
Abstract
Objectives:
In the current study we used an integrated approach to late midlife sexuality. Using a biopsychosocial approach combined with spillover/crossover theory, we examined various common biological (feeling rested and physical intimacy), psychological (positive and negative mood), and social (giving and receiving support) daily processes linked with actor and partner daily physical intimacy.
Methods:
Data from 191 late midlife, heterosexual, White, couples (97% married, 3% cohabiting) across 14 days were used to examine our hypotheses. Participants had attended some college and about half lived in an urban area.
Results:
Results from dyadic logistic multilevel models suggest that even when accounting for all covariates, physical activity, positive mood, and both giving and receiving partner support were associated with an increased likelihood of daily physical intimacy. Differences in these associations were found for women compared to men.
Discussion:
Physical intimacy in late midlife is likely encouraged from a number of factors. Using simplistic designs may inhibit our understanding of important sexual interactions. When compared to health factors, relational factors appear to be more connected to physical intimacy. Physicians, therapists, and community educators can encourage late midlife couples to pay attention to the support they give and receive which may provide an important environment for sexual interactions.
Although earlier research examining late midlife sexual development has emphasized the need to accept sexual decline as part of the aging process, recent research encourages a more hopeful and integrated approach to late midlife aging (Pruchno & Carr, 2017) and sexuality in particular (e.g., Laumann et al., 2008). Midlife is a time of gains (increased income, freedom from childcare) and losses (health problems, increased erectile dysfunction), but maintaining healthy sexual relationships is associated with physical and social benefits (Galinsky & Waite, 2014). Using the biopsychosocial (BPS) model we respond to a call for a more complex understanding of the intersections of the physical, psychological, and social components of midlife adults (e.g., Laumann et al., 2008), which is needed in understanding sexuality in midlife and late midlife. Although associations between individuals’ physical, emotional, and relational health and sexual health have been examined longitudinally (e.g., Yeh et al., 2006), we know of only limited work that explores the microprocesses (DeWitte & Mayer, 2018), or small daily practices involved in midlife couples’ sexual relationships. Like other research, we broadly conceptualize sexual health as a state of physical, emotional and relational well-being in sexuality (Waite et al., 2017). Additionally, we know of no research that examines late midlife daily sexuality in the context of simultaneous biological, psychological, and social processes.
To address these issues, we positioned this research in late midlife using the biopsychosocial approach, combined with spillover/crossover theory to examine some of the most common biological (feeling rested and physical intimacy), psychological (positive and negative mood), and social (giving and receiving support) daily processes linked with actor and partner daily physical intimacy. Although it is fairly well established that general social circumstances, or BPS factors over longer periods of time, affect levels of sexual intimacy, we examine how day-to-day processes are linked to sexual intimacy. Daily interactions are an important timeframe as they are highly amenable to intervention. We follow the pattern of other research (Leavitt & Willoughby, 2015; Waite et al., 2017) acknowledging participants’ subjective gauge of physical intimacy that may include activities from cuddling to intercourse allowing for gendered and individual differences in norms of physical intimacy within couples. Historically, men and women have often followed different sexual scripts, and these gendered processes may produce different outcomes for men and women (Carpenter, 2010). Thus, this approach may be more inclusive as people consider a range of sexual activities and preferences as a part of their sexual experiences (McPhillips et al., 2001; Waite et al., 2017), which may be particularly salient in late midlife as couples likely adjust their physical intimacy to accommodate sexual dysfunctions like arousal or desire disorder and erectile dysfunction (McCabe et al., 2016).
Examining men’s and women’s experience of physical intimacy in conjunction with biological, psychological and social variables helps individuals, therapists, educators, and researchers evaluate the relative importance of these links. For example, while feeling fatigue on a given day may influence the expression of affection within a relationship, the quality of the couple’s daily interactions may be more influential on decisions to be physically intimate.
Theoretical framework: Biopsychosocial spillover and crossover
The BPS model is a holistic approach that acknowledges the multiple dimensions of influence within a person’s life (Engel, 1977) and helps identify predictors of midlife physical intimacy. Spillover and crossover mechanisms may specifically account for associations between BPS experiences and physical intimacy outcomes. Within individuals, experiences in one domain often spillover to affect other life domains (Grzywacz et al., 2002). From a dyadic perspective, studies indicated that both positive and negative experiences crossover from one partner to the other (Westman et al., 2013). In the current study, biological, psychological, and social factors as experienced by one partner may relate to the other partner’s experience of physical intimacy.
Biological factors: Feeling rested and physical activity and physical intimacy
Early in the development of the BPS model, Engel (1977) recognized biology as a primary component for understanding the circumstances and development of individuals. Although many biological factors may contribute to physical intimacy (e.g., sexual functioning) we focus on two broad biological variables that impact all individuals.
