
Abstract
Most first-time mothers experience a decline in both their sexual and relationship satisfaction from prepregnancy, which has negative consequences for the couple and their family. Prior studies have begun to identify risk and protective factors (e.g., empathy) for postpartum sexual and relationship satisfaction. Causal attributions for postpartum sexual concerns may be important because a specific cause can be difficult to pinpoint given the wide range of postpartum sexual problems among first-time parents. In the current study, 120 first-time mothers (3–12 months postpartum) completed validated measures assessing attributions for postpartum sexual concerns, sexual satisfaction, and relationship satisfaction. Attributions were measured on four dimensions: internal/external (i.e., is the sexual concern due to the self or the situation), stable/unstable (i.e., will the cause of the concern occur again in the future), global/specific (i.e., will the cause of the concern affect other situations), and partner responsibility (i.e., is the partner the cause). When new mothers reported more stable and partner attributions for postpartum sexual concerns, they were less sexually satisfied, and when they attributed greater responsibility for sexual concerns to their partners, they were less satisfied with their overall relationship. These associations remained significant after controlling for potential challenges that may also impact sexual and relationship satisfaction during this period (i.e., breastfeeding, sexual frequency, depressive symptoms, fatigue, sexual functioning). As postpartum sexual concerns are common, attributions for these changes may be a valuable target for interventions aimed at strengthening the intimate relationships of women making the transition to parenthood.
Keywords
The transition to parenthood presents notable sexual and relationship challenges. At 6 months postpartum, 36% of new mothers describe themselves as discontent with their sexual relationship (Ahlborg, Dahlof, & Hallberg, 2005). Sexual concerns, such as reduced or mismatched sexual desire with a partner, lack of time or energy for sexual activity, and lower sexual frequency, are especially common in the first year after giving birth for both new mothers and fathers (Schlagintweit, Bailey, & Rosen, 2016; Yildiz, 2015). In tandem with postpartum sexual concerns, longitudinal research shows that the vast majority (up to 93%) of first-time mothers experience a decline in relationship satisfaction after the birth of a child. These declines are steeper than those experienced by nonparents over the same time period and persist up to a decade postpartum (Doss, Rhoades, Stanley, & Markman, 2009; Keizer & Schenk, 2012). Difficulties in the intimate relationship can have wider reaching consequences for the couple (e.g., relationship dissolution), the parent–child relationship (e.g., less warm parenting), and the child’s later development (e.g., behavioral problems; Goldberg & Carlson, 2014; Røsand, Slinning, Røysamb, & Tambs, 2014; Stroud, Meyers, Wilson, & Durbin, 2015). As such, identifying risk and protective factors for postpartum sexual and relationship satisfaction is critical for promoting the well-being of the couple and the family as a whole. Although there is considerable research examining physiological predictors of postpartum sexual well-being (e.g., breastfeeding, mode of delivery), recent work has highlighted the importance of considering psychological factors (e.g., empathy, parenting stress, body image) for understanding both the sexual and relationship satisfaction of new parents (Jawed-Wessel, Herbenick, & Schick, 2016; Leavitt, McDaniel, Maas, & Feinberg, 2017; Muise, Kim, Impett, & Rosen, 2017; Rosen, Mooney, & Muise, 2016). The aim of the current study was to investigate associations between a psychological factor—mothers’ causal attributions for postpartum sexual concerns—and women’s postpartum sexual and relationship satisfaction.
Causal attributions
Causal attributions refer to an individual’s attempt to assign a cause to an experience (Kelley, 1967; Weiner, 1986). Earlier research on causal attributions focused primarily on the domains of depression and achievement (Graham, 1991; Seligman, Abramson, Semmel, & Von Baeyer, 1979). This work was later extended to examine attributions in the context of a broad range of negative life events (e.g., illness, death, crime, sexual assault, interpersonal conflict; Fincham & Bradbury, 1992; Hall, French, & Marteau, 2003). Although key types of causal attributions have been defined in various ways (see Bradbury & Fincham, 1990, for a review), attributions are most often conceptualized along three dimensions: (1) internal versus external (i.e., whether the cause is due to the self or the situation), (2) stable versus unstable (i.e., whether or not the cause will occur again in the future), and (3) global versus specific (i.e., whether or not the cause affects other situations; Bradbury & Fincham, 1992; Weiner, 1986). An example of an internal, stable, and global attribution for concerns about sexual frequency among new mothers is “Now that I am a mother I am no longer a sexual person,” whereas an example of an external, unstable, and specific attribution is “Because I just had a baby, I have less energy for sex right now.” A unique consideration when examining attributions about events that arise in a dyadic context, like a romantic relationship, is that external attributions can refer to the situation, the partner, or both. Partner responsibility attributions assign the cause of an event to the partner. For example, a new mother with high partner responsibility attributions may explain decreased sexual frequency by concluding “My partner is no longer attracted to me” or “My partner is always too tired for sex.” According to attribution theory, attributions create psychological (i.e., affective and cognitive) and behavioral consequences, such as negative affect or hostile actions toward a partner, which shape later outcomes, such as sexual or relationship satisfaction (Weiner, 1986). Thus, in the context of postpartum sexuality, as compared to holding more external, unstable, or specific attributions, holding stronger internal, stable, global, or partner responsibility attributions may trigger negative affective (e.g., anxiety, disrupted emotional regulation), cognitive (e.g., catastrophizing), and behavioral (e.g., avoidance of affection and intimacy) responses, resulting in lower sexual and relationship satisfaction.
