
Abstract
In most African states, the majority of the population depend on indigenous healing knowledge for their healthcare. This knowledge is in danger of being obliterated due to a number of factors such as it being not documented, low life expectancy where people die before transferring it to the next generation and the governments failing to incorporate it into the mainstream health system that is often overloaded. This qualitative study adopted a hermeneutic phenomenology to investigate the development of a framework to integrate knowledge of traditional healing into the mainstream healthcare system in the Limpopo province. Data were collected through interviews with traditional healers chosen through snowball sampling technique augmented by observations and analysis of legislation, notes, records and other forms of documents held by healers. Data were analysed and interpreted thematically according to the objectives of the study. The study established that indigenous medical knowledge is marginalised, and healers are not getting support from the government despite the important role they play in the national health systems. Traditional healing is not properly regulated creating a loophole for anyone to practise as a healer. A framework that points the link factors that attempt to create an understanding of how knowledge of traditional healing can be managed and integrated into the mainstream healing is proposed. It is concluded that failure to recognise traditional healing and integrate it in the mainstream health system will continue to hamstring the health system with resources in South Africa.
Keywords
Introduction and background to the problem
Traditional medical knowledge through the use of plants and herbs is indigenous to Africa’s healthcare system. This practice is as old as mankind and is used across the globe, particularly in third-world countries. Traditional medical knowledge consists of the collective knowledge, skills, experiences of healers and knowledgeable people in a community. This knowledge has safeguarded the health of indigenous communities for centuries. According to Poorna, Mymoon and Hariharan (2014), the World Health Organization (WHO) report estimated that 70% to 80% of the population in developing countries depends on traditional medicines for their primary healthcare needs. People in the cities possibly make more use of western medicine than those in the rural areas, because they have easier access to hospitals. However, there is a change in the demographics as townships are now closer to the cities, which makes healers more accessible to the city people, while the government is striving to provide western medical health care to rural communities by providing them with clinics.
Adekannbi, Olatokun and Ajiferuke (2016) suggest that traditional healing is usually the first choice for primary health care by rural communities in developing countries. There may be a number of reasons for this, ranging from trust and affordability to proximity. However, Popat et al. (2001) argue that there is a mythical, yet predominant view that herbal medicines are harmless and free of side effects because they are natural. Moodley, Sutherland and Oulanova (2008) opine that: ‘while the need to seek traditional healing is embedded in a cultural paradigm of cure seeking; the appeal for traditional healing is also based on the holistic nature of traditional approaches which seek to restore harmony and balance within the individual and between the individual and his or her environment’.
Mathibela, et al. (2015) argue that the South African government’s healthcare system in itself has negatively influenced the practice of traditional healing, as patients consult government health centres before turning to traditional healers. Some doctors in those hospitals discourage patients from using traditional healers for health reasons. Similarly, some religious leaders (mostly Christians) label traditional healers as evil and consistently discourage their members from consulting them. Children grow up not understanding what traditional healing is about and continue to transfer the stigma that is attached to traditional healing. They are led to believe that traditional healing is a dirty job, done by the poor and only in rural areas. As a result, knowledge of traditional healing is disappearing because of a lack of interest.
The problem is compounded by media reports of traditional healers claiming to have a cure for AIDS or submitting their patients to dangerous or ineffective treatments. Stories are also appearing in the news about suspected killings linked to healing and traditional healers, where it is believed people are killed for their body parts for healing purposes. Such stories make matters worse for indigenous medical knowledge in third-world countries, especially Africa. Indigenous medical knowledge is now gradually facing extinction as the younger generation is not interested in it. Furthermore, indigenous medical knowledge is not integrated into the mainstream health system in most African countries, including South Africa (Maluleka 2017). This study is therefore aimed at developing a framework for integrating indigenous medical knowledge into the mainstream healthcare system in in the Limpopo province of South Africa. The specific objectives were to: evaluate the regulation of traditional healing in the Limpopo province of South Africa identify issues impeding traditional healing practice in the Limpopo province of South Africa assess level of collaboration between traditional healers and Western doctors suggest a framework for integrating traditional healing into mainstream health system.
