
Abstract
Introduction
New developments in the treatment of complex deep venous disease have become available in the last decade. Besides analysing patencies as a surrogate outcome for these treatments we analysed the Quality-of-Life (QoL) changes for successful and failed deep venous treatments.
Materials and methods
Patients with proven venous occlusive disease, referred to our department of Venous Surgery at the Maastricht University Medical Centre, were included. After inclusion patients were treated by percutaneous transluminal angioplasty and stenting and when indicated endophlebectomy with an arteriovenous fistula. QoL was assessed with the disease specific VEINES-QOL/Sym and the generic Short-Form (SF)-36 questionnaires preoperatively at baseline and post-operatively after 3, 12 and 24 months.
Results
One hundred fifty-three interventions were analysed, showing a primary, assisted primary and secondary patency of respectively 65%, 78% and 89% at 24 months. The VEINES-QOL and Sym scores improved at 3, 12 and 24 months. The overall improvement at 24 months is 22.7 for QoL and 18.18 for Sym with respective p values of 0.013 and 0.016. The improvement of the VEINES-QOL and Sym scores after a successful (patent) treatment remained highly significant (QoL: p < 0.001, Sym: p = 0.004). Also the generic QoL (Short-Form 36v2) shows significant improvement after 12 months for physical functioning (p = 0.004) and role physical (p = 0.004) scales.
Conclusions
The overall patencies of interventions for deep venous pathology are exceptionally good after two years. Concomitantly the VEINES-Sym and VEINES-QOL scores improve significantly for 3, 12, and 24 months when compared to the baseline (T0) after treatment. Successful interventions showed, as expected, a significant greater QoL improvement between T0 and T3, T12, T24 for both VEINES-QOL and VEINES-Sym scores when compared to the failed interventions. The one-year linear improvement of two SF-36 scales (PF and RP) is also significant.
Keywords
Introduction
The last decade has shown some interesting developments regarding the treatment of deep venous occlusive and/or obstructive (DVO) disease. New thrombectomy devices1,2 have been brought to the market to improve cloth removal in deep venous thrombosis (DVT). Also new dedicated venous stent shapes have been designed in order to improve clinical outcome.3–5 Clinicians are developing and perfecting deep venous treatment protocols, using new supportive techniques such as intravenous ultrasound (IVUS). After thrombolysis the need for treating an underlying cause with venous stenting is recognized and implemented. 6 As a result slowly more and more research data are being published on the clinical and technical results of these new techniques and devices. At vascular conferences more time and discussion are dedicated to venous disease showing the increased awareness and popularity amongst researchers and clinicians. 7
Improved screening and diagnostic tools such as magnetic resonance venography (MRV), next generation duplex ultrasonography machines (DUS) and improved contrast agents have led to an increased number of identified potentially treatable patients. 8
Short-term Quality-of-Life (QoL) results of venous stenting in patients with DVO have been reported earlier. 9 These short-term results were promising, but to really assess and quantify the beneficial effects of interventional treatments for DVO, more data were needed.
Risk factors and predictors for treatment success are identified.
From mid 2009 till 2014, 771 patients were referred to our venous centre, of which 267 were treated with one or more venous stents for either DVO, occlusion or both.
In 153 of these patients, the dataset with registered patencies, VEINES-QOL/Sym questionnaires, which are increasingly used amongst venous researchers, and the generic Short-Form 36v2 QoL, was complete.10,11
The generic and disease specific QoL results up to 24 months post-intervention related to successful and failed procedures are presented.
Definition of population
In this observational cohort study, we concurrently included patients who were referred to our department of Venous Surgery in the Maastricht University Medical Centre between April 2009 and January 2014. These patients all had chronic complaints of severe venous disease according to the CEAP classification (scores C4-6) or venous claudication combined with other signs of DVO.
The inclusion criteria and diagnostic procedures have been described in a previous publication on the short-term results in this study population. 9
Materials and methods
Quality-of-life
The SF-36v212 is used for generic QoL and the VEINES-QOL/Sym 10 for disease specific QoL. These QoL instruments have been described before.9,13
Clinical and radiological examination
All patients underwent a clinical examination, the VCSS score was assessed, the C of the CEAP classification was scored and the Villalta scale was used to score the severity of (any) post-thrombotic syndrome.