Feeling rested
Feeling rested is regularly addressed as an important element of sexual responsiveness. While getting necessary rest may largely be a biological factor, feelings of restedness could tap both biological and psychological aspects of sleep/restedness (Yorgason, Godfrey, et al., 2018).
Sleep, often connected to feelings of rest, is associated with higher levels of testosterone among older community samples, which is connected to sexual frequency for men (Goh & Tong, 2009) and various aspects of sexual functioning for midlife women (Lee & Tetley, 2019). Partners are also affected by poor sleep patterns. For example, middle to older adult patients treated for sleep apnea not only slept better and experienced improve sexual functioning, but partners’ sexual functioning also improved (Acar et al., 2016). Additionally, there may be important social processes associated with feeling rested. Older individuals whose sleep is troubled report greater negative aspects in their relationships (Chen et al., 2015), which may extend to their sexual relationship.
Physical activity
Like feeling rested, physical activity benefits both mental and physical health and is universally acknowledged to improve sexual health even when other health-related issues are present (e.g., Cormie et al., 2013). Physical activity is broader than exercise, but certainly may include exercise. Physical activity benefits cardiovascular health, mood and positive body image which are linked to physical intimacy (Stanton et al., 2018). However, we are aware of no research that has examine whether an individual’s physical activity is associated with their partner’s physical intimacy. Yet, some research indicated an association between couple’s physical activity and relational well-being (Yorgason, Johnson, et al., 2018). Physical activity provides a mechanism for physical stamina, cardiovascular health, and positive psychological perspectives (Levin, 1993), which is linked to increased desire for physical intimacy (Kukkonen et al., 2007).
Psychological factors: Positive and negative mood and physical intimacy
In addition to biology, we examined individuals’ positive and negative mood, which has consistently shown associations with physical intimacy. Although negative mood (i.e. worry, anger, disgust) likely diminishes feelings of subjective sexual arousal, it may increase their feeling of physiological arousal (Nobre et al., 2004). One explanation for this finding is that individuals may transfer their negative emotional arousal to physical arousal. For example, an individual may have fought with their partner and this negative mood transfers to physical sexual arousal. Other research suggests that high levels of positive mood (i.e. pleasure, excitement, interest) are associated with increased sexual arousal, whereas low levels of positive mood are associated with diminished sexual arousal (e.g., Waite et al., 2017). There is little research on partners’ moods effecting the other. However, one study found that partners of spouses experiencing sexual functioning difficulties also felt more satisfaction with sex when partners presented a more positive mood (Rosen et al., 2004).
Social factors: Emotional support and physical intimacy
The social environment completes the BPS model and accounts for the interactions that individuals have with others. One common social variable is support. We examined both giving and receiving support between spouses across adulthood. Although some actor partner research found older women’s emotional support (e.g., listening, comforting, and reassurance) was associated with older men’s frustration (Carr et al., 2015), emotional support has also shown positive associations with sexual functioning, particularly for women. A study examining midlife adult women’s sexual function, found emotional support was associated with all sexual functioning domains (e.g., Crisp et al., 2015). Moreover, younger men who show more positive emotional partner interactions report more interest in sex (Birnbaum & Reis, 2012). Giving support also may benefit one’s own health as well as provide benefits to their partner from receiving support (e.g., Inagaki et al., 2016). These reflect cohort norms of support and recent research suggests that wives benefit from husband involvement in their daily lives; whereas, sometimes husbands’ perceive wives’ involvement in daily activities as supportive and other times, they perceive it as intrusive (Taylor, 2011). Microprocess of emotional support and physical intimacy are likely reciprocal and may require an examination of smaller daily interactions to disentangle the association (Iveniuk & Waite, 2018).
The present study
We examine the dyadic associations between both husbands’ and wives’ microprocesses of daily physical factors, psychological factors, and social factors and daily physical intimacy among late midlife couples. As there is little work in how daily behaviors contribute to daily physical intimacy, this study is exploratory in nature; however, we propose the following hypotheses: Husbands and wives who report feeling rested and engaged in physical activity will be more likely to report physical intimacy the same day. We anticipate that feeling rested and physical activity will be positively linked with both actor and partner physical intimacy outcomes. Husbands and wives who report greater positive mood will also be more likely to report physical intimacy the same day. We explore the question as to whether negative mood will be associated with reports of physical intimacy the same day. We anticipate that psychological microprocesses will be linked with actor and partner outcomes. Husbands and wives who report higher levels of giving emotional spousal support or receiving emotional spousal support will also be more likely to report physical intimacy the same day. We anticipate that social microprocesses will be linked with actor and partner outcomes.
We control for factors shown to be strong predictors of sexual health, such as age, education, (e.g., Laumann et al., 2008), self-reported physical health (e.g., Lindau et al., 2007), and income (Veenstra, 2013).
