
Abstract
Collaboration with families and communities has been identified as one of six overarching principles to speech and language therapists’ (SLTs’) engagement in culturally competent practice (Verdon et al., 2015a). The aim of this study was to describe SLTs’ collaboration with families and communities when engaging in practice to support the speech, language and communication of children from culturally and linguistically diverse backgrounds. The study also aimed to identify the benefits and tensions related to such collaborations and to describe opportunities for SLTs to enhance their cultural competence through collaborative practice. The current study drew upon three data sources collected during the ‘Embracing Diversity – Creating Equality’ study: field notes, narrative reflections by the researcher, and semi-structured interviews with SLTs. This study was conducted in 14 international sites across five countries (Brazil, Canada, Hong Kong, Italy and the USA), representing a diverse range of cultural and practice contexts. Cultural-Historical Activity Theory (CHAT, Engeström, 1987) was used as both an heuristic framework through which the study was conceptualized and as a tool for analysis to describe the varied nature of collaboration in different cultural contexts, the benefits of collaborating with families and communities, and the tensions that can arise when engaging in collaborative practice. The results illuminate the importance of SLTs’ collaboration with families in order to gain an understanding of different cultural expectations and approaches to family involvement, and to build partnerships with families to work towards common goals. Collaboration with communities was highlighted for its ability to both facilitate understanding of children’s cultural context and build respectful, reciprocal relationships that can act as a bridge to overcome often unspoken or invisible tensions arising in cross-cultural practice. The findings of this study highlight opportunities for professionals to enhance the cultural competence of their practice through engagement with families and communities.
Keywords
I Introduction
True collaborative practice requires respect, trust, shared decision-making and partnerships (World Health Organization, 2010). Collaborative practice draws upon the combined knowledge, skills and resources of a range of people, working together to achieve the same outcome (Lasker and Weiss, 2003). However, definitions and interpretations of collaboration can vary among different stakeholders involved in collaboration, resulting in divergent expectations and experiences (Chaskin, 2001). This is particularly true when collaborators are from different cultural backgrounds, as culture influences the lens through which people interpret the world and plays an important role in their construction of strategies for resolving problems (Swidler, 1986). For the purpose of this article the term ‘culture’ is defined as ‘the shared, accumulated, and integrated set of learned beliefs, habits, attitudes and behaviors of a group or people or community … the context in which language is developed and used and the primary vehicle by which it is transmitted’ (Kohnert, 2008: 28). Culture is not static and can vary within and between groups and communities. The term culture can be used in reference to the beliefs or practices of a variety of groups, for example, a workplace culture, an ethnic culture or the culture of an individual family. While the combination of multiple perspectives and interpretations of a task can be seen as strengths of collaboration, the negotiation of tensions arising from different expectations is essential if collaboration is to be effective in achieving a mutually agreed upon objective.
1 Collaborative practice in speech and language therapy
In the field of speech and language therapy, collaboration between speech and language therapists (SLTs) and other stakeholders has been highlighted as an essential component of effective practice (American Speech-Language-Hearing Association, 1991, 2007; Royal College of Speech and Language Therapists, 2006). In particular, collaboration with communities and families is identified as a key element for supporting cross-cultural practice (International Expert Panel on Multilingual Children’s Speech, 2012). The ability to engage in effective cross-cultural practice is a requisite skill for SLTs given that the speech and language therapy profession is reported to be largely monolingual, particularly in English-dominant nations, while the populations SLTs serve are increasingly culturally and linguistically diverse (Caesar and Kohler, 2007; Stow and Dodd, 2003; Williams and McLeod, 2012). For the purpose of this study, the term ‘culturally and linguistically diverse’ (CALD) refers to children and families with multiple linguistic and cultural influences or who are not of the dominant language and cultural background of the broader social context in which they reside.
In order to provide appropriate cross-cultural services to families from CALD backgrounds, SLTs need to engage in culturally competent practice. Culturally competent practice is defined as practice that ‘acknowledges and incorporates – at all levels – the importance of culture, assessment of cross-cultural relations, vigilance toward the dynamics that result from cultural differences, expansion of cultural knowledge, and adaptation of services to meet culturally unique needs’ (Betancourt et al., 2003: 294). Cultural competence is conceptualized not as a fixed endpoint that can be attained by professionals, but rather as an ongoing collaborative process of professional development (Verdon, 2015a). Professionals working cross-culturally can enhance the cultural competence of their practice by engaging in self-reflective practice and repositioning themselves from a place of expert to a place of learner (Kearney et al., 2014). Berlin and Fowkes Jr (1983) suggest using the LEARN framework (Listen, Explain, Acknowledge, Recommend and Negotiate) to find common ground to navigate the different explanatory models of health that can be held by practitioners and families in cross-cultural health care practice. In education, Mapp and Kuttner (2013) recommend a dual capacity building framework to enhance partnerships between schools and families. This partnership framework scaffolds effective engagement by supporting professionals to recognize the assets of families as collaborators in practice and to create opportunities for families to negotiate multiple roles in the facilitation of children’s learning (Mapp and Kuttner, 2013).
