
Abstract
The prevalence of low vision is expected to increase at the national and international levels, given the aging population and the association between the prevalence of ocular disease(s) and increasing age. Thus, it is important to establish knowledge of the distribution, adequacy, and quality of available low vision rehabilitation services nationally and internationally. This will in turn help prioritize eyecare plans and initiatives, and thus deliver effective services. This cross-sectional study enumerated and surveyed all local government and information regarding the geographic location of each participating entity, entity affiliation, availability and types of low vision rehabilitation services, types of providers, and referral patterns were determined. The results of the current study showed that only 4% of the entities provided low vision rehabilitation services and most (75%) were located in the central region. Additionally, the majority of the services (95%) were basic optometric rehabilitation services whereas other services were either rarely offered or not offered at all. Overall, the current low vision rehabilitation services in Saudi Arabia are inadequate to meet the increasing prevalence of the low vision population. Thus, careful planning of eyecare services is required to meet this demand.
Introduction
Low vision (LV) is defined as vision loss that is uncorrectable by conventional eyeglasses or contact lenses and interferes with a person’s ability to perform daily tasks (Corn & Koenig, 1996; Orr, 1992). Many agencies, on the other hand, have defined and classified LV based on the amount of remaining vision. For example, the National Eye Institute defines LV as having a best-corrected visual acuity (VA) of 20/50 or poorer in the better-seeing eye (National Eye Institute, 2010). The International Classification of Diseases categorizes LV based on presenting (1) distance VA into mild (worse than 6/12 and equal to or better than 6/18), moderate (worse than 6/18 and equal to or better than 6/60), severe (worse than 6/60 and equal to or better than 3/60), and blindness (worse than 3/60 to no light perception) and (2) near VA as having a VA of N6 (M 0.8) or poorer with existing correction (World Health Organization, 2006).
Globally, it is estimated that there are approximately 237 million people with LV in 2020, and this number is predicted to increase to 588 million by 2050 (Bourne et al., 2017). Locally, it was estimated that there were approximately 850,000 individuals with LV in 2017, accounting for almost half of the population with disability in Saudi Arabia (Saudi General Authority for Statistics, 2017). The prevalence of LV is expected to increase at the national and international levels, given the aging population (Lutz et al., 2008; United Nations, 2015) and the association between the prevalence of ocular disease(s) and increasing age (Akpek & Smith, 2013; Congdon et al., 2004). Thus, LV is a major public health issue and will continue to be so, emphasizing the importance of comprehensive LV rehabilitation.
LV rehabilitation (LVR) aims to maximize an individual’s functional vision and, thus, helps the visually impaired perform activities of daily living, increase their independence, and improve their quality of life. This is achieved through a variety of LVR services (LVRS) such as comprehensive clinical LV evaluation, prescription of optical and non-optical devices, instruction for the use of these devices, loans of prescribed devices, and referral to individuals or agencies that provide other related services. The LV team includes a multidisciplinary group of professionals, such as optometrists, ophthalmologists, occupational therapists, psychologists, orientation and mobility instructors, assistive technology specialists, and vision rehabilitation teachers, depending on the patient’s needs.
Given the dramatic local and global increase in LV prevalence (Bourne et al., 2017; Saudi General Authority for Statistics, 2017) and the essential role that LVR plays in improving visual functions (Leat et al., 1994; Scott et al., 1999; Watson et al., 1997), it is important to establish knowledge of the distribution, adequacy, and quality of available LVRS nationally and internationally. This will, in turn, help prioritize eyecare plans and initiatives, and thus deliver effective services.
Chiang et al. (2011) reported that out of 178 countries, 63 countries had no LVRS (namely, zero coverage), while 39 countries had poor LVRS coverage (⩽ 10%). In addition, while 22 countries had a coverage range between 11% and 50%, only 8 countries had a coverage of >50%, highlighting the lack of LVRS at the global level, which is in line with the findings of previous local studies (Alotaibi, 2006; Alsaqr, 2021; Chiang et al., 2011; Ovenseri-Ogbomo & Alghamdi, 2021). Locally, Alotaibi (2006) found that LVRS was provided in only 4 out of 75 (5%) randomly selected eyecare facilities in Riyadh, whereas Alsaqr (2021) reported that only 22 out of 154 practicing optometrists routinely provided LVRS.
