
Abstract
Compression therapy is the most important basic treatment modality in venous leg ulcers. The review focusses on the materials which are used: 1. Compression bandages, 2. Compression stockings, 3. Self-adjustable Velcro-devices, 4. Compression pumps, 5. Hybrid devices. Compression bandages, usually applied by trained staff, provide a wide spectrum of materials with different elastic properties. To make bandaging easier, safer and more effective, most modern bandages combine different material components. Self-management of venous ulcers has become feasible by introducing double compression stockings (“ulcer kits”) and self-adjustable Velcro devices. Compression pumps can be used as adjunctive measures, especially for patients with restricted mobility. The combination of sustained and intermittent compression (“hybrid device”) is a promising new tool.
The interface pressure corresponding to the dosage of compression therapy determines the hemodynamic efficacy of each device. In order to reduce ambulatory venous hypertension compression pressures of more than 50 mm Hg in the upright position are desirable. At the same time pressure should be lower in the resting position in order to be tolerated. This prerequisite may be fulfilled by using inelastic, short stretch material including multicomponent bandages and cohesive surfaces, all characterized by high stiffness. Such materials do not give way when calf muscles contract during walking which leads to high peaks of interface pressure (“massaging effect”).
Gravity is the reason why most “wounds” are localized on the lower extremities. Compression counteracts gravity and will therefore stay the basic therapy for managing all sorts of leg ulcers also in the future. In many so-called real life studies the healing rates of venous leg ulcers is still reported to be less than fifty present after twelve weeks. As shown by several trials this situation can be dramatically improved by choosing adequate compression materials applied with adequate pressure. The additional use of pressure pumps in combination with conventional compression is a promising tool especially in patients with restricted mobility. New ways of self-management have been developed in the last years. The main obstacle to better ulcer healing in the community is not the lack of good material but the lack of information and training of medical staff and patients to use existing materials properly.
Basic requirements for effective compression
The main parameters responsible for clinical efficiency are the interface pressure exerted on the leg and stiffness. Stiffness is defined by the pressure increase due to an extension of the compression material, 1 as this happens in vivo when the leg circumference increases due to muscle contraction during standing and walking. The ideal compression device has a tolerable resting pressure and a high pressure during standing and walking in order to achieve intermittent compression of the veins with every muscle contraction. In patients with venous insufficiency it could be demonstrated that the best results concerning a reduction ambulatory venous hypertension 2 and an increase of the ejection fraction of the calf pump 3 could be obtained with interface pressures of more than 60 mmHg in the upright position.
The difference between the resting pressure in the lying position and the standing pressure measured at the site which shows the most extensive increase of leg-circumference at the transition between the muscular and tendinous part of the medial gastrocnemius muscle, the so called B1 point, has been termed “static stiffness index”. 4 SSI values of more than 10 correspond to stiff material, while values lower than 10 are typical for elastic material.5,6
To achieve a pressure range of more than 60 mmHg in the upright position single elastic bandages need to be applied with very high resting pressure which is intolerable due to the strong restrictive force of this material. (If the SSI is for example 5, the resting pressure would be 55 mmHg). Inelastic and short stretch material does not give way when the leg enlarges so that the pressure will increase under the rigid cuff around the leg. (If the SSI is e.g. 20, a resting pressure of 40 mmHg would result in a standing pressure of 60 mmHg).
Which material do we have?