In the field of speech and language therapy, Verdon, McLeod and Wong (2015a) identify six key overarching principles to guide SLTs’ engagement in culturally competent practice with children and families from CALD backgrounds. One of these six principles is ‘consultation with families and communities’ (p. 18). Working with children within their natural environment in collaboration with families and communities is a key focus in the field of early intervention (Childress, 2004). This is for two main reasons: first, so that intervention can be provided in the daily routines and setting of children’s lives and second, so that families and communities can be involved in the decision-making process around planning and implementing intervention (Hanft and Ovland Pilkington, 2000). However, little has been documented regarding the realities, benefits and tensions of collaborative practice when engaging in speech and language therapy with children from CALD backgrounds. The current study aims to contribute to the literature by investigating collaboration with families and communities in SLTs’ practice with children from CALD backgrounds in a range of different practice contexts from around the world.
2 Collaboration with families
Historically, the speech and language therapy profession was based on a medical model of professional autonomy (Bailey et al., 1992). Assessment, diagnosis and intervention planning were tasks undertaken by SLTs based on their professional knowledge, expertise, training and research evidence. However, in recent decades, a paradigm shift toward family-centred practice has occurred, making the role of families and other stakeholders more prominent (Coufal, 1993). Family-centred practice is based on three key principles: (1) a strengths-based approach rather than an emphasis on deficits; (2) privileging the family’s voice and giving them choice and control over intervention decisions; and (3) the development of a collaborative relationship between parents and professionals (Espe-Sherwindt, 2008).
Families can involve many different people depending on who is actively involved in a child’s life, including, but not limited to, parents, grandparents, siblings and the child at the focus of therapy. Families are the constant in children’s lives and therefore should be acknowledged as experts in their children’s lives (Espe-Sherwindt, 2008). Effective engagement in family-centred practice involves creating collaborative partnerships with families that treat them with dignity and respect, honour their values and choices, and provide support and education to inform choices which strengthen and enhance their functioning as a family (Dunst et al., 2007).
Included in family-centred practice is the need to value the voice of the child in planning and decision-making (International Expert Panel on Multilingual Children’s Speech, 2012). Often when working with children, their autonomy and capacity to make decisions regarding their own lives is overlooked and authority is given solely to the therapist or to their parents (Dockett and Perry, 2011). However, children have the ability to make decisions concerning outcomes of their own therapy and their needs are also to be respected and valued. Article 12 of the United Nations Convention on the Rights of the Child (1989) states ‘Parties shall assure to the child who is capable of forming his or her own views the right to express those views freely in all matters affecting the child, the views of the child being given due weight in accordance with the age and maturity of the child.’
For SLTs, engaging in family-centred practice can be challenging as there is a need to shift from a familiar, therapist-centred clinical focus to creating, negotiating and embedding intervention goals within individual families’ daily routines and settings (Hanft and Ovland Pilkington, 2000). In addition to this, SLTs report many challenges when working with families from cultural or linguistic backgrounds different from their own (Caesar and Kohler, 2007; Stow and Dodd, 2003; Williams and McLeod, 2012). Therefore, the combination of engaging in family-centred practice with CALD populations can be doubly challenging for SLTs as differences in cultural understandings, expectations, routines, priorities and ways of viewing the world can act as barriers to the formation of functional and cohesive partnerships (Harry, 1997).
Of particular significance are the differing cultural expectations of the role of the SLT and the expected level of involvement of families in children’s language development and education (De Gioia, 2013; Huntsinger and Jose, 2009). In some cultures the SLT is seen as a medical professional who should work in isolation to resolve children’s speech, language and communication needs. In contrast, in some cultures the family may be expected to be involved in every aspect of speech and language therapy and its transfer to the home environment. Nevertheless, even in contexts where SLTs report engaging in family-centred ways, parental involvement in service planning and delivery is often limited (Watts Pappas et al., 2008). Therefore, it is important for SLTs to actively seek to include families in goal-setting and intervention planning in order to discuss and establish mutual expectations prior to commencing therapy (Verdon et al., 2015a). Without explicit planning and discussion in regards to service provision, unspoken differences in expectations between SLTs and families can lead to difficulties in effective goal-setting and progression towards positive outcomes for children (Harry, 1997).
3 Collaboration with communities
Forming relationships with communities can assist SLTs in gaining an understanding of the context of a family and the cultural influences upon a family’s participation in society (Verdon et al., 2015b; Zeidler, 2011). Community can be defined both on a basis of geographical location and interconnected relationships (McMillan and Chavis, 1986). For the purpose of this study, the term ‘community’ relates to the broader political, social and cultural context of children’s lives. Depending on the context, this can refer to both children’s geographical surroundings and the community of human relationships in which their lives are situated. People live and participate in multiple political, social and cultural communities, for example, neighbourhood communities, sporting communities or religious communities. Community engagement is recognized for its ability to give a voice to the people of a community and facilitate their participation in achieving health and education development objectives for their own community (Lasker and Weiss, 2003). Consideration of community is particularly important when working with families from CALD backgrounds, as an understanding of children’s cultural context is an essential component of SLTs’ engagement in culturally competent practice (Verdon et al., 2015b).
Services that are developed and implemented in collaboration with communities can benefit communities by offering a safe, convenient and culturally appropriate model to engage with families from CALD backgrounds, whom the literature attests are less likely to access health services (Ball and Lewis, 2011; Peltier, 2011). Reasons found for not accessing health services include a lack of knowledge about services, lack of transport, mismatches between professionals’ and families’ cultural approaches to working with children, and feelings of shame and guilt in relation to disability (Harry, 2008; Maloni et al., 2010; Semela, 2000).