Radiological work-up included a duplex ultrasound (DUS) exam and a MRV in order to identify the extent of the pathology. DUS was also used to assess patency during follow-up. After three months a three-way X-ray image of the stented trajectory was made. After 12 and 24 months only clinical, DUS and QoL assessments were performed, in case of worsening of/and/or sustaining complaints additional radiological examinations were performed.
Type of diagnosis and treatment
Patients described are divided into three categories, based on the cause, extent and treatment of the DVO:
Iliac vein compression syndrome (IVCS) treated by percutaneous transluminal angioplasty (PTA) and stenting. Post-thrombotic syndrome (PTS) treated by PTA and stenting. Extended post-thrombotic syndrome (EPTS) treated by PTA and stenting, with additional endophlebectomy and an arteriovenous (AV) fistula.
The pathology was determined by pre-treatment, DUS and MRV, imaging of the obstruction/occlusion and the length of the pathological vein segment(s). The involvement of the common femoral vein (CFV) and the predicted inflow were the main criteria for deciding when to perform an extended procedure. Depending on the determined pathology patients were treated with PTA and stenting, or in the extended diseased cases, by a combination of PTA, stenting and endophlebectomy combined with the creation of an AV fistula, as described in previous publications.4,5,9
Patency
A patent stent was defined as a venous stent showing adequate radial expansion without lumen reduction (i.e. absence of intima hyperplasia or thrombus) and no limitation of flow. Three types of patency were defined: (1) primary, (2) primary assisted and (3) secondary.
Primary patency means a successful intervention without additional treatments like ballooning and/or stenting afterwards. Primary assisted patency is registered in patients who were additionally treated for a potential in- or outflow or stent related problem that might interfere with patency and could cause failure. Secondary patency means that the intervention failed and a secondary intervention was performed to restore patency.
Follow-up study
Standardized follow-up was planned for each patient at six weeks, three months, six months and one year, after which a yearly follow-up was conducted, with no predetermined end. Our current follow-up data have reached 60 months for a small number of patients. Patency of stents was measured using DUS examination.
Statistics
Metric data are represented by means and standard deviations, if normally distributed. If not, lowest and highest scores are also given. Normality of statistical distributions is measured by the Shapiro-Wilk test. Like the SF-36 scales, the VEINES-QOL measures have been transformed to VAS (0–100) scales with corresponding linear, equal distances, whether items are dichotomous or polytomous. Both VEINES-QOL overall results and VEINES-Sym results are given at baseline (T0), at three months post-operatively (T3), at 12 months post-operatively (T12) and at 24 months post-operatively (T24). Correspondingly, the 8 SF-36 scales are also given at the same follow-up moments.
Data analysis starts with paired t tests. Next, a repeated measures analysis of variance (ANOVA) is done for the one-year follow-up (T0, T3, T12). For this specific analysis data must have complete, non-missing follow-up. Finally, a multiple dummy regression analysis was performed on the patients’ one-year linear progression in the applicable SF-36 scales (bodily function, bodily pain (BP) and role physical (RP)) using gender, age, patency and type of intervention as predictors. A p value of less than 0.05 was assumed to be statistically significant. All data analyses were performed with SPSS-pc version 22.
Results
Patient characteristics
There are 153 baseline patients subdivided into three treatment groups; IVCS: 41, PTS: 67 and EPTS: 45 interventions. The mean age of the patients is 43.5 years (standard deviation (SD): 14.4, range 17–77). Forty-six patients (30.1%) are male and 107 (69.9%) are female.
Patency scores
The primary, assisted primary and secondary patencies were, respectively, 65%, 78% and 89% after two years, as shown in Figure 1. The standard error of the mean (SEM) is less than 10% for all patency measurements.