For the management of venous leg ulcers the following compression devices are available:
Compression bandages Compression stockings Self-adjustable Velcro-devices Compression pumps Hybrid devices
Material of compression (Modified table reproduced with permission from WOUNDS).7
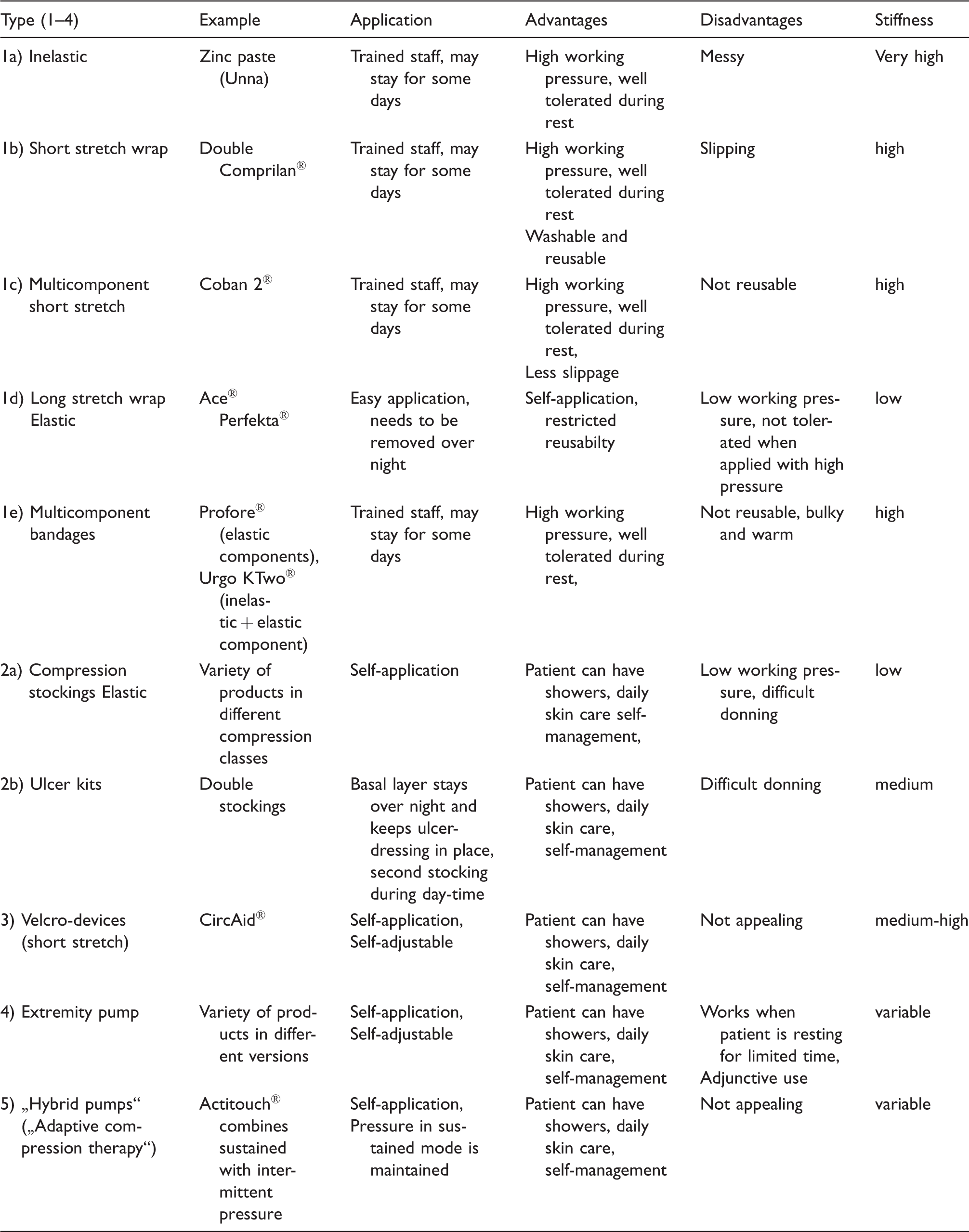
Regarding the elastic property of the textiles used, alone or in combination, the following categories may be differentiated:
6
1a) Inelastic bandages
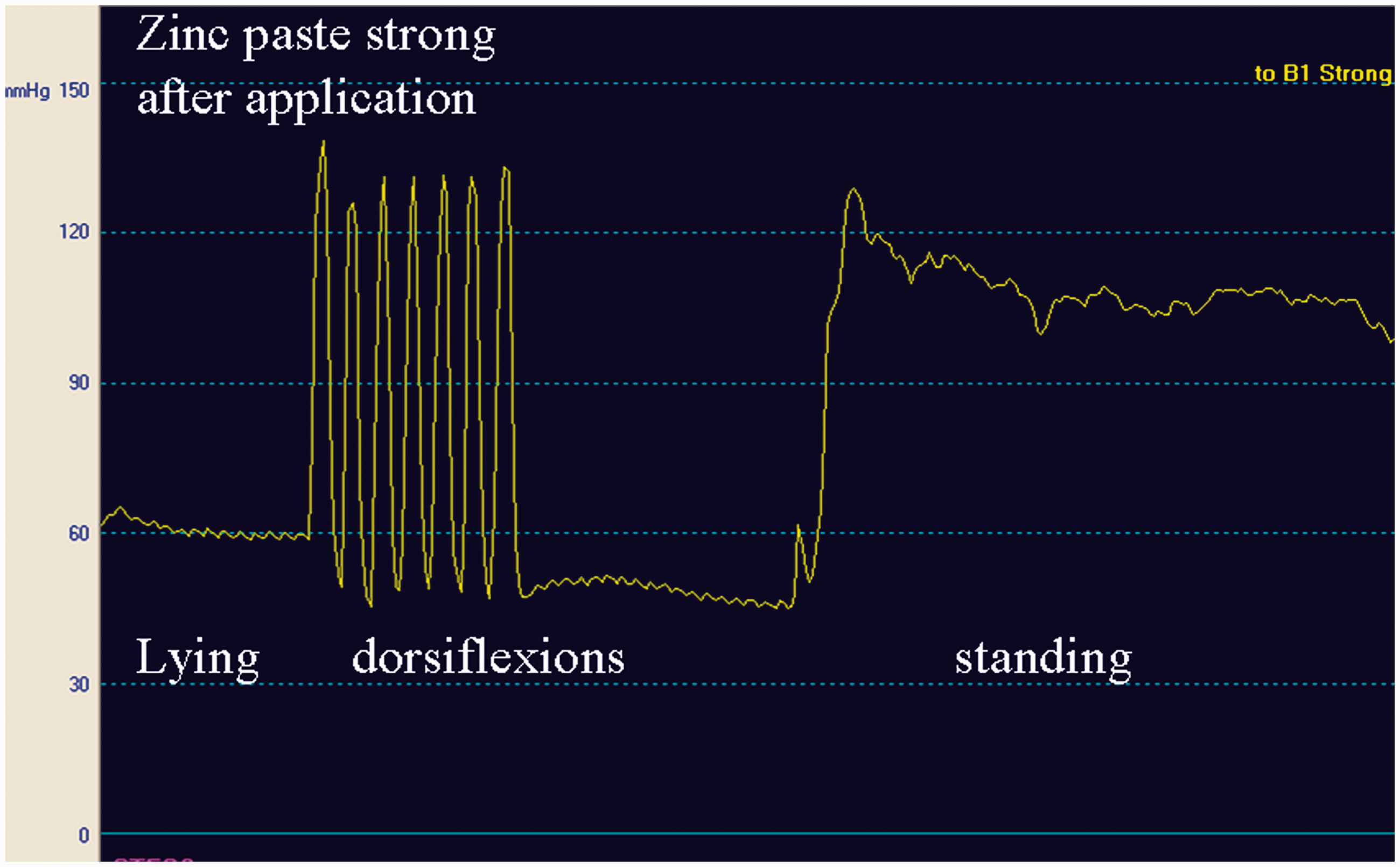
Non- stretchable textiles impregnated with zinc paste (Unna´s boots) are typical examples. Such bandages applied with very high initial resting pressure (>60 mmHg) (Figure 1) will loose pressure immediately and will achieve a pressure of less than 20 mmHg on the following day. In spite of this pressure drop stiffness will remain high which means that the standing and walking pressure may still exceed 50 mmHg (Figure 2).
1b) Short stretch bandages Pressure measured in the medial gaiter area immediately after application of a strong Unna boot bandage. Pressure under the same bandage 26 hours later.

Maximal extensibility in the laboratory is 100 %. Two bandages applied over each other (e.g. the so-called Pütter bandage®) should preferably used with a thin foam padding layer to prevent slippage.
1c) Multicomponent short stretch bandages
All single components consist of short stretch material, which may have cohesive surfaces, as. e.g. Coban 2® and Coban lite®.
1d) Long stretch bandages
Maximal extensibility is more than 100%. These bandages can be applied by untrained personnel and even by the patients themselves, in contrast to the above mentioned types 1 a–1 c) which should be applied by well trained staff.