Literature review
Regulation of traditional healing in South Africa
The fall of the apartheid government brought with it many changes and had a direct influence on traditional African practices. The South African government post-apartheid recognised a person who uses indigenous medical plants for healing as an indigenous healer (Sodi et al., 2011:101). The government also passed into law the Traditional Health Practitioners (THP) Act, No. 22 of 2007, which regulates the activities of indigenous healers. The Act states that “traditional healing means the performance of a function, activity, process or service based on a traditional philosophy that includes the utilization of traditional medicine” (Government Gazette, 2008). Traditional healers were now free to practice and were protected by law.
The purposes of the Traditional Health Practitioners Act of 2007 were: to establish the Interim Traditional Health Practitioners Council of South Africa (THPCSA); provide for the registration, training and practices of traditional health practitioners in the Republic; and serve and protect the interests of members of the public who use the services of traditional health practitioners. The Act applies to traditional health practice in South Africa and to the traditional health practitioners and students engaged in or learning traditional health practice in the Republic (Government Gazette, 2008).
According to Tshetlha (2015), the interim Traditional Health Practitioners Council, which is responsible for regulating and controlling traditional health practice, was inaugurated in February 2013. In May 2014, the sections of the Traditional Health Practitioners Act that give it full powers came into effect. The purposes of the Traditional Health Practitioners Act were: to establish the Interim Traditional Health Practitioners Council of South Africa; to provide for the registration, training and practices of traditional health practitioners in the Republic; and to serve and protect the interests of members of the public who use traditional health practitioners. The Act applies to the traditional health practice in South Africa and to the traditional health practitioners and students engaged in or learning traditional health practice in the Republic (Government Gazette, 2008).
The government has established the Traditional Healers Council and one of its functions is to approve minimum requirements for the education and training of traditional health practitioners, in consultation with the relevant departments, quality assessment bodies or a body of traditional health practitioners accredited by the council. However, there is no agreement between the council and some of the professional bodies. An example is the statement by the leader of the Traditional Healers Organisation (THO), Nhlavana Maseko, in 2012, when he said that members of his organisation do not want to be integrated into the Ministry of Health because traditional medicine existed long before western medicine was introduced in the country; instead they want to work in collaboration with it, but independently (Traditional Healers Organisation, 2012).
The THPCSA has not done much in carrying out its mandate of regulating and registering traditional healers (Maluleka, 2017). Most of the healers were registered by associations that existed prior to the establishment of the THPCSA, such as the Traditional Healers Organization (THO), the African National Healers Association, the Association of Traditional Healers of Southern Africa, the Congress of Traditional Healers of South Africa, the African Dingaka Association and the African Skilled Herbalists Association (Freeman and Motsei, 1992; Kale 1995). which are operating independently. These associations have their downside because at times registration is done without proper verification as to whether the healer received training or not. Traditional healing thus remains exposed to exploitation by fraudsters because it is easy to practice as a healer.
Collaboration between western doctors and traditional healers
Colonialism and apartheid had an impact on the way western doctors and traditional healers view one another. According to Mokgobi (2014:24), many South Africans are still divided between Western and African philosophies. These divisions are mainly on issues like gender, religion, medicine, ceremonies and many other practices that are unique to Africa. This makes South Africa unique because it consists of diverse cultures and beliefs. Mbatha et al. (2012) highlight that in some provinces in South Africa, the health departments have created a position of traditional medicine manager, who oversees collaboration and encourages two-way referrals of patients between government hospitals and traditional healers.
In Limpopo province, there is some evidence of collaboration between traditional healers and western doctors in different regions between healers and government hospitals. Collaboration is very important in a province like Limpopo, considering the number of rural communities where cultural practices such as traditional circumcision are highly practiced. When it comes to circumcision, which is a traditional practice in South Africa, collaboration between western doctors and traditional doctors takes place in some of the hospitals in Limpopo and other provinces where western doctors do health checks on the initiates before they are sent to the mountain, which will reduce the number of fatalities. Initiates can only be circumcised in the hospitals in a safe environment, where care is taken to reduce infections and the spreading of diseases. However, Mokgobi (2013) warns that collaboration between western hospitals and traditional healers will be biased and might always favour western medicine. In this regard collaboration may not be simply a spreading of health care, but “may be a paternalistic way of making the clients of traditional healers available to western interventions” because traditional healers become more involved in first-line health ‘on behalf of’ scientific medicine, so the modus operandi and the ‘culture’ of traditional healing are likely to be undermined (Mokgobi, 2013).