Causal attributions and sexual and relationship well-being
Higher internal, global, or stable attributions, as compared to more external, unstable, or specific attributions, have been linked with lower relationship satisfaction in community and clinical samples (Fincham & Bradbury, 1993; Neff & Karney, 2004; Péloquin, Brassard, Arpin, Sabourin, & Wright, 2017, Shnaider, Belus, Vorstenbosch, Monson, & Langhinrichsen-Rohling, 2014). In a sample of 130 newlywed couples, those with greater internal, global, or stable attributions for negative spouse behavior during the second year of marriage (e.g., being criticized by a partner) reported lower marital satisfaction 18 months later, compared to couples who reported more external, specific, or unstable explanations for their spouse’s negative actions (Fincham, Harold, & Gano-Phillips, 2000). Partner attributions influence negative behavior toward a spouse and perceptions of the relationship (Bradbury, Beach, Fincham, & Nelson, 1996; Davis, Bergeron, Sadikaj, Corsini-Munt, & Steben, 2015; Ellison, Kouros, Papp, & Cummings, 2016). Indeed, individuals who attribute more blame to a partner for a negative event tend to fare worse in their romantic relationships compared to those who do not blame their partner for negative events (Miller & Bradbury, 1995; Mitchell, King, Nazareth, & Wellings, 2011; Péloquin et al., 2017; Shnaider et al., 2014). In a longitudinal study of 280 newlywed couples, attributing greater responsibility to the partner for relational conflict during the first year of marriage was associated with participants’ own, and their partners’, lower marital quality 4 years later (Durtschi, Fincham, Cui, Lorenz, & Conger, 2011).
Applications of attribution theory in the sexual domain show similar patterns: In cross-sectional studies more internal, stable, global, or partner attributions for negative sexual experiences (e.g., genito-pelvic pain, low sexual desire or arousal, erectile dysfunction) are associated with poorer sexual and relationship well-being, compared to more external, unstable, or specific attributions (Jodoin et al., 2011; Meana, Binik, Khalife, & Cohen, 1999; Reissing, 2012; Rowland, Kostelyk, & Tempel, 2016; Scepkowski et al., 2004; Sims & Meana, 2010; Weisberg, Brown, Wincze, & Barlow, 2001). In a study of women experiencing common sexual problems (e.g., difficulties with desire, arousal, orgasm, or pain), endorsing more internal, global, or stable attributions for their sexual problem was associated with lower sexual satisfaction, and greater partner attributions were linked with lower sexual and relationship satisfaction (Stephenson & Meston, 2016). Further, among women experiencing pain during sexual intercourse, holding stronger global or stable attributions for their pain was associated with lower relationship adjustment, but contrary to predictions based on attribution theory, women with stronger internal attributions reported higher relationship adjustment (Jodoin et al., 2011). Overall, these studies underscore the value of attributions for shaping the sexual and relationship well-being of those coping with sexual challenges, as well as the unique role that partner responsibility attributions may play in an interpersonal context such as the sexual or romantic relationship.
Attributions for postpartum sexual concerns
First-time mothers’ attributions for postpartum sexual concerns may be of particular importance to their well-being because the specific cause is difficult to pinpoint given the wide range of postpartum sexual concerns among first-time parents. Indeed, a recent survey of 239 first-time parent couples found that 89% of new mothers endorsed 11 or more sexual concerns (M = 16, range = 0–20; Schlagintweit et al., 2016). Further, postpartum sexual challenges may be unexpected, especially for women who are becoming a parent for the first time. Many women do not receive information about postpartum sexuality from their health-care providers (Bartellas, Crane, Daley, Bennett, & Hutchens, 2000; Guerra-Reyes, Christie, Prabhakar, & Siek, 2017) and mothers who are aware of the likelihood of these problems may still be unprepared for the suddenness, severity, and persistence of these changes. Given that attributions aim to assess explanations that people make for unexpected events (Kelley, 1967; Weiner, 1986) and that the majority of women experiencing a sexual problem report trying to understand the cause of their problem (Mitchell et al., 2011), it follows that first-time mothers who are faced with postpartum sexual concerns will form attributions for their experiences, with potential implications for their sexual and relationship satisfaction. In addition, because women bear the physical burden of childbirth and becoming a parent is a life-changing experience, forming internal (e.g., “My body is physically recovering”), stable (e.g., “I am now a parent”), or global (e.g., “Our whole life has changed now that we have a baby”) attributions to explain postpartum sexual concerns may be, to some degree, normative. Yet, the outcomes associated with attributions for postpartum sexual concerns have not previously been examined.
Measuring attributions that are specific to postpartum sexual changes offers several advantages. First, general measures such as general attributional style (e.g., Peterson & Vilanova, 1988) or nonsexual relationship attributions (e.g., Fincham & Bradbury, 1992) assess broader attributions for other characteristics of the relationship (e.g., relationship conflict) or stressors in a person’s life, beyond sexuality. In contrast, measuring attributions for postpartum sexual changes, as compared to more general attributions, allows respondents to focus on the changes in their sexual relationship since having a baby. Indeed, adapting a general attributions measure to focus on a specific context of interest such as attributions for illness (Cope, David, & Mann, 1994), nonsexual behavior of a romantic partner (Bradbury & Fincham, 1992), sexual pain (Jodoin et al., 2011), and sexual dysfunction (Scepkowski et al., 2004) is common practice. Second, adapting general psychological measures specifically to a sexual context improves the predictive validity of the measure and has been shown to have unique effects on sexual and relationship outcomes (above and beyond general measures). The enhanced validity of sexuality-specific measures has been demonstrated in a wide range of domains, including the sexual communal strength (Muise & Impett, 2015), sexual narcissism (McNulty & Widman, 2013), sexual intimacy (Bois, Bergeron, Rosen, McDuff, & Grégoire, 2013), and sexual communication (Rancourt, Flynn, Bergeron, & Rosen, 2017).
Current study
The aim of the current study was to examine the associations between attributions for postpartum sexual concerns and sexual and relationship satisfaction in first-time mothers. Based on attribution theory and our review of the literature, we predicted that more internal, stable, global, and partner responsibility attributions for postpartum sexual concerns would be associated with lower sexual and relationship satisfaction compared to more external, unstable, specific, and nonpartner responsibility attributions. We also wanted to rule out the possibility that our observed effects could be accounted for by other variables that are present during the postpartum period and that past research has linked with maladaptive attribution styles or sexual and relationship satisfaction. Specifically, depression is associated with greater maladaptive attribution styles (Alloy et al., 2006; Gavin et al., 2005), physical affection and frequency of partnered sexual activity is linked with greater sexual and relationship satisfaction (Muise, Giang, & Impett, 2014; Muise, Schimmack, & Impett, 2016; Young, Denny, Luquis, & Young, 1998), depression and fatigue are associated with lower levels of postpartum sexual and relationship satisfaction (De Judicibus & McCabe, 2002; Frohlich & Meston, 2002; Whitton & Kuryluk, 2012), and earlier sexual and relationship satisfaction tends to predict later sexual and relationship well-being (Fallis, Rehman, Woody, & Purdon, 2016). We therefore also tested our hypotheses when controlling for these relevant covariates.