Research conducted to assess LVRS in Saudi Arabia is not only scarce but also has limitations (Alotaibi, 2006; Alsaqr, 2021; Ovenseri-Ogbomo & Alghamdi, 2021). Specifically, Alotaibi, 2006 assessed LVRS in only 1 region (i.e., Riyadh) out of the 13 Saudi regions (Alotaibi, 2006). On the contrary, Alsaqr (2021) surveyed 154 optometrists while Ovenseri-Ogbomo and Alghamdi (2021) surveyed only 49 optometrists out of the 1886 licensed optometrists in Saudi Arabia (Saudi Commission for Health Specialties, n.d.). Thus, given that the prevalence of LV is rapidly increasing owing to an aging population (Bourne et al., 2017; Saudi General Authority for Statistics, 2017) and that the LVRS studies assessed in Saudi Arabia have limitations (i.e., limited coverage of Saudi regions and small sample sizes) (Alotaibi, 2006; Alsaqr, 2021; Ovenseri-Ogbomo and Alghamdi, 2021), this study aimed to determine the extent of provision and type of LVRS in terms of geographic distribution, characteristics of LVRS and providers, and referral patterns across Saudi Arabia. This will, in turn, help prioritize eyecare plans and initiatives, and thus deliver effective services.
Methods
Ethics
Ethical approval was obtained from the Institutional Review Board of King Saud University (Ref. No. 21/01105/IRB) on 14 December 2021. Informed consents were collected from participants in this study. The procedures were conducted in conformity with the Declaration of Helsinki ethical principles.
LVRS survey
The survey used in this study has been previously described (Owsley et al., 2009). In summary, the survey included geographic location of each participating healthcare entity (entity name, city, and region), entity type and affiliation (government [Ministry of Health, Ministry of Defense, Ministry of Education, Ministry of Interior, or National Guard] or private [hospital, ophthalmology practice, or category A optometry practice]), availability of LVRS, types of LVRS (for example, optical aid fitting and dispensing with basic training in device use, eccentric viewing training, and orientation and mobility training), types of LVRS providers (for example, optometrists, ophthalmologists, and occupational therapists), and entity referral patterns.
Study design
An updated list of all government and private healthcare entities was obtained from the investment office and the official website of the Saudi Ministry of Health. Unrelated monodisciplinary healthcare facilities, such as mental health, dental, dermatology, obstetrics, and gynecology, were excluded from the study. In addition, categories B and C optical shops were excluded because they did not provide LVRS. In more detail, Category B optical shops were staffed with a licensed optometrist and allowed to assess vision (i.e., refraction eye exam) and prescribe and dispense spectacles. Category C optical shops, however, were staffed with a licensed optician and only allowed to dispense spectacles.
The survey was cross-sectionally administered either in person by visiting a facility, through phone calls, or via email within a 5-month period beginning January 2022. Along with the survey, the role of different LVR providers (optometrists, ophthalmologists, occupational therapists, vision rehabilitation teachers, social workers, orientation and mobility specialists, and psychologists) was explained. Subsequently, an electronic version of the survey was created using SurveyMonkey, and all responses were electronically entered by two investigators and crosschecked by two different investigators to ensure the accuracy and veracity of data.
Data analysis
Descriptive statistics were used to highlight the extent of provision and type of LVRS in terms of location of the entity, entity type, entity affiliation, availability of LVRS, types of LVRS, types of LVRS providers, and entity referral patterns.
Results
According to the Saudi Ministry of Health, 737 healthcare entities (329 government and 408 private) were enumerated. A total of 115 unrelated monodisciplinary facilities (51 government and 64 private entities) were excluded, whereas 110 facilities did not respond despite repeated contact attempts. Out of the 622 contacted facilities, 512 completed the survey, yielding a response rate of 82%.
