
Abstract
Research shows that social isolation and loneliness are important health issues for older adults. This message is increasingly being recognized by policy makers and service providers. Although the concepts of loneliness and social isolation are often discussed and compared with one another, they are largely examined separately, even if they are both included in the same study. In the present article, we argue for bringing together these two related concepts. For example, focusing only on social isolation overlooks differences between those older adults who are socially isolated and lonely versus socially isolated but not lonely. Consequently, we discuss four groups of older adults: isolated, but not lonely; lonely in a crowd; isolated and lonely; and not isolated or lonely. We argue that considering loneliness and social isolation together will aid in the understanding of the social situation of older adults and can provide new directions for research and intervention programs for older adults.
Keywords
In the past two decades, there has been an increased recognition and acceptance of the importance of social isolation and loneliness to the health and well-being of older adults. Importantly, studies have uncovered potential direct (e.g., blood pressure, immune system function) and indirect (e.g., restorative sleep processes) pathways that can explain such connections (e.g., Cacioppo et al., 2002; Hawkley, Burleson, Berntson, & Cacioppo, 2003; Pressman et al., 2005; Theeke, 2010). Perhaps the most strongly worded argument that social isolation and loneliness are public health risks was put forth by Holt-Lunstad, Smith, and Layton (2010), who at the conclusion of their comprehensive meta-analysis of social relationship-related constructs and mortality note:
“Data across 308,849 individuals, followed for an average of 7.5 years, indicate that individuals with adequate social relationships have a 50% greater likelihood of survival compared to those with poor or insufficient social relationships. The magnitude of this effect is comparable with quitting smoking and it exceeds many well-known risk factors for mortality (e.g., obesity, physical inactivity)…. Physicians, health professionals, educators, and the public media take risk factors such as smoking, diet, and exercise seriously; the data presented here make a compelling case for social relationship factors to be added to that list.…Social relationship–based interventions represent a major opportunity to enhance not only the quality of life but also survival” (Holt-Lunstad, Smith, & Layton, 2010, pp. 14–15).
Holt-Lunstad et al.’s (2010) and Holt-Lunstad, Smith, Baker, Harris, and Stephenson’s (2015) observation that social isolation is a health risk factor comparable to smoking is a particularly compelling message. Placing social factors as a health issue has caught the attention of policy makers and service providers working with older adults. An excellent example is the UK’s Campaign to End Loneliness which has galvanized health, government, and nonprofit organizations to take the issue of loneliness in older adults seriously (e.g., Jopling, 2015). In Canada, social isolation of older adults was the topic of the National Seniors Council’s most recent reports (2014, 2017) and the federal government recently supported targeted funding initiatives (Employment and Social Development Canada, 2016).
With increasing recognition that social factors like social isolation and loneliness are health issues for older adults comes the question: What can we do to address social isolation or loneliness? The present article argues that in moving toward developing and refining prevention and intervention efforts, it will be useful to consider loneliness and social isolation together. Before elaborating on our argument, we discuss the topic of definitions, which forms the springboard for our current article and discussion.
Social isolation and loneliness defined
There is a great deal of inconsistency in defining or measuring social isolation (e.g., Holt-Lunstad et al., 2010; Nicholson, 2009; Sabir et al., 2009; Valtorta & Hanratty, 2012; Valtorta, Kanaan, Gilbody, & Hanratty, 2016; Victor, Scambler, Bond, & Bowling, 2000). Definitions and measurement scales include structural (e.g., number of contacts) or functional (e.g., social support) aspects of social relationships, or both; and some draw on subjective impressions of relationships (Valtorta et al., 2016). Valtorta et al.’s (2016) study comparing and contrasting social relationship measurement scales based on dimensions of structural, functional, and objectivity/subjectivity highlights and clarifies some of these discrepancies. For the purposes of the present discussion, we define social isolation as a more objective measure of social relationships such as put forward by de Jong Gierveld and van Tilburg (2006): “Social isolation…has to do with the objective characteristics of a situation and refers to the absence of relationships with other people” (p. 583).