Finally, we planned two sets of exploratory analyses due to a lack of prior research to form firm hypotheses. The first set of analyses tested the possibility that the attributions of women experiencing more severe sexual problems may be stronger predictors of sexual and relationship satisfaction as compared to the attributions of women who are experiencing fewer sexual problems. As such, we examined women’s sexual functioning as a moderator of the link between attributions and sexual and relationship satisfaction. In the second set of analyses, we explored the possibility that specific types of attributions may interact to predict sexual and relationship satisfaction. One study found that couples with lower levels of marital adjustment were more likely to attribute positive spouse behavior to causes that were both unstable and internal as compared to causes that were both stable and internal (Lavin, 1987), suggesting that examining specific combinations of types of attributions may provide unique insight into the associations between attributions and sexual and relationship satisfaction. To test this possibility, we examined the two-way interactions among all four types of attributions (i.e., internal, stable, global, partner responsibility) in an exploratory manner.
Method
Participants and procedures
The final sample was comprised of 120 first-time mothers. Demographics and postpartum characteristics can be found in Table 1. Participants were recruited from a hospital ultrasound clinic in a mid-sized Canadian city as part of a larger longitudinal study examining postpartum physical and psychosocial functioning. Eligible women were 18–25 weeks pregnant with their first child at the time of recruitment into the larger study, 18 years of age or older, with an uncomplicated, singleton pregnancy (to minimize the possibility of third variables, such as increased fatigue associated with caring for twins, or greater physical burden on the pregnant participant impacting relationship and sexual satisfaction), able to read and write in English, and had access to a personal e-mail. Women were excluded from the broader study if they self-identified as having a severe and unmanaged medical or psychiatric disorder (e.g., major depression that is not being treated) and excluded from the current study if they indicated that they were not in a romantic relationship. Women were initially enrolled from July 2015 to September 2016. They were invited to participate in the current cross-sectional study between December 2016 and April 2017 when they reached the 3, 6, or 12-month postpartum time point of the longitudinal study (and were invited at only one time point).
Descriptive statistics for participant characteristics and predictor and outcome variables.

Note. n = 120 unless otherwise noted.
a n = 119.
b n = 118.
For the current study, eligible women completed online surveys at 18–25 weeks pregnancy (demographics, sexual satisfaction, relationship satisfaction) and at 3-, 6-, or 12-month postpartum (attributions for postpartum sexual concerns, sexual satisfaction, relationship satisfaction, breastfeeding, fatigue, affectionate and partnered sexual behaviors, depressive symptoms, and sexual functioning). The measure assessing attributions for postpartum sexual problems was added after participants had provided initial consent to participate in the larger longitudinal study. As such, 219 participants were asked the following at 3-, 6-, or 12-month postpartum: Since you started the study we have added a new measure to each postpartum survey. This measure asks about changes to your sex life since having your baby, and will take 5–10 min to complete. Do you wish to complete this measure? Please note, that choosing to skip this measure will not affect your compensation or ability to complete future surveys.
Measures
Sample characteristics
Participants responded to questions assessing age, education, cultural background, income, sexual orientation, relationship status, relationship duration, and proportion of feedings in the past 4 weeks that were comprised of the mother’s breast milk (either from breast or bottle).
Attributions for postpartum sexual concerns
Sexual attributions were assessed using a modified Sexual Attributional Style Questionnaire, similar to that used by Jodoin et al. (2011) in a study of genito-pelvic pain, and which we pilot tested prior to use in this study. 1 The complete measure can be found in the Online Appendix. The scale includes seven scenarios, each representing a hypothetical negative sexual event that is highly common during the postpartum period (Schlagintweit et al., 2016). Participants were asked to imagine that they had experienced the event in the past 4 weeks and to identify what they believed was the main cause of each event (open-ended item). Participants then rated the cause of each event on 7-point Likert-type scales assessing four subscales: Internal Versus External, Stable Versus Unstable, Global Versus Specific, and Partner Responsibility. Scores on each subscale can range from 1 to 7, and higher scores indicate greater internal, stable, global, and partner responsibility attributions. Consistent with prior studies using similar measurement of attributions (Jodoin et al., 2011; Scepkowski et al., 2004), reliability in the current sample was acceptable for the Internal (α = .71), Global (α = .78), Stable (α = .78), and Partner Responsibility (α = .75) subscales.
Sexual satisfaction
Sexual satisfaction was assessed using the well-validated global measure of sexual satisfaction (Lawrance & Byers, 1995). Participants rated their sexual relationship on five 7-point bipolar scales (e.g., good–bad, pleasant–unpleasant). Scores can range from 5 to 35, and higher scores indicate greater sexual satisfaction. Reliability in the current study was high (α = .95).
Relationship satisfaction
Relationship satisfaction was assessed using the 4-item Couples Satisfaction Index—Short form (CSI-SF; Funk & Rogge, 2007). Participants rated different facets of their relationship satisfaction in the last 4 weeks (e.g., happiness, warmth) on 6- or 7-point Likert-type scales. Scores can range from 0 to 21, and higher scores indicate higher relationship satisfaction. A score below 13.5 is indicative of significant relationship distress. The CSI-SF demonstrated strong reliability in the current study (α = .93).
Affection and sexual behavior
Participants indicated how often they had engaged in kissing, touching, giving manual genital stimulation, receiving manual genital stimulation, giving oral sex, receiving oral sex, and vaginal intercourse, in the prior 4 weeks on a 7-point scale ranging from 0 (never) to 6 (daily). Responses to the 2 items assessing kissing and touching were summed to create a total “affection” score and responses to the 5 items assessing manual genital stimulation, oral sex, and intercourse were summed to create a total “partnered sexual activity” score.
