
Abstract
Individuals living with HIV experience higher rates of stigmatizing social interactions that may negatively impact psychological and physical health. We examined depressive symptoms as a mediator of the relationship between HIV-specific unsupportive social interactions (USIs) and health behaviors in 87 Black and White men living with HIV (MLWH). We also examined ethnicity as a moderator of this model. Depressive symptoms were an indirect mechanism through which HIV-specific USIs explained poorer health behaviors. The indirect effects between disconnecting USI, more depressive symptoms, and poorer health behaviors were significant for Black men but not for White men. Depressive symptoms may be one pathway through which USI are associated with physical health, and disconnecting USI may be particularly detrimental for Black MLWH.
The benefits of social relationships for physical and psychological health in individuals with HIV are well documented (Cohen, 2004; Uchino, 2013). Less research attention, however, focuses on the links between HIV-specific unsupportive social interactions (USIs), psychological well-being, and physical health in people living with HIV. People living with HIV who experience more negative or stigmatizing interactions regarding their illness may experience higher levels of stress and distress (Hutton, Misajon, & Collins, 2013; Song & Ingram, 2002), which in turn may be associated with poorer physical health, including health behaviors (Bekele et al., 2013). Therefore, the primary aims of the current study are to (1) examine the relationship between HIV-specific USIs and both depressive symptoms and health behaviors in a sample of men living with HIV (MLWH) and (2) examine depressive symptoms as a mediator of the relationship between HIV-specific USIs and health behaviors in MLWH. This work is grounded in the findings that health disparities in HIV-related health and well-being may be explained by the minority stress model, evidencing that individuals from ethnic minority populations have higher levels of stress and stigmatizing interactions and lower levels of personal and social resources to cope with stress (Clark, Anderson, Clark, & Williams, 1999; Williams, Neighbors, & Jackson, 2003). Thus, a third aim of the study examined whether ethnicity (Black vs. White) moderated the associations among HIV-specific USIs, depressive symptoms, and health behaviors in MLWH.
People living with HIV with more supportive social relationships report lower levels of psychological distress and a better quality of life (Gordillo et al., 2009; Jia et al., 2005). Positive social interactions such as emotional support or encouragement to engage in a healthy lifestyle are also associated with increased health behaviors and slower disease progression (Deichert, Fekete, Boarts, Druley, & Delahanty, 2008; Leserman et al., 2002; Simoni, Frick, & Huang, 2006). Further, individuals who are more satisfied with the social support they receive report fewer HIV-related symptoms over time (Ashton et al., 2005).
While social relationships can be a positive factor in health promotion for persons living with HIV, a growing body of research demonstrates that some types of social interactions have deleterious effects on psychological health (Hutton et al., 2013; Ingram, Jones, Fass, Neidig, & Song, 1999; Song & Ingram, 2002). Although social network members often have benevolent intentions when providing support to individuals with HIV, they may also harbor negative feelings and attitudes toward individuals with HIV due to the stigma associated with HIV or because of a lack of knowledge or fear about the illness (Ingram et al., 1999; Song & Ingram, 2002). As a result, social network members may express these negative feelings through negative behaviors that are perceived as unsupportive or stigmatizing by individuals living with HIV (Song & Ingram, 2002). In some cases, these negative or USIs may have a stronger impact on health than positive interactions (Rook, 1984).
Such perceived HIV-specific USIs might include behaviors like blaming (expressions of disapproval or fault), disconnecting (disengagement or refusals to provide support), or being insensitive (expressing discomfort or a lack of empathy) toward someone because of their HIV diagnosis (Ingram, Betz, Mindes, Schmitt, & Smith, 2001). These interactions may be considered a form of “felt stigma” or shame felt by individuals because of their illness and are associated with poorer subjective well-being in people living with HIV (Hutton et al., 2013). Particularly when coupled with low levels of HIV-related social support, negative social interactions from social network members are associated with higher levels of depression (Siegel, Raveis, & Karus, 1997). Moreover, even after accounting for the beneficial effects of social support or positive social interactions, HIV-specific unsupportive interactions are consistently linked to heightened levels of depressive symptoms in PLWH (Ingram et al., 1999; Song & Ingram, 2002).
The majority of research on HIV-specific USIs focuses on the negative impact that these types of interactions have on the psychological health of individuals with HIV. Less research examines how HIV-specific USIs may be associated with health behaviors in MLWH. However, just as supportive social interactions are associated with positive physical health outcomes in individuals living with HIV (e.g., Deichert et al., 2008; Leserman et al., 2002; Simoni et al., 2006), it is possible that negative social interactions can impact the physical health, including health behaviors, of individuals living with HIV. Given the importance of positive health behaviors for the progression of illness among those with HIV (Collins et al., 2001), understanding the role that negative social interactions play for health behaviors may be important for promoting good health and keeping illness symptoms at bay among MLWH.
Research with nonchronically ill adults suggests that social conflict and deficits in social support are associated with decreases in health behaviors, which in turn may be associated with poorer physical health status (Cohen, 2004; Kiecolt-Glaser, Gouin, & Hantsoo, 2010). In a sample of HIV-negative college students, USIs were associated with greater amounts of physical illness symptoms (Ingram et al., 2001). While we could find no specific research linking HIV-specific unsupportive interactions to physical health or health behaviors, a recent meta-analysis found that higher levels of HIV-related stigma, which includes stigmatizing social interactions, are associated with poorer physical health (Logie & Gadalla, 2009). Thus, it is plausible that experiencing blaming, disconnecting, and insensitive interactions may also have adverse effects on health behaviors in MLWH.