Mngqundanisoa and Peltzerb (2008) suggest that traditional healers believed that western practitioners undermined their work. They argue that while mutual referral of patients appears to be fair, the reality is that it favours western medicine and this is not likely to change. Summerton (2006) opines that western practitioners lack knowledge about traditional theories of disease and health. This causes mistrust between the two sides. While some traditional healers feel undermined by the western practitioners, some western doctors feel that traditional healers are putting the lives of patients at risk.
Issues impeding traditional healing practice in South Africa
A number of issues impede the practice of traditional healing in South Africa. There are always negative reports in the media about traditional healers and it is impossible to tell whether fake traditional healers are the ones responsible or not, because it is impossible to differentiate between bogus healers and legitimate healers who received proper training. The country is struggling to establish the correct number of healers currently practicing, because healers are scattered and registered by non-statutory associations and their numbers are not consolidated anywhere. There is also a huge number of healers who are not registered with any association and only deal with patients on a daily basis. The THPCSA is mandated to consolidate the numbers and develop a database of traditional healers, but that is proving to be difficult because of the current state of traditional healing. Truter (2007) estimates that South Africa had approximately 200,000 practicing traditional healers in 1995 and around 300,000 in 2005. The number is expected to have risen significantly because those figures are not current and the lack of proper regulation makes it difficult to provide an up-to-date figure. According to Tshetlha (2015), the Traditional Health Practitioners Council does not seem able to deliver satisfactorily on its mandate yet. One reason is the difficulty the council is likely to face in differentiating between credible practitioners and bogus ones for registration.
Integrating traditional healing into mainstream health system
The South African health system is under tremendous pressure in terms of human resources and finance, among other things. The pressure has been increased by the burden of disease, fuelled by a range of risk factors, including unsafe sex and sexually transmitted infections, interpersonal violence and alcohol abuse. Despite the South African Department of Health being among the top departments that receive a bigger slice of the country’s budget, it is struggling to provide adequately for all citizens of the country. Nevertheless, traditional healing, which is said to be the first-choice primary health care in third-world countries, is still not adequately explored to help with the country’s health problems and South Africa is not maximising the opportunities that are available. Traditional healing has the potential to benefit the country economically, especially if the sector is integrated into mainstream healthcare as traditional healers would be paying tax (Maluleka, 2017). This can also benefit traditional healers as they will also receive proper support from the government.
Hybrid use of western and traditional medicine is necessary because there are patients who may need assistance from either side. For example, the results of the study by Bopape, Mothiba and Malema (2013) suggest that illnesses such as hlogwana 1 , themo/lekone 2 , makgoma 3 , sekgalaka 4 and sephate 5 are known to be cured by traditional healers in Limpopo. Most hospitals never consider sending patients with such illnesses to healers, resulting in healers indicating that collaboration is one sided because they (healers) are always referring patients to the hospitals when faced with illnesses that they don’t understand while hospitals never refer patients to them even when they know which illnesses they are facing are commonly cured by traditional healers. A positive collaboration was an agreement signed between the South African Department of Health and the Congress of Traditional Leaders of South Africa (Contralesa) whereby western doctors would help traditional initiation schools with pre-circumcision screening, circumcision and after-care (Brand South Africa, 2014). This was aimed at reducing deaths and injuries associated to traditional initiation schools.