Depressive symptoms
Depressive symptoms were assessed using the well-validated Edinburgh Postnatal Depression Scale (EPDS; Cox, Holden, & Sagovsky, 1987; Matthey, Barnett, Kavanagh, & Howie, 2001). Participants rated their feelings in the past week on a 10-item scale. Response options ranged from 0 to 3. An example item is: “I have looked forward with enjoyment to things” with the response options 0 (as much as I ever did), 1 (rather less than I used to), 2 (definitely less than I used to), and 3 (hardly at all). Scores range from 0 to 30, with higher scores indicating more severe depressive symptoms. The EPDS demonstrated strong reliability in the current study (α = .86).
Fatigue
Participants indicated their average energy level on a typical day using a single-item 7-point scale ranging from 1 (high energy) to 7 (extreme fatigue; Rosen et al., 2016).
Sexual functioning
Sexual functioning was assessed using the Female Sexual Functioning Index (FSFI; Rosen at al., 2000), a well-validated and reliable measure. The FSFI includes 19 items and assesses six domains of sexual functioning (i.e., desire, arousal, lubrication, orgasm, satisfaction, and pain). The FSFI is only valid among women who have engaged in sexual activity in the past 4 weeks. To minimize multicollinearity between the sexual functioning variable and our outcome variables (i.e., sexual and relationship satisfaction), we excluded the 3 items assessing the satisfaction domain when calculating the FSFI total score. Participants respond to each item on a 5- or 6-point Likert-type scale. Total scores range from 1.2 to 30, with higher scores indicating higher sexual functioning. The scale demonstrated strong reliability in the current study (α = .92).
Data analyses
There were less than 5% missing data and mean substitution was used to replace these values (Tabachnick & Fidell, 2013). Primary analyses were two multiple linear regressions in which the four attributions subscales (Internal, Global, Stable, and Partner Responsibility) were included as simultaneous predictors. Separate models were conducted for sexual satisfaction and relationship satisfaction. We repeated these analyses using hierarchical regressions to control for potential covariates that may shape attributions for postpartum sexual concerns and contribute to sexual and relationship satisfaction postpartum, as well as to examine interactions between attributions and sexual functioning and two-way interactions between the four attribution dimensions. Postpartum sexual satisfaction was negatively skewed (Z skewness = 3.12, p < .01). As such, a square root transformation was applied before conducting all analyses. After the transformation was applied, values were reverse scored, so higher values indicated higher sexual satisfaction. The means and standard deviations presented in Table 1 represent nontransformed data. All other analyses (i.e., correlations, analyses of variance [ANOVAs], regressions) use the transformed sexual satisfaction data. The data met all other statistical assumptions.
Results
Descriptive characteristics and correlations
Descriptive characteristics of all predictor and outcome variables can be found in Table 1. Overall, participants reported moderate levels of sexual and relationship satisfaction, and 24.2% of participants met the cut-off score for low relationship satisfaction, which indicates relationship distress. A repeated-measures ANOVA was conducted to examine mean differences in endorsement of the four types of attributions, Wilks’s λ = .25, F(3, 117) = 114.70, p < .001. Follow-up pairwise comparison tests revealed that stable and internal attributions received significantly higher endorsement by participants as compared to global and partner responsibility attributions. Partner responsibility attributions received a significantly lower level of endorsement as compared to stable, internal, and global attributions.
Examination of bivariate correlations provided partial preliminary support for hypotheses (see Table 2). Stable and partner responsibility attributions were associated with lower sexual and relationship satisfaction. Internal and global attributions were unrelated to outcome variables. Age, income, relationship length, and breastfeeding were not associated with the predictor and outcome variables (see Table 3). Depression and fatigue were negatively correlated with sexual and relationship satisfaction and positively correlated with stable and global attributions. Frequency of physical affection was associated with greater relationship satisfaction, and frequency of partnered sexual activity was linked with greater sexual and relationship satisfaction. Greater sexual functioning was associated with higher sexual and relationship satisfaction. Finally, women who reported higher sexual and relationship satisfaction during pregnancy reported higher postpartum sexual and relationship satisfaction. A one-way ANOVA revealed that women who were married were more satisfied with their relationship than unmarried women (Ms = 16.48 vs. 14.56), F(1, 117) = 7.95, p < .01.
Bivariate correlations between postpartum sexual satisfaction, relationship satisfaction, and attributions subscales.

Note. n = 120.
*p < .05. **p < .01. ***p < .001.
Bivariate correlations between covariates, postpartum sexual and relationship satisfaction, and attributions subscales.