Method
Participants were from the Life and Family Legacies Daily Diary study (LFLDD), a subsample of the larger Life and Family Legacies study of 6,729 1966 high school graduates (see Otto et al., 1981). The original sample was surveyed again in 1979/1980, and then again in 2010. Baseline measures included in this study were collected in 2010. For the current sample, married participants in the 2010 wave were selected based on stratification of certain characteristics to ensure variability. Stratification characteristics included rural versus urban residence, healthy versus ill, and veteran versus non-veteran status. Of the 559 late midlife adults and their partners who were invited to participate, 194 couples returned surveys, drawing a 35% response rate. Data from 2 of those couples was not usable, leaving us with data from 192 couples (384 individual participants) who successfully completed the 2011 daily diary study. All but one couple was heterosexual and because same-gender couples (especially in this birth cohort) might experience certain relationship dynamics in meaningfully different ways than two-gender couples. Consequently, this couple was excluded from the current analysis leaving 191 heterosexual couples in the analytic sample.
Participants
The mean age of respondents was 61.82 years (SD = .74), and they had been married on average for around 30 years (Men’s Mean = 30.41, SD = 10.83; Women’s Mean = 29.77, SD = 11.70). Five of the couples were not married, but they were still included as they reported to be in marriage-like relationships. The majority of the sample had some college experience (85%) with an average of 3 years of college. Sixty-five percent of the men were veterans (which is expected since these men were young adults during the Vietnam conflict, with attendant draft, and the sample was stratified by veteran status, and the husbands of women in the sample were sometimes veterans), and 52% of the sample lived in urban areas. All participants initially lived in the Northwestern region of the U.S. and were White, reflecting the demographics of high school graduates in this region in the mid-1960s. Around 50% of the men and 24% of the women in the sample were still working, with 40% of husbands and 50% of wives reporting to be retired. Participants reported to have very good to good health, on average (ranging from excellent to poor). Most couples in the sample lived alone, with less than 20% reporting that more than two people lived in their household. See Table 1 for summary sample descriptive statistics.
Descriptive statistics for the sample by gender of the original study respondents.
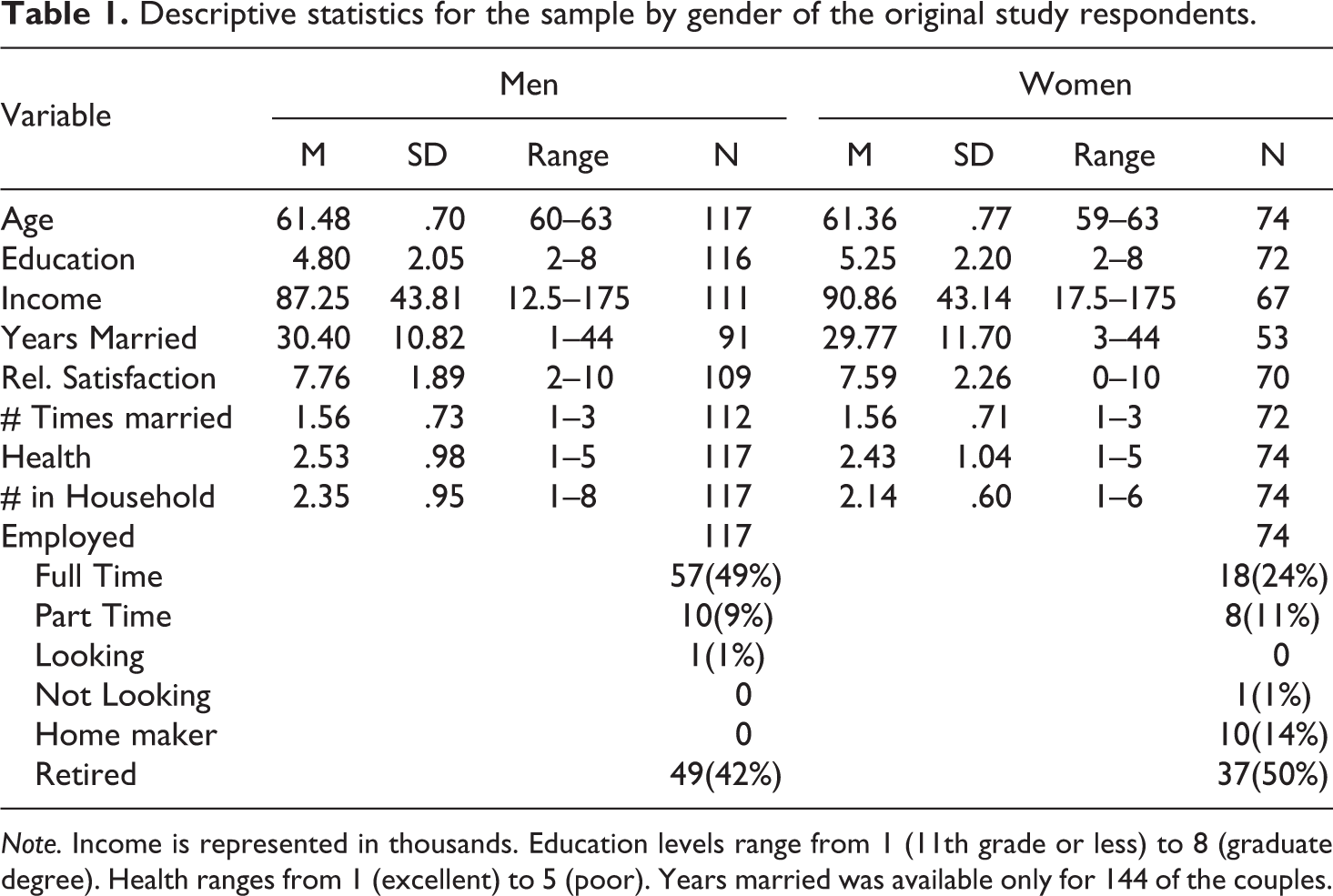
Note. Income is represented in thousands. Education levels range from 1 (11th grade or less) to 8 (graduate degree). Health ranges from 1 (excellent) to 5 (poor). Years married was available only for 144 of the couples.
