
Abstract
Aim
Endovenous foam sclerotherapy (EFS) is used widely throughout the USA for the treatment of venous disorders. The purpose of the quantitative meta-analysis was to systematically and comprehensively evaluate the literature to provide accurate estimates of safety and efficacy outcomes for this procedure.
Methods
A comprehensive electronic search of published literature in several databases was performed using a wide variety of MESH headings. In addition, meeting abstracts and bibliographies of selected references were reviewed for eligible papers. Two reviewers abstracted selected treatment-related data.
Results
Of 684 identified manuscripts and abstracts reviewed, 104 papers were abstracted and analysed. More than 50% were published between 2004 and 2008. EFS was found to be effective with similar vein occlusion rates to laser therapy, but less effective than surgery. In addition, major adverse effects were rare.
Conclusions
EFS is a safe and effective therapy for the treatment of venous disorders.
Introduction
Venous disorders including varicose veins (VVs) are commonly seen by health-care providers. Treatment options have evolved over the past 20 years. While surgery is historically the gold standard for treatment of these disorders, there has been an explosion of endovascular techniques developed, and an increase in the number of specialties treating these disorders including internists and family medicine physicians, dermatologists and interventional radiologists.
VVs are defined as dilated, bulging superficial veins usually classified by size. VVs are the most obvious manifestation of chronic venous insufficiency, affecting 25% of women and 15% of men. 1 Smaller reticular veins and telangiectasia may be found in 80% of men and women. 2 Risk factors for VVs include female gender, advancing age, family history, pregnancy, prolonged standing, obesity, vascular malformations and hormone therapy. 1,3 VVs are more common in patients of European ethnicity compared with patients of African or Asian descent. 3 VVs cause symptoms of pain, swelling, burning, ache and pruritis. 3 Due to the chronic nature of the disease, VVs have a deep impact on health-care resources, especially when VVs cause venous ulcers. In addition, VVs and venous disorders including congenital venous malformations are associated with impaired physical activity and mobility and increased pain. 3
Injection of a liquid sclerosant into a vein has been used to treat VVs and other venous disorders for nearly a century. While surgical stripping has been used for removal of larger and deeper veins, it has been largely replaced by endovascular thermal laser and radiofrequency vein ablation. These techniques require specialized equipment and training, and may only be suitable for straighter and larger truncal veins.
Cabrera has been credited with the use of ultrasound-guided foam sclerotherapy after publishing his case series results in the mid 1990s. 4 Today, endovenous foam sclerotherapy (EFS) is most commonly performed by combining a sclerosant agent, usually sodium tetradecyl sulphate or polidocanol, with air, carbon dioxide or a carbon dioxide/oxygen mix. A foam is created using a double syringe system and this foam is injected into the affected vein to achieve sclerosis of the VV. Despite documented widespread use of this technique for treatment of venous disorders, it remains controversial and many question the efficacy and safety of this therapy. 5
In 2009 a multidisciplinary consensus panel of US experts was convened with three purposes: (1) to conduct a comprehensive questionnaire of those performing foam sclerotherapy in the USA to describe practice patterns and to identify areas of common usage and methodology; 5 (2) to conduct a systematic review of the published literature to evaluate safety and efficacy of EFS for the treatment of venous disorders; and (3) to provide quality improvement guidelines and identify important areas of needed research where there is lack of evidence. The panel consisted of seven representatives from the American College of Phlebology, the Society for Vascular Medicine, the Society for Interventional Radiology and the American Venous Forum as well as a biostatistician and epidemiologist. This publication reports the results of the quantitative systematic review of the published literature.