A number of challenges exist to effective engagement with communities (Israel et al., 1998; Peltier, 2011). These challenges include a lack of trust between community members and outsiders, a lack of respect for the community’s cultural ways of knowing and doing, imbalances in power and control, and conflicting perspectives, priorities and assumptions between communities members and professionals (Israel et al., 1998). To overcome these challenges it is recommended that SLTs take time to build relationships with the communities in which they work and be flexible in their approaches to practice in accordance with the needs and desires of a community (Ball and Lewis, 2011; Zeidler, 2011).
Contemporary literature highlights the possibilities for SLTs to engage in culturally competent practice through collaboration with families and communities. However, limited data exist to describe the enactment of cross-cultural collaboration with families and communities in speech and language therapy. Therefore, the current article aims to move from theoretical recommendations to practical examples of, and suggestions for, cross-cultural collaboration by drawing upon data from international practices to describe the realities, benefits and tensions of collaborative practice with families and communities in speech and language therapy. The implications of these findings for SLTs’ engagement in culturally competent practice are discussed.
4 Aims of the current study
The overarching aim of this article is to investigate collaboration with families and communities in SLTs’ practice with children from CALD backgrounds by answering the following research questions:
What are the benefits of collaboration with families and communities in the practice of speech and language therapy with children from CALD backgrounds and their families?
What tensions exist regarding effective collaboration with families and communities?
How can SLTs enhance the cultural competence of their practice through engagement with families and communities?
5 Theoretical orientation
Cultural-Historical Activity Theory (CHAT; Engeström, 1987) was adopted as both a heuristic framework and tool for the analysis of data in this study. Using the CHAT framework, SLTs’ practice with children from CALD backgrounds is conceptualized as a complex system working towards a mutually desired outcome comprising of different but interconnected elements that are in constant tension with each other (as depicted in Figure 1). These elements are identified as the: object (the goal of the activity), subject (the person undertaking the activity), mediating artefacts (tools used to facilitate attainment of the object), rules (codes of conduct governing the activity), community (the context in which the activity is set) and division of labour (other parties involved in undertaking the activity).
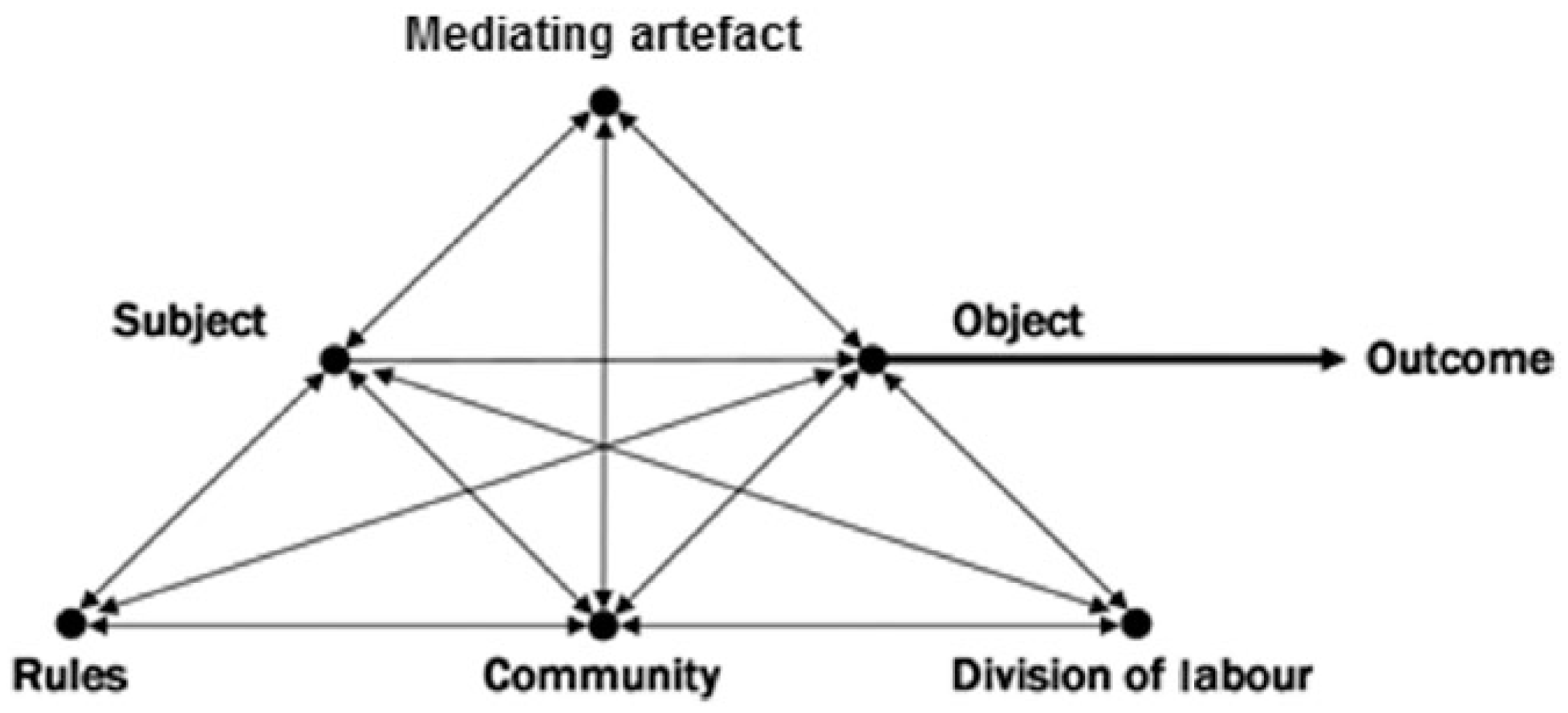
Representation of cultural-historical activity theory.