Patency rates for all interventions up to 24 months.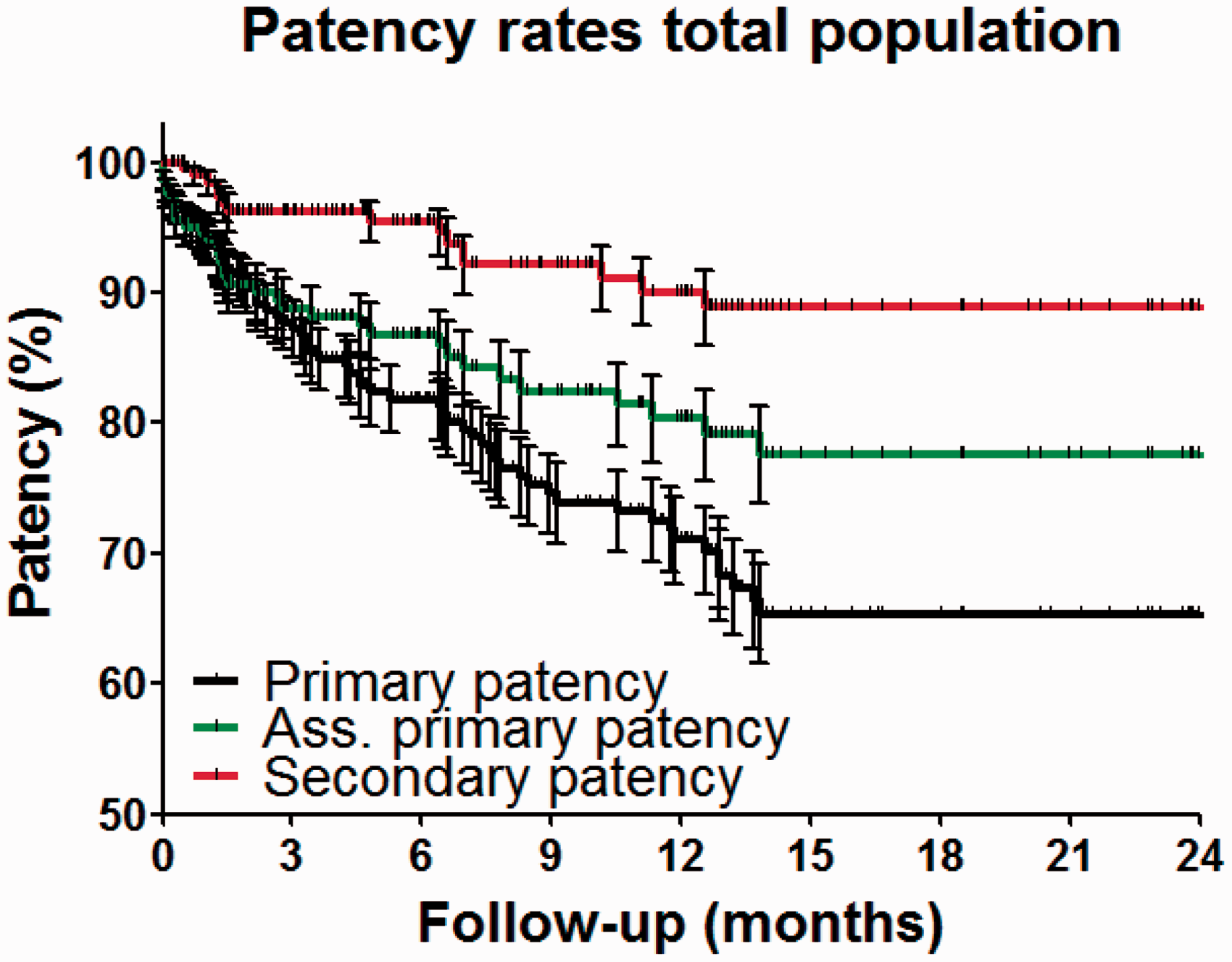
QoL data
Overall VEINES-QOL and Sym scores (disease specific) at baseline (T0), at 3 months (T3), at 12 months (T12) and at 24 months (T24). a
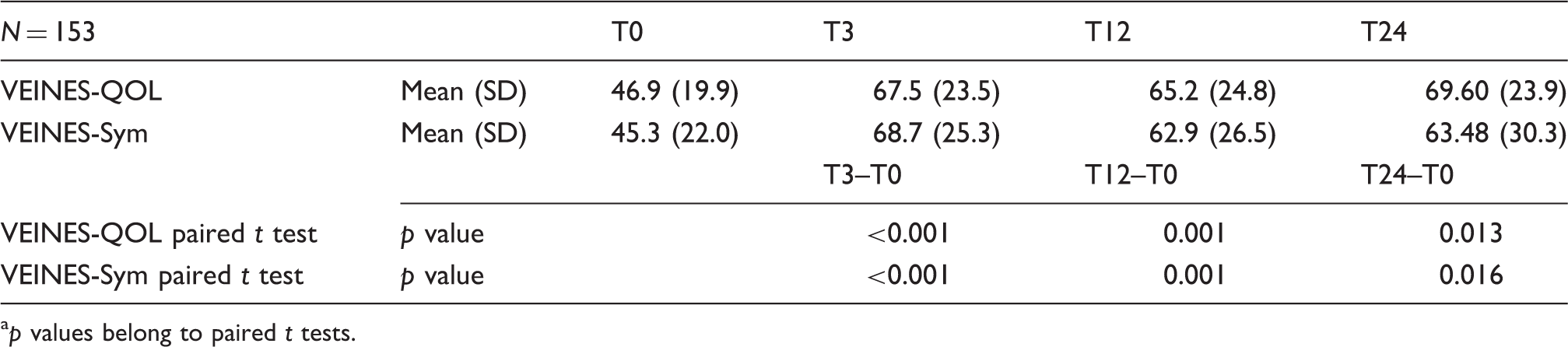
p values belong to paired t tests.