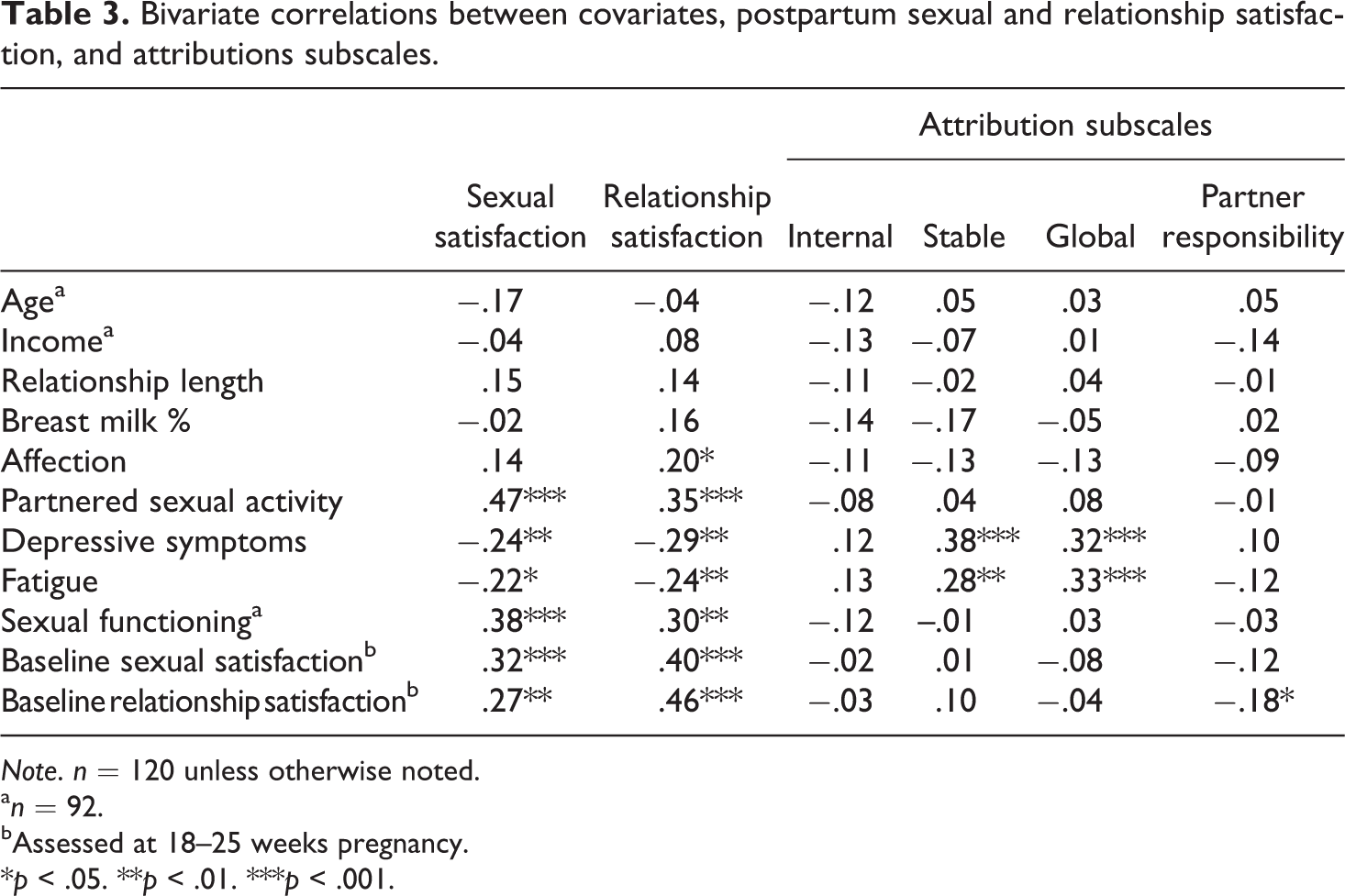
Note. n = 120 unless otherwise noted.
a n = 92.
bAssessed at 18–25 weeks pregnancy.
*p < .05. **p < .01. ***p < .001.
Sexual and relationship satisfaction
The results of the regression analyses are presented in Table 4. Overall, the model predicting sexual satisfaction accounted for 12% of the variance. Consistent with hypotheses, greater stable and partner responsibility attributions were each uniquely associated with lower levels of sexual satisfaction. However, internal and global attributions were unrelated to sexual satisfaction. The model predicting relationship satisfaction accounted for 12% of the variance. As hypothesized, greater partner responsibility attributions were associated with lower relationship satisfaction. Internal, stable, and global attributions were not associated with relationship satisfaction.
Regression analyses predicting sexual satisfaction and relationship satisfaction, using attributions for postpartum sexual concerns.
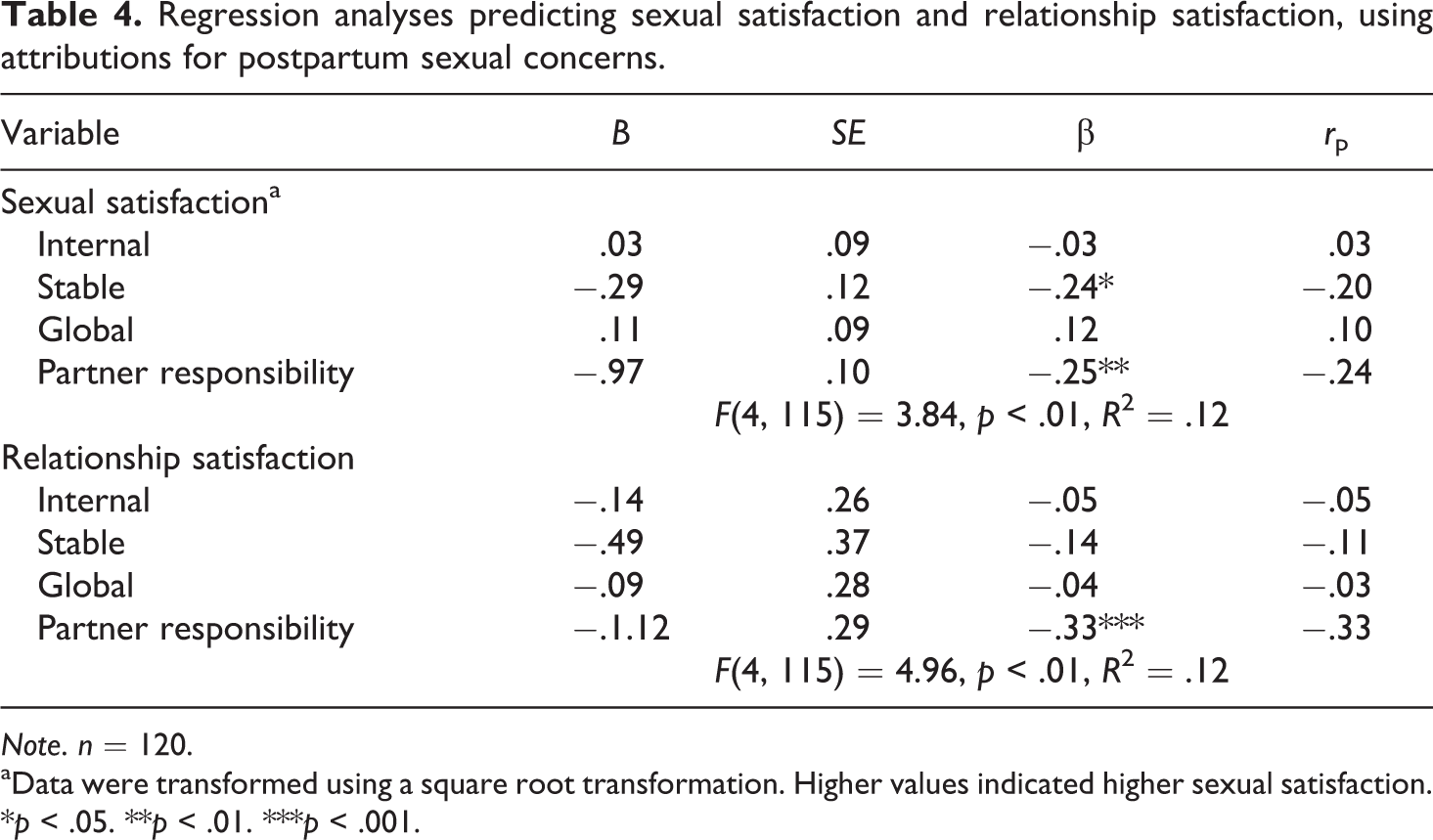
Note. n = 120.
aData were transformed using a square root transformation. Higher values indicated higher sexual satisfaction.