Private optometry practices represented approximately half of the surveyed entities (n = 250, 49%), whereas government hospitals affiliated with the Ministry of Health and private hospitals were the next most common types, representing 24% (n = 124) and 14% (n = 72) of surveyed entities, respectively (Figure 1). Most respondents were optometrists (n = 347, 68%) with administrative personnel or receptionists being the next most common respondents (n = 124, 24%). Only 33 ophthalmologists (6%) and 8 nurses (2%) completed the survey on behalf of the entity.

Distribution of entities that completed the survey.
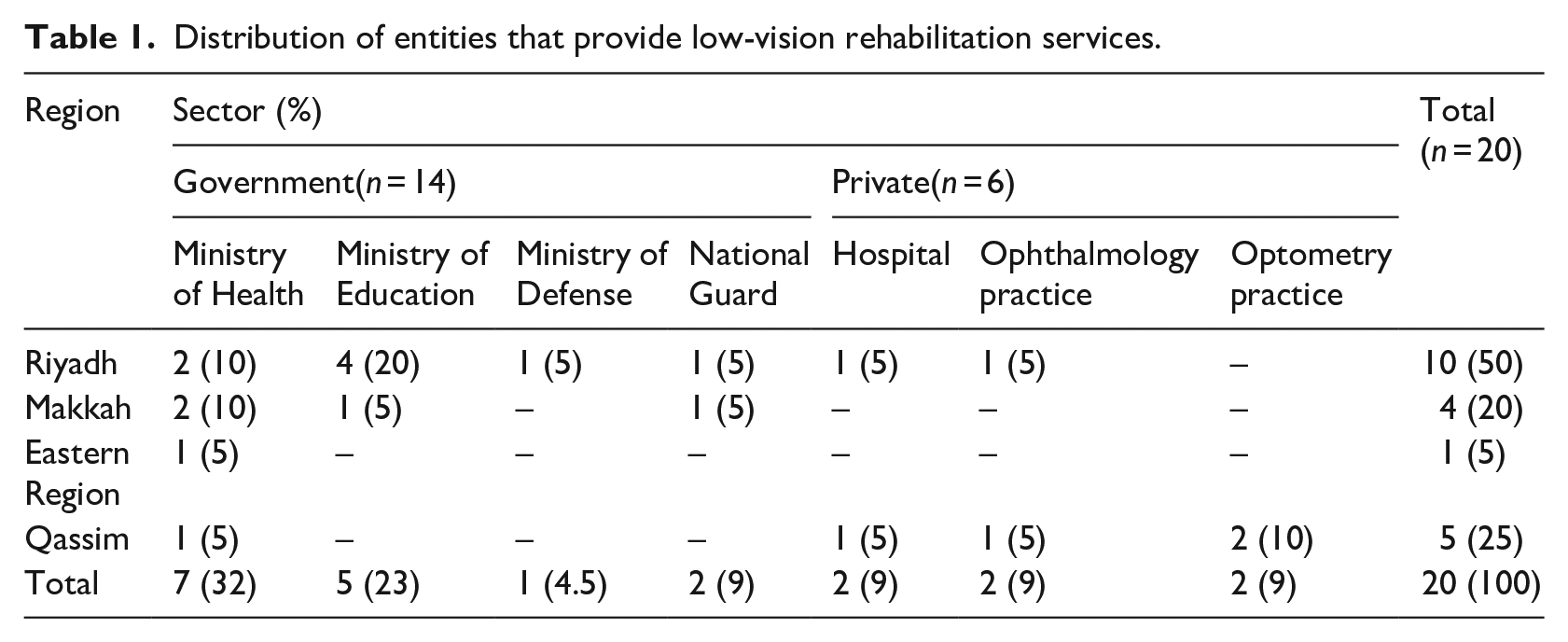
Among the 512 facilities that completed the survey, LVRS was provided in only 20 (4%; Table 1). It is worth mentioning that two additional entities known to provide LVRS were not included because they did not complete the survey despite repeated contact attempts. Of the 20 entities that provided LVRS, 14 (70%) were government entities while 6 (30%) were private entities. LVRS was mostly located in the central region (n = 15, 75%), whereas approximately three-quarters of the 13 Saudi Arabian regions lacked LVRS (Figure 2).