Not only may USIs contribute to poorer psychological health and health behaviors of MLWH, it may be that poorer psychological health helps to explain the relationships between HIV-specific unsupportive interactions and health behavior. Indeed, prior literature has evidenced that social interactions may exert their influence on physical health, including health behaviors, through various psychological health factors (Bekele et al., 2013; Deichert et al., 2008; Gonzalez et al., 2004). In men and women living with HIV, depressive symptoms explain the relationship between perceptions of social support and health-related quality of life (Bekele et al., 2013). Similarly, in our prior research, MLWH who received more emotional support from a primary social network member had fewer depressive symptoms, which in turn was associated with a healthier lifestyle (Deichert et al., 2008). However, we did not examine whether negative social interactions, especially illness-specific unsupportive interactions, were associated with depressive symptoms and, in turn, health behaviors.
In addition to the lack of research examining associations between HIV-specific USIs and physical health, the role of ethnicity in the associations between USIs, psychological well-being, and health has not been thoroughly explored. Examining ethnic differences in the impact of USIs on psychological well-being and health behaviors may be important given that compared to non-Hispanic Whites (Whites), Blacks are diagnosed with HIV/AIDS 10 times more frequently, experience faster disease progression, and have a higher mortality rate from HIV (Hall, Byers, Ling, & Espinoza, 2007). Importantly, the minority stress model has provided some explanation for the health disparities observed between Whites and Blacks living with HIV. Specifically, the model suggests that individuals belonging to ethnic minority groups may experience more socioeconomic hardships, have fewer social resources, and experience added stress and marginalization as a result of racism or discrimination (Meyer, 2003; Williams et al., 2003).
In this way, MLWH who are also ethnic minorities may be at increased risk for the negative impact of USIs. That is, minorities’ greater risk for discrimination, socioeconomic strain, and other stress due to their minority status may create an increased vulnerability due to decreased coping resources. Indeed, research outside of the context of HIV provides consistent evidence that racism encountered by minority groups, such as Blacks in the US, is related to decreased health status and serves as some explanation for disparities in health (Williams, 1999). Moreover, racism may become internalized such that Black’s may endorse society’s negative view of their racial group and further explain negative health outcomes (Williams, 1999). Additionally, research focused on stigma and internalized stigma in relation to poverty and violence is linked to unsupportive responses from one’s support network and negative outcomes (Mickelson & Williams, 2008; Williams & Mickelson, 2008). Thus, ethnic minority men with HIV may experience multiple or “layered” stigma, in that HIV-related stigma may be exacerbated in individuals facing other stigmatized characteristics.
Stigma research in the context of HIV specifically among African American men, although limited, links stigma with physical health symptoms. Specifically, Buseh, Kelber, Stevens, & Park (2008) found that perceived stigma was related to increased intensity in the physical symptoms of HIV, underscoring the potential harmful associations between stigma and symptoms of infection. However, comparisons of stigma levels between Blacks and Whites living with HIV have been limited to work, suggesting that the type of stigma experienced may be different by ethnicity or culture. African Americans were more likely to encounter public or enacted stigma where others actually discriminated against them for having HIV, whereas Whites reported more self- or internalized stigma of holding HIV by way of wanting to keep their status a secret and a fear of rejection from others (Rao, Pryor, Gaddist, & Mayer, 2008).
Thus, it may be that there are ethnic differences in the strength of the association between HIV-specific USIs and psychological and physical health, particularly when those types of interactions are perceived as being stigmatizing. However, a paucity of research examines the links between ethnicity and HIV-specific USIs. Importantly, Song and Ingram (2002) did find that disconnecting social interactions (e.g., behavioral or emotional disengagement, refusals to provide support) were associated with greater mood disturbance in a sample of Black men and women with HIV. To our knowledge, however, no study directly examines how ethnic differences in HIV-specific USIs are associated with depressive symptoms and health behaviors.
The present study
The primary aims of the present study were to examine the associations between HIV-specific USIs, psychological well-being, and health behaviors in a sample of Black and White MLWH. Our first hypothesis predicted that higher levels of HIV-specific USIs would be associated with higher levels of depressive symptoms and poorer health behaviors in MLWH. Our second hypothesis included that depressive symptoms would serve as a mediator of the relationship between HIV-specific USIs and health behaviors in MLWH. Specifically, we predicted that higher levels of insensitive, disconnecting, and blaming social interactions would be associated with increased depressive symptoms, which in turn would be associated with poorer health behaviors. A third aim of our study was to examine ethnicity as a moderator of the indirect associations between HIV-specific USIs, depressive symptoms, and health behaviors in MLWH. Based on the minority stress model, we expected that the negative impact of insensitive, disconnecting, and blaming interactions on depressive symptoms and health behaviors would be stronger in Black MLWH than in White MLWH.
Method
Participants and procedures
Data for this study were part of a larger study examining the effects of social interactions on physical and psychological health in MLWH who lived in a large urban metropolitan city in the Midwestern US. The current study included 87 men (48 Black and 39 White) over the age of 18, who were diagnosed with HIV/AIDS. All methods were reviewed and approved by the institutional review board of the University through which the study was conducted. Participants were referred to study investigators through local social service agencies. Men completed a questionnaire anonymously and were compensated US$5 upon completion.