Methods
An electronic search of published literature was performed using the following Medical Subject Headings (MeSH) headings for the medical condition (Term Set 1): Varicose Veins (including subheading Varicose Ulcer), Saphenous Vein, Venous Insufficiency (including subheadings Postphlebitic Syndrome and Post-thrombotic Syndrome), Vascular Patency, Arteriovenous Malformations, Vascular Fistula (including subheadings Arterio-Arterial Fistula and Arteriovenous Fistula) and Key Words (title, abstract, name of substance work, subject heading word) with truncation as indicated by the symbol: Varicose vein, venous ulcer* varicose ulcer*, venous hypertension ulcer*, stasis ulcer*, venous malformation*, vascular malformation*, venous insufficiency, vascular patency, saphenous vein*, varic*, and reticular vein*, where the symbol * is a wildcard. Additional MeSH headings were included to reflect the treatment of interest (Term Set 2): Sclerotherapy, Sclerosing Solutions, and Sodium Tetradecyl Sulfate with Key Words (title, abstract, name of substance work, subject heading word): Sclerotherapy, sclerosant*, sclerosing agent*, sclerosing solution*, Sodium Tetradecyl Sulfate, and Polidocanol. A third set of terms were included to reflect the form of sclerotherapy with Key Words (Term Set 3): Foam* and Chemical*. All items in Term Set 1 were combined using OR, all items in Term Set 2 were combined with OR, all items in Term Set 3 were combined with OR, and then Sets 1, 2 and 3 were combined with AND.
The databases searched included Medline (January 1948–April 2010), EMBASE (January 1980–April 2010), and Evidence-Based Medicine Reviews (through April 2010): Cochrane Database of Systematic Reviews, American College of Physicians Journal Club, Database of Abstracts of Reviews of Effects, Cochrane Central Register of Controlled Trials, Cochrane Methodology Register, Health Technology Assessment and NHS Economic Evaluation Database using the OVID database search interface. The references cited in the selected publications were manually searched for other relevant manuscripts. Abstracts from four professional meetings were also searched including: Phlebolymphology 2003–2010, American College of Phlebology 2004–2009, American Venous Forum 2005–2010 and Society of Interventional Radiology 2002–2010. All English language reports were included as well as non-English reports when English translation was available. The search was restricted to humans and studies reporting data from subjects aged 19 or over (adults are defined as age at least 19 years in OVID). All papers identified through the electronic search were reviewed and entered into an electronic database. Papers that did not meet study criteria were entered into the database with exclusion criteria noted, but no further data recorded. Inclusion criteria for manuscripts included in the review were studies with patients treated using EFS; treatment of VVs, congenital malformations or venous ulcers of the skin; adult patients aged 19 or older; and studies that reported safety or efficacy data. Case reports and observational studies were included. Studies that did not report original findings, such as review articles or editorials, were excluded. Studies were not excluded based on study quality. Instead, detailed study quality information was abstracted for each paper and summarized in the analysis. Papers that reported data from adult patients aged 19 years and older were included even if younger patients were also included in the reported sample.
Two reviewers (SR, JS) evaluated each abstract relative to the inclusion and exclusion criteria. Full articles were retrieved for those studies which could not be excluded based on the review of the abstract using the predefined criteria which were based on established methodological standards for meta-analyses evaluating therapy. Studies were reviewed for characteristics of study subjects, vein treatment characteristics and methodology, comparative treatments, concomitant therapy, follow-up period, efficacy, safety and study quality. The reviewers met after independent data abstraction to resolve any disagreements. The data abstraction tool is provided in the online Supplementary Appendix.
Statistical analysis methods
The Q statistic was calculated and a formal test of homogeneity was conducted.
6
The I
2 index and corresponding 95% confidence interval (CI) were used to summarize the proportion of the total variability in effect sizes due to between-study variation.
7
The proportions or relative risk (RR) estimates from each study were pooled by using the inverse variance or Mantel–Hanszel fixed-effects method, respectively.
8
Estimates were also combined using the random-effects model by DerSimonian and Laird.
9
The Freeman–Tukey double arcsine transformation of proportions was used to stabilize the variance when calculating the pooled estimated proportion and corresponding 95% CI for the proportion.
