
Abstract
The constant evolution of endo-venous ablative techniques for varicose veins arises from the need for: better patient's comfort, reduced incidence of side effects, better results at short-, mid- and long-term follow-up, as well as reduction of operating time and technical simplicity. All these goals have been aimed at but so far no new technology has been able to achieve them all or to demonstrate it, furthermore the increase of price must be compensated by a considerable improvement of results and a serious reduction of side effects to be incrementally cost effective. We present in this article several recent evolutions of sclerotherapy (chemical ablation). New technologies include: proprietary ready-made foam (Varithena®) foam sclerotherapy with catheter and tumescence, foam + Holmium laser (LAFOS®), liquid sclerosant with rotating wire (clarivein®), liquid sclerosant + endo-venous clip (V-Block®) and endovenous cyano-acrylate glue (Venaseal™)
Introduction
Improving existing methods and developing new ones is a permanent tickle for most of us. But do we have serious reasons to modify or change our current (validated, 1 described, 2 reimbursed, registered) chemical ablation of varicose veins (VVs) methods, apart from leaving our name in a book, or increasing our income?
If we consider the current state of ultrasound guided foam sclerotherapy (UGFS) the situation is quite satisfactory, 3 but we can certainly hope to observe less mid- or long- term recanalizations, less adverse events (although the incidence of severe complications remains extremely rare),4–6 and also a better efficacy (at short and long term) on huge VVs with less effects.
However, we certainly can’t expect a less painful and cheaper technique than UGFS (with «home made» foam), since it requires no local anesthesia, and no expensive equipment (besides a DUS machine). As we’ll discuss further, cost effectiveness analysis should be considered too, although it does not necessarily gives the definitive answer.
Presentation of (known) new techniques
Foam sclerotherapy modifications, evolutions, and news
Foam registration
Sclerotherapy with echoguidance has been allowed and reimbursed in France for years under the code number EJNJ001 (37.46 euros) but the use of foam was still neither legal nor illegal (despite reference to studies using exclusively foam), fortunately, this weird situation has been solved by the official registration of Polidocanol (Aetoxysclerol®) 2% and 3% for use in the foamed form. Foam should be obtained by Tessari or DSS technique, using sterile air (this condition has surprised most physicians since no serious infectious threat had been evidenced, but the sales of 0.2 microns filters is expected to burst French economy). A similar registration is expected soon for sodium tetradecyl sulphate. More and more countries have validated UGFS with certain conditions.
Foam with tumescence
A perivenous injection of tumescent solution, with or without local anesthetics is suggested by some (Parsi, 7 Thibault, Cavezzi, and others). Tumescence is carried out after introduction of a catheter in the saphenous trunk; it generates a radial compression and thus a reduction of diameter. Better efficacy on huge trunks, less recanalizations, and less secondary blood deposits are expected. So far, one comparative study shows a non-superiority of the method, more research is necessary. 8 In the past, many studies failed to demonstrate the interest of catheter delivered sclerosing agent, whether foamed or liquid, complications such as deep vein thrombosis have been observed with an increased incidence (supposedly due to a passage through perforating veins) and a case of severe necrosis has been reported. 9
Varithena®
Varithena (formerly known as Varisolve®) is a pharmaceutical-grade, low-nitrogen, Polidocanol foam dispensed from a proprietary canister device. It has been allowed in the USA in November 2013. Two placebo-controlled studies Vanish 1 and 2 have demonstrated its efficacy and tolerance. 10 Initial results are satisfactory, however, we wonder how it compares to home made foam in terms of results, side effects, adverse events, and most of all: COST.