Procedure
Couples were asked to complete 14 nightly surveys by pencil and paper 30 minutes before bed. Using a successful retention approach, research assistants provided nightly courtesy reminder phone calls to encourage compliance with survey instructions and to answer participants’ questions (see Yorgason et al., 2006). As a result, only three individuals did not complete all 14 days. Each spouse placed their own surveys in a sealed envelope and those sealed envelopes were mailed together to the researchers. Couples received a $50 Visa card for their participation. Human subjects institutional review board approval was obtained at the first author’s institution (IRB #F100229).
Daily diary measures
Biological predictors
To measure daily feeling rested, respondents were asked “How rested did you feel today?” (Penrod et al., 2007). Responses ranged from 1 (“not at all”) to 7 (“very much”), with higher scores indicating feeling more rested. To measure physical activity, participants were asked if they engaged in any physical activity (coded as “1”) or not (coded as “0”) during each day of the study. Respondents subjectively reported on what they did for the physical activity. Given the sample is comprised of community dwelling older adults, it is not surprising that types of physical activity varied widely, ranging from yard work to formal cardiovascular workouts. A small number of respondents reported “sex” as their physical activity (n = 11 men, n = 5 women), yet given that these reports occurred on fewer than 20 out of 2600 days on which physical activity could be reported, these days were included in our analyses.
Psychological predictors
Using a modified version of the Thomas and Diener (1990) scale of positive and negative emotions, respondents were asked to indicate the degree to which he or she experienced each of nine different emotions (e.g., happy, frustrated, worried/anxious, etc.) in the past 24 hours. Responses ranged from 0 (not at all) to 4 (extremely). Positive and negative emotions that were endorsed were respectively aggregated to comprise a positive mood scale (4 items, husbands: α = .89; wives α = .90) and a negative mood scale (5 items, husbands: α = .75, wives: α = .79). Higher scores indicated higher positive and negative mood respectively.
Social predictors
To measure emotional spousal support, participants responded to whether they received emotional support from and whether they offered emotional support to spouses/partners during the past 24 hours (Rafaeli et al., 2008). For example, “In the past 24 hours, to what extent did you
Outcome measure: Physical intimacy
To assess physical intimacy, participants were asked to indicate whether they “shared physical intimacy with [their] spouse/partner” in the last 24 hours (“Yes” = 1) or (“No” = 0). Physical intimacy was not specified for participants but may include activities such as hugging, touching, kissing, and/or sexual intercourse. Although it could be anticipated that reports of physical intimacy are highly correlated between spouses, we allowed each partner’s report to be considered as independent because much like individuals may view intimacy differently, these views may also vary across individuals of the same as well as different genders.
Control variables
We adjusted for 2010 measures of age, income, number of times married, relationship duration, and education in our analyses. Ages ranged from 59 to 63 with a mean age of 61.48 for men and 61.36 for women. To assess income, participants were asked to select which category represented their total household income in 2009. Categories ranged from 1 (less than $10,000) to 15 ($150,000 or more a year). Household income ranged from $12,500 to $175,000 with an average of $87,250. Respondents reported the number of times they had been married. Relationship duration was calculated by subtracting the year of reported marriage by the current year. Approximately 25% of the sample did not report the date of their current marriage, and this was addressed below in the analysis strategy. Education was assessed with 1 item asking “what is the highest grade level or year in college that you have completed?” Responses ranged from 1 (11th grade or less) to 8 (graduate degree). Descriptive statistics for all control variables are reported in Table 1.