Measures
HIV-Specific USIs
The USI Inventory (USII; Ingram et al., 2001, 1999) assessed HIV-specific unsupportive interactions in MLWH. This measure is designed to assess stressor-specific unsupportive interactions and has been adapted to examine HIV-specific unsupportive interactions (Ingram et al., 1999). For the current study, we utilized three of the four individual subscales measuring blaming, disconnecting, and insensitive interactions rather than a total scale score. Participants were asked, “in the past two months, how often did you experience the following as a result of your HIV/AIDS?” Examples of items on the blaming subscale included “blamed me or tried to make me feel responsible for having HIV/AIDS,” and “told me I had gotten myself into the situation in the first place, and now must deal with the consequences.” Examples of items on the disconnecting subscale included, “they didn’t seem to want to hear about it,” and “they changed the subject about my HIV/AIDS before I wanted to.” Examples of items on the insensitive subscale included “someone acted cold, aloof, or nasty toward me because of my HIV/AIDS” and “from voice tone, expression or body language, I got the feeling he or she was uncomfortable talking about my HIV/AIDS.” We did not use the forced optimism subscale that measures the extent to which others tried to force a positive focus on the participant, because prior research suggests that this subscale is more susceptible to individual interpretation than the other three subscales (Ingram et al., 1999; Song & Ingram, 2002). Moreover, we chose to examine each type of unsupportive interaction separately rather than creating a summed total-scale score because while strongly correlated, each type of interaction has been shown to have distinct theoretical and predictive characteristics (e.g., Ingram et al., 2001).
Men rated the extent to which they experienced 18 different HIV-specific unsupportive interactions over the last 2 months on a scale from 1 (rarely or none of the time) to 4 (most or all of the time). The mean scores for each domain revealed an average score toward the lower end of the subscale, although a broad range of scores was observed across blaming interactions (M = 8.69, SD = 4.2; potential range = 6–24; observed range = 6–24), disconnecting interactions (M = 9.04, SD = 4.0; potential range = 6–24; observed range = 6–24), and insensitive interactions (M = 10.70, SD = 4.2; potential range = 6–24; observed range = 6–22). Consistent with prior research (e.g., Ingram et al., 1999), the three subscales were strongly correlated (insensitive and disconnecting r = .77, p < .001; insensitive and blaming r = .74, p < .001; and disconnecting and blaming r = .89, p < .001), and each subscale showed high internal consistency (α = .92 for blaming, α = .87 for disconnecting, and α = .81 for insensitive).
Depressive symptoms
Depressive symptoms were measured with the Center for Epidemiologic Studies–Depression scale (CES-D; Radloff, 1977). The CES-D is a widely used 20-item scale that assesses levels of depressive symptoms during the past week, with a score of 17 or above set as an indicator of risk for clinical depression in chronic illness populations (Katz, Kopek, Waldron, Devins, & Tomlinson, 2004). Men’s mean CES-D score was 20.52 (SD = 13.2; potential range = 0–60; observed range = 1–58; α =.93), and 54.0% of men in our study were at risk for clinical depression (i.e. CES-D scores of 17 or above).
Health behaviors
Men reported how often they engaged in 11 different health behaviors to stay healthy in the past 2 months. These behaviors included eating right, avoiding drugs and alcohol, not smoking, getting plenty of sleep, practicing safe sex, taking prescribed medications, attending medical appointments, practicing relaxation techniques, avoiding stress, exercising, and staying informed about their HIV. Items for this scale were created for the purpose of this study to examine the extent to which MLWH engaged in a variety of health behaviors known to be associated with medication adherence and disease status (Collins et al., 2001). The General Health Behaviors measure developed by the Adult AIDS Clinical Trials Group (AACTG) was used as a guide in creating this measure (Chesney et al., 2000). Men rated how often they engaged in each health behavior on a scale from 0 (never) to 3 (all of the time), with higher scores representing a generally healthier lifestyle. The mean number of health behaviors that men reported engaging in was 9.41 (SD = 1.5; potential range = 0–11; observed range = 4–11). The mean frequency of engaging in these health behaviors was 20.66 (SD = 5.9; potential range = 0–33; observed range = 7–32; α =.72). In the present study, the frequency with which men engaged in health behaviors, rather than the count of how many health behaviors they engaged in, was used in all analyses.
Ethnicity
Men self-identified their race/ethnicity as either Black or White. Ethnicity refers to groups who share a common history, language or communication system, values and beliefs, normative beliefs and customs, and a common country of origin (Brislin, 1993). An individual’s race is part of their ethnicity and refers to group membership based on physical features such as skin color, hair type, and facial features (Kaplan & Bennett, 2003). For the purposes of our analyses, we used self-identified race as a proxy for ethnicity. White MLWH were coded as 0 and Black MLWH were coded as 1.
Covariates
For our first and second hypotheses, covariates included any sociodemographic, social, or health characteristics that were correlated with the dependent variables. Potential covariates included age, education, income, years with HIV, HIV symptoms, sexual orientation, relationship status. Income and HIV symptoms emerged as covariates for the models examining depressive symptoms as an outcome (r = −.21, p < .05 for income and r = .33, p < .01 for HIV symptoms) and HIV symptoms emerged as a covariate for the models examining health behaviors as an outcome (r = −.28, p < .01). For our third hypothesis, we utilized chi-square analysis and t-tests to examine ethnic differences in sociodemographic, social, and health characteristics. Sexual orientation, χ 2(4, n = 87) = 9.7, p < .05, and relationship status, χ 2(3, n = 87) = 13.8, p < .05, emerged as additional covariates for these analyses (Table 1).
Ethnic differences in men’s sociodemographic, social, and health characteristics.