Foam sclerotherapy with Laser: LAFOS®
The concept is to reduce the diameter of the varicose venous trunk by application of a Holmium laser beam prior to the injection of sclerosing foam through the same catheter. A precisely computed succession of low energy rapid laser pulses allows media collagen shrinking without endothelium damage. The technique is painless (almost) and does not require local anesthesia or tumescence, which is an advantage. The idea of obtaining a media shrinking is interesting since this is probably what UGFS does not provide enough. However, we have seen decades ago with cryotherapy that media shrinking may not be durable. So far only preliminary feasibility results are available and according to A Frullini (personal communications at various meetings) 100 % occlusion is observed. The device and its catheter and fiber optics are expected to be cheaper than other laser’s. We need long-term data to compare LAFOS with UGFS and thermal (radio frequency and laser) ablations.
Mechanochemical sclerotherapy with liquid sclerosant MOCA: ClariVein®
This device (Figure 1) associates a catheter with a fast rotating thin wire tip and an infusion of liquid sclerosing agent. It can be applied along the saphenous trunk without local anesthesia and provides excellent immediate and mid-term closure rates.
11
Patients describe a vibration along the thigh during the application, and the process remains perfectly acceptable. It is appealing since it can already present with robust outcomes, does not use foam (interesting since several contra indications to foam do exist like symptomatic PFO or previous side effects), and does not require anesthesia or tumescence.
The ClariVein® MOCA, hand piece, catheter, and wire tip.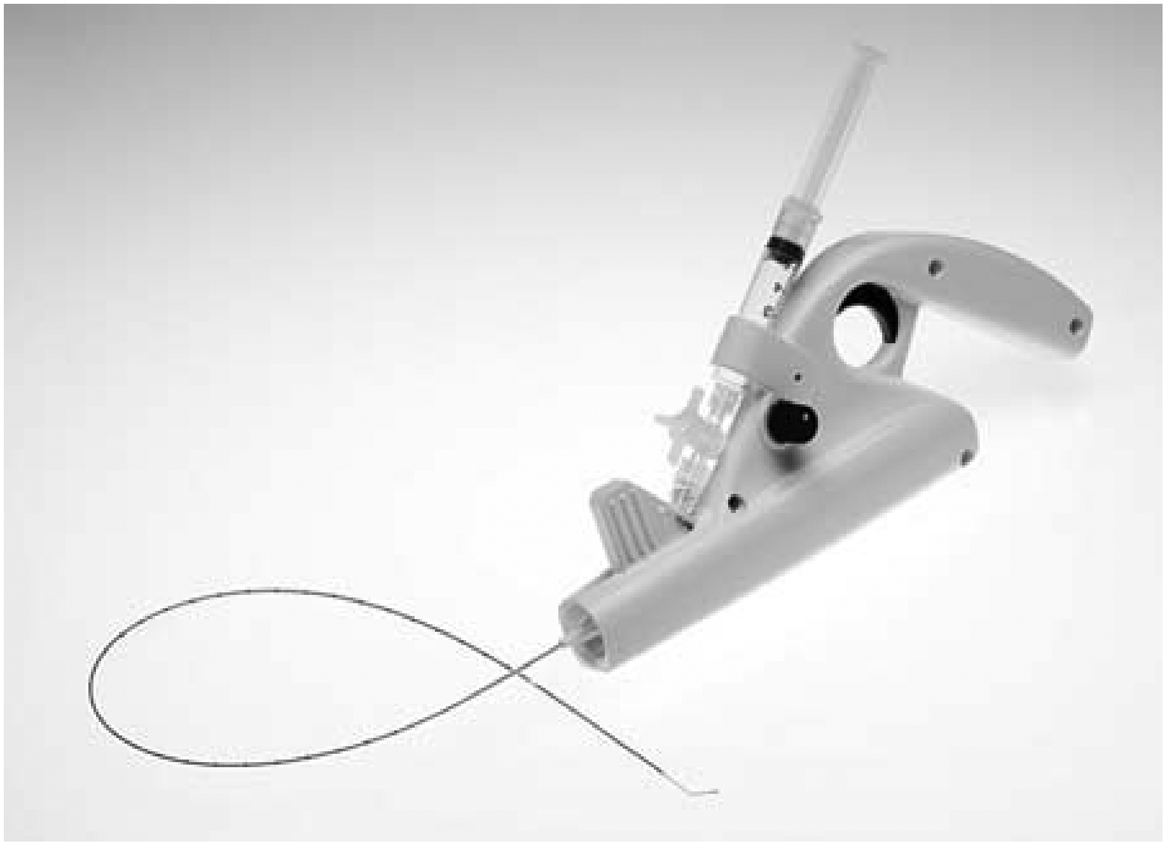
Endovenous device with liquid sclerotherapy: V-Block®
This method consists in the placement of a V-shaped nitinol/PTFE “conic basket” below the saphenous junction, complemented or not with the injection of liquid sclerosant. It has been demonstrated only in animals so far. 12 It has been used in 12 sheep with 12 occlusions and no migrations. It may be of some use in patients contraindicated for foam. It is similar to the V-Clip patented by Van Cleef several years ago, which was a flat V wire, designed to flatten the junction in order either to restore valve competence or to facilitate sclerotherapy when indicated, it has been discontinued. 13 Most devices of this kind seem to remain palpable under the skin, which is a drawback.