In examining the system of SLTs’ practice with families from CALD backgrounds, the current study focuses on the elements of community and division of labour to investigate both the benefits of, and the tensions arising from, SLTs’ collaboration with families and communities in their practice with children from CALD backgrounds. Using this systems-based approach to analysis, the interconnected nature of these two elements within the activity system and their impact on the activity system as a whole can be understood.
From a CHAT perspective, the interconnectivity of all elements means that a change occurring in one element of the activity system (e.g., the division of labour among parties involved in supporting children) can lead to a flow on effect of change to the entire activity system. In this way CHAT illuminates the power of the individual to effect change within a larger activity system through small changes to just one element. Thus, if an SLT forms a positive relationship with a family or community in their practice, this has the potential to have a positive impact on practice as a whole. In addition, by considering these two elements in the context of the activity system, the tensions occurring with other elements in the system and thus potential barriers to collaborative practice with families and communities can be identified and explored. A detailed explanation of CHAT and its application to speech and language therapy is provided in Verdon et al. (2015b).
II Method
1 Sites
The current study draws upon data from the ‘Embracing Diversity – Creating Equality’ study of 14 international sites. Each site was engaged in speech and language therapy with children and families from CALD backgrounds. The sites were located in Brazil (n = 1), Canada (n = 2), Hong Kong (n = 4), Italy (n = 1), the USA (n = 6) (see Table 1). Sites were recruited through referral from professional networks and an invitation to nominate sites that engaged in high quality practice with CALD populations posted on online speech and language therapy discussion groups. Identified sites were invited to via email or personal contact to participate. At least one professional in each of the sites was required to be a fluent speaker of English to allow for communication with the first author during data collection. The primary contact in each site was an SLT. Some sites were run by individual SLTs, while other sites involved a team of SLTs and other health and education professionals in a variety of contexts including hospitals, schools, private practice, clinics and community-based services. In many of the sites a diverse range of languages were used both in practice and in the community.
International sites included in the ‘Embracing Diversity – Creating Equality’ study.
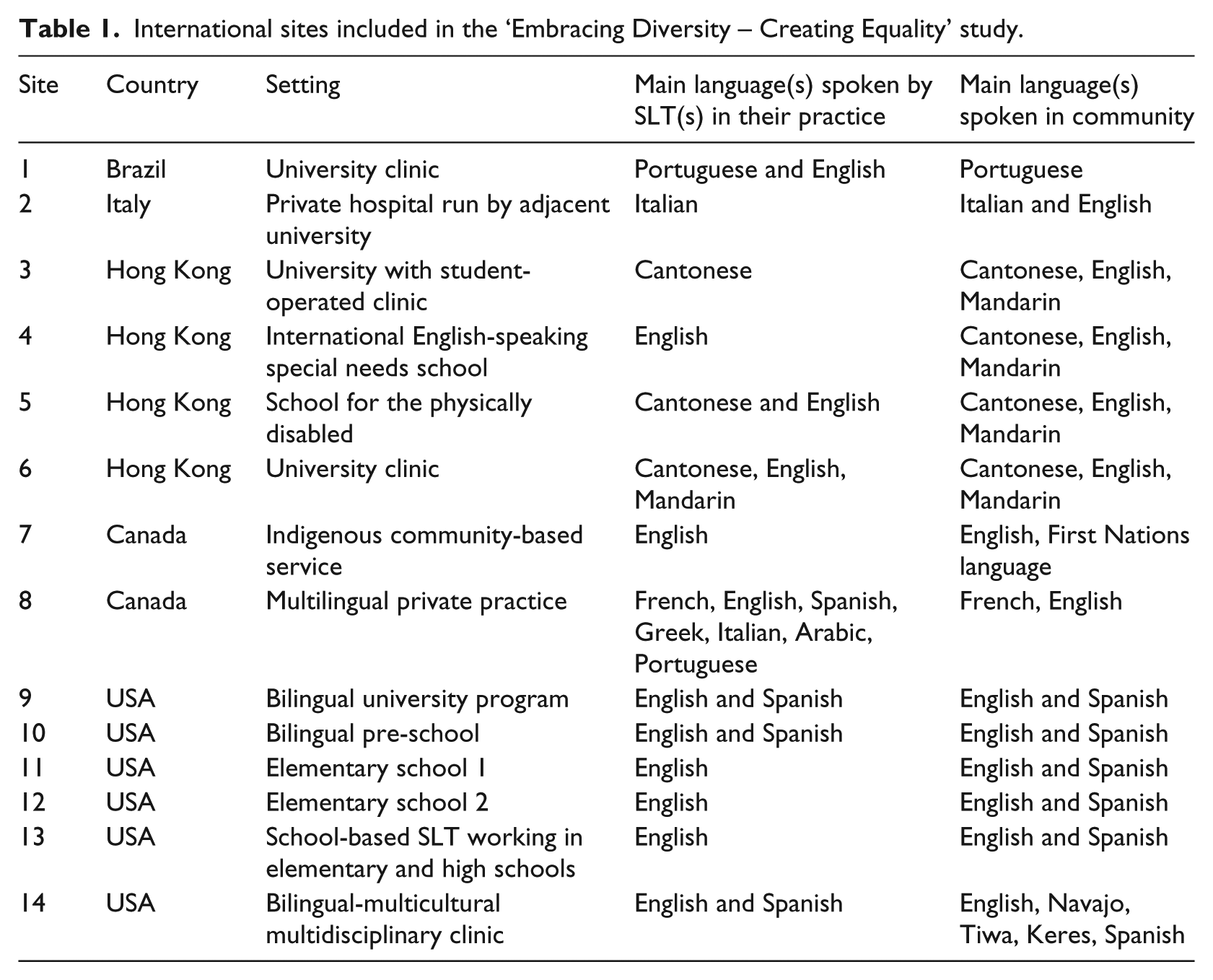
Levels of collaboration with families and communities varied between the sites depending on the setting and broader socio-political context. Sites 1 and 2 involved SLTs working alone with children, with feedback and discussion with parents occurring at the end of sessions. Sites 4, 5, 10, 11, 12 and 13 were all based in school settings and therefore parents were not present during sessions but in some sites were consulted outside of school hours by SLTs. Site 9 was a university-based masters program and no collaboration with communities and families was observed at this site. In contrast, sites 4, 6, 8 and 14 all involved parents during sessions with the SLT. Site 7 was a community-based parent-training program that focused on family enrichment in supporting children’s speech, language and communication development and therefore had a high level of collaboration with both families and communities.