Analytic strategy
Our main analyses were conducted using multilevel structural equation models in Mplus, providing a multilevel analysis of daily dichotomous outcomes (Muthén & Muthén, 2017). Models were multilevel in two aspects. First, daily diaries across 14 days involved repeated measures of predictor and outcome variables. Second, because data from men and women are not independent (partner responses are expected to be correlated within couples (see Kenny et al., 2006; Olsen & Kenny, 2006), dyadic outcomes require modeling of individuals nested within couples. With outcomes that are dichotomous, Mplus produces raw logit coefficients. We provide these along with exponentiated coefficients which represent odds ratios of the occurrence of physical intimacy on a specific day of the study given the model predictors. As many of our health and relational variables were correlated, we first estimated separate multi-level logistic models for each key predictor that included both within-person (person-mean centered) and between-person (grand mean centered) predictors for men and women (see Supplementary Material). We modeled groups of biological predictors (see Model 1, Table 2), then psychological predictors (see Model 2, Table 2), then social predictors (see Model 3, Table 2), followed by a model with all predictors combined (see Model 4, Table 2). This approach allowed for some exploration of each construct separately, of biological, psychological, and social constructs in groups, and then as a combined BPS analysis. Within-person variables were calculated by subtracting a person’s mean across days from their daily value, indicating variability from a person’s mean on a given day. Between-person predictors were calculated by subtracting the sample mean from a person’s average value across all study days. It is of note that although control variables were included in all models, none of the control variables significantly predicted physical intimacy.
Men’s and women’s zero-order correlations, means, and mean differences for main study variables.

Note. Men’s values are reported above the diagonal and women’s values are reported below. The diagonal represents correlations between men and women. Sp. Support = spousal support.
* p ≤ .05. **p ≤ .01. ***p ≤ .001.
Minimal data were missing on baseline variables (all <3%, except income missing at 7%, and calculated relationship duration missing for 25%). There were no missing values for daily reports of intimacy, yet some daily measures were missing at <2% for all variables. An examination of data missingness indicated that respondents with missing predictor variables were somewhat less likely to report physical intimacy. To address missing data, models were estimated using multiple imputation with 20 imputed datasets that included all cases.
Results
Preliminary analyses
Bivariate correlations were estimated between individual biological measures (feeling rested and physical activity), psychological measures (positive and negative mood), social measures (receiving spousal support and giving spousal support), and physical intimacy (see Table 3). Paired t-tests between partners on the main study variables showed no significant mean differences between partners for feeling rested or for reports of physical intimacy. However, wives reported higher average levels of receiving spousal support (women M = 1.12; men M = 1.10; t(2554) = 7.67, p ≤ .001) and giving spousal support (wives M = 1.98; husbands M = 1.90; t(2513) = 2.60, p ≤ .01), while husbands reported significantly more days of physical activity (wives M = .62; husbands M = .66; t(2541) = 2.72, p ≤ .01).
Combined multi-level logistic regression models predicting physical intimacy on a given day.