In contrast to social isolation being an objective measure of social relationships, loneliness is typically described as a subjective phenomenon, with one of the most common conceptualization being the discrepancy perspective on loneliness (Dykstra & Fokkema, 2007; Peplau & Perlman, 1982; Perlman, 2004; Pinquart & Sorensen, 2001). This cognitive perspective conceptualizes loneliness as stemming from a discrepancy between the quantity or quality of relationships that people have versus what they want (e.g., de Jong Gierveld, 1987; Perlman, 2004).
Importantly, the discrepancy perspective provides an understanding of how loneliness differs from social isolation and is used to explain the following observations: (1) that a person can be isolated and not lonely; (2) that a person can be not isolated (and even be married and cohabitating and have friends, for example) and be lonely. The discrepancy theory of loneliness would suggest that people may have little contacts or contact (be isolated) but may not feel lonely if their actual relationships (quantity or quality) match with what they want. Further, people with a large number of relationships (not isolated) may be lonely if the quantity/quality of relationships are insufficient to what they desire (de Jong Gierveld, 1987). de Jong Gierveld, Keating, and Fast (2015) recently emphasized the distinction this way, “An individual who is well positioned in terms of objective social participation can occupy virtually any position on the subjective continuum” (p. 2).
Examining loneliness and social isolation together
Many researchers use the discrepancy theory of loneliness to explain and distinguish the concepts of loneliness and isolation, ourselves included (e.g., Newall et al., 2009; Perlman, 2004; Steptoe, Shankar, Demakakos, & Wardle, 2013). But the potential groupings of people characterized by this perspective have not been explored in detail, which we argue is particularly important for the development of interventions. Figure 1 shows the dimensions of social isolation and loneliness together. People at moderate levels of social isolation and loneliness are pictured at the center as potentially “at risk.” Of particular relevance for the present discussion, Figure 1 also highlights the four groupings that result from their 2 × 2 combination: socially isolated and lonely; socially isolated, but not lonely; not socially isolated, but lonely; and not isolated and not lonely.