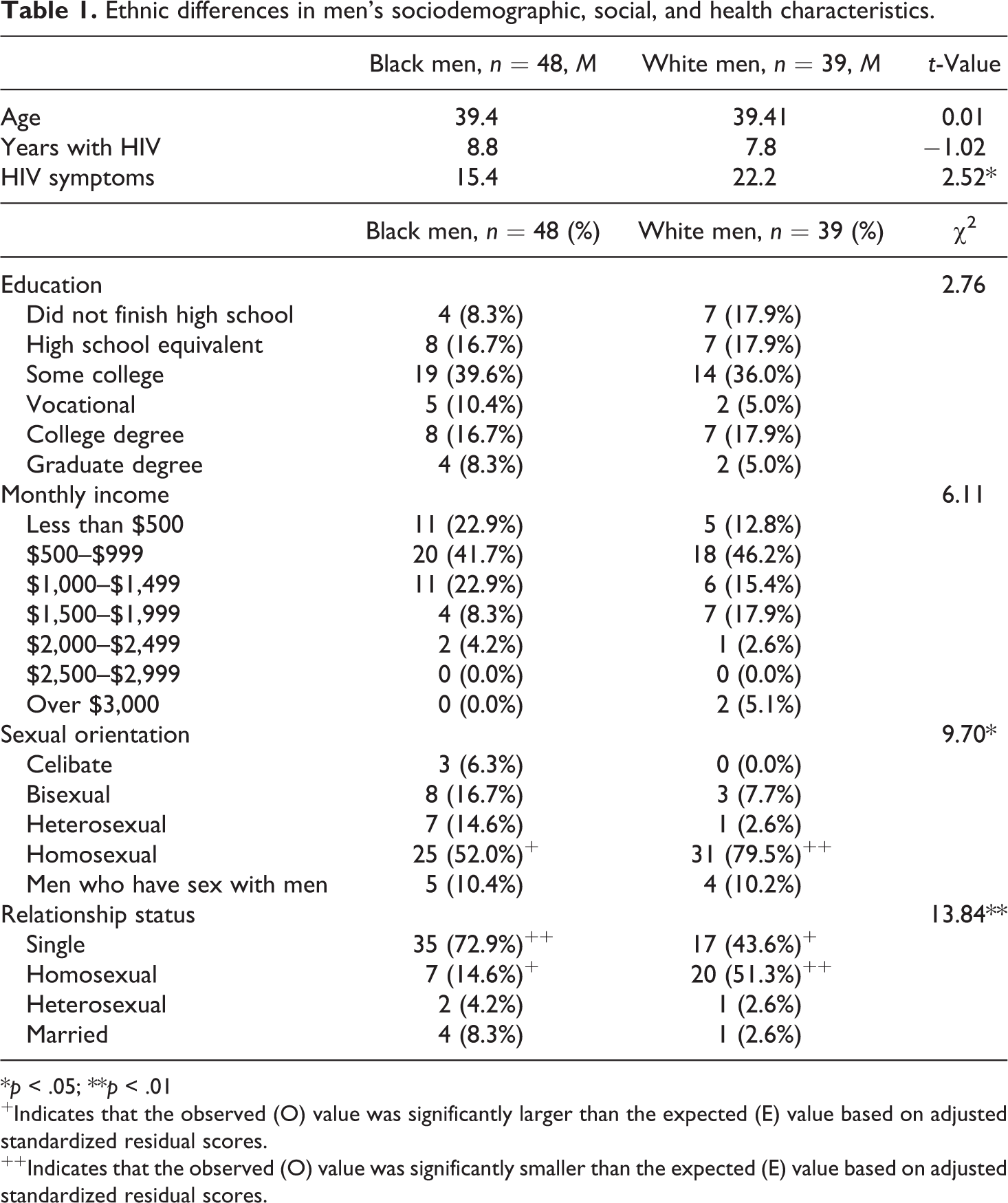
*p < .05; **p < .01
+Indicates that the observed (O) value was significantly larger than the expected (E) value based on adjusted standardized residual scores.
++Indicates that the observed (O) value was significantly smaller than the expected (E) value based on adjusted standardized residual scores.
Analysis plan
To examine our first hypothesis that higher levels of HIV-specific USIs would be associated with greater levels of depressive symptoms and poorer health behaviors, we used hierarchical multiple regression analyses. Covariates were entered into the first block of the model, followed by men’s reports of their insensitive, disconnecting, or blaming interactions. To examine our second hypothesis that depressive symptoms would mediate the relationship between USIs and health, we conducted mediation analyses using guidelines recommended by Preacher, Rucker, and Hayes (2007). Bootstrap procedures were used to estimate indirect effects and confidence intervals. The bootstrap method is more appropriate to use than traditional tests of indirect effects (e.g., Sobel) when sample sizes are small to moderate because it provides a more precise estimate of indirect effects (MacKinnon, Lockwood, & Williams, 2004). To examine our third hypothesis that ethnicity would moderate the relationship between HIV-specific USIs and depressive symptoms and health behaviors, we conducted moderated mediation analyses using an SPSS program designed by Preacher and colleagues (2007). This analysis examined the conditional indirect effects of HIV-specific USIs on health behaviors through depressive symptoms. We predicted that ethnicity would moderate both the relationship between the predictor and mediator variable and between the mediator and outcome variable.