Research methodology
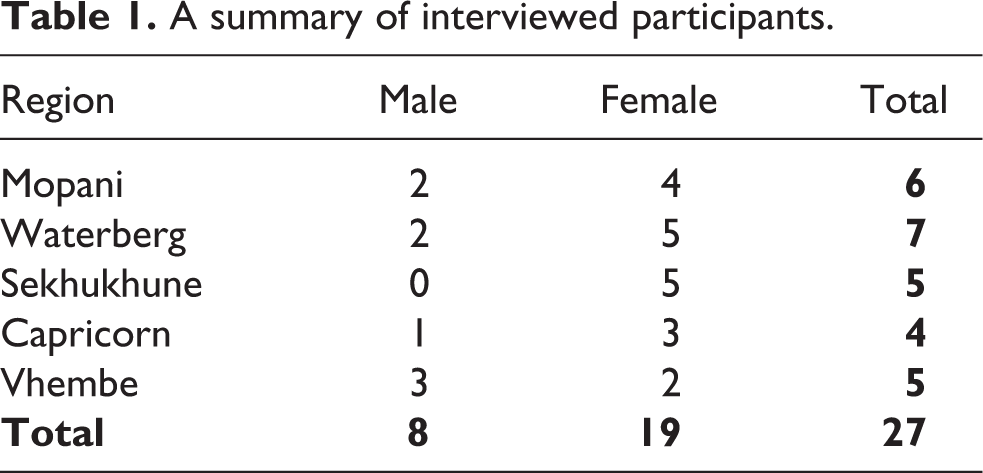
This qualitative study adopted the hermeneutic phenomenology method because it investigated the lived experiences of traditional healers who share similar experiences in their practice of traditional healing. Data were collected through interviews augmented by observations and analysis of legislation, notes, records and other forms of documents held by healers. The snowball sampling technique was employed because of the nature of the population being investigated. Data were collected until saturation was reached. To ensure authenticity, the investigators went back to some of the healers and shared with them what was captured and allowed them to make further comments. This allowed the investigators to have continuous discussions with healers and that gave the investigators some leverage to interpret what the traditional healers have contributed. In total, 27 healers were interviewed, 19 of whom were female and eight were male. All these were from the five regions of the Limpopo province in South Africa, i.e. Waterberg, Sekhukhune, Capricorn, Vhembe and Mopani (See Table 1). Interviews were conducted in Tsonga, Venda and Pedi and the answers were translated into English during transcribing. The interview schedule was tested with two traditional healers. It was realized during the testing that the questions would not be asked in a sequence as the flow of discussions during interviews determined which questions were asked and which ones to leave out so that there were no interruptions. The investigators listened to the recorded tapes from the interviews and transcribed them from tape to paper while translating them into English. The data were grouped according to each theme emanating from the objectives of the study. A similar approach was taken to data collected through observation and document analysis.
A summary of interviewed participants.
Each interview participant was informed as to who was conducting the research, why they were invited to participate, that participation was voluntary and they were free to withdraw anytime, and that anonymity and confidentiality would be maintained at all times. For data collected through observation, permission was granted by the senior healer, who was responsible for the training of the healers, after consulting with the trainees. For anonymity, participants were assigned letters such as Participant A.
Findings and discussions
The findings are presented as per the objectives of the study.
Regulation of traditional healing
Traditional healing is regulated through the South African Traditional Health Council in South Africa. Some of the core functions of the Council worth highlighting, include ensuring the efficiency, safety and quality of traditional health care services, and providing for the management and control over the registration, training and conduct of practitioners, students and specified categories in the traditional health practitioner’s profession. However, despite the existence of the Council, some associations with no statutory status are registering traditional healers and somehow play a regulatory role to the healers. This was confirmed from an analysis of certificates which were found in possession of the healers that participated in the study. Associations that were doing the registration for healers in Limpopo, included: Traditional Healers Organisation, African Dingaka Association, Natural Dingaka Herbal Medupe Association, Dingaka Herbal cc and Mbofho Traditional Doctors Association of Limpopo Province in South Africa. Of the 27 healers’ investigated, 24 were part of associations and some were in possession of more than one certificate.
The certificates only contain signatures of the association leaders and no evidence of where the certificate holder received his or her training. Participants mentioned that they had to deposit money in the association’s bank account and then they received their certificates without any form of testing and verification. In other words, they were not requested to produce proof of training. All the certificates examined from the above mentioned associations had no evidence of where the training was done. None of the certificates had the signature of the person who provided training. This situation has the potential to open doors for fake healers who can easily apply for and receive these certificates without any hassles. This is compounded by the fact that one participant (I) indicated that ‘patients do not worry or care whether a healer is certificated or not. Most patients trust traditional healers due to referrals from families or friends.’ Participants believe such associations can help when there is a dispute with the trainees or when patients are not paying after being treated. However, no participants indicated ever using the services of the associations they belonged to. Participant D indicated that he joined the association mainly for certificate and to use it as insurance in case he is in trouble with authorities regarding administration of medication to patients. The other reason for joining cited by Participant H is “the need for protection when we come across police carrying some herbs, as they will need some form of identification”.