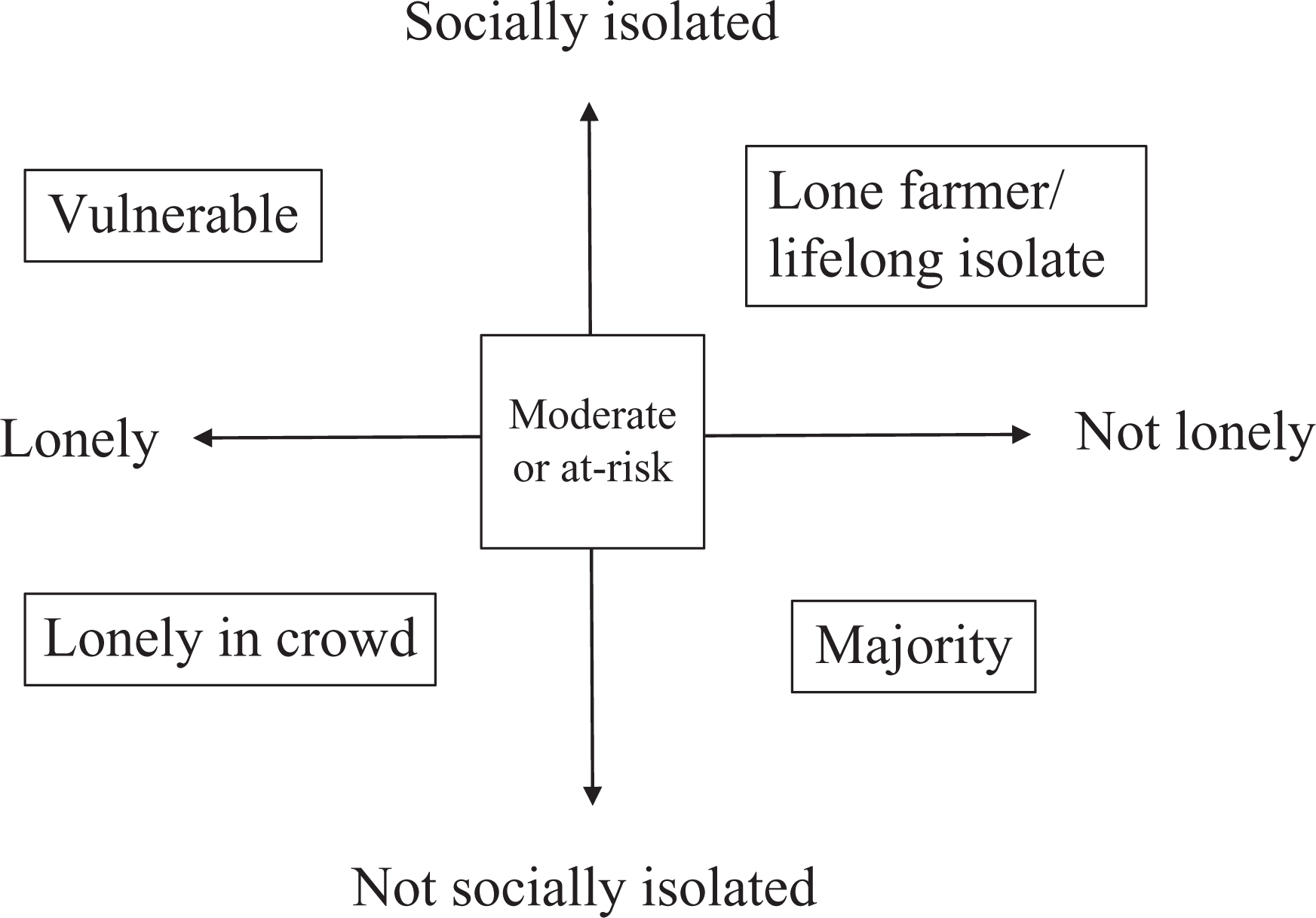
Four groups based on dimensions of loneliness and social isolation among older adults.
As discussed above, the idea that “isolated” people may or may not be lonely is not new (de Jong Gierveld, 1987; de Jong Gierveld, Keating, & Fast, 2015). Other researchers have also drawn attention to the combination of loneliness and social isolation (e.g., Victor, Bond, & Scambler, 2009; Victor et al., 2000; Wenger & Burholt, 2004). For example, Victor et al. (2009) discussed the four groups in relation to their Economic and Social Research Council (ESRC) study, citing comparable studies dating back to 1957 and 1966 (Townsend, 1957 and Tunstall, 1966; cited in Victor et al., 2009). However, there has to date been no systematic discussion and research on how the four groups compare and how they might benefit from different interventions. More commonly, when researchers do consider both concepts in the same study, the focus has been on testing how the concepts are distinct from one another or to show differences in correlates or risk factors (e.g., Wenger, Davies, Shahtahmasebi, & Scott, 1996). Recently, researchers have begun to include both concepts into their studies to determine which might be the more important predictor. That is, studies are comparing the social aspects to see which is the most important predictor of outcomes like health (e.g., Shankar, McMunn, Banks, & Steptoe, 2011), dementia (Rafnsson et al., 2017), and mortality (e.g., Steptoe et al., 2013; Tanskanen & Antilla, 2016).
Although examining the relative importance of the two concepts in relation to a specific outcome measure is important, we would argue that this approach overlooks potential insights that could also be gained by viewing the two concepts in combination with one another. We are not disputing that social isolation and loneliness are distinct concepts and we agree that including both concepts in a study gives a better picture of people’s social world than if only one or the other were considered. However, what we are suggesting here is that researchers sometimes miss the mark and perhaps even add confusion by keeping these two constructs separate. We argue here that going forward with explicitly exploring social isolation and loneliness in combination with one another will provide fruitful insights especially when it comes to the development of interventions.