10,11
All pooled risk ratios were reported with the associated 95% CI. In the presence of significant heterogeneity (P < 0.1) and for consistency when the fixed and random effects modelling results were similar but heterogeneity was not statistically significant, the random-effects model results were presented. A value of 0.5 was added to each cell in 2 × 2 tables with zero cell frequencies. Analyses were performed with and without case series reports of fewer than 20 patients to determine the influence of the targeted sampling on the overall pooled estimates. A two-tailed P value ≤0.05 was considered statistically significant. Data were analysed using R (R: A Language and Environment for Statistical, R Development Core Team,
Results
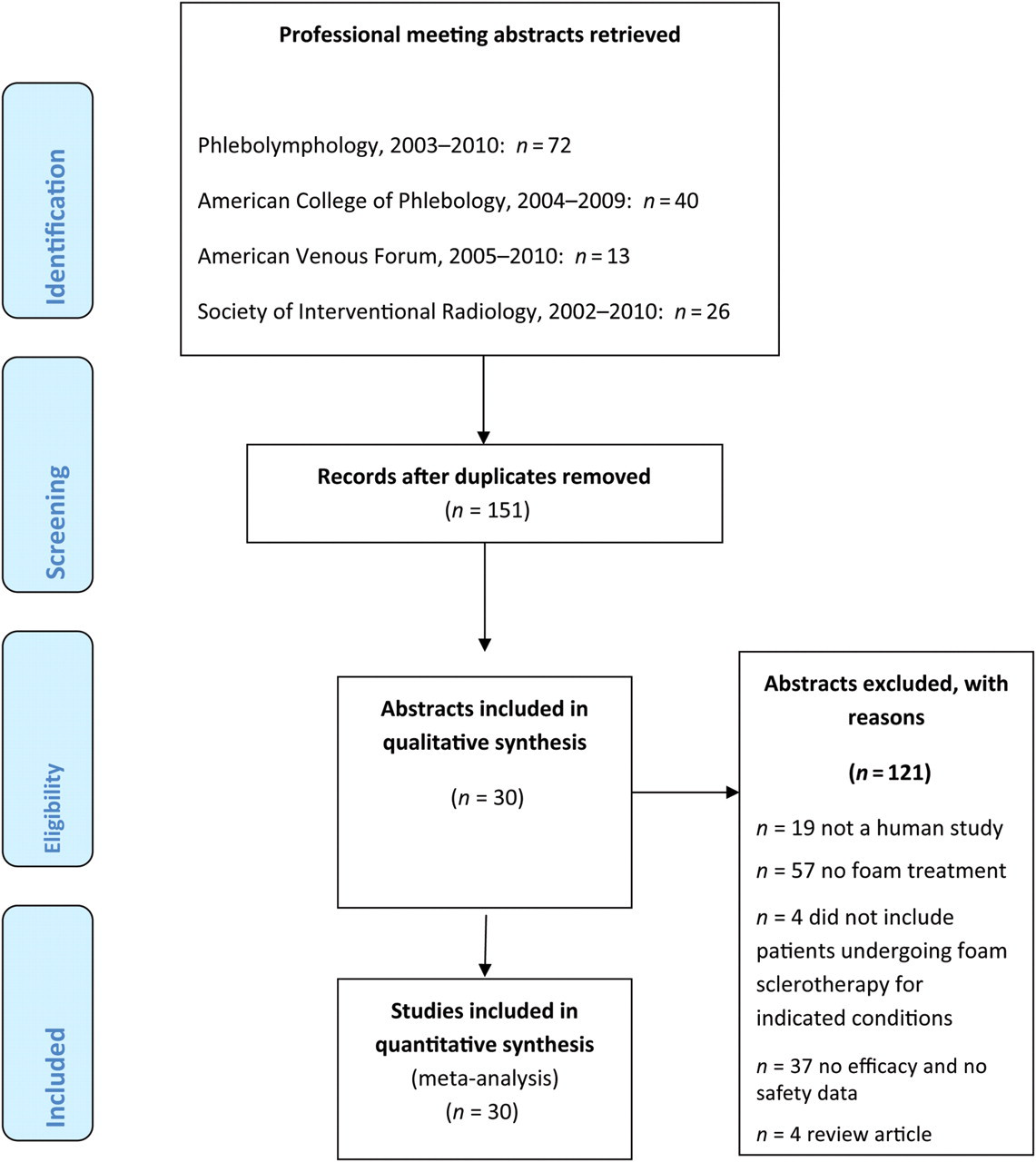
The manuscript review results for full articles and abstracts are given in Figures 1 and 2. Of the 104 reports identified, 20 (19%) were randomized clinical trials, 82 (79%) were observational studies and two could not be classified.