Distribution of entities that provide low-vision rehabilitation services.
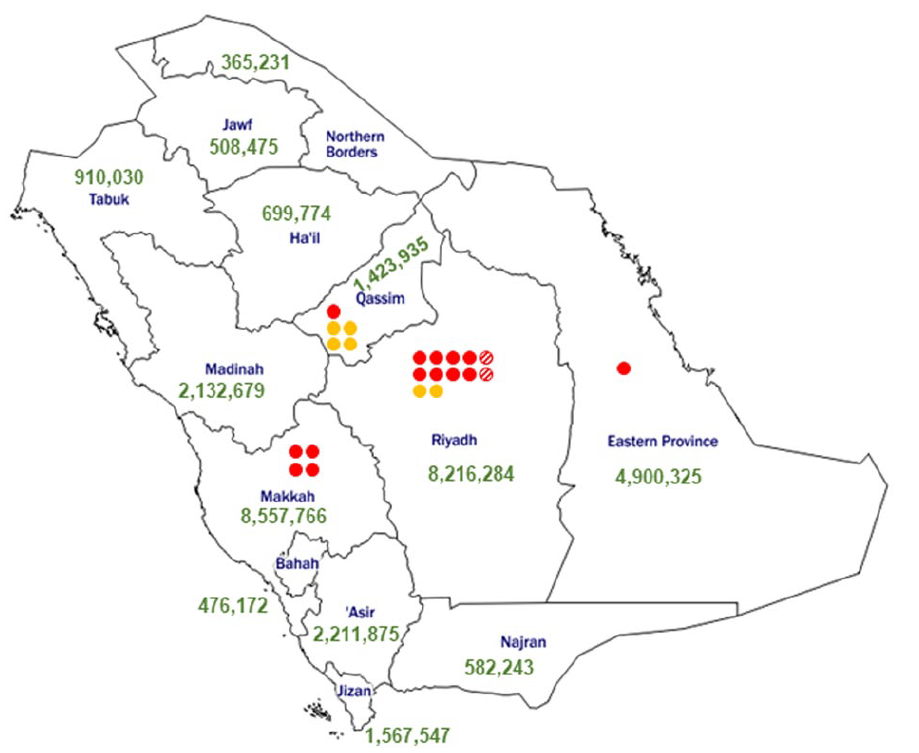
Location of low-vision rehabilitation services across the 13 Saudi regions. Solid red circles indicate government-affiliated entities. Solid orange circles indicate private entities. Circles with diagonal stripes indicate entities that provide LVRS, but did not complete the survey. Numbers in green indicate the total population of each region as per the Saudi General Authority for Statistics. Courtesy of d-maps.com.
Of the 20 respondents who provided LVRS, 11 (55%) completed formal training in LVR, whereas 9 (45%) did not complete any form of training other than the training they received in their academic programs (namely, optometry programs). When asked about the training they completed, 6 of the 11 respondents (55%) indicated that they obtained a higher degree (MSc and/or PhD) in LVR, whereas 5 (45%) stated that they completed intensive LVR workshop(s).