Results
Sample characteristics
Men were on average 39.4 years of age (SD = 7.0; range 24–60), and almost three quarters (71.1%) had at least some college or vocational education. Most participants were not currently employed (62.2%) and had an average monthly income of less than US$1,000. Many men reported that they received financial assistance such as state or city welfare (6.7%), food stamps (20.0%), social security or disability (53.3%), or financial support from partners or family members (7.8%). The average number of years men had been HIV positive was 8.2 (SD = 4.7; range = <1 year–19 years), and the most commonly reported illness symptoms were low energy/fatigue (78.9%), diarrhea (66.7%), headache (65.6%), cough (61.1%), and night sweats (60.0%). The majority of the sample (63.3%) identified their sexual orientation as homosexual, with a smaller proportion identifying themselves as bisexual (13.3%), men who have sex with men (MSM; 11.1%), heterosexual (8.9%), or celibate (3.3%). Over half of the men in our study reported that they were not currently in a relationship (61.1%) and the rest reported they were either in a committed relationship (33.3%) or married (5.6%).
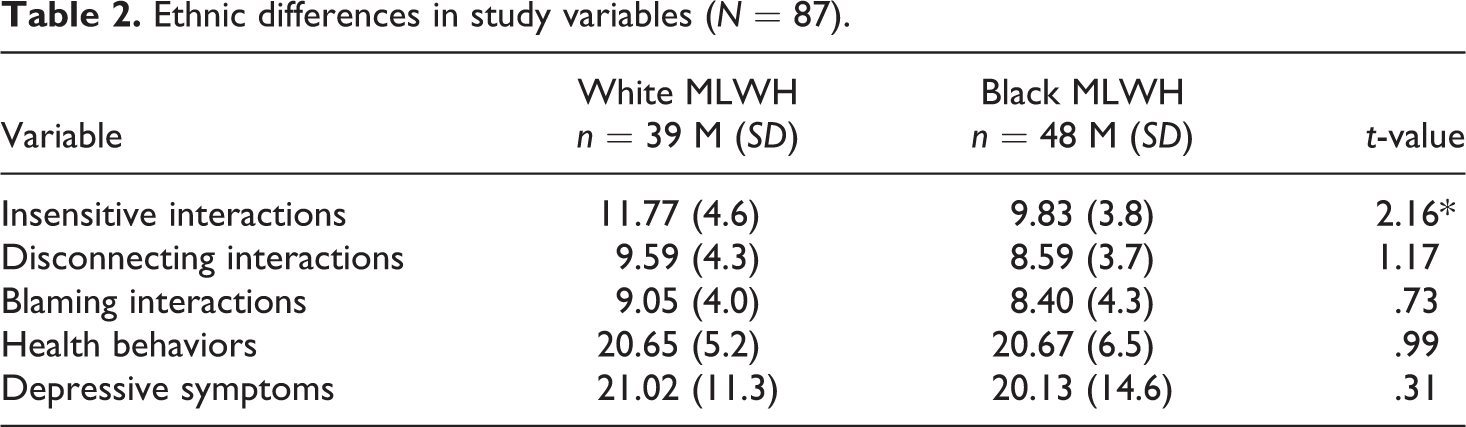
Several ethnic differences emerged among men’s sociodemographic, social, and health characteristics (Table 1). Specifically, compared to Black MLWH, White MLWH had more HIV-related symptoms, M White = 22.2; M Black = 15.4; t(85) = 2.52, p < .05, were more likely to report their sexual orientation as homosexual, χ 2(4, n = 87) = 9.70, p < .05, were less likely to be single, and were more likely to be in a homosexual relationship, χ 2(3, n = 87) = 13.84, p < .01. We also examined ethnic differences in our study variables (Table 2). Compared to Black MLWH, White MLWH reported higher levels of insensitive interactions, M White = 11.8; M Black = 9.8; t(85) = 2.16, p < .05. No ethnic differences were found in men’s reports of disconnecting or blaming interactions, depressive symptoms, or health behaviors.
Ethnic differences in study variables (N = 87).
Direct effects of HIV-specific unsupportive interactions
As predicted, after accounting for HIV-related symptoms and income, MLWH who reported more insensitive interactions regarding their HIV status also reported higher levels of depressive symptoms (β = .42; SE = .10, p < .001; ΔR 2 = .14, p < .001). Similarly, MLWH who reported more disconnecting and blaming interactions regarding their HIV also reported higher levels of depressive symptoms (β = .42; SE = .10, p < .001; ΔR 2 = .10, p < .001 for disconnecting and β = .42; SE = .10, p < .001; ΔR 2 = .14, p < .001 for blaming). Contrary to expectations, none of the HIV-specific unsupportive interactions were directly associated with men’s health behaviors (β = −.16; SE = .11, ns; ΔR 2 = .02, ns for insensitive; β = −.17; SE = .11, ns; ΔR 2 = .03, ns for disconnecting; and β = −.17; SE = .11, ns; ΔR 2 = .03, ns for blaming).
Depression as a mediator of HIV-specific unsupportive interactions and health behaviors
Our next hypothesis examined whether men’s depressive symptoms were a mediator of the relationship between HIV-specific USIs and health behaviors. Although the direct associations from HIV-specific USIs to health behaviors were not significant, we still examined the indirect associations of HIV-specific USIs on health behaviors through men’s depressive symptoms as current approaches to examining intervening variables suggest that variable X can have an indirect association on variable Y through an intervening variable (M) in the absence of a direct association between X and Y (Hayes, 2009).