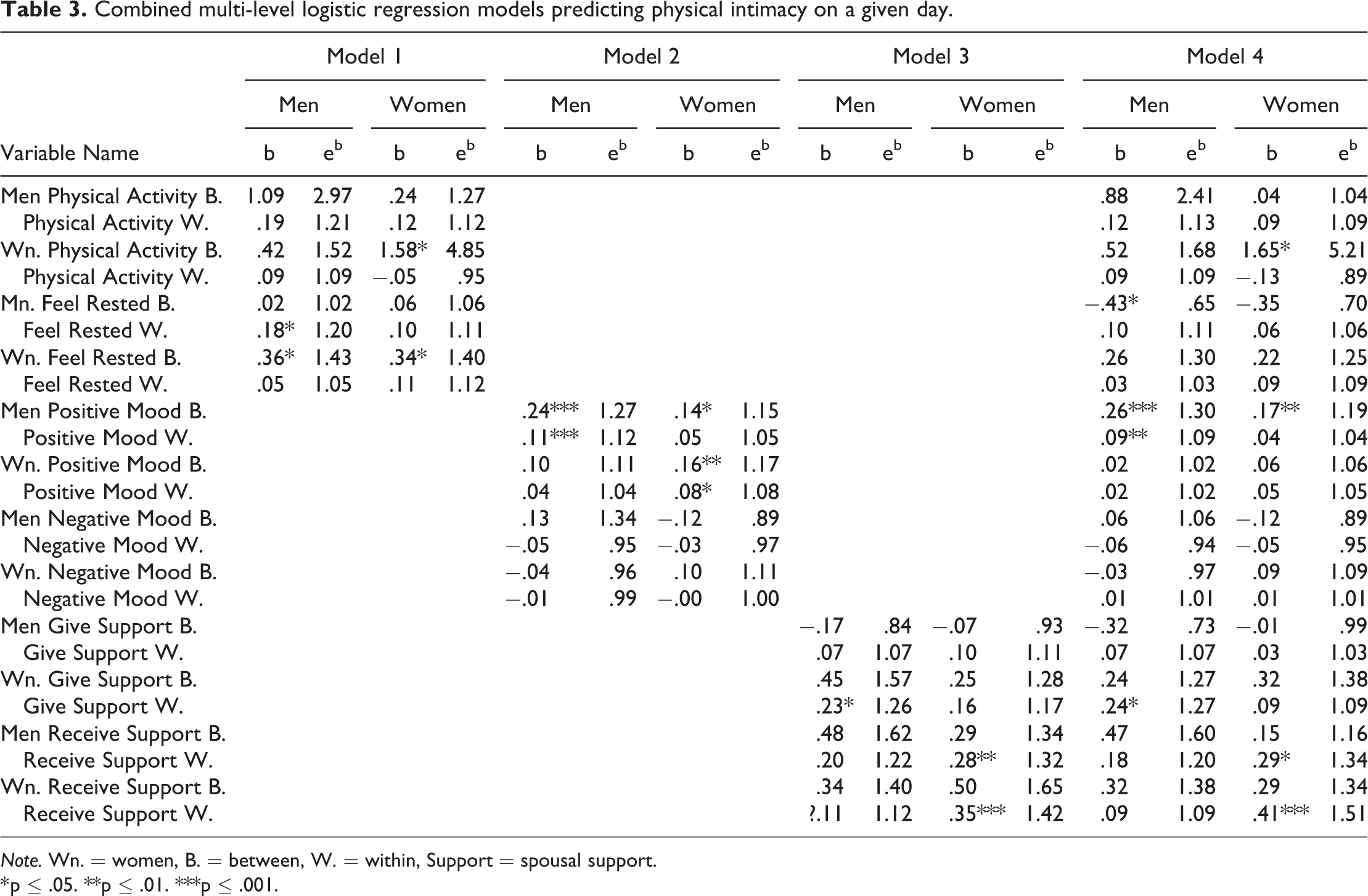
Note. Wn. = women, B. = between, W. = within, Support = spousal support.
* p ≤ .05. **p ≤ .01. ***p ≤ .001.
Full models
We estimated multi-level logistic models found in Table 2, which combined groups of similar predictors of physical intimacy. The first model included only biological measures (feeling rested, physical activity), the second only psychological measures (positive, negative mood), and the third included only social measures (giving spousal support, receiving spousal support). The fourth and final model included all measures together.
Biological predictors
When health behaviors alone were included in the model (see Model 1, Table 2), husbands’ and wives’ higher physical activity across days significantly predicted a greater likelihood of self-reported physical intimacy (husbands between: b = 1.59 p ≤ .05; wives between: b = 1.64, p ≤ .01). Husbands’ feeling more rested on a given day (b = .19, p ≤ .05), and wives feeling more rested across days (b = .42, p ≤ .05) predicted a greater likelihood of self-reported physical intimacy. No other biological predictors were associated with physical intimacy.
Psychological predictors
When psychological measures alone were included in the model (see Model 2, Table 2), husbands’ higher positive mood on a given day and across days were associated with a greater likelihood of self-reported physical intimacy (between: b = .25, p = .001; within: b = .12, p = .001) while only higher husband positive mood on a given day was associated with greater partner-reported physical intimacy (between: b = .18, p ≤ .05). Wives’ higher positive mood on a given day and across days were associated with a greater likelihood of self-reported (between: b = .14, p ≤ .05; within: b = .09, p ≤ .01) physical intimacy.
Social predictors
When relational behaviors alone were included (see Model 3, Table 2), wives’ reporting giving more spousal support on a given day was associated with an increased likelihood of self (b = .20, p ≤ .05) and partner-reported physical intimacy (b = .26, p ≤ .01). Husbands’ reporting to have received higher spousal support on a given day was associated with an increased likelihood of self (b = .25, p ≤ .05) and partner (b = .31, p ≤ .01) reported physical intimacy. Also, wives’ receiving higher spousal support on a given day reported an increased likelihood of self-reported physical intimacy (b = .31, p = .001).
All predictors
In the final model, all biological, psychological, and social predictors were included. Among biological measures, wives’ and husbands’ higher physical activity across days were associated with an increased likelihood of self-reported physical intimacy (husbands between: b = 1.22, p ≤ .05; wives between: b = 1.62, p ≤ .01). Among psychological measures, husbands’ higher positive mood across days was significantly associated with an increased likelihood of self-reported (b = .26, p = .001) and partner reported (b = .21, p ≤ .01) physical intimacy. Husbands’ higher positive mood on a given day was significantly associated with an increased likelihood of self-reported (b = .09, p ≤ .05) physical intimacy. Among social behaviors, wives giving greater spousal support on a given day was associated with an increased likelihood of partner-reported physical intimacy (b = .24, p ≤ .05). Husbands receiving greater spousal support on a given day was associated with an increased likelihood of self (b = .23, p ≤ .05) and partner-reported (b = .28, p ≤ .05) physical intimacy, while wives receiving greater spousal support on a given day reported an increased likelihood of physical intimacy (b = .38, p = .001).