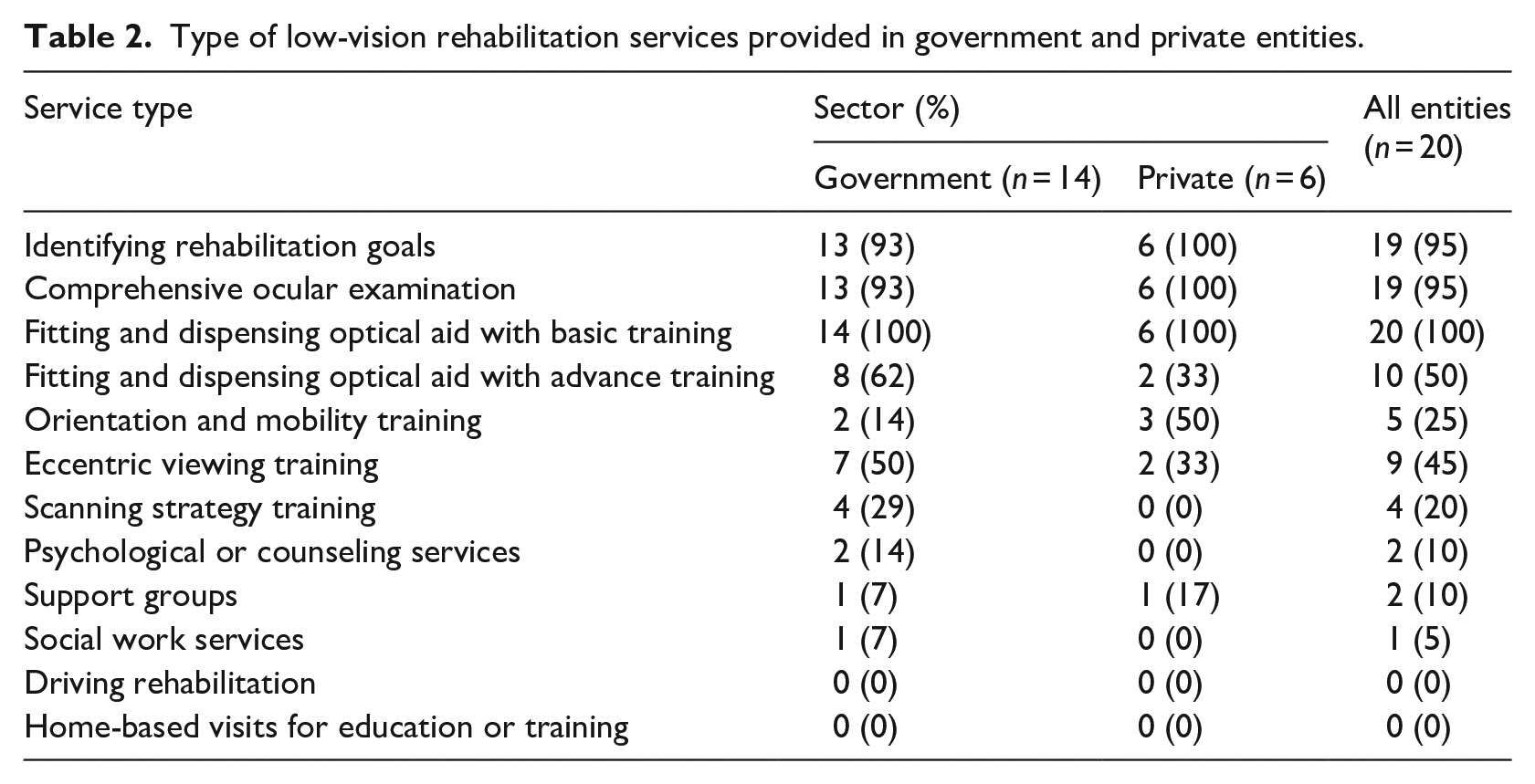
When asked about the type of LVRS provided, almost all respondents indicated that they determined patient’s rehabilitation needs (95%), assessed their visual functions (95%), and fitted or dispensed optical aids with basic training (100%; Table 2). Approximately half of the respondents offered optical aid fitting or dispensing with intensive training in device use and eccentric viewing training (50% and 45%, respectively; Table 2). The aforementioned LVRS was most likely offered by government-affiliated entities. The remaining LVRS were either rarely offered, such as scanning strategy training and support groups (20% and 10%, respectively), or not offered, such as driving rehabilitation (Table 2). If the required LVRS was unavailable, half of the entities (50%) reported that they would refer the patient to another entity.
Type of low-vision rehabilitation services provided in government and private entities.