*p < .05. **p < .01. ***p < .001.
Alternative explanations and exploratory analyses
We conducted additional analyses to rule out potential alternative explanations for our findings that might contribute to negative attributional styles or sexual and relationship satisfaction. First, we tested whether our effects could be attributed to variability in sexual and affectionate activity, depressive symptoms, postpartum fatigue, or earlier sexual and relationship satisfaction (i.e., satisfaction levels assessed in pregnancy). Breastfeeding was not correlated with our key variables and was therefore no longer considered as a potential covariate. We also examined time point (i.e., 3-, 6-, or 12-month postpartum) as a covariate and a potential moderator and found no effects. We reran our analyses using two hierarchical linear regressions whereby the potential covariates were entered in Step 1 (frequency of affection, frequency of partnered sexual activity, depressive symptoms, fatigue, and sexual or relationship satisfaction at 18–25 weeks pregnancy) and the four attribution variables (internal, stable, global, partner responsibility) were entered in Step 2. In both the model of sexual satisfaction and relationship satisfaction, all of our effects remained significant when controlling for the covariates, suggesting that our effects were not being driven by these other factors. Indeed, attributions continued to account for 10% of the variance in sexual satisfaction and 9% of the variance in relationship satisfaction. However, one additional significant effect emerged when including the covariates: Contrary to our hypothesis, more global attributions were associated with greater sexual satisfaction (β = .22, p < .05). Table 4 of the Online Supplement reports the results of these analyses in detail.
Next, we conducted our first set of exploratory analyses, which examined whether the severity of postpartum sexual problems moderated the associations between attributions and sexual and relationship satisfaction. To test this possibility, we conducted two hierarchical linear regressions whereby sexual functioning was entered in Step 1, the four attribution variables (internal, stable, global, partner responsibility) were entered in Step 2, and the four 2-way interactions between sexual functioning and attributions were entered in Step 3. All variables were centered. As a total, sexual functioning score could be calculated for only the women who had engaged in sexual activity in the past 4 weeks, these analyses focused on the subsample of sexually active women (n = 92). Greater sexual functioning was significantly associated with greater sexual (β = .38, p < .001) and relationship (β = .30, p < .001) satisfaction. In both the model of sexual satisfaction and relationship satisfaction, all of our effects remained significant when controlling for sexual functioning, and attributions predicted 19% of the variance in sexual satisfaction and 18% of the variance in relationship satisfaction. Sexual functioning did not moderate the associations between attributions and sexual and relationship satisfaction. See the Online Supplemental Table 5, which reports the results of these analyses in detail.
Finally, we conducted our secondary set of exploratory analyses, which tested whether there might be important interactions between the specific types of attributions. We conducted two hierarchical linear regressions (one for each outcome) whereby the four attribution variables (internal, stable, global, partner responsibility) were entered in Step 1, and all six possible two-way interactions between attributions (Internal × Global, Internal × Stable, Global × Stable, Internal × Partner, Global × Partner, Stable × Partner) were entered in Step 2. All variables were centered. There were no significant interactions in the regression predicting sexual satisfaction, FΔ(6, 109) = 1.48, ns. However, in the regression predicting relationship satisfaction, there were two significant interaction terms on Step 2, FΔ(6, 109) = 2.69, p < .05, R 2Δ = .11: Internal × Partner (β = .25, p < .05) and Stable × Partner (β = –.25, p < .05). When we followed up the Partner × Internal interaction, we found that at lower levels of internal attributions, greater partner responsibility attributions were associated with lower relationship satisfaction, β = −.58, t(109) = −4.75, p < .001, whereas at higher levels of internal attributions, partner responsibility attributions were not significantly associated with relationship satisfaction, β = −.08, t(109) = −.08, ns. When we followed up the Partner × Stable interaction, we found that at higher levels of stable attributions, greater partner responsibility attributions were associated with lower relationship satisfaction, β = −.58, t(109) = −4.56, p < .001, whereas at lower levels of stable attributions, partner responsibility attributions were not significantly associated with relationship satisfaction, β = −.09, t(109) = −.62, ns. See the Online Supplemental Table 6 and Figure 1, which report the results of these analyses in detail.
Discussion
The aim of the current study was to examine the associations between attributions for postpartum sexual concerns and sexual and relationship satisfaction among first-time mothers during the first-year postpartum. When women reported greater stable and partner attributions for postpartum sexual concerns, they were less sexually satisfied, and when they attributed greater responsibility for sexual concerns to their partners, they were less satisfied with their overall relationship. These associations remained significant after controlling for relevant factors that may affect attributions or sexual and relationship satisfaction during this period (i.e., affection, frequency of partnered sexual activity, depressive symptoms, fatigue, earlier sexual or relationship satisfaction, and sexual functioning). In addition, after controlling for these other factors, more global attributions were associated with greater sexual satisfaction, which was contrary to our original hypothesis. Finally, the results of our exploratory analyses revealed interactions between specific types of attributions: Greater partner responsibility attributions were associated with lower relationship satisfaction when new mothers also held stronger external and stable attributions, as compared to more internal or unstable attributions. Overall, although these results are cross-sectional, they are consistent with attributions theory (Weiner, 1986), as it has been applied to sexual and romantic relationships (Jodoin et al., 2011; Stephenson & Meston, 2016), which suggests that attributions have affective, cognitive, and behavioral consequences that shape later sexual and relationship well-being. The current study extends this theoretical model to the context of sexuality during early motherhood and indicates a novel potential target for interventions aimed at improving the sexual and relationship satisfaction of first-time mothers.