12–115
Fifty-one reports (49%) were prospective reports, 26 (25%) were retrospective, and in 27 (26%), the design could not be determined.
Manuscript review Abstract review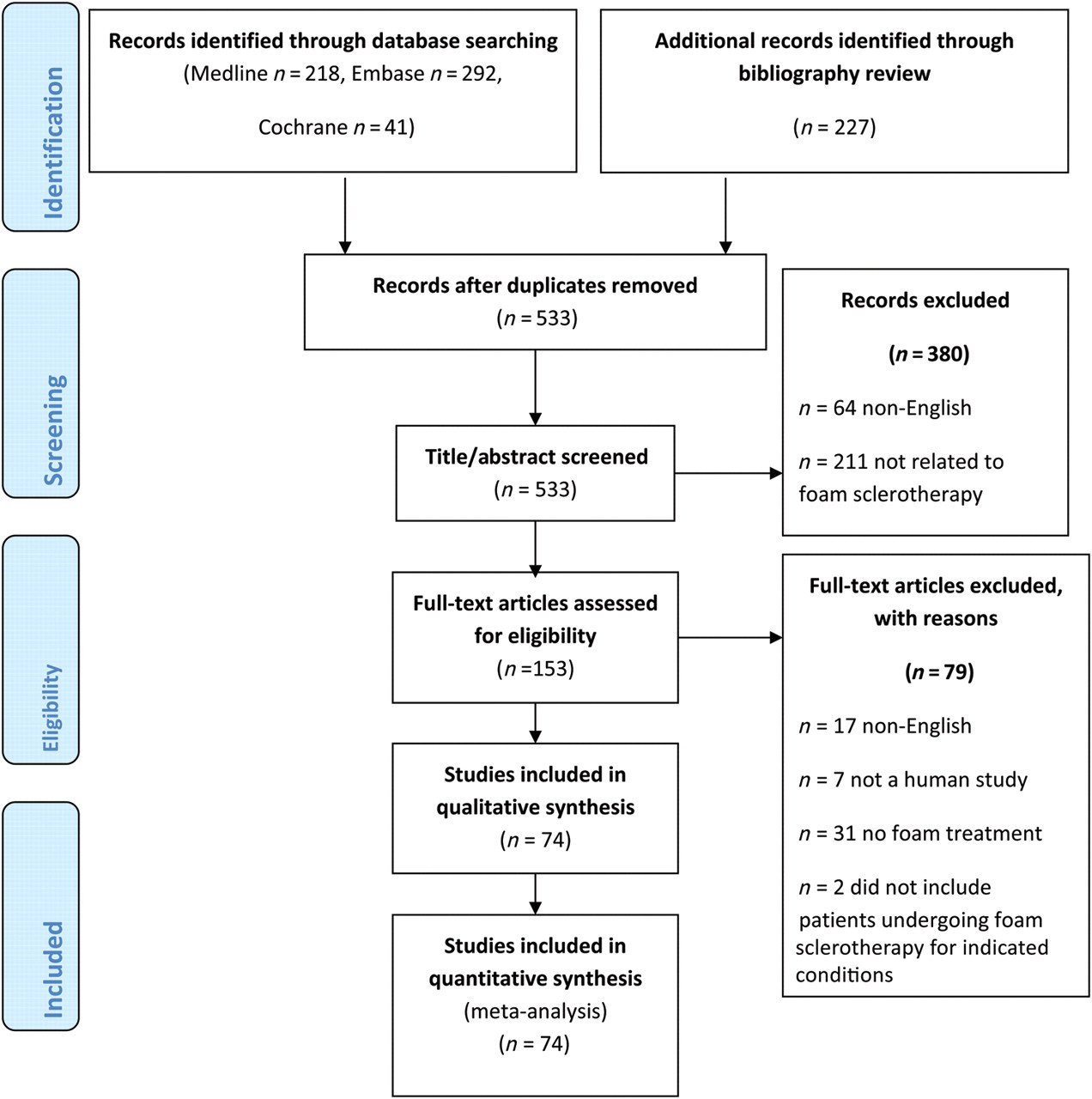
More than 50% of studies were published between 2004 and 2008. Of the 104 reports identified for review, the majority were from Europe (54, 52%), with 16 reports from the USA.