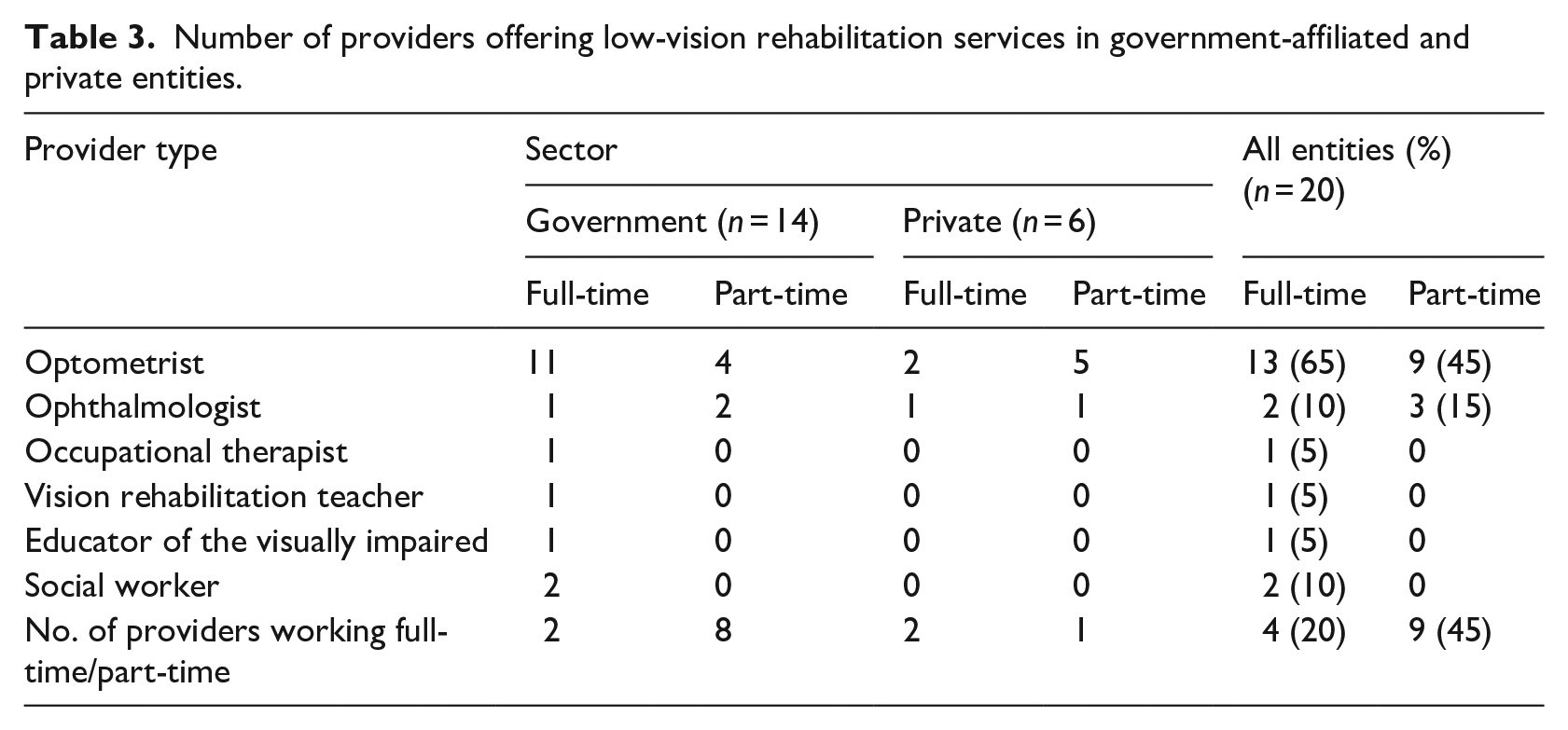
Optometrists had the highest representation rate among the different LVRS professionals working full-time (65%) and part-time (45%; Table 3). Other LVRS professionals (such as ophthalmologists, occupational therapists, vision rehabilitation teachers, educators of the visually impaired, and social workers) had poor representation irrespective of their employment status (full-time vs part-time; Table 3), whereas professional categories such as orientation and mobility specialists and psychologists are not yet available in any of the entities that provide LVRS.
Number of providers offering low-vision rehabilitation services in government-affiliated and private entities.