2 Data collection
The data reported in this study were collected as part of the Embracing Diversity – Creating Equality study (for a detailed description, see Verdon, 2015a). Data were collected by the first author who visited each of the sites in the order indicated by the site number. Data collection was undertaken using ethnographic observation of SLTs’ practice with children and families from CALD backgrounds in each of the sites. The first author shadowed the daily activities of SLTs in each site to observe and document their practice with CALD populations. During these observations data were collected in the form of field notes, photographs of sites, activities and resources, videos of therapy techniques, narrative reflections, artefacts collected from the sites and interviews with SLTs, parents and children. The current article draws upon the three data sources from the Embracing Diversity – Creating Equality study in which references to collaboration with families and communities were found, these were: field notes, narrative reflections by the researcher, and semi-structured interviews with SLTs at the site.
3 Data analysis
Prior to commencing analysis, all data were anonymized to protect the identity of participants. Site names were replaced with site numbers and participants were referred to by their site number. While the larger Embracing Diversity – Creating Equality study collected ethnographic data to consider the holistic practice of SLTs with children from CALD backgrounds, the current study specifically draws upon a subset of data pertaining to SLTs’ collaboration with families and communities in their practice. To achieve this, the data were analysed in three phases:
Phase 1: All forms of data were coded into individual CHAT elements (i.e. object, subject, mediating artefacts, rules, community, and division of labour) using NVivo 9 software (QSR International, 2010).
Phase 2: Data coded under community and division of labour were selected as the focus for this article. Data contained within each of these elements were analysed using inductive coding to derive themes relating to collaboration with families and communities.
Phase 3: Tensions and contradictions were identified in the data in relation to SLTs’ collaboration with families and communities.
As the first author collected the data it was also necessary that the first author undertook data analysis to allow for the contextual understanding that was gained from being physically present in the sites to underpin the interpretation of the data (Silverman, 2011). The second and third author also considered the data that were collected, and the second author made suggestions for coding and the identification of themes within selected elements as well as tensions and contradictions between the elements.
III Results and discussion
To facilitate discussion around examples of collaboration found in this study the results and discussion will be presented together. SLTs in the study highlighted the importance of effective collaboration with both families and communities when working with children from CALD backgrounds. Themes identified in the data regarding collaboration with families and communities are presented separately, followed by a discussion of tensions associated with collaboration with each of these groups. While the themes emerged from the entire corpus of data regarding community and division of labour, illustrative examples have been selected to highlight each theme.
1 Collaboration with families
Two main themes were derived from the data in relation to SLTs working collaboratively with families from CALD backgrounds. These were the importance of SLTs:
understanding different cultural expectations and approaches to family involvement; and
building partnerships with families to work towards common goals.
a Understanding different cultural expectations and approaches to family involvement
Expectations and approaches to family involvement in speech and language therapy varied considerably between the sites as a result of different cultural contexts, organizational structures and the needs of individual families. An example given by an SLT in site 6 (Hong Kong) illustrated the way in which cultural expectations can impact upon the success of collaboration with families. The SLT described implementing the same type of therapy, using the same approach to service delivery, with families from two different cultural contexts. In the cases described, one family lived in the USA and the other in China, both were seeking speech and language therapy in their respective home languages (Cantonese and Mandarin). Therapy was conducted via SkypeTM by the multilingual SLT based in Hong Kong. The SLT planned to take a parent-training approach to therapy with both families. The SLT found that the parents in the USA were enthusiastic about taking a lead role in therapy, while the parents based in China had expected a medical-model approach to therapy in which the SLT would take the lead role and the parents would act as observers. The following example demonstrates how a mismatch between parents’ and SLTs’ expectations for family involvement can cause a barrier to engaging in collaborative practice. When the SLT asked the parents from China to implement the therapy tasks, the parents thought that the SLT was refusing to do the work himself because they had not yet paid for the sessions. In an interview with the SLT he explained:
When I worked with the American Asian couple, I think they were more westernised in a certain way, they were happy with doing the therapy … very happy to get their hands dirty very early on and [receive] training … When I was working with … the Beijing parents, and I think because there is a bit of a difference between the cultures, the parents just kept talking about ‘Oh, I need to make sure I pay you money’, [to] which I said ‘I don’t mind’, and I think they felt that I was trying not to interact with the kid too much because they haven’t paid yet [and they thought I was] refusing, stopping therapy because they had not paid yet.
