postoperative feelings of anxiety (OR = 38.5; CI = 27.5, 56.03), worry (OR = 8.2; CI = 3.14, 9.81), and postoperative infection at the surgical site (OR = 6.2; CI = 2.03, 7.80).
Thus, telephone monitoring has a protective effect against the feeling of anxiety, that is, a patient who did not receive telephone follow-up was 38.5 times more likely to feel anxiety than a patient who did. Therefore, association tests and OR analysis indicate that telephone follow-up patients have a reduced risk for DSR.
The nursing interventions implemented in the experimental group through the telephone follow-up were performed with higher frequency, with reduction at the end of the intervention: discomfort management, use of eyecup, care in the cleaning of the operated eye, care in the use of eye drops, use of sunglasses, and guidance on self-care (Table 2).
The first call lasted an average of approximately 18.1 min, the second and third lasted an average of 13.7 min, and the fourth lasted an average of 13.3 min. The coefficients of variation (CV) show that the duration of the telephone calls varied more in the second and third calls. The Friedman test shows that the durations of the calls were significantly statistically different (p-value = 0.000). The Wilcoxon’s test comparisons reveal no significant difference between the second, third and fourth call durations. However, the first call was significantly different from the others, presenting a longer duration.
Discussion
The effect of the telephone follow-up intervention, performed by the nurse, produced a significant difference in the surgical recovery of the patients in the experimental group compared with the patients in the conventional treatment. The control group presented a higher occurrence of DSR, with 8.5 times greater odds of presenting complications (OR = 0.118; CI = 1.02, 10.23) in the second evaluation (performed on the seventh postoperative day). This finding indicates that telephone monitoring can strongly protect against DSR.
The DSR diagnosis was significantly present on the seventh postoperative day in the control group. At this point, patients are expected to present full recovery, since the estimated time for surgical recovery and return to work in the case of cataract surgery is from 3 to 7 days (Rothrock, 2014). Therefore, a delay in surgical recovery occurs when, by the seventh postoperative day, the patient still presents any type of complication and needs to extend the postoperative care.
The very definition of the DSR diagnosis corroborates this idea, as it refers to the “extension of the number of postoperative days” necessary to initiate and perform activities that maintain life, health and well-being (Herdman & Kamitsuru, 2018).
Researchers conducted a study in which they observed that the mean time to onset of symptoms of postoperative complications was 6 days (when assessed from 1 to 30 days) for cataract surgery (Coelho, Souza, & Tanure, 2015). Other authors stated that the estimated time for postoperative complications after cataract surgery is typically up to 3 days after the surgical procedure (Hayashi, Sasaki, Manabe, & Hirata, 2018; Luz, Cvintal, Silva, & Padoveze, 2018; Nizamani, Bhutto, & Talpur, 2013) and may occur until the 30th day after (Cetinkaya, Cetinkaya, Dadaci, & Acir, 2016; Mattos, Saraiva, Angotti-Neto, & Passos, 2013; Råen, Sandvik, & Drolsum, 2013; Toyama, Ueta, Yoshitani, Sakata, & Numaga, 2018). This fact corroborates this study, since, at the third evaluation performed on the 30th postoperative day, the DSR diagnosis decreased.
Therefore, nurses should provide guidance in the initial days after surgery to older persons and their families to prevent or reduce the chances of complications in the first week. The importance of providing guidelines from the preoperative period until the fourth postoperative day, when there is a greater frequency of complications, is reinforced, allowing full surgical recovery until the seventh day.
In this sense, the importance of telephone monitoring for the early identification of complications and for adherence to guidelines regarding home care of the operated eye stands out. Such home care includes cleaning with a clean compress moistened with 0.9% saline solution; cleaning, with the eye closed, in a single from the inner corner to the outer corner; application of eye drops only after cleaning the eye; washing hands before using eye drops; avoiding activities that may increase intraocular pressure, such as carrying weight, performing excessive exercise, or bowing; and following instructions on the application of eye drops, as well as reviewing medication name, dosage, and timing. In addition, the patient and his or her family also need instructions to observe and report symptoms such as redness, discharge, watering, edema, blurred vision, sudden onset pain, decreased visual acuity, and severe headache, which may indicate an increase in intraocular pressure (Cunha et al., 2014; Domingues et al., 2016; Rothrock, 2014).
Furthermore, providing guidelines and clarifying doubts in the postoperative period reduce anxiety, increase the professional-patient bond, and increase the satisfaction of those who receive care (Cunha et al., 2014; Jost et al., 2018). At each visit, the participants were more confident in their home care and, therefore, less anxious and worried. Anxiety, stress, and fear release catecholamines, which can lead to increased cortisol and consequent muscle and protein exhaustion, prolonging the healing time of the surgical wound (Jomar et al., 2017). This study highlights the protective effect of telephone monitoring on the anxiety that the lack of information in the postoperative period can generate in the patient and family, and such feelings of anxiety and worry can be diminished through the educational process (Cunha et al., 2014).
If used properly, technologies can contribute to streamlining and improving the nursing communication process, helping patients to achieve better results as safely as possible and improving support for nurses in patient care. Therefore, technologies incorporated into clinical practice are important tools, provided they are integrated into human care.
As a limitation of the study, the fact that the facectomy is a small, clean, short-term, and fast recovery surgery stands out. This may have contributed to reduce the identification of the presence of some defining characteristics and related factors over the follow-up weeks. In addition, because the patients were elderly and the majority probably retired, there may have been a difficulty in identifying the outcome, postponing return to work.
Conclusion
The telephone follow-up intervention proved to be significant for the surgical recovery of the experimental group compared with the control group, especially in the second evaluation, when the occurrence of DSR was significantly higher in the control group than in the experimental group. This fact leads to the conclusion that patients followed up by telephone after cataract surgery have a reduced risk for DSR diagnosis.
The telephone follow-up performed by the nurse for patients in the postoperative period of cataract surgery can be an efficient strategy for postoperative follow-up and prevention of complications. For older persons, guidelines delivered by telephone are able to increase adherence to treatment, promote clinical improvements and surgical recovery in the shortest possible time, and improve independence and autonomy.
Recommendations
It is recommended to use telephone follow-up in the postoperative period of cataract surgery to avoid complications. The technologies incorporated in the clinical health practice are important, integrated to human care in its multiple dimensions and specificities.
Footnotes
Author contributions
T.M.D.M., R.F.S., and C.T.B.d.S. made substantial contributions to the concept and design, acquisition of the data, or analysis and interpretation of the data, and approved the version to be published. P.A.S. drafted the article or revised it critically for important intellectual content. R.D.V. made substantial contributions to the concept and design, acquisition of the data, or analysis and interpretation of the data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research was conducted with financing from the Foundation for Research Support of the State of Rio de Janeiro—FAPERJ (process E26/103.269/2012), and the Institutional Program for Scientific Initiation Scholarships (AGIR/PROPPI/UFF) of the National Council for Scientific and Technological Development (CNPq) (process IT-134354/2014-2015).