Importantly for the present discussion, there is a paucity of research to date that has systematically examined whether different groups of socially isolated and/or lonely people may have different needs and may require different interventions. For example, Burholt and Scharf (2014) noted that increasing social contact is often considered the “cure” for loneliness, but that this approach does not consider other facets besides social network size that contribute to an older person’s experience of loneliness. For instance, would someone who is lonely but not isolated be “cured” with enhancing social contact? Considering loneliness and social isolation together (Figure 1) leads to questions like these as well as several other empirical research questions which we present next. Note that, for all groups, we realize the issue of causes of loneliness and/or social isolation is extremely important in helping or intervening. Simply trying to enhance someone’s social network or increase their social activities is not suitable for someone who is experiencing social anxiety as a result or cause of their isolation, for example. But we argue that knowing that someone is socially isolated and/or lonely is an important piece of information in developing interventions.
Four main groups based on loneliness and social isolation
In the following paragraphs, we discuss the four groups as presented in Figure 1. After a general discussion of each group, we discuss future directions in terms of research.
The vulnerable group: Socially isolated and lonely
We begin with the socially isolated and lonely (vulnerable) group (Figure 1), which we name as such because this group has the most vulnerable social profile. According to the discrepancy perspective of loneliness (Perlman, 2004), these individuals are theoretically dissatisfied with their (objectively) very low amount of social contact. Because they are not as socially connected with people or the community, this may be a group that is particularly hard to reach. Moreover, though true of any of the socially isolated groups, at the extreme, people in this group may be so isolated that they might not come to the attention of service providers until there is an emergency (e.g., Molloy, McGee, O’Neill, & Conroy, 2010). From this point of view, there is an urgency in developing ways of reaching and helping this group of potentially “hidden citizens” (Goodman, Swift, & Adams, 2015; Portocalone et al., 2017).
How can past research help describe this group?
There is little known about the risk factors or correlates specific to this group of individuals. In one study, Wenger and Burholt (2004) explored changes in loneliness and social isolation over 20 years (N = 47) and characterized the group who became lonelier/more isolated as being widowed and having deteriorating physical health. Similarly, Cloutier-Fisher, Kobayashi, and Smith’s (2011) qualitative study of the “lived experience” of isolation described an isolated group who were simultaneously struggling with loneliness due to loss of loved ones.
Given that this group is both lonely and isolated, we can also draw on the extensive literature on correlates of loneliness/social isolation. Examining the overlapping and differential correlates of loneliness and social isolation provides an avenue for offering possible distinctions among the four groups. Empirically, the concepts of social isolation and loneliness are not entirely orthogonal but nonetheless have been consistently shown to be only moderately correlated (e.g., Shankar et al., 2011). However, research suggests much overlap between predictors or correlates. Wenger et al. (1996) summarized and examined correlates of loneliness and social isolation and found extensive overlap among them, including sociodemographics (age, living alone, widowhood) and health. Other research has found similar overlapping correlates and including income (e.g., Kobayashi, Cloutier-Fisher, & Roth, 2009; Pinquart & Sorensen, 2001; Steptoe et al., 2013). This pattern suggests that those who are both lonely and isolated may be more likely to be characterized by these characteristics (e.g., older, living alone, widowed, poor health, low income).
Future research questions
This is the most vulnerable of the four groups and may be hard to reach, but, interestingly, it is possible that individuals who are socially isolated/lonely may be the most apt to seek, participate in, and benefit from many types of intervention. This is because these individuals who lack a social network and are lonely might be particularly motivated to enhance their social network (Cacioppo et al., 2006; Qualter et al., 2015). Thus, programs designed to increase social contacts may be especially appealing and suitable for this group. On this note, in discussing social interaction-enhancing interventions, Qualter et al. (2015) stated, “Specific groups of lonely people that might benefit from such interventions, but for whom empirical data are not available, are those who are unable to reconnect because they have few opportunities to engage with others” (p. 259).