Despite the fact that the SLT spoke the same language(s) as both families, his cultural approach to practice was more aligned with the family from the USA than the family from China. This example demonstrates the important point that a mismatch in cultural expectations can be present even when SLTs speak the same language(s) as the families with whom they are working. Similarly, previous research has found that differences in expectations and approaches to practice between cultures can hinder the development of trust and relationships between families and professionals, and thus impact upon the effectiveness of intervention (Banerjee and Luckner, 2014). Therefore, the findings of this study emphasize the need for SLTs to be aware of different cultural expectations regarding parent involvement, and deviations from such expectations need to be discussed and negotiated to allow families to have input and control over the way in which intervention is implemented (Berlin and Fowkes Jr, 1983).
b Building relationships to work towards common goals
SLTs in the study emphasized the need to build relationships with families in order to work towards common goals. For example, the SLT from site 7 (a First Nations community in Canada) emphasized the importance of listening to parents’ goals and taking them seriously without being judgmental, even if their answers were not what an SLT may expect to hear. She stated:
[SLTs need to] be prepared for the ‘wrong’ answer you know? … Like [not passing] judgment on parents who choose potty training over a communication system … [SLTs may think] oh gee … what? potty training? …
This statement reflects upon the preconceived notions that SLTs may have about the ‘right’ answer when it comes to parents’ goals for their children. It is important for SLTs to recognize that families’ hierarchy of priorities for their children may differ depending on their social or cultural context (Schwartz and Bardi, 2001). The SLT from site 7 stressed the need to value and incorporate parents’ goals for their children into therapy in order to ensure that goals are mutually motivating and can be implemented in children’s daily routines and settings.
Similarly, the SLT from site 6 in Hong Kong described the way in which building a relationship helped to overcome the misunderstanding that had arisen from a mismatch in expectations between himself and the parents from China when trying to conduct parent-based therapy over SkypeTM. He explained:
I had to do a lot of reassurance to mother [to say] the child was doing okay … I think [because] I had a bit more of a conversation with mum, she felt okay about working with me [she understood] the whole idea that we’re actually working for the child rather than all the money thing … and we’re very comfortable now.
This response demonstrates the benefits of open communication and building trusting relationships when collaborating with families to move forward with therapy goals. Similar findings have been noted in previous studies, where the importance of engaging in open conversation as well as listening, learning about the family’s culture and taking time to build trust and respectful relationships have been identified as key to effective cross-cultural collaboration between parents and SLTs (Beverly and Thomas, 1999; Zeidler, 2011).
c Tensions arising in collaborative practice with families
Despite the recognition of its importance, a number of tensions were identified in SLTs’ collaboration with families. The broader social and political context was found to create a tension for SLTs attempting to engage in collaborative practice. For example, school-based SLTs in sites 10, 12 and 13 (situated in the USA) worked in a state where many of the families they served were of a Spanish-speaking background, while the use of Spanish in schools was forbidden under the state’s educational policy. The SLTs commented that while parents did not approach the school to complain overtly about this policy, they knew that it was not always conducive with the parents’ wishes for their children. The SLT from site 10 commented that many parents from Spanish-speaking homes were unable to complete forms that were sent home since the forms were only available in English, and often when parents were asked the main language they spoke at home they said English because they believed that this was the ‘correct’ answer given the political context of the educational system. The language barrier created by this policy made it difficult for parents to be well informed about their children’s speech and language therapy, and it silenced the voices of the parents in these sites, making it difficult for SLTs to engage in family-centred practice.
In some cases, to overcome such barriers, SLTs engaged in what is referred to in CHAT as ‘rule bending’ behaviour (Edwards, et al., 2009: 22) in an attempt to allow parents to make a valuable contribution to their child’s speech, language and communication development. For example, the SLT from site 13 independently sought input from the parents by engaging in home visits to build relationships with parents and to develop goals for therapy together, ensuring that they were functional and motivating. Previous research has found that when SLTs engage with parents in home visits and provide specific coaching strategies, an increase in parental involvement in therapy can be seen among families from CALD backgrounds (Cambray-Engstrom and Salisbury, 2010). Rule bending behaviours such as these demonstrate the power of the individual SLT to work outside the constraints placed on their practice by political or organizational rules which are not in the best interests of the children and families they serve (Edwards et al., 2009). It is important to note that while rule bending can be instrumental in leading to organizational change, it can only take place within reason, and this will be determined by the individual contexts. Ethical implications may arise if SLTs practice outside of their allocated job description, and therefore the level of flexibility that exists within a position can only be determined by the individual SLT.
On the other hand, it is important to recognize that in some cases the tensions identified in the study may have arisen from the families themselves not wishing to take a lead role in family-centred practice. For example, the Chinese family from site 6 expected that the SLT would undertake therapy without parental input. However, due to the fact that services were being delivered via telehealth, the role of the parent in facilitating generalization of skills between sessions was essential to successful therapy outcomes, and therefore negotiation of roles was needed to facilitate the collaboration. Furthermore, students in site 9 learned that parents from an Hispanic background were less likely to be involved in therapy or to question the decisions of SLTs as it was seen as culturally inappropriate to interfere or appear to be rude. Therefore, it is possible that parents from some cultural backgrounds did not want to participate in session despite SLTs’ desire for them to do so. An Australian study of parental involvement in speech and language therapy for children with speech sound disorder revealed that parents had limited involvement in goal-setting and intervention, but that they were satisfied with their level of involvement and in allowing the SLT to be the primary decision-maker (Watts Pappas et al., 2008). Thus, if practice is to be truly ‘family-centred’ the right of families not to be involved also needs to be respected if practice is also to be culturally appropriate. On the other hand, it is important for SLTs not to assume that a lack of involvement by families equates to a desire to not be involved as it is possible that language and cultural barriers may exist that are preventing family involvement.