1e) Multicomponent bandages
They consist of different materials. The so-called “Four layer bandage” is a combination of four different bandages, all of them long-stretch, which, applied over each other, produce a system with an SSI >10. This high stiffness is explained by the friction between the single layers.
8
2a) Compression stockings
In order to put compression stockings over the heel they need to be elastic. They are able to reduce oedema and are indispensible to maintain an ulcer closed after healing.
9
However, due to their restricted pressure and stiffness, they are much less effective to improve venous hemodynamics. Figure 3 shows the pressure tracings of a knee-high compression stocking in the mostly used pressure class.
2b) Ulcer kits Pressure under a compression stocking, pressure range 20–30 mmHg.

One basic stocking (liner), worn day and night, keeps the local dressing in place and a second compression stocking applied on top is worn during daytime. By applying two stockings over each other pressure and stiffness of the final kit is increased. Such ulcer kits may be used in patients with small and not long standing ulcers.
Instead of the outer compression stocking also elastic bandages have been used
10
showing that high pressures were associated with high healing rates. Due to the restrictive force of these elastic bandages used as an outer layer the high pressures (70 mmHg) were poorly tolerated.
11
3) Velcro devices
Such compression products consisting of short stretch material wrapped over the leg and fixed by Velcro bands are the only inelastic products which can be properly applied by the patient. The patient is able to adjust the pressure to a comfortable level.
12
Better ulcer healing was reported in comparison with conventional compression therapy.
13
Some Circaid® products come with measuring cards helping to adjust the pressure in a predefined range.
4) Extremity pumps
Pneumatic chambers or battery operated, peristaltic pumps (Venowave®) generate a wave-form motion on the leg. In spite of ambiguous metaanalyses in the field of ulcer healing
14
such devices make sense especially in people whose mobility is restricted.
5) Hybrid systems
Newly developed devices offer a combination between sustained pressure which is automatically kept at constant levels and intermittent pressure waves which can be used during resting periods of the patient. 15
Clinical implications
Compression is still the most important basic treatment modality for managing leg ulcers. If no clear clinical improvement can be achieved by proper compression in some weeks the diagnosis of a purely venous ulcer needs to be reassessed (Doppler/Duplex examination, biopsy, blood testing etc.). Reflux abolition by endovenous procedures may prevent recurrence of venous ulcers even without ongoing life-long compression.
There is clear evidence that higher compression pressure is correlated with a higher healing rate. 16 Practically important is to achieve high enough pressure especially in the ulcer region which may be problematic if ulcers are located behind the ankle. By putting local pads over such ulcers or by applying external straps over the bandage local pressure can be increased. 17 High pressure is especially important in the upright position in order to counteract the elevated hydrostatic pressure in the veins. Compression systems with high stiffness are preferred because they provide high pressures during walking and at the same time relative low resting pressures in the lying position which are well tolerated. Due to the instant pressure drop such inelastic bandages should be applied with initial pressures over 60 mmHg. 18 Typically this pressure will drop immediately due to oedema reduction in the lying but much less in the upright position (Figures1 and 2). This is the reason why such bandages will still be hemodynamically efficient after a wearing time of 1 week. 19
A second important action of inelastic compression is their so- called massaging effect, characterized by high pressure peaks during muscle contractions. These pressure peaks can be compared with the waves produced by intermittent pneumatic pressure pumps.
In patients with mixed, arterial-venous ulcers “modified compression “can be used as long the systolic ankle pressure is more than 50 mmHg (toe pressure >30 mmHg). This modified compression is characterized by inelastic material not exceeding pressures of 40 mmHg after application in the lying position, which should be renewed every one or two days in order to inspect the skin carefully for potential damage, together with walking exercises. We were able to demonstrate that such bandages are able even to increase skin blood flow under the bandage and also to enhance the ejection fraction of the venous pump during walking. 20 Ankle pressures of lower than 50 mmHg (-toe pressures <30 mmHg) characterize critical ischemia and are a clear contraindication for sustained, but not for special forms of intermittent pneumatic compression.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of interest
The author has no conflict of interest and nothing to disclose.