Research questions that stem from studying this group include: Are these individuals particularly motivated to get help? What are barriers for these individuals in terms of seeking and obtaining help (health, bereavement after loss, socioeconomic or environmental factors such as lack of transportation)? Are social interaction-enhancing programs particularly beneficial (Qualter et al., 2015)? In extreme or chronic situations, what role might mental health difficulties play in precipitating or perpetuating both isolation and loneliness?
The lone farmers/lifelong isolates: Socially isolated but not lonely
The next group we consider are those who are socially isolated but not lonely (Figure 1). We label these individuals lifelong isolates or lone farmers, as it is not uncommon to hear reports of people who are living by themselves in an extremely isolated situation (like on a rural farmland) who are seemingly entirely content with their social situation (e.g., CBC News, 2016).
We would argue that adding the dimension of loneliness is particularly important in fully understanding this group of socially isolated individuals. From an “objective” level, this group may appear quite vulnerable and therefore in need of help. Based on the present analysis, we should also ask: Are they lonely? If not, then following from the discrepancy perspective of loneliness, by definition this means that they are satisfied with the quantity/quality of their relationships, even if that quantity is extremely low.
How can past research help describe this group?
There is very limited empirical research directly focusing on this group per se. Studies that have indirectly/directly examined this group have characterized these individuals as having retiring and content personalities (Cloutier-Fisher et al., 2011; Wenger & Burholt, 2004), and being childless (Wenger & Burholt, 2004). Cloutier-Fisher et al. (2011) speculated that some isolated adults may have chosen not to replace lost social ties, citing socioemotional selectivity processes (e.g., Carstensen, 2006) suggesting they might keep only a few of the most meaningful relationships (hence have low quantity but highest quality of relationships). Dykstra and colleagues’ work on relationship preferences (Dykstra, 1995; Dykstra & Fokkema, 2007) alerts us to the possibility that lifelong isolates or lone farmers might have stronger preferences to being alone than others (see also Perlman, 2004), suggesting a level of choice.
Indeed, the question of whether older adults are choosing to be alone is particularly salient for this group. Research by Capitanio, Hawkley, Cole, and Cacioppo (2014) is relevant here in which they examined loneliness as an outcome of smaller/greater social network ties and lower/higher perceived choice of daily social interactions among older adults. Results showed that loneliness was highest among those older adults with a smaller social network and a lower amount of choice. Of particular relevance to a discussion of the lone farmer group, results showed that those with a smaller social network but higher choice had “intermediate” loneliness. Results support the idea that a distinguishing characteristic between the vulnerable group (small social network/high loneliness) and lone farmers (small social network/lower or “intermediate” loneliness) may be perceived choice of daily social interactions. Thus, future research should continue to investigate the role of choice. Yet, other factors besides choice may be relevant to this group. For example, from the discrepancy perspective of loneliness, it may also be possible that individuals of this group have lowered their expectations of relationships and contacts (desires) to align with their experiences. Matters are further complicated because what appears a choice on the surface may actually not be one, but rather reflect structural constraints. For example, Portacolone, Perissinotto, Yeh, and Greysen (2017), studying the lived experience of older adults in high-crime neighborhoods, described isolated adults “longing for social integration” (p. 3). These authors challenged conclusions that isolated adults are “choosing” solitude, pointing to socio-structural factors that impede social integration. Indeed, for ALL four groups, the idea of choice in accessing social activities, friends, family, etc., in the context of low income, poor housing, and/or poor access to transport is crucial to consider in developing or assessing interventions.
Taken together, although little empirical research directly addresses this group, we can speculate that those who are isolated but not lonely may have lower preferences to be in relationships (and may be choosing to be alone), have lowered their expectations, or have higher quality of existing relationships that align with their needs (possibly due to selection processes), and/or personality profiles that are more reserved. Portocalone et al.’s (2017) study on impoverished neighborhoods points to socio-structural factors that need to be investigated before concluding people are “choosing” to be alone.
Future research questions
This group may pose a puzzle for service providers or health frontline who see people who are vulnerable due to their social situation but who may not want help (e.g., Newall, 2015). Note that this complexity only arises in the context of intervening around social isolation, not loneliness. This is because, unlike loneliness which is viewed as an unpleasant state, there is a concern with intervening around social isolation that people are choosing—and hence may be content—to be left alone (but see Portacolone et al., 2017).