2 Collaboration with communities
The value of collaborating with the communities of children from CALD backgrounds was highlighted in the study, particularly by SLTs in sites 7 and 14 who engaged in practice with Indigenous communities. Two key themes were identified regarding collaboration with communities. These were the need for SLTs to:
understand the cultural context of communities; and
build respectful, reciprocal partnerships with community members.
a Understanding the cultural context of communities
A key finding from the study was the importance of SLTs’ understanding the cultural context of communities. Collaboration with communities allows SLTs’ practice to be grounded in the cultural context in which children participate on a daily basis (Zeidler, 2011). For example, the SLT from site 7, a First Nations community in Canada, emphasized the importance of gaining an understanding of a community’s history, traditions and teachings and working with the community to align therapy with such teachings. Additionally, the SLT discussed the importance of accepting critical feedback from community members about whether ideas for therapy were culturally appropriate. She gave the example of a parental education program, which likened parent communication styles to local animals and their meaning to the community. She explained the importance of:
making connections with the [community] cultural centre and … looking at [whether] there are traditional teachings that … support [therapy] … I’m looking at … the bear parent, and the bear is the one that’s connected and focused on the kids … I think it’s culturally appropriate … [but] you have to be able to be at a point with the people you’re working with for them to say actually I think that’s a bad example of using the bear, I think we should use something else.
This example raises the importance of cultural humility (Tervalon and Murray-Garcia, 1998) when collaborating with CALD communities. That is, being able to reflect on potential biases that may be unconsciously applied to practice when working cross-culturally and being able to accept that the dominant approach is not necessarily ‘right’ but that there are other ways of knowing and doing (Harry, 1997).
b Building respectful, reciprocal partnerships with community members
A second dominant theme regarding collaborating with community was the need for SLTs to build respectful, reciprocal relationships with community members. The SLT in site 7 described the need to understand how people in the community perceive the role and purpose of the SLT in order to build strong working relationships with communities. She stated: ‘I learned through those years of dealing with parents that they sometimes saw me as the next-door neighbour to a social worker.’ In this quote she meant that parents were worried that the SLT was there to judge their parenting behaviour and report back to the authorities about their children’s well-being. This fear arose for a history of such practices occurring in the community. The fear of being judged made it difficult for parents to open up and trust the SLT in her work.
The SLT in site 7 explained that through spending time and engaging in conversation with the community she was able to gain an understanding of what the community wanted and how to provide a service that was appropriate to their needs: ‘[I realised] I had never asked people what they saw in a health service provider, that was important to them, and … the first thing that came out of a lot of people’s mouths is non-judgmental and I would have never thought that.’ Harry (2008) describes the importance of understanding that perceptions and belief systems are relative to individual experiences. Therefore, if community members have had negative experiences with professionals from outside the community in the past, SLTs need to take time to establish trust and relationships so that practices are respectful to a community’s past experiences and that families feel safe to engage with the SLT (Peltier, 2011).
The examples from the Embracing Diversity – Creating Equality study strengthen the existing literature, which emphasizes the importance of taking time to listen and build relationships in order to engage effectively with CALD communities (Zeidler, 2011). Furthermore, these findings support existing research regarding engagement with Indigenous communities, which highlights the need to shape practices around the suggestions of community elders and members to ensure that approaches are culturally relevant for children and families (Ball and Lewis, 2011; Peltier, 2011).
c Tensions arising in collaborative practice with communities
Tensions were identified in collaborating with the community members to support children’s speech, language and communication in relation to power imbalances in intervention planning and implementation. The SLT in site 7 described a situation where collaboration with a community-based speech and language therapy assistant challenged the practices that were being used by an SLT in the community:
an SLT was in [the community] school and was doing some kind of sequencing test and so put out the pictures of the school bus, and the breakfast, and getting dressed, and asked the child … what did you do when you got up this morning? … [but] it didn’t go very well and the child said nothing … So [the SLT’s assistant from the community] went up to the child after the SLT had left and said ‘so tell me, what did you do this morning, you didn’t want to talk about it’, and the little boy said ‘well I didn’t have breakfast, I slept in my clothes and I turned on the TV and watched it until the school bus came’. So none of those examples were relevant for him. To the community member, that’s a no brainer, but [if consulted] that community member could have explained or, you know, provided some support to help the SLT.
This example demonstrates the potential benefits of gaining insight into different cultural perspectives by working alongside members of the community and how collaboration can act as a bridge to overcome cultural differences between SLTs and the children with whom they work. However, in order for this collaboration to be successful, the role of the community SLT assistant needed to be recognized as equivalent to the SLT so that session could be planned collaboratively before engaging with the child, rather than having the community SLT assistant rectify the situation after the fact. Shared decision-making in the planning of services, as opposed to a therapist-driven model, can assist in balancing the power in collaborative partnerships by giving each person an opportunity to voice concerns and critique existing approaches to practice prior to their implementation in a particular community (Hanft and Ovland Pilkington, 2000; WHO, 2010).