Patient characteristics
The age of study participants ranged from five months to 95 years, with an overall mean age of 49 years and a median age of 47 years (central tendency 50 years). The number of patients included in the reports ranged from one to 1200 with a median of 60 patients and an average size of 153 subjects. Among the 70 reports that reported the number of female subjects, the percentage of females ranged from 0% to 100% with a median percentage of 73% and a mean of 71%. The number of patients with patent foramen ovale was reported in three separate, single-case reports and two additional retrospective reports, reporting data from seven of 35 patients in one report and 13 of 20 patients in another report with patent foramen ovale.
Vein disorder characteristics
Venous disorders treated
Types of veins treated
GSV, great saphenous vein; SSV, small saphenous vein
Clinical aetiology anatomical pathology (CEAP) classification of treated veins
Treatment characteristics
Sclerosant and gas combinations used
The review also included 17 groups of patients treated with liquid sclerotherapy among the 104 references, including polidocanol (7, 41%), sodium tetradecyl sulphate (4, 24%), glycerin (2, 12%), and combinations of agents (1, 6%) or not otherwise specified (3, 18%). Five groups of patients were treated with laser among the 104 references. There were no studies that reported using radiofrequency ablation with foam. However, it did include 12 groups of patients that were treated with surgery, seven reporting ligation and nine reporting stripping, where a given study may have used multiple surgical approaches.
Compression stockings were used after the procedure in 45% and compression bandaging in 39%. Legs were elevated during or after the procedure in 27% and heparin or low-molecular-weight heparin was used for thrombosis prevention postprocedure in 8%.
Efficacy
Efficacy results summary
GSV, great saphenous vein; SSV, small saphenous vein
Treatment failure of endovenous foam sclerotherapy (EFS) was also investigated. Among 32 studies, the pooled estimated percentage of patients with residual incompetence of the great saphenous vein or small saphenous vein after foam sclerotherapy is 17% (95% CI, 13–22%) (see online Supplementary Figure 2). The pooled rate of recurrence of treated varicosities was 16% (95% CI, 11–23%), and the pooled percentage requiring re-treatment was estimated to be 19% (95% CI, 14–24%). Only seven studies reported on the incidence of neovascularization, resulting in a pooled estimate of 5% (95% CI, 3–7%).
Comparisons to other therapies for venous disorders could be made in some cases. Six studies reported the anatomical closure with liquid sclerotherapy. Due to study heterogeneity, using the random effects model, anatomic closure was 86% more likely with foam sclerotherapy compared with liquid sclerotherapy (RR = 1.86, 95% CI: 1.18–2.94, P = 0.0077). In seven studies, residual saphenofemoral or small saphenopopliteal junction incompetence was 44% less likely following foam sclerotherapy compared with liquid sclerotherapy (RR = 0.56, 95% CI: 0.38–0.84, P = 0.0055). Similarly, based on four studies reporting outcomes after laser ablation, anatomical closure did not differ significantly between foam sclerotherapy and laser; however the CI was wide (RR = 1.02, 95% CI: 0.82–1.28, P = 0.85). Reported in three studies, residual incompetence rates did not differ for foam sclerotherapy relative to laser therapy (RR = 1.52, 95% CI: 0.19–12.45, P = 0.70).