Collaboration between traditional health system and western health system
When asked about the level of collaboration between western doctors and traditional healers, Participant B mentioned that traditional healers sometimes attend meetings with nurses. This participant indicated that in some instances nurses are invited at initiation schools to administer medication. According to Participant K “traditional healers do attend meetings with local hospital. In the meeting it was agreed that each side would refer patients to one another.” Of concern from the participant was that the nurses were treating them badly as ‘they (nurses) think traditional healers are backward’. In addition, Participant A lamented that “collaboration is one sided because hospitals never refer patients to us while we do refer patients to hospitals”. Participant C corroborated Participant A by indicating that when referring patients to hospitals nurses sometimes fight with both patients and traditional healers asking why they (patients) consulted traditional healers first instead of going to the hospitals. Participants were of the opinion that hospitals are highly unlikely to refer patients to traditional healers. Some of the reasons cited include: “Collaboration with doctors is difficult because they undermine our practice maybe because we did not read books that they read”; “The western doctors call us in all hard and wrong names such as witches and witchdoctors”; “Western doctors have one problem; they think what they do is better than what we do. I believe that there are things that can only be treated by African healers. We do refer patients to hospitals on things we can’t do like if someone wants a drip or blood transfusion but when doctors see that someone needs traditional help they never refer these people.” In addition, Participant H indicated that “I never got referrals from western doctors, but I always refer patients to the hospitals for sicknesses I cannot deal with.”
However, there were those who cited a formal relationship with hospitals. For example, Participant E indicated that “I had a relationship with our local hospital and we had problems when it came to issues of payment. After treating the patients, the hospital just signed them off and I got nothing which was unfair to me considering that some of the herbs I use I pay a lot of money to get, while others require that I travel long distances to other areas for me to get them which is costly.” The participant indicated that he never sought the assistance of the association he belonged to. As well, Participant P indicated that “I currently have a patient who is at the hospital, the person came here, and I was not happy with the cough they were having so I decided to send them to the hospital to check for TB before I can administer any herbs. Another one had a running tummy and I gave them herbs to stop it and send them to hospital for further checking, we get workshopped at the hospitals and are taught about HIV and TB, so we normally encourage our clients to get tested however we don’t have papers we can use to write those referrals to the hospitals.” However, there were those who indicated that they never had any interaction with hospitals such as Participant N who said that “I have never received any patient from the hospital and never referred any to them before, but I don’t mind doing it.”
Issues impeding practice of traditional healing
When asked to identify challenges they face during their practice, issues that kept on recurring include: receiving of clients at night impacting on the security of traditional healers. For example, Participant F indicated that “Most often I don’t open for prospective clients at night because it might be robbers. If it is a genuine client that might also affect his/her health.” Of interest from Participant M who indicated that despite being a woman she attends patients at night with the believe that ancestors will protect her from evil spirits. She cited societal perception of traditional healing as a factor contributing to people consulting healers in secrecy at night. As she put it “some of our clients are the very same pastors who condemn us in their synagogues. So they do not want to be seen to be consulting traditional healers.” Participant P indicated that by virtue of being a traditional healer he felt safe as even harden criminals have stereotype views that if you hurt a healer you would be cursed for life. The other issues include lack of recognition and government support, criminals who masquerade as clients, solicit of bribery by police, bogus healers who taint the image of traditional healing and difficulty in recovering money from clients. In a nutshell, as indicated by participants, traditional healers face the following challenges on daily basis: Traditional healers have a safety challenge, especially female healers who mentioned that sometimes they do not open their gates at night for clients because they fear robbers. At times, criminals consult them for herbs to use for criminal activities and they find themselves in a difficult position. In addition to that, it is difficult to work long hours into the night, especially if you have a day job and are expected to report for duty the next morning. Healers are less supported by the government despite them playing a major role in the health of the people in the country. They are exposed to different health hazards because they deal with different illnesses, sometimes without being paid. Because of little protection from the government, healers are exploited by some government officials who demand bribes when they find them in possession of herbs or when trying to cross the border to collect herbs or to check on their clients. Traditional healers depend on the money they make from healing people to put food on the table. They mostly heal people and never receive payment. They end up finding themselves in a difficult situation because their ancestors do not allow them to turn the sick people away if they come to them without money. As a result, they end up treating the people but their families go hungry and they end up with no money to buy herbs. There is a serious concern among healers about the bogus healers who are practising in the province. Many of these bogus healers are not even South Africans and they find it very easy to practice as healers in the country. The interviews revealed that it is easy to receive a certificate from the non-statutory bodies offering certificates to healers, which makes it easy for these bogus healers to operate. This makes the job of genuine healers very difficult as they are painted with the same brush when something bad that was done by a bogus healer is reported.