As predicted, greater partner responsibility attributions were associated with lower sexual and relationship satisfaction. This finding is consistent with research showing that blaming a partner for problems in the sexual or romantic relationship is linked with a less satisfying sexual and romantic relationship (Miller & Bradbury, 1995; Mitchell et al., 2011; Péloquin et al., 2017; Shnaider et al., 2014). Among the new mothers in our sample, only greater partner responsibility attributions were associated with lower relationship satisfaction, suggesting that this specific type of attribution may signal broader problems in a romantic relationship. Other studies have found that stronger partner attributions—such as blaming the partner for negative relationship events—are related to less effort to improve a relationship and lower levels of willingness to forgive a partner (Fichten, Spector, & Libman, 1988; Furman, Luo, & Pond, 2017; Hall & Fincham, 2006). Partner attributions have also been shown to influence behavior toward a spouse (Bradbury et al., 1996; Davis et al., 2015) and, in turn, perceptions of the relationship (Ellison et al., 2016). In one study, greater partner responsibility attributions regarding relationship conflict were associated with more hostile behaviors toward a spouse, which, in turn, was linked to lower relationship satisfaction 2 years later (Durtschi et al., 2011). Over time, new mothers who place more blame on their partner for postpartum sexual concerns may be less likely to focus on maintaining or strengthening their sexual and romantic relationship during this highly vulnerable transitional period, resulting in less satisfaction. This hypothesis would have to be tested in a longitudinal study design, however. Moreover, from our exploratory analyses, greater partner responsibility attributions were linked to lower relationship satisfaction when new mothers also held stronger external and stable attributions (compared to more internal or unstable attributions). Thus, partner attributions appear to be less problematic when women also share responsibility for sexual concerns (i.e., internal attributions) or believe that the cause of the sexual concerns is likely to change over time (i.e., unstable attributions). On average, endorsement of partner responsibility attributions was not particularly high in this study (M = 2.5 on a scale ranging from 1 to 7, with higher scores indicating higher endorsement). That said, even at these comparatively low levels, perceiving postpartum sexual concerns as caused by the partner was linked with poorer sexual and relationship well-being, highlighting the powerful role that partner responsibility attributions may play in an interpersonal context.
New mothers’ stable attributions for postpartum sexual concerns were associated with lower sexual satisfaction but were not directly related to relationship satisfaction, which is in line with other research examining women’s attributions for sexual problems (Jodoin et al., 2011; Stephenson & Meston, 2016). The transition to parenthood is undeniably a life-changing event that new mothers are likely to view as affecting many aspects of their future life. As such, women may be more likely to form a stable explanation for the changes they experience to their sexuality. It is common for women to experience a change in their self-schema after the birth of a child and, more specifically, to report a more family-focused identity (Katz-Wise, Priess, & Hyde, 2010). Indeed, many women report difficulty reconciling their maternal role with their identity as a sexual person and a partner (Sims & Meana, 2010). It follows that stable attributions for postpartum sexual changes, such as “Now that I am a mother I am too tired for sexual activity,” may have negative repercussions for women’s sexual satisfaction. However, these negative repercussions may not extend to women’s perceptions of their romantic relationship more broadly. In the context of postpartum sexuality, mothers who form more stable attributions for their sexual concerns may feel more negatively about their sexual relationship, be less attuned to their own physiological responses during sex, be less sensitive to their partner’s intimate or sexual cues, or be less likely to initiate intimate behavior, resulting in lower sexual satisfaction. Future research should examine these potential mechanisms (Barlow, 1986; Nobre & Pinto-Gouveia, 2008; Rancourt, MacKinnon, Snowball, & Rosen, 2016).
In contrast to our hypotheses, internal attributions were not associated with sexual and relationship satisfaction. Although there is considerable empirical support for the link between greater internal attributions and more negative psychological and interpersonal functioning (Fincham et al., 2000; Mitchell et al., 2011; Péloquin et al., 2017; Shnaider et al., 2014), it is possible that for some women, internal attributions may serve a protective function when coping with postpartum sexual challenges. Indeed, in our exploratory analyses, higher internal attributions appeared to buffer against the link between higher partner responsibility attributions and lower relationship satisfaction. In samples of women coping with a sexual dysfunction (e.g., pain during intercourse, low desire), women with greater internal attributions for the sexual problem reported higher relationship satisfaction (Jodoin et al., 2011; Stephenson & Meston, 2016). While internal attributions may be problematic for some new mothers, for others, stronger internal attributions may create a feeling of control over their sexual relationship and as a result, these women may perceive sexual concerns as less harmful to their overall romantic relationship. Thus, variability in the positive versus negative associations between internal attributions and mother’s well-being could explain the null findings in this study. Future research should consider examining variables such as sexual locus of control (Catania, McDermott, & Wood, 1984) or sexual self-efficacy (Reissing, Laliberté, & Davis, 2005) as potential moderators of the association between internal attributions and sexual and relationship satisfaction. Further, as mothers are the one to bear the physical burden of pregnancy and childbirth, internal attributions for postpartum sexual concerns such as “My body is healing, so my desire for sex is lower right now” may be somewhat normative. Consequently, they may be less likely to lead to affective, cognitive, and behavioral consequences, as compared to stable or partner responsibility attributions.
One unexpected result emerged in this study: Although global attributions were not associated with sexual or relationship satisfaction in our original analyses, after controlling for physical affection, sexual frequency, depressive symptoms, fatigue, and earlier satisfaction, higher global attributions were associated with higher sexual satisfaction. This finding stands in contrast to past research linking stronger global attributions with poorer sexual and relationship satisfaction (Fincham & Bradbury, 1993; Fincham et al., 2000; Shnaider et al., 2014; Stephenson & Meston, 2016). It is possible that after controlling for other factors that contribute to new mothers’ postpartum sexual, relationship, and general well-being, there is a benefit to perceiving the cause of postpartum sexual concerns as something that affects their life globally. It may be that viewing the cause of sexual concerns as something that is not-specific to the sexual relationship (e.g., becoming a parent) may help women to focus on the positive aspects of their sexual relationship and thus maintain higher levels of sexual satisfaction. However, as this association was not predicted, does not follow directly from attribution theory, and appeared only after controlling for several covariates, this result requires replication in future research and should be interpreted with caution.