Six studies reported anatomical closure following vein surgery. When compared with foam sclerotherapy, surgery showed statistically better anatomical closure rates (RR = 0.92, 95% CI: 0.86–0.97, P = 0.0036). All of the studies reporting head-to-head comparisons between foam sclerotherapy and surgery utilized a randomized trial design. Reported in four studies, the residual saphenofemoral incompetence rates did not differ for foam sclerotherapy relative to surgery, but the CI of this finding is wide (RR = 0.92, 95% CI: 0.56–1.51, P = 0.73).
Safety
Safety results summary
There were a much smaller number of studies that reported other adverse events including pain and coughing. Few studies reported myocardial infarction (0.1% pooled incidence, 95% CI 0–0.52%) and death (0.01% pooled incidence, 95% CI 0–0.05%). Again, events were not subject to independent adjudication.
Skin-related adverse events were also documented. Skin pigmentation occurred in 18% (95% CI, 11–26%), injection site ulceration in 0.98% (95% CI, 0–1.6%), paraesthesias in 1.2% (95% CI, 0.42–2.4%), severe allergic reaction in 0.2% (95% CI, 0–0.38%) and ecchymosis in 28% (95% CI, 13–47%).
There were insufficient studies to compare the cerebral vascular event rates for foam sclerotherapy relative to liquid sclerotherapy or surgery. No studies with laser therapy reported cerebral vascular events. The rate of DVT was not statistically greater with foam sclerotherapy compared with liquid sclerotherapy (RR = 4.53, 95% CI: 0.86–23.95, P = 0.076). There were insufficient studies to perform an estimate of DVT with laser therapy. The incidence of DVT did not significantly differ for foam sclerotherapy relative to surgery, but again, the CI was wide (RR = 1.45, 95% CI: 0.47–4.53, P = 0.52).
Minor safety outcomes were also evaluated. There was no difference in the rate of superficial thrombophlebitis for foam relative to liquid sclerotherapy (RR = 1.43, 95% CI: 0.77–2.67, P = 0.26). However, the RR of superficial thrombophlebitis was elevated for foam sclerotherapy compared with laser (RR = 2.03, 95% CI: 1.11–3.73, P = 0.022) and surgery (RR = 16.85, 95% CI: 2.27–124.74, P = 0.0057). Skin pigmentation did not differ between liquid sclerotherapy, laser and surgery compared with foam sclerotherapy using the fixed effects model (P > 0.1 for each). Similarly, the rates of paraesthesia did not differ between liquid sclerotherapy, laser or surgery compared with foam, but these estimates are limited by the small sample size and interstudy variability (P > 0.2 for each). Ecchymosis did not differ with liquid sclerotherapy and laser compared with foam sclerotherapy, but was significantly lower with foam sclerotherapy compared with surgical treatment (RR = 0.40, 95% CI: 0.25–0.64, P = 0.0001). There were inadequate numbers of studies to compare pain following treatment, although one study suggested no difference between liquid and foam sclerotherapy (P = 0.20), and a second study of 488 patients suggested pain was less frequent for foam sclerotherapy (n = 418 patients) compared with post-surgery (n = 70 patients) (RR = 0.32, 95% CI: 0.17–0.62, P = 0.0006).
Discussion
This systematic review of the published literature from more than 25 countries evaluates the widespread use of EFS for the treatment of venous disorders. This analysis represents an up-to-date analysis of the published literature using comprehensive methodology. EFS was used primarily for the treatment of VVs with fewer studies reporting its use in the treatment of venous ulcers or congenital malformations.
Based on this analysis, several conclusions can be made. First, EFS was efficacious with overall anatomical vein closure rates of 85% with more than 90% of subjects reporting improvement in symptoms. These efficacy outcomes were better than that reported with liquid sclerotherapy and comparable to laser vein treatment. Surgical treatment of venous disorders was found to be slightly superior, but the paucity of available studies to make adequate comparisons limit interpretation of this finding. EFS also showed modest results in the anatomical closure and cosmetic improvement of congenital venous malformations.