Furthermore, the investigators wanted to know whether the participants only subscribe to the ancestral beliefs or if there are other beliefs they subscribe to as a result of how other religious leaders perceived them. Participant M put it simple that “the source is one, God. We just approach Him in different cultures. And He is helping us in different ways.”
Framework to integrate traditional healing into mainstream health system
The ultimate aim of this study was to develop a framework to integrate knowledge of traditional healing into the mainstream healthcare system. When requested to provide recommendations about the improvement of traditional healing, participants provided the following recommendations: building of regional offices for healers. proper regulation of traditional healing. access to fenced farms which have healing herbs. sensitising of communities about traditional healing as some people view it as witchcraft and barbaric. training of traditional healers on hygiene.
This study proposes a framework for integration of traditional healing into the mainstream health system (see Figure 1). In the proposed framework, the Department of Health should give equal attention to traditional healing and western medicine. Regulation of traditional healing should be a primary mandate of the department. The THPC should demonstrate its absolute powers and perform its duties as required by legislation. There should be well-established statutory bodies regulated by the THPC for the smooth running of traditional healing. This will eliminate illegal activities taking place in the name of traditional healing in the country.
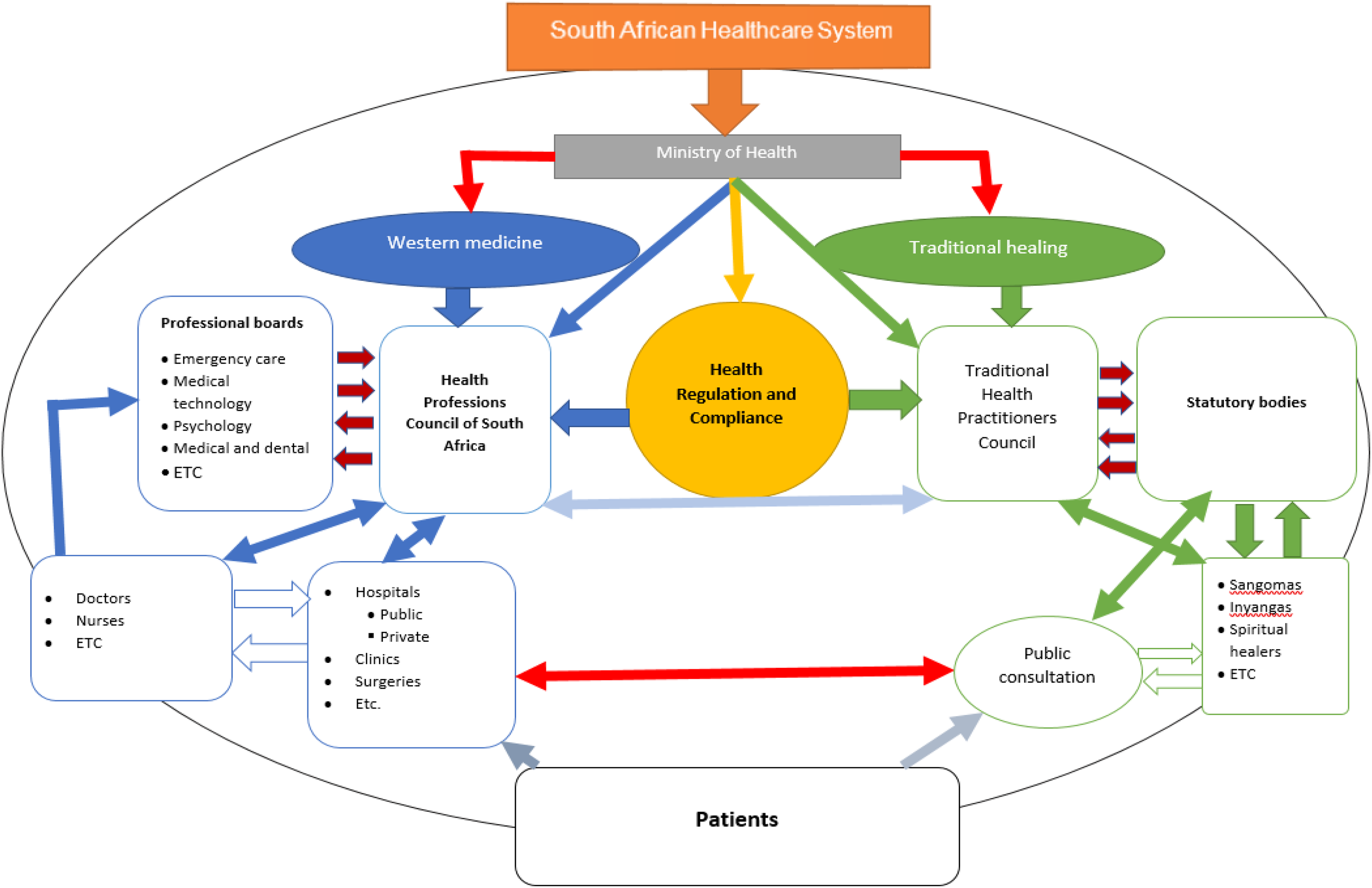
Framework for the integrated healthcare system in the Limpopo province of South Africa.
Collaboration between western hospitals and traditional healers is encouraged. For example, when patients consult either they could be referred to the other, depending on the nature of consultation or illness. This could be the case where patients need the intervention of western testing like HIV testing. In this regard, traditional healers can be encouraged to refer patients to consult hospitals. Likewise, doctors should also refer patients to traditional healers for diseases which may require the interventions of traditional healers. There should be feedback from either side for the purpose of identifying issues and solutions. There should be public consultation areas for traditional healers accessible to patients. Some traditional healers should be employed by hospitals on a full-time basis. Traditional medicine should be tested and packaging be modernised, even though the quantity of administering medication differs from patient to patient.