Decisions on whether a patient needed to be referred for occupational therapy, psychological, or social work services were made by optometrists and ophthalmologists in 20%, 5%, and 5%, respectively, of the entities that provided LVRS. Optometrists were the primary source for referral for occupational therapy, psychological, and social work services in 15%, 10%, and 15% of the entities, respectively. In contrast, ophthalmologists were the primary source for referral for occupational therapy, psychological, and social work services in 10%, 20%, and 10%, respectively, of the entities that provided LVRS.
Figure 3 shows the referral patterns of the other LVRS professionals. Two-thirds of the entities that provide LVRS do not refer to occupational therapy, psychological, or social work services. Optometrists referred to occupational therapy, psychological, and social work services in 25%, 15%, and 20% of the entities, whereas ophthalmologists referred to these services in 20%, 25%, and 15% of the entities that provided LVRS, respectively (Figure 3). It should be noted that referrals to other LVRS (namely, occupation therapy, psychological, and social work services) were all made in government-affiliated entities. None of the private entities that provided LVRS indicated that they had referred to other LVRS professionals.
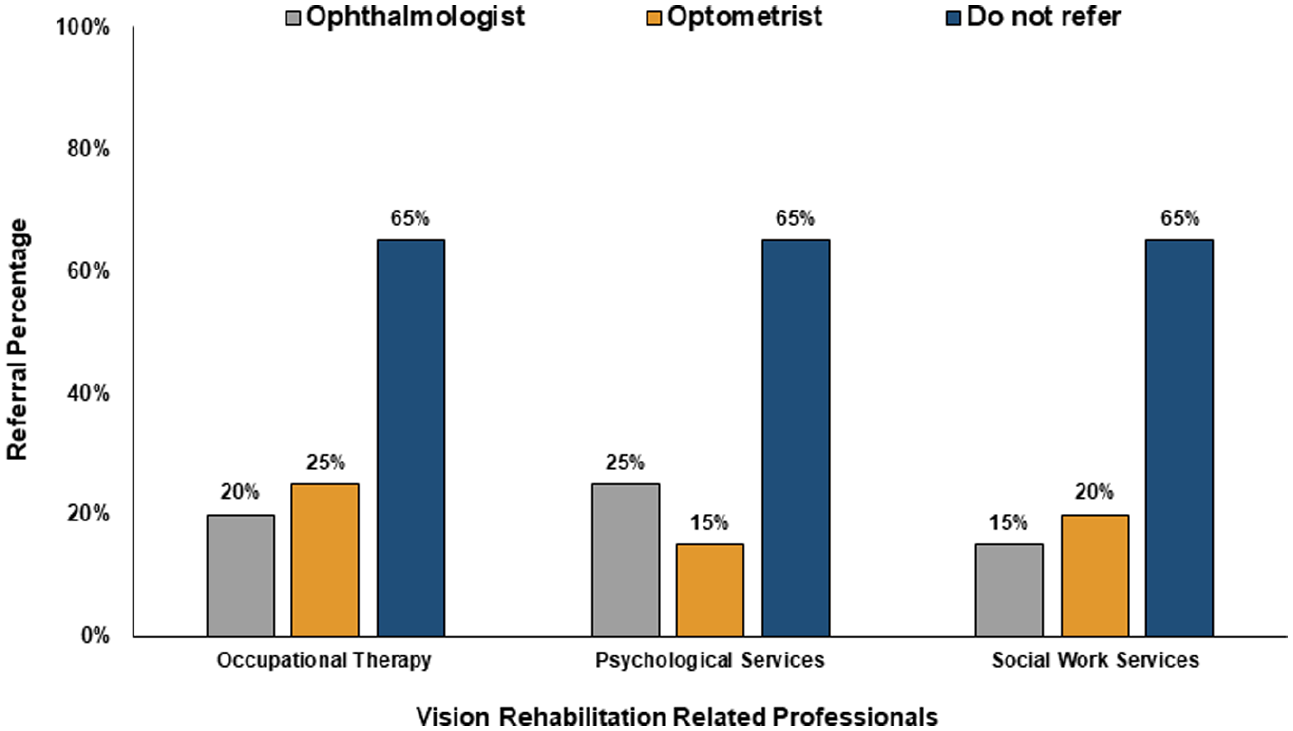
Proportion of optometrists and ophthalmologists referring to other vision rehabilitation professionals.