As predicted (Table 3), depressive symptoms functioned as an intervening variable in the relationship between insensitive interactions and health behaviors. Specifically, the path between insensitive interactions and depressive symptoms was significant (b = 1.29, SE = .31, p < .001), and the path between depressive symptoms and health behaviors was also significant (b = −.18, SE = .05, p < .001). The indirect effect of insensitive interactions on health behaviors through depressive symptoms was also significant (estimate = −.24, confidence interval [CI] = −.44, −.11, p < .05), and the total model accounted for 23% of the variance in health behaviors (adjusted [Adj.] R 2 = .19, p < .001).
Depressive symptoms as a mediator of the relationship between HIV-specific unsupportive social interactions and health behaviors.
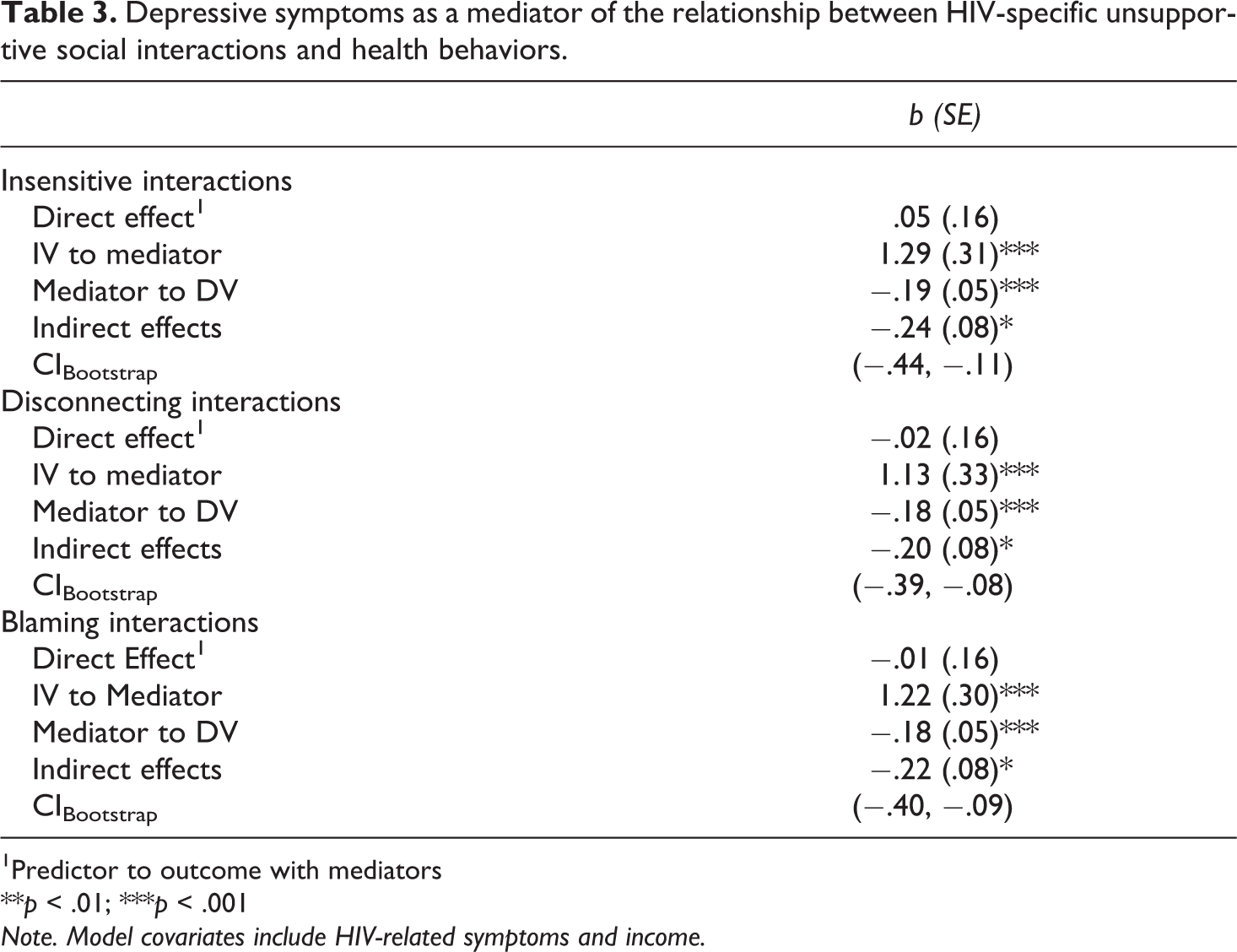
1Predictor to outcome with mediators
**p < .01; ***p < .001
Note. Model covariates include HIV-related symptoms and income.
Similarly, depressive symptoms were an intervening variable in the relationship between disconnecting interactions and health behaviors (Table 3). The path between disconnecting interactions and depressive symptoms was significant (b = 1.13, SE = .33, p < .001), and the path between depressive symptoms and health behaviors was also significant (b = −.18, SE = .05, p < .001). The indirect effect of disconnecting interactions on health behaviors through depressive symptoms was also significant (estimate = −.20, CI = −.39, −.08, p < .05), and the total model accounted for 23% of the variance in health behaviors (Adj. R 2 = .19, p < .001).
Finally, depressive symptoms were an intervening variable of the relationship between blaming interactions and health behaviors (Table 3). The path between blaming interactions and depressive symptoms was significant (b = 1.22, SE = .30, p < .001), and the path between depressive symptoms and health behaviors was also significant (b = −.18, SE = .05. p < .001). The indirect effect of insensitive interactions on health behaviors through depressive symptoms was significant (estimate = −.22, CI = −.40, −.09, p < .05), and the total model accounted for 23% of the variance in health behaviors (Adj. R 2 = .19, p < .001).