Conclusion and recommendations
The findings indicate that traditional healing is marginalised and healers are not receiving enough support from the government. Traditional healing is not properly regulated, which allows anyone to practice as a healer without question. As a result, many bad things are happening which paint a dark picture for the practice. Despite constant negative reports, traditional healers serve their communities and they sometimes do that without compensation. The study established that traditional healing is very important and continues to play a role in relieving the pressure on the countries’ government health resources. With that in mind, as reflected in the proposed framework, the following recommendations are made: The government must take an active role in ensuring that healers are formally incorporated into the country’s healthcare system, which will benefit both the healers and the communities they serve. Healers are exposed to various kinds of illness with limited resources; the government needs to intervene to protect healers from such illnesses and assist in the process of ensuring that the sick are treated under good conditions. The policies passed by government on traditional healing need to be implemented and enforced. Traditional healing is harbouring criminals and those who continue to do bad things shelter behind it, as those in power are unable to carrying out the mandates given to them. Traditional healing needs to be regulated to eliminate the current exploitation it is facing from those with dubious intentions. Community leaders should play an active role in educating the youth about African practices and how important it is to preserve these practices. The damage done through political and religious interference will never be undone but all is not lost.
Failure to recognise traditional healing and integrate it in the mainstream health system will continue to hamstring the health system with resources in South Africa. The provinces that are on the periphery, such as Limpopo, can be on the forefront of integrating traditional healing into a western healing system that is already fully fledged. In this way, traditional healing can help reduce the heavy burden on the public health sector in terms of treating patients and can also contribute to the economic development of the country. The overview given in this study has obvious limitations as western medical practitioners were excluded. Therefore, a further study that include the views of western medical practitioners on the integration of traditional medical knowledge into mainstream healthcare is recommended.