The issue of imbalances in power and control in partnerships with community members was also highlighted by the SLTs in site 14. They described an incident where elders had been interviewed by a woman outside their community to assist in the development of content for a government funded program to support Indigenous children.
It had been her job to interview the elders [in the community], to get their stories and to then … write them down to be used in [the program], she … then went back [and] realised she had been cutting little parts out, because she thought it didn’t relate to the story. As part of that, she came up [with] lots of materials … [that] were inappropriate. [The funding body changed the materials because they had thought] the [tasks the elders suggested] were way too complex for five year olds. And [the elders responded] ‘Our three year olds are doing these’.
This example demonstrates the way in which information and cultural knowledge can be taken from a community, while giving communities little control over how the information is used (Israel et al., 1998). This example also highlights the dangers of making assumptions about what is important, as the true meaning of the elders’ stories were lost by the interviewer selecting the parts she felt were important based on her own cultural lens. In doing so, the interviewer, perhaps unconsciously, showed a lack of cultural humility by giving primacy to her own cultural views over those expressed by the elders in the community (Tervalon and Murray-Garcia, 1998).
3 Collaboration with children
It is important to facilitate children’s participation in decisions that affect their lives, including goal-setting for intervention (Söderbäck et al., 2011; United Nations Convention on the Rights of the Child, 1989). In the context of the UN Convention on the Rights of the Child, Lansdown (2010) defines children’s participation as the right to ‘express views freely and have them taken seriously, along with the other key civil rights to freedom of expression, religion, conscience, association and information, and the right to privacy’ (pp. 11–12). James and Prout (2015) insist that children need to be viewed not simply as products of social processes, but as active players within such processes. Acknowledgement of the agency of children allows for recognition of the role that children play in the reproduction of cultural practices within existing social structures (James et al., 1998). SLTs in sites 6 (Hong Kong) and 8 (Canada) both commented that when working with adolescents, there was consultation with regards to goals and the selection of the language for intervention. However, aside from this, there was little evidence of children being included in decision-making. Söderbäck et al. (2011) reflects on the need to differentiate between applying ‘a child perspective’ (p. 100) to practice, that is an adult’s perspective of what is best for their individual child and applying ‘the child’s perspective’, that is, the child’s own perspectives, beliefs and priorities. The findings of the current study suggest that while some international practices have shifted towards a family-centred approach that incorporates the views of adults, and a child perspective, less is being done to incorporate the child’s perspective in intervention planning and goal-setting.
IV Implications for speech and language pathology practice
Crais et al. (2006) state that ‘the key to providing family-centered services is not to identify the perfect set of practices but to recognize the family’s role in helping decide on those practices’ (p. 365). Therefore, family-centred practice does not necessarily involve families engaging in the enactment of practice, but rather it involves listening to the desires and expectations of families and identifying pathways to practice that respect their views. Regardless of the extent to which families wish to be involved in children’s speech and language therapy, opportunities need to be provided for open and fully informed discussion between SLTs, families and communities (using interpreters and translated materials if necessary) so that expectations of therapy from all parties can be made explicit. Engaging in such conversations with families and communities can help to ensure that practice is culturally appropriate and tailored to the needs of each individual family so that SLTs can move forward in accordance with these wishes.
V Conclusions
The data presented in this study are in keeping with previous research by Dunst et al. (2007) regarding effective collaborative partnerships which highlighted the need to (1) treat families with dignity and respect, (2) honour their values and choices, and (3) provide support and education to inform choices that strengthen and enhance their functioning as a family. The examples drawn from the breadth of cultural and practice settings included in the current study further emphasize the importance of collaboration when working across cultures to assist in the negotiation of tensions that may exist due to different cultural understandings or expectations. While the current study focuses on SLTs, the practical implications of these data are just as relevant for a range of professionals working to support children from CALD families, including educators and child support workers. Each collaborator has the potential to enhance children’s communication and participation in their various contexts including the home, school and community. Therefore, a lack of recognition of the strengths of people involved in children’s lives (including children themselves) can deny a child an important and unique contribution to their development. Further research would be beneficial to consider the value of collaboration from a broader range of perspectives including families, communities and children. It is acknowledged that the types of collaboration used to support children’s speech, language and communication will vary depending on the social, cultural and political context of practice, and that the data presented here provide only a few examples of the highly diverse and complex contexts in which SLTs practice. However, this article provides an overview of the importance of consultation with families and communities, a critique of the enactment of collaboration in different international contexts, and the potential benefits and tensions of collaboration that can arise in SLTs’ practice with children from CALD backgrounds. The findings of this article provide examples of how respectful, reciprocal working relationships with families and communities can enhance the cultural competence of SLTs’ practice by facilitating the development of culturally appropriate, mutually motivating goals to support the speech, language and communication needs of cultural and linguistically diverse children.
Footnotes
Acknowledgements
Sarah Verdon acknowledges support from a scholarship from the Australian Department of Education and the Research Institute for Professional Practice, Learning and Development and an Excellence in Research in Early Years Education Collaborative Research Network scholarship from Charles Sturt University, Australia. Sarah would like to thank the participants in this study for their hospitability, generosity of ideas, and for the contribution they have made to the profession by sharing their experiences. Sandie Wong and Sharynne McLeod acknowledge the support of the Excellence in Research in Early Years Education Collaborative Research Network.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.