Given that this group is not lonely and hence theoretically satisfied with their relationships, unsurprisingly, offering this socially isolated group services that increase their network or contact might simply not be suitable and might result in refusal of services. On this note, Cloutier-Fisher et al. (2011) discussed how older adults with a lifelong pattern of isolation may not be distressed at weakening social ties; but rather would be distressed at circumstances (e.g., health declines) that affect their ability to pursue solitary activities. This should not mean that no social services should be offered (as having knowledge of services and choice is important), but that a focus on building social ties might miss the mark for this group. As mentioned previously, the question of whether social isolation is a choice or not is, therefore, a critical one that needs to be examined in future research to better understand this group.
With this said, we know that socially isolated individuals are at a greater risk of health-related problems (e.g., Holt-Lunstad et al., 2010). And if they lack someone in their life who they could call for help (due to an emergency; health situation), this may leave them in a vulnerable situation, regardless of their feelings about their social relationships. For frontline who are encountering isolated individuals or for service providers trying to do outreach, this presents a problem. How to reconcile this situation? Given that social disconnectedness is framed as an important risk factor to health as smoking cigarettes (Holt-Lunstad et al., 2010), perhaps we can return to this analogy: If people know it is bad for their health and do it anyways, what can be done? There has been a lot of energy spent on educating about the risks of smoking; in an analogous way, perhaps more education is needed around the health risks of social isolation.
Finally, it has been suggested that some individuals may be less likely to admit being lonely due to stigma (particularly for males) (Pinquart & Sorensen, 2001). It has also been suggested that chronically lonely people may cope by denying that they are lonely (Cacioppo & Patrick, 2009) or by compensating with other goals, such as materialistic pursuits (Pieters, 2013). 1
Research questions that stem from studying this group include: Would an education campaign designed to show the health value of having a larger robust network have an impact on this group (who may be choosing solitude)? Do individuals have a plan in place in case of an emergency, such as a fall, so that somebody will come to their aid? Are these individuals ultimately choosing to be alone or not (Portacolone et al., 2017; Wenger & Burholt, 2004)? That is, can we determine whether a proportion of “lone farmers” are actually “lonely farmers”?
Lonely in a crowd: Lonely but not isolated
We now turn to the group of individuals who, in contrast to the vulnerable group, are not isolated but are lonely, which leads to the question: Might the loneliness we experience when we feel disconnected or dissatisfied with an existing network of friends and family be especially hurtful?
How can past research help describe this group?
Again we can turn to several lines of (limited) research to help describe this group and to guide future research questions. Some have characterized this group as being likely to be caregivers (e.g., Cloutier-Fisher et al., 2011; Wenger & Burholt, 2004). Others have pointed out that simply having social relationships does not “safeguard” against feeling lonely, as some relationships may provide negative (not positive) support or may even be toxic (e.g., Cloutier-Fisher et al., 2011; Portacolone et al., 2017). Others speculate that culture or norms may influence how relationships are interpreted (e.g., Cloutier-Fisher et al., 2011; Perlman, 2004). In this same vein, Dykstra and colleagues’ (e.g., Dykstra, 1995; Dykstra & Fokkema, 2007) work around partnership preferences may be particularly salient for the lonely in a crowd group. Dykstra and Fokkema (2007) found, in contrast to their expectations, that married individuals with higher partner-centeredness were more likely to be lonely. The authors speculated that very high partner expectations or high reliance on their partners might explain loneliness in the married.