Mediated moderation
Our third hypothesis examined ethnicity as a moderator of the indirect effects of HIV-specific USIs on men’s health behaviors through depressive symptoms. Ethnicity emerged as a moderator of the model examining the associations between disconnecting social interactions and health behaviors through depression. Specifically, a significant interaction emerged between disconnecting interactions and ethnicity (b = −.88, SE = .30, p < .01) but not between depression symptoms and ethnicity (b = −.01, SE = .10, ns). Moreover, the conditional indirect effect was significant for Black men but not White men (indirect effect = −.23, SE = .12, z = −2.00, p < .05 for Black men; indirect effect = −.13, SE = .11, z = −1.22, ns for White men). Ethnicity did not emerge as a significant moderator of the associations between insensitive social interactions and health behaviors through depression or between blaming interactions and health behaviors through depression.
Discussion
This study extended prior research by examining HIV-specific USIs, depressive symptoms, and health behaviors among an ethnically diverse sample of MLWH, and whether depressive symptoms explain how unsupportive interactions come to be associated with more negative health behaviors. Identifying factors that put MLWH at risk for negative health behaviors is particularly important, given the significance of a healthy lifestyle for progression of disease (Collins et al., 2001). Consistent with prior research (Ingram et al., 1999; Song & Ingram, 2002), our study found that higher levels of HIV-specific insensitive, disconnecting, and blaming interactions were associated with more depressive symptoms in MLWH. Moreover, we found that increased depressive symptoms in the face of HIV-specific USIs served as an indirect mechanism that explained how the unsupportive interactions may become linked with poorer health behaviors among MLWH.
These findings further support the conclusion that higher levels of negative or USIs have a deleterious impact on well-being in individuals living with HIV (Ingram et al., 1999; Siegel et al., 1997; Song & Ingram, 2002). It is possible that when men experienced interactions that were overtly critical or negative, or when they perceived that a social network member was avoiding them or blaming them because of their HIV status, they felt stigmatized or discriminated against, which in turn led to increased feelings of distress (Hutton et al., 2013). Despite advances in HIV treatment and management making the illness more of a chronic than life threatening illness, HIV still carries a high stigma associated with it (Logie & Gadalla, 2009). Even if social network members have the intention of providing support, they may inadvertently send messages that men perceive as being unsupportive or critical. Experiencing different types of illness-specific USIs may be one factor that helps to explain why individuals with HIV have higher rates of depression than the general population (Cruess et al., 2003).
Contrary to our expectations, no direct associations emerged between HIV-specific USIs and health behaviors in MLWH. However, we did find evidence suggesting that HIV-specific social interactions were indirectly linked to poorer health behaviors through increases in men’s depressive symptoms. While prior research asserts that social support is associated with health behaviors and health-related quality of life in individuals with HIV through reduced depressive symptoms (Bekele et al., 2013; Deichert et al., 2008), our study is among the first to suggest that USIs may also be linked to health via their impact on depressive symptoms.
The association between HIV-specific USIs, depressive symptoms, and poorer health behaviors is notable as the rate of depression in MLWH is significantly higher than that of the general population (Cruess et al., 2003). In general, depression is linked to engaging in poorer health behaviors (Gottlieb & Green, 1984). In our study, over half of the men were at risk for being clinically depressed. MLWH who are depressed are more likely to cope with depression through the use of alcohol and drugs and engaging in risky sexual behaviors (Porche & Willis, 2006). In addition, depression, along with negative health behaviors such as smoking and alcohol consumption, is linked to poorer immune function and faster disease progression (Collins et al., 2001; Cruess et al., 2003). Thus, understanding how unsupportive interactions regarding men’s illness may indirectly be linked to the health behaviors and physical health of men through their psychological well-being is an important aspect of HIV-disease management.
Another reason that social relationships may be related to health behaviors through depressive symptoms is that a primary function of social relationships is their indirect promotion of health through social influence. Social control theory posits that one reason individuals engage in health behaviors is that they can remain healthy for those around them who depend on them (Umberson, 1987). This would suggest that MLWH engage in healthy behaviors, in part, so that they can remain healthy for their family and friends. Thus, when men encountered more USIs from members of their social network, they may have experienced higher levels of depression and thus less motivation to engage in a healthier lifestyle.
We also found the evidence that the relationships among disconnecting interactions, depressive symptoms, and health behaviors were dependent, in part, on men’s ethnicity. Specifically, the indirect effects of disconnecting interactions on health behaviors through depressive symptoms was significant for Black men but not for White men. One reason for these ethnic differences may be because individuals from ethnic minority populations tend to experience higher levels of stress and fewer resources to cope with that stress than individuals from nonminority populations (Meyer, 2003; Williams et al., 2003). This elevated level of stress coupled with the stress associated with negative interactions regarding one’s HIV status might become internalized and have a particularly negative impact on health, including health behaviors (Buseh, Kelber, Stevens, & Park, 2008; Hatzenbuehler, 2009). In addition, HIV is a highly stigmatized illness in many ethnic minority cultures, including Black culture, due to its associations with various behaviors including sexual orientation and drug use (Logie & Gadalla, 2009). Social support efforts from others may be undermined because of a lack of knowledge or fear regarding HIV and how HIV is transmitted (Song & Ingram, 2002). Thus, Black MLWH who perceived that their close social network members were withdrawing or distancing from them because of their HIV diagnosis may have experienced feelings of isolation, rejection, and stigma, which may in turn be associated with their tendency to engage in fewer self-care behaviors (Taylor, Repetti, & Seeman, 1997).