Secondly, EFS was found to be safe and associated with few serious adverse events. The incidence of cerebrovascular events was extremely low, but with poor reporting of timing of events, follow-up and prognosis. Other neurological adverse events were also rarely reported. The serious adverse events of suspected cerebrovascular accident were primarily from case reports with no prospective studies reporting long-term outcome or disability following the incident. DVT was reported overall in less than 1% of patients, again with treatment and prognosis details lacking. Minor adverse events of hyperpigmentation and pain were more common. Fewer studies evaluating thermal or surgical vein therapy limited comparisons of adverse events of these treatment modalities. Indeed, no studies were included that compared EFS to radiofrequency ablation of VVs.
There have been three other more recently published meta-analyses evaluating foam sclerotherapy. 116–118 Jia et al. 116 in 2007 evaluated 69 eligible vein treatment studies and found an 87% rate of complete vein occlusion following EFS with an 8.1% recurrence rate. Deep vein thrombosis and pulmonary embolism was found in less than 1%, visual disturbances in 1.4%, headache in 4.2%, thrombophlebitis in 4.7%, pigmentation in 17.8% and pain at injection site in 25.6%. The authors felt that study heterogeneity limited comparisons of liquid sclerotherapy and surgery with foam, although there were non-significant trends in favour of surgery for complete vein occlusion and less efficacy with liquid sclerotherapy. Two meta-analyses were published in 2008: Luebke and Brunkwall 117 reporting 22 of 83 total studies with foam sclerotherapy, and van den Bos et al. 118 reporting 30 of 64 eligible studies using foam sclerotherapy. Luebke found similar short-term occlusion rates between foam and surgery, which were both superior to radiofrequency ablation, but less efficacious especially compared with laser at three-year follow-up. 117 Compared with thermal ablation, foam sclerotherapy had the lowest rates of deep vein thrombosis and paraesthesias. Van den Bos et al. 118 reported that foam sclerotherapy and radiofrequency ablation were as effective as surgical stripping, but less effective than laser therapy. Adverse events were not systematically evaluated. A more recent comparative meta-analysis concluded that low-quality data indicated surgery was as effective as other endovascular techniques for the treatment of VVs, but resulted in more pain and disability. 119 Based on these reviews and other studies, the Society for Vascular Surgery and American Venous Forum recently concluded that endovenous thermal ablation should be recommended over surgery for initial treatment of VVs associated with axial reflux, and foam sclerotherapy considered only for the treatment of telangiectasia, reticular and other VVs. 120 This recommendation contradicts the comparative efficacy findings of this and other meta-analyses.
Although comprehensive, this meta-analysis is limited by the large number of observational and case studies with few randomized controlled trials included. Definitive analysis of key outcomes of effectiveness and safety could not be completed due to the small number of eligible studies, and formal comparisons between methods of vein treatment are limited. However, this analysis represents a comprehensive and intensive search and data extraction of studies evaluating EFS for the treatment of common venous disorders.
Finally, there are several questions still to be answered. For example, there is insufficient data to determine the best methodology for performance of EFS including differential preparation of foam with sclerosant and gas mixture as well as injection technique. In addition, there are few head-to-head studies with other endovenous treatments, namely thermal laser and radiofrequency ablation limiting any definitive comparisons. In contrast to other reviews, we found no difference in efficacy compared with laser therapy, insufficient studies to assess radiofrequency ablation and superiority of surgical therapy. However, as noted above, study quality was low with wide confidence intervals surrounding risk estimates. Low study numbers and poor quality also limited conclusions about comparative safety; however, it appears that foam sclerotherapy is associated with a low-risk profile that is no greater than other VV treatments.
Conclusions
The results of this comprehensive meta-analysis reveal that foam sclerotherapy is a safe and effective therapy for treatment of venous disorders. With a growing and more elderly population and wider awareness of venous disease, phlebologists will be increasingly involved in the treatment of these venous disorders. EFS can be used as a simple, efficacious and safe procedure. However, guidelines are needed for the effective use of this treatment.
Footnotes
Acknowledgements
Endovenous Foam Sclerotherapy Consensus Panel: Nick Morrison, Kathleen Gibson, Pauline Raymond-Martimbeau, Robert Worthington-Kirsch, Eric Hohenwalter and Joann Lohr.
This work was funded by the American College of Phlebology Foundation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.