Wenger et al. (1996) noted in their examination of correlates of loneliness and social isolation that loneliness (and not social isolation) was related to some form of loss of relationships or loss in general. Thus, based on this approach, it is possible that this lonely in a crowd group, though they have a large network, may be experiencing loss of certain close or important relationships. Very relevant to this discussion, a recent article examined how loneliness and social network size interact to predict day-to-day (close- and weak-tie) social interactions (Lee & Ko, 2017). Results showed that the relationship between loneliness and lower number of day-to-day interactions with close social ties was only statistically significant for those with a greater social network. Results suggest that it is possible that some people who have a large social network may be lonely because they have invested in quantity of relationships over quality. Taken together, the lonely in a crowd group may be characterized as having reasons they may be dissatisfied with their existing relationships due to such factors as having extensive caregiving duties, having poor quality or even toxic relationships, or having high expectations/preferences for relationships.
Future research questions
Examining this group has particular implications for research examining the structural versus functional or quality (positive/negative) aspects of relationships and their impact on loneliness. A question of interest that has consequences for future research is whether people who already have an existing network (and possibly are caregivers) would benefit from social interaction-enhancing programs? In other words, would social contact be the “cure” (Burholt & Scharf, 2014)? Of particular relevance for the lonely in a crowd group may be feelings of low personal perceived control in terms of accessing their existing social relationships (Cohen-Mansfield & Parpura-Gill, 2007; Newall et al., 2009). Indeed, we would speculate that it is possible that this lonely in a crowd group may be particularly amenable to interventions suggested by Masi, Chen, Hawkley, & Cacioppo (2011) that address expectation and cognitions around social relationships. Another question that arises is whether this group might be facing conflict with family or friends (i.e., existing relationships may be negative or toxic). Finally, it would be of value to study older adults who are institutionalized and presumably have a built-in social network. Although more research is needed, Drageset, Kirkevold, and Espehaug (2011) reported that among older adults who were cognitively intact and living in a nursing home, approximately 56% experienced loneliness often or sometimes. To what extent might people living in an institution be lonely in a crowd? 2
The majority group: Not socially isolated and not lonely
Past research citing prevalence rates ranging between 20% and 40% for loneliness (e.g., Pinquart & Sorensen, 2001; Victor, Scambler, Bowling, & Bond, 2005; Wenger & Burholt, 2004) and 20% (or less) for social isolation (e.g., Kobayashi et al., 2009; Lubben et al., 2006; Steptoe et al., 2013) suggests that the majority of older adults will not be lonely, nor socially isolated, hence the label (Figure 1). Caveats to this conclusion are that at older ages such as 80+, it appears prevalence rates for loneliness could be as high as 50% (Dykstra, 2009). Moreover, less is known of the prevalence of the extremely isolated who are hard to reach (e.g., Portacolone et al., 2017).
What needs to be determined yet is what the prevalence of the majority group is (Figure 1), given that most studies have, to date, examined social isolation and loneliness separately. Based on the ESRC study described in Victor et al.’s (2009) book and two studies cited within (Townsend, 1957 and Tunstall, 1966; cited in Victor et al., 2009), the majority of older adults could be expected to be neither lonely nor isolated. Using a cutoff that included the “moderate” or “sometimes” isolated/lonely into the “neither isolated/lonely” group, results from the ESRC study showed: “majority group,” 69%; “life-long isolates,” 22%; “lonely in a crowd,” 6%; “Vulnerable group,” 3%. Given the paucity of research in this area, it would be important to conduct more research to confirm the prevalence of the four groups, keeping in mind the difficulties in reaching extremely isolated individuals, as well as the complexities of measurement and cutoff point decisions (Victor et al., 2009) as is discussed below.
How can past research help describe this group?
To describe the majority is to again draw on past research on correlates of social isolation and loneliness (as examined separately, not together) like was done for the vulnerable group. This group could be characterized as being married, being younger, having higher education/income, as well as stable or good health, as all of these factors serve as known correlates for both social isolation and loneliness (e.g., Kobayashi et al., 2009; Pinquart & Sorensen, 2001; Steptoe et al., 2013; Wenger et al., 1996). Indeed, though longitudinal research is helping to advance knowledge of transitions or changes in loneliness (e.g., Hawkley & Kocherginsky, 2017; Newall, Chipperfield, & Bailis, 2014), at this point, we still know more about the risk factors of becoming lonely or socially isolated than we know of what it takes to intervene and overcome loneliness/isolation, so ensuring that individuals in the “majority” group stay in that group is the ultimate goal.