Endovenous glue: VenaSeal™ Sapheon
Surgical glue had tempted phlebologists for a long time and early experiences (in the 80s) demonstrated only the exothermic and painful character of glue polymerization, thus the abandon of the concept. Interestingly, a company was able to create a combination of efficient and well-tolerated glue, and non adherent to the glue catheter and injector kit (Figure 2), making it easy to apply glue at the junction and along the saphenous trunk. Obviously, this concept is seducing since it fulfills most phlebologists’ dreams: no anesthesia, no pain, no tumescence, no foam, no generator, no compression, etc … Initial reports are convincing14,15 but like for all new methods, more assessment of mid- and long-term results, and comparison with other methods is necessary. As of today, the glue and its applicator are extremely expensive and scant patients can afford such a treatment (at least in France).
VenaSeal® Adhesive. All three images have been supplied courtesy of Sapheon, Inc.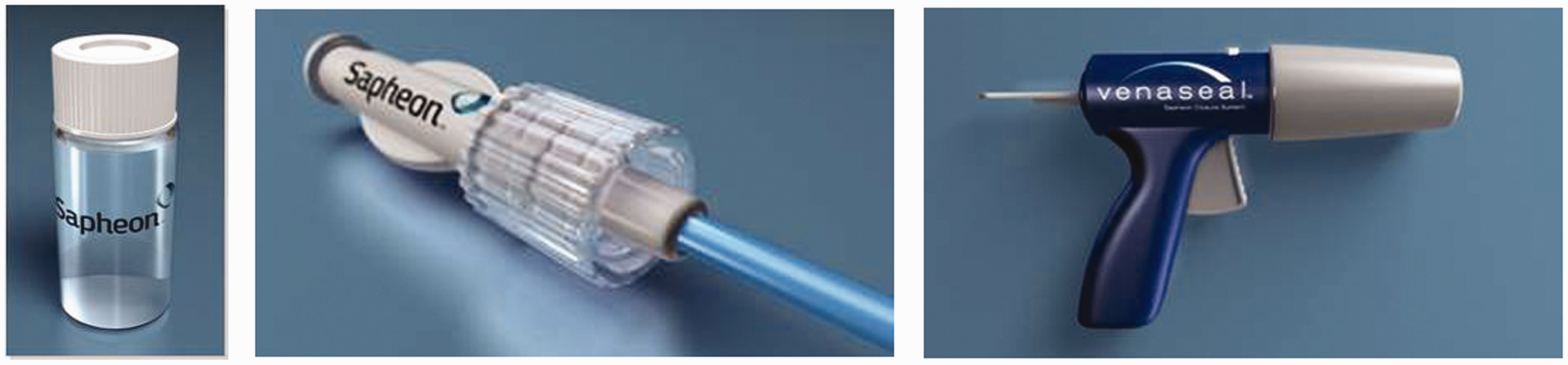
Conclusions
A decade ago, we commented that new concepts and new techniques for VVs treatment evolved faster than the chronic venous disease itself, and that satisfactory RCTs always came too late or only compared obsolete technologies. This must not discourage us of carrying out well-designed studies since it is the only serious way to eliminate rubbish and to avoid further advertisement about them. However, so far none of these techniques presents with any long term cohort study, or with RCTs. Therefore, they appear in no official recommendation, but if we remember how long it took to see endovenous thermal and sclerosing foam ablations to appear in meta-analysis, 16 we can estimate a dozen years before such a publication.