As seen in Supplemental Table 1, two covariates were significant predictors of outcomes in the final model. Specifically, wives were less likely to report daily physical intimacy when respondents reported to have been married more times, and husbands were more likely to report physical intimacy when respondents reported higher marital duration. Also, we calculated the between-person correlation between husband and wife reports of physical intimacy based on output from the final model. Dividing the residual covariance by the product of the square root of the residual variance parameters (or item standard deviations), it was seen that husband and wife reports of physical intimacy were correlated at .76.
Discussion
This study is the first to examine how daily microprocesses from variables in all three areas of the BPS model contribute to the likelihood of late midlife physical intimacy on a given day. Interestingly, both within and between-person factors in each area of the BPS model contributed to physical intimacy indicating the importance of considering other complex variables in late midlife. Even when accounting for other variables, we found that husbands and wives, who engaged in more physical activity across days, were more likely to engage in physical intimacy (Stanton et al., 2018). Similarly, husbands’ higher positive mood on a given day was also associated with their own and their partners’ likelihood of physical intimacy. Wives giving spousal support on a given day benefited husbands’ chances of reporting physical intimacy, and both husbands and wives receiving higher spousal support were linked with an increased likelihood of wives’ report of physical intimacy. In summary, late midlife physical intimacy is a complex interaction and is influenced by how individuals perceive spousal support within the relationship, how they experience physical activity and feeling rested, and the positive mood they feel on a given day.
Biological factors contributing to physical intimacy
Feeling rested and physical activity vary in their contributions to physical intimacy. Although husbands’ feeling rested was significant in the biological predictor model, when other variables were included, husbands’ feeling rested did not contribute to their own or their partners’ physical intimacy on a given day. Spillover theory may help explain these results (Grzywacz et al., 2002). Specifically, although feeling more rested is beneficial when examined in a limited context, in a larger relational setting, other factors such as emotional spousal support may contribute far more to feelings of closeness and connection which then spill over to encourage physical intimacy. However, wives’ and husbands’ daily physical activity were important for the biological predictor model, and for the model with all predictors included. Physical activity may contribute to one’s own physical intimacy for many reasons. Husbands and wives who are physically active may be more in tune with their physical body and sexual needs (Stanton et al., 2018), whether this physical activity involves taking a walk, doing yard work, or a more vigorous cardio workout. According to spillover theory (Grzywacz et al., 2002) such self-care may create an environment where women feel more life balance and/or healthier body image and therefore more connection and activity with their partner.
Psychological factors contributing to physical intimacy
In the psychological predictor model, both late midlife husbands’ and wives’ positive mood contributed to physical intimacy. Previous research indicated that negative mood may or may not contribute to physical intimacy (Nobre et al., 2004;Peterson & Janssen, 2007). We did not find that daily negative mood was significantly associated with physical intimacy. Furthermore, although women’s positive mood contributed to her own reports of physical intimacy on a given day in the psychological predictor model, men’s higher positive mood made a significant contribution to his own and his partner’s report of physical intimacy in both the psychological model and the model with all variables. Although not explored in the current study, this finding may be bidirectional in that men who experience more frequent sex also report more positive emotions (Blanchflower & Oswald, 2004).
Social factors contributing to physical intimacy
We found strong support that social variables contributed to increased likelihood of late midlife physical intimacy, even when accounting for various other factors. Findings from this study indicate that physical intimacy can be predicted by small daily interactions. On days when wives gave spousal support, husbands were more likely to report physical intimacy which is consistent with the spillover theory, in that, men likely feel greater connection with their partner as they create an environment of acceptance, appreciation, or help (Grzywacz et al., 2002). Future research could study these interactions as nested in the broader contexts in which they occur, to better tease out different factors that matter for physical intimacy. For example, daily interactions occur between people and are nested in the broader community that includes social, political, legal, and policy contexts. These contexts may also be connected to physical intimacy and may, in some cases, matter more than dyadic microprocesses. Additionally, gendered sexual scripts must also be examined and better understood in a sexual context. Our findings showed that women reported physical intimacy on days they or their partner reported receiving higher spousal support. Wives reported greater physical intimacy on days when their partners’ emotional needs were met. Women’s sensitivity to men’s emotional need (and not vice versa) may indicate some gendered sexual scripts where women are highly concerned with their partner’s well-being (Sanchez et al., 2006). Men’s likelihood of reporting physical intimacy increased when women reported giving spousal support, but women’s likelihood of physical intimacy increased when they or their partner reported receiving emotional spousal support. It is likely that participants learned and internalized traditional gender scripts from their youth, during an era that was more gender-traditional than today.