Future research questions
Figure 1 shows where on the continuum prevention efforts could be targeted: those who are experiencing moderate levels of social isolation and/or loneliness. Target groups for prevention can also come from known correlates of social isolation and loneliness. As an example, though we know that not everyone who lives alone is lonely, living alone is a consistent risk factor for loneliness (e.g., de Jong Gierveld, 1987). Therefore, a logical target group for prevention efforts are those who live alone who may be moderately lonely or moderately socially isolated (Figure 1).
Future directions and complexities going forward
Above we have outlined some of the research questions that arise in the context of each of the four social isolation/loneliness groups particularly as pertains to future directions in intervention. Obvious points of future directions include tackling some of these questions empirically. For example, do “lone farmers” stay in interventions designed to enhance social networks or do they drop out? Which group might benefit the most from befriender programs? Beyond individual-level interventions, which group may benefit the most from more socio-structural interventions (e.g., transportation, housing)? In addition, further empirical examination of the groups and associated risk factors is warranted. Another avenue of investigation relates to how our typology applies to younger individuals and how people change over the life course. For example, were the “lonely in a crowd” adults lonely even at younger ages?. Such research would also help to address whether the four groups are stable over time or whether and why individuals transition in and out of different groups.
However, it is necessary to acknowledge that going forward with this line of research may be complicated by several factors. That is, several interrelated issues need to be addressed for further research and interventions in this area. First, a pressing issue is: how do we define and measure social isolation? As mentioned previously, a recent review by Valtorta et al. (2016) provides a useful framework for classifying social relationship measurement scales based on structural, functional, and objective/subjective dimensions. Nonetheless, there continues to be a lack of consensus in the literature on how to define and measure social isolation. Indeed, researchers may need to work harder with older adults themselves or with practitioners (service providers, helping agencies, etc.) to better understand what social isolation looks like in all its diversity for the older population (e.g., Cloutier-Fisher et al., 2011). For example, Cloutier-Fisher et al.’s (2011) qualitative work with older adults helps describe how small social networks are experienced and points to looking at life experiences and life histories.
Second, and related to measurement and intervention, more work is needed in terms of determining appropriate cutoffs to identify socially isolated or lonely individuals and in conceptualizing what social aspects should be included in a definition of social isolation and corresponding research scales. Resolving these definitional and measurement issues will help make it possible to have clear cutoffs to distinguish isolated from non-isolated individuals. For loneliness, cutoffs can be done using 1-item subjective questions (Pinquart & Sorensen, 2001; Victor et al., 2005); and de Jong Gierveld and Kamphuis’ scale (1985) has established cutoff values. There are few measurement scales of social isolation that include established cutoffs, an exception being Lubben’s scale (1988). Being able to categorize people as isolated or not becomes important when we try to determine whether programs are reaching target groups of socially isolated. Cutoffs are also necessary in screening for services or unmet needs as well as determining what works in terms of intervention, and for whom. Lastly, being able to examine the groups presented in Figure 1 requires creating these groups in clear ways (Victor et al., 2009).
Conclusion
In this article, we have argued that researchers, like us, are missing how together the two concepts of loneliness and social isolation can help us better understand the social situation of older adults and potentially provide insight on targeted interventions. For example, a person who is lonely but not isolated may have a different health trajectory and may benefit from a different type of intervention than someone who is both lonely and isolated. This perspective has led to a consideration of unique questions that we may begin to address relating to four groups of people: isolated, but not lonely; lonely in a crowd; isolated and lonely; and not isolated and not lonely. Beyond a richer understanding of these groups of individuals, we believe that examining loneliness and social isolation in combination with one another will help bring further clarity to the literature and allow a better understanding of the social situation of older adults and possible health and well-being consequences.
Footnotes
Author contributions
N. E. G. Newall wrote first drafts and both N. E. G. Newall and V. H. Menec worked on the ideas together and wrote the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.