Only 35% of the participants indicated that LVRS professionals conducted care team meetings for patients with LV. These were all government-affiliated entities, since none of the private entities that provided LVRS indicated that they had held care team meetings. In addition, in two-thirds of the entities, patients with LV first interacted with an ophthalmologist, whereas in 35% of the entities that provided LVRS, they were most likely to interact with an optometrist.
The lead time for LVRS appointment was less than 1 week in 45% of the entities, whereas 30% and 20% of the entities reported that it took 1–2 and 3–4 weeks, respectively, to schedule a patient for LVRS. In addition, over half of the entities (55%) reported that a patient was seen within 15 min of arrival, whereas 35% of the entities indicated that a patient was seen within 30 min of arrival.
Discussion
The primary aim of this study was to document the provision and type of LVRS in Saudi Arabia. The results of this study indicate that local LVRS is not only inadequate to meet the growing number of individuals with LV (Bourne et al., 2017; Saudi General Authority for Statistics, 2017), but is also unevenly distributed across the country. This is because LVRS is provided in only 4% of local government and private healthcare entities, and 75% of LVRS entities are only located in the central region (Figure 2).
The finding that LVRS is provided in only 20 local entities (plus two entities that did not complete the survey) agrees with the results of Alsaqr (2021) and Ovenseri-Ogbomo and Alghamdi (2021) who reported that 22 and 24 optometrists routinely provide LVRS. In addition, in line with the findings of previous studies (Alsaqr, 2021; Ovenseri-Ogbomo and Alghamdi, 2021), the majority of these LVRS are provided by government-affiliated entities, although private entities represented 67% of all surveyed entities.
The results of this study revealed that LVRS entities are more likely to be available in highly populated regions. Indeed, all entities that provide LVRS (100%) are located in four regions (Riyadh, Makkah, Eastern Province, and Qassim, with a total population of approximately 23 million), whereas the remaining nine regions (with a total population of approximately 9.5 million) are underserved. This higher likelihood of LVRS in metropolitan areas than others is consistent with the findings of previous local and global studies (Alsaqr, 2021; Carlson & Hinkley, 2011; Chiang et al., 2011; Ovenseri-Ogbomo & Alghamdi, 2021; Owsley et al., 2009; www.d-maps.com, n.d.).
LV rehabilitation integrates various services and professionals that aim to assess and mitigate the impact of vision loss on an individual’s ability to perform activities of daily living. The results of this study suggest that LVRS is mainly an optometric rehabilitation service, whereas other services are less common. This most likely occurred because most LVRS providers were optometrists, whereas other professionals had either poor or no representation (Table 3).
This study showed that LVRS focused more on ocular examination and fitting and dispensing optical aids, whereas LVRS is a holistic approach to support patients with LV. Thus, other LVRS, such as eccentric viewing, scanning strategy, orientation and mobility, and driving rehabilitation, must be available in addition to referral to other professionals in the LVR team.
Our findings showed that most patients with LV first interacted with an ophthalmologist, a primary source of referral to LVRS, which might pose a challenge to LVRS accessibility. This is mainly because of the long lead time for an ophthalmology appointment, which significantly increases the no-show rates (Chiam et al., 2021; Culham et al., 2002; Mäntyjärvi, 1994). Indeed, the lead time for an ophthalmology outpatient appointment has been shown to be as long as 3 months (Culham et al., 2002; McMullen & Netland, 2015). On the contrary, this study reported that most optometric LVRS appointments were scheduled within 1–2 weeks and that patients were seen within 30 min of arrival, which makes the LVRS easily accessible.
A limitation of this study was that respondents who indicated providing LVRS (namely optometrists) might have overestimated or underestimated the extent of LVRS. In addition, 26% of respondents were administrative personnel, receptionists, or nurses. Thus, these respondents might have inadvertently indicated that an entity did not provide LVRS while it did. However, this is most likely improbable because the roles of the different LVR professionals were explained to the respondents.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors extend their appreciation to the Deanship of Scientific Research at King Saud University for funding this work through Research Group no RG-1441-403.