The links between disconnecting interactions, depressive symptoms, and poorer health behaviors in Black men are consistent with prior research showing that African American men’s perceptions of stigma about their illness were linked with more negative physical symptoms (Buseh et al., 2008). It is possible that a drop in self-care behaviors such as getting proper amounts of sleep, avoiding drug and alcohol use, and medication adherence may lead to more serious symptoms of infection, including faster disease progression. It is also possible that Black MLWH who perceive unsupportive interactions from their networks as stigmatizing might equally perceive their support networks as less available (Mickelson & Williams, 2008). This lack of contact with social network members, in turn, may negatively impact health behaviors in various ways. For example, Black MLWH may intentionally isolate themselves if they perceive that their network members are not available. This isolation may lead to feelings of loneliness and depression, which may, in turn, be associated with poorer health behaviors.
We did not find links between USIs and health behaviors in White MLWH. This is interesting considering that the White MLWH in our study reported experiencing more insensitive interactions than the Black MLWH in our study. These results suggest that there may be nuanced differences in the social relationships of Black and White MLWH. For example, White MLWH in our study were more likely to report their sexual orientation as being homosexual and were more likely to be in a homosexual relationship. While we controlled for these factors in our analyses, it is possible that White MLWH were more embedded in a social network that was accepting and understanding of their sexual orientation and HIV status. Even though White MLWH reported that they received higher levels of insensitive social interactions regarding their HIV status, it is unclear whether these interactions were from close or distant social network members. Although our study was unable to examine the specific sources of HIV-specific USIs, we did have descriptive data regarding men’s primary support providers.
When asked who their primary support providers were, 41.4% of men reported a friend, 24.1% reported a family member, 21.8% reported a spouse, partner, or regular sex partner, and 12.6% reported a health care provider. There were significant differences between the primary support providers of White MLWH and Black MLWH, χ 2(3, n = 87) = 11.6, p < .01. Specifically, Black MLWH were more likely to report that their primary support provider was a friend or family member, whereas White MLWH were more likely to report that their primary support provider was a spouse, partner, or regular sex partner. In addition, of the White MLWH who reported that they were in a relationship, 42.9% reported that their partner was also HIV positive. It is possible that, regardless of their status, partners were more knowledgeable about HIV, understanding of, and accepting of men’s HIV-positive status. Future research should examine the specific sources of USIs in Black and White MLWH as well as how positive sources of support or satisfaction with support received may buffer the negative effects of these negative social interactions on health. Moreover, it is possible that in addition to ethnicity, factors such as sexual orientation and relationship status may moderate the associations between USIs and health.
Our study has several limitations that should be noted. Because the study design was cross-sectional, we were unable to establish the temporal ordering of HIV-specific social interactions, depressive symptoms, and health behaviors. It is possible that compared to men with lower levels of depressive symptoms, men with higher levels of depressive symptoms were more likely to recall interactions that they experienced as being more negative and unsupportive (Levine & Safer, 2002; Matt, Vázquez, & Campbell, 1992). In addition, men’s health behaviors or perceptions of their own health status may have preceded their experience of various USIs. For example, it is possible that men’s poor health behaviors sent a message to their social networks that they were not caring for themselves properly. Thus, the disconnecting and withdrawing of social network members that Black MLWH experienced may have been a result of frustration and anger because the patient was not engaging in proper self-care behaviors. It is also possible that men who engaged in poorer health behaviors were less likely to be integrated into health-related social activities such as working out at a gym or exercising with friends. This lack of social contact could have also contributed to their feelings of being disconnected. As evidence suggests that depressive symptoms are associated with faster HIV-disease progression, problems with immune function, and more disease complications (Cruess et al., 2003; Leserman, 2003), future research should examine the temporal associations between HIV-specific USIs, depressive symptoms, and physiological markers of disease (e.g., immune function, viral load). Research should also examine the role that USIs play in longer term disease management and psychological well-being.
Another limitation of our study is that we measured self-identified race as a proxy for ethnicity. It is possible that some of the MLWH in our study did not necessarily identify with their ethnicity. However, because race is a part of an individual’s ethnicity (Kaplan & Bennett, 2003), it is commonly used as a proxy for examining racial/ethnic differences in social interactions and health. Future research should assess Black-identity-related components (Sellers, Rowley, Chavous, Shelton, & Smith, 1997) in relation to HIV, USIs, and health. Finally, it is unclear how our results would generalize to women living with HIV, other ethnic groups, or other chronically ill individuals who experience illness-specific USIs. Future research should examine longitudinal associations among illness-specific USIs, cultural values, and health in both men and women from multiple ethnic backgrounds living with HIV or other chronic illnesses. In addition, future research should examine variables that may account for the associations between USIs and health in White and Black MLWH, such as men’s interpretations of USIs or perceived stigma or discrimination.
Despite its limitations, our study strengthens and expands the literature on social interactions, depressive symptoms, and health in MLWH in several ways. Our study suggests that various types of HIV-specific USIs are negatively associated with psychological well-being, but not physical well-being, in MLWH. The associations between HIV-specific USIs and physical health are more complex and may be explained, in part, by both depressive symptoms and ethnic differences in MLWH. These results have implications for psychosocial interventions, such that interventions should focus on the links between depressive symptoms and health behaviors in MLWH. In addition, interventions should acknowledge that the experience of living with HIV/AIDS may be different for Black and White MLWH and that their social networks and social experiences related to HIV and health outcomes may differ as well.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.