Strengths, limitation, and future directions
The primarily cross-sectional design of this study limits our ability to draw causal conclusions and did not allow us to control for any sexual concerns that were present prior to the postpartum. It’s possible that preexisting concerns could be driving the association between attributions and sexual and relationship satisfaction. Longitudinal and experimental research is needed to determine the direction of these associations. However, by controlling for earlier levels of sexual and relationship satisfaction (as assessed during pregnancy), we limited the possibility that new mothers who were already in less satisfying sexual and romantic relationships were more inclined to place blame for sexual concerns on a partner or view sexual concerns as more likely to persist over time. The Attributions for Postpartum Sexual Concerns Scale is a novel measure. Despite having demonstrated good reliability and predictive validity in our pilot work and the current study, it would benefit from further validation in broader samples of first-time parents. Further, the measure is comprised of hypothetical situations and we did not assess whether women had experienced each of these scenarios. Although the use of hypothetical scenarios is standard across widely used measures of attributions (Fincham & Bradbury, 1992; Jodoin et al., 2011; Peterson & Villanova, 1988), it would be beneficial to assess women’s attributions for their actual postpartum sexual experiences. We did not include a measure of general relationship attributions, and as such cannot determine whether the results are specific to attributions for postpartum sexual changes. The data were obtained via self-report and are subject to the limitations of self-reports including the possibility of recall and social desirability bias. The sample was fairly homogeneous (i.e., predominantly English Canadian, heterosexual, married, highly educated, high income), which limits our ability to generalize the results to broader populations. Although the sample largely reflected the characteristics of the patients attending the clinic where recruitment took place, future research should engage in oversampling of underrepresented populations (e.g., ethnic and sexual minorities, lower income parents). Finally, we collected data from first-time mothers only. As such, these results may not generalize to women with multiple children or to partners. Partners’ attributions for women’s experiences of painful sex are linked with partners’ own relationship adjustment and sexual satisfaction and women’s severity of pain (Davis et al., 2015; Jodoin et al., 2008). Further, in new-parent couples, the perceptions and experiences of mothers’ and partners’ (e.g., sexual concerns, sexual motives, dyadic empathy) predict their own and their partner’s sexual and relationship well-being (Muise et al., 2017; Rosen et al., 2016; Schlagintweit et al., 2016). Given the interpersonal nature of sexual and relationship well-being, future studies should take a dyadic approach and assess attributions in both mothers and their partners.
Overall, the current study enhances our understanding of attributions for sexual problems in several ways. First, the findings suggest that attributions are an important correlate of women’s postpartum sexual and relationship satisfaction, adding to the existing literature that has demonstrated similar patterns among women coping with sexual dysfunction (Jodoin et al., 2011; Stephenson & Meston, 2016). Second, we demonstrated that the associations between attributions and postpartum sexual and relationship satisfaction were not merely driven by earlier levels of sexual and relationship satisfaction in pregnancy. Controlling for pregnancy levels of satisfaction provides stronger support for the theoretical directional links between attributions and outcomes (Weiner, 1986), which have yet to be demonstrated in the sexual attributions literature. Further, although the data in the current study are primarily cross-sectional, they offer a valuable starting point for investigating the link between attributions and sexual and relationship satisfaction in a novel population (i.e., first-time mothers). Finally, our exploratory analyses found that the strength of the associations between partner attributions and relationship satisfaction varied based on the degree to which women also endorsed internal or stable attributions. Although both the present study and past research have identified partner attributions as a strong correlate of relationship well-being (Mitchell et al., 2011; Péloquin et al., 2017; Shnaider et al., 2014), the current study is the first to our knowledge to suggest that partner responsibility attributions may interact with other types of attributions to predict satisfaction. Future research that examines partner responsibility attributions should test for similar interactions. In addition, as the analyses examining interactions between attributions were exploratory, and our sample size limited the statistical power available to test interactions, we examined only the two-way interactions among the four types of attributions. Future research should explore possible three- and four-way interactions.
Conclusions
In summary, when first-time mothers perceived their partner to be responsible for possible postpartum sexual concerns, or that these concerns were unlikely to change over time, they were less satisfied with their sexual and romantic relationship. These associations remained significant after controlling for physical affection, sexual frequency, depressive symptoms, and fatigue. The current study highlights the importance of partner responsibility attributions, and to some degree, stable and global attributions, in predicting sexual and relationship well-being during the transition to parenthood. Interventions designed to improve the sexual and relationship satisfaction of new parents are modest in efficacy (Pinquart & Teubert, 2010), indicating a clear need for novel empirically supported targets to improve these interventions. For example, educating new parents that changes in sexual well-being are common, and can be temporary, may help to reduce stable sexual attributions and possibly buffer against declines in postpartum sexual satisfaction. Further, clinicians might ask new mothers about the sexual and relationship impact of having a baby, and if mothers report concerns, clinicians could inquire about women’s beliefs about the cause of these concerns. This study highlights the value of examining psychological factors, such as causal attributions, with the ultimate aim of improving the sexual and relationship well-being of women making the joyful, yet challenging, transition to motherhood.
Supplementary Material
supplementary_material - Is it me or you? First-time mothers’ attributions for postpartum sexual concerns are associated with sexual and relationship satisfaction in the transition to parenthood
supplementary_material for Is it me or you? First-time mothers’ attributions for postpartum sexual concerns are associated with sexual and relationship satisfaction in the transition to parenthood by Sarah A. Vannier, Kaitlyn E. Adare, and Natalie O. Rosen in Journal of Social and Personal Relationships
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by funding from the Canadian Institutes of Health Research (RNS-135870) and the Nova Scotia Health Research Foundation (8903) and postdoctoral fellowships awarded to the first author from the Social Sciences and Humanities Research Council and the IWK Health Centre.
Supplementary material
Supplementary material for this article is available online.
Note
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.