In this article, we face a couple of other issues of evaluation of new methods, including the most difficult of them: the problem of the price.
Cost effectiveness assessment can be used to compare methods but it will be biased by many factors affecting costs computation. In the same country, it may work like in Gohel’s 17 and Rasmussen’s2 studies, demonstrating the superiority of UGFS’ cost-effectiveness. But in these studies, prices are known and the same for all patient of one arm of the study. However, in other countries, the importance of the price difference is such that no serious choice is allowed: for example in France a session of UGFS is reimbursed about 40 euros +5 euros for sclerosant and disposable, while a VenaSeal™ Kit is available at about 1 500 euros (not reimbursed). It will be extremely difficult to demonstrate that glue’s advantages are worth 1 455 euros, even if several UGFS redo injections are likely to be necessary. Furthermore, complementary treatment for tributaries and reticular veins after endovenous thermal ablation is never taken into account, although it is carried out most of the time by sclerotherapy (sometimes by Muller phlebectomy). Similarly, the ultimate treatment for recurrences of any size is also sclerotherapy (UGFS or visual). 18 In these conditions, adding one single UGFS of one remaining incompetent saphenous trunk segment is extremely cheap, and patients never complain.
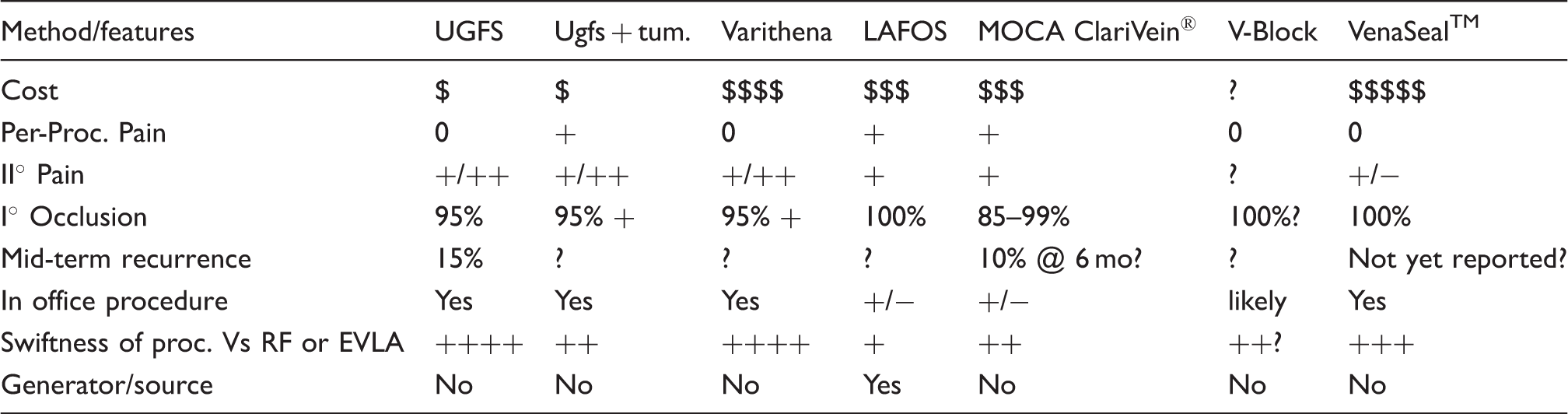
Comparison of most recent and relevant chemical and pharmaco-mechanical ablation methods.
Footnotes
Declaration of conflicting interest
The authors has no conflict of interest and nothing to disclose.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.