One additional explanation of greater couple physical intimacy, when wives give spousal support, is that late midlife husbands may feel less anxiety about engaging in physical intimacy when their partner is emotionally supportive (Perelman, 2003). Women who are aware and accepting of physical changes that occur in late midlife may provide support to enable greater physical and thereby, emotional intimacy. Like men, women who received partner support also reported more physical intimacy. Women may experience this support as relational awareness and responsiveness, which is associated with relational satisfaction (Gadassi et al., 2016)
Limitations and future research
Despite this study’s contributions, there are some important limitations. We were not able to calculate the length of marriage for 46 of the couples in the sample, and so omitted it as a covariate in our main analyses. Due to the initial set-up of the project, basic demographic information from spouses was not obtained. Patterns of physical intimacy might differ for those in long versus short-term marriages, and so this should be considered in future research. Follow-up sensitivity analyses that included relationship duration as a covariate showed similar results to our main analyses, giving confidence that the current findings are robust. Although this study uses daily diary data, we do not suggest this study is causational. For example, men who engaged in physical intimacy with their partner (which might include sex) might find themselves in a better mood as a result and be more willing to accept their partner’s emotional support.
Our measure of self-reported health was a single item and has limited interpretation. Although this measure is correlated with objective health assessments (see Rutledge et al., 2010), it may be that individuals with chronic health problems or sexual health concerns perceive their health as comparatively good, while individuals without chronic health problems perceive their health as comparatively fair. Additionally, our measure of physical intimacy was limited. The 1 item measure was open to the participant’s own interpretation of how physical intimacy was defined, which is not unprecedented (Waite et al., 2017). However, future research could examine specific sexual activities such as hugging, touching, kissing, and sexual intercourse, and their associations with elements of the BPS model. This study had no measures of sexual dysfunction or gender ideology, which would have provided important control variables. Further research could assess objective health, sexual health, sexual dysfunction, and gender ideology, which would increase confidence in related results.
Our sample is entirely White, financially stable, relationally satisfied couples in late life. The sample is select in that couples who participated often involved a veteran that survived military service. Further, participants had been married fewer times than non-responders (t (499.74) = −2.059, p = .04; equal variances not assumed), yet they did not report any difference in marital satisfaction compared to that group (t (557) = 1.545, p = .108). This study may not apply to LGBT adults, minority group members, and individuals living in nursing homes or other institutional settings.
The couples from this sample are part of the Baby Boomer cohort. Specifically, Baby Boomers experienced in their youth and young adult lives secure prosperity, consumerism, social justice movements, and contraceptive options not previously available. As such, the social norms of the 1950s through the 1970s suggest that these individuals may approach sexual intimacy with different expectations that previous or that have followed them (Carpenter, 2010). Findings should be interpreted within this context. Another important caution is the notion that healthy aging may sometimes imply a need to be regularly sexual or put undue pressure on midlife or late midlife adults to constantly strive for improved physical intimacy and/or use medication to enhance sexual performance (Pack et al., 2019). In a culture of medicalized sex, we instead aim to encourage couples to examine interaction patterns within their relationship that may contribute or diminish feelings of intimacy.
Conclusion
Each area within the BPS model contributed to physical intimacy but not equally. Examining daily BPS processes emphasized the complex daily microprocesses of adult physical intimacy. Physical intimacy during late midlife appeared to largely rotate around the day to day emotional and social experiences of husbands and support received by wives. It is important to examine midlife sexuality with a broader lens and evaluate what contributes or detract from sexual experiences. In this sample, participants were financially secure, likely lived in safe neighborhoods, and had reliable health care. This study shows that nuanced variables such as sleep, mood, and support can link to couples’ physical intimacy. Couples who deal with layered stresses may find their sleep, mood, and ability to give or receive support is diminished. More detailed research on midlife physical intimacy is needed.
This research has important implications for healthcare providers, clinicians, and policy makers. Clinicians and educators may find ways to encourage couples to engage in healthy behaviors such as promoting sleep hygiene, mental health awareness, and couple-level support behaviors, which may be more difficult in higher stress environments. In sum, this research provided a foundation for how daily biological, psychological, and social processes experienced by late midlife couples can be important factors in physical intimacy.
Supplemental material
Supplemental Material, Little_things_Supplementary_Material_(1) - Little things mean a lot: Using the biopsychosocial model for daily reports of sexual intimacy
Supplemental Material, Little_things_Supplementary_Material_(1) for Little things mean a lot: Using the biopsychosocial model for daily reports of sexual intimacy by Chelom E. Leavitt, Amber J. Siedel, Jeremy B. Yorgason, Mallory A. Millett and Joe Olsen in Journal of Social and Personal Relationships
Footnotes
Authors’ note
This paper was presented at IARR in 2018.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Veterans Rural Health Resource Center (Western Region VA SLC).
Open research statement
As part of IARR’s encouragement of open research practices, the author(s) have provided the following information: This research was not pre-registered. The data used in the research are available. The data can be obtained by emailing
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.