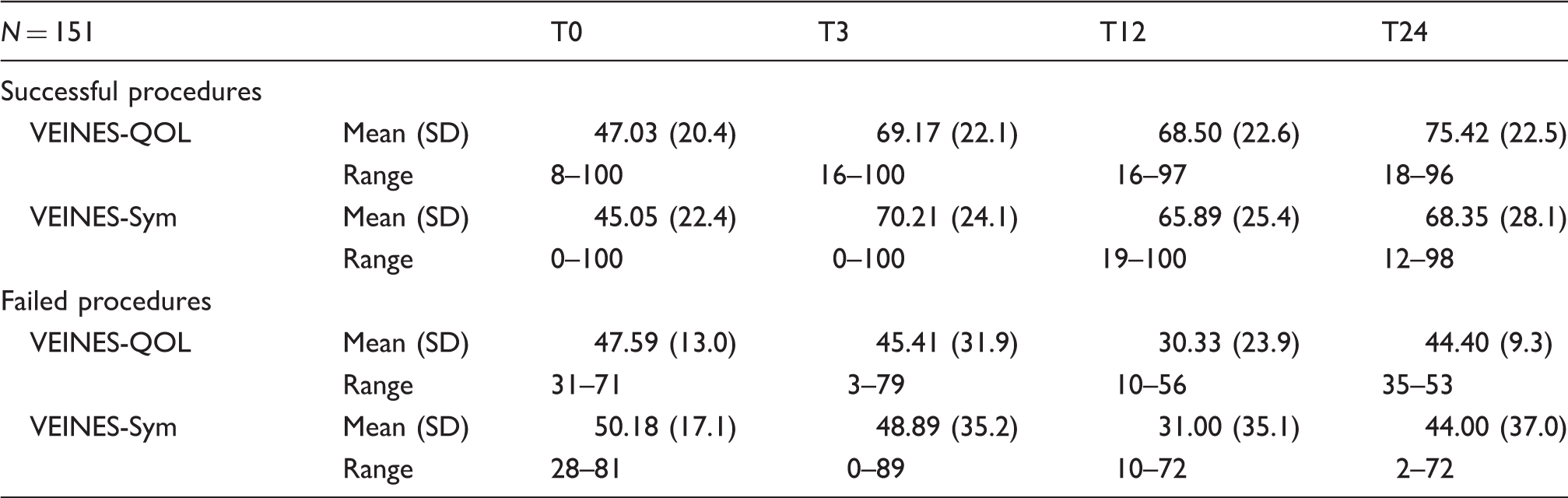
When the overall VEINES-QOL/Sym scores are selected for patency (failed vs. successful) the improvement is much larger in the successful group. The failed group shows no improvement. The overall improvement at 24 months is 28.4 for QoL and 23.3 for Sym in the “successful” group, compared to −3.2 for QoL and −6.2 for Sym in the “failed” group. In repeated measures ANOVA, the effect of patency on the one year progression of the VEINES-QOL/Sym measures is significant: QoL: (overall F = 10.86 by 2 and 56 degrees of freedom (df), p < 0.001, n = 33), Sym: (overall F = 6.20 by 2 and 54 df, p = 0.004, n = 32) (see Table 2 and Figure 2).
Overall VEINES-QOL and Sym scores selected for patent and failed reconstructions. Overall VEINES-QOL and Sym scores (disease specific) selected for patency (successful vs. failed) at baseline (T0), at 3 months (T3), at 12 months (T12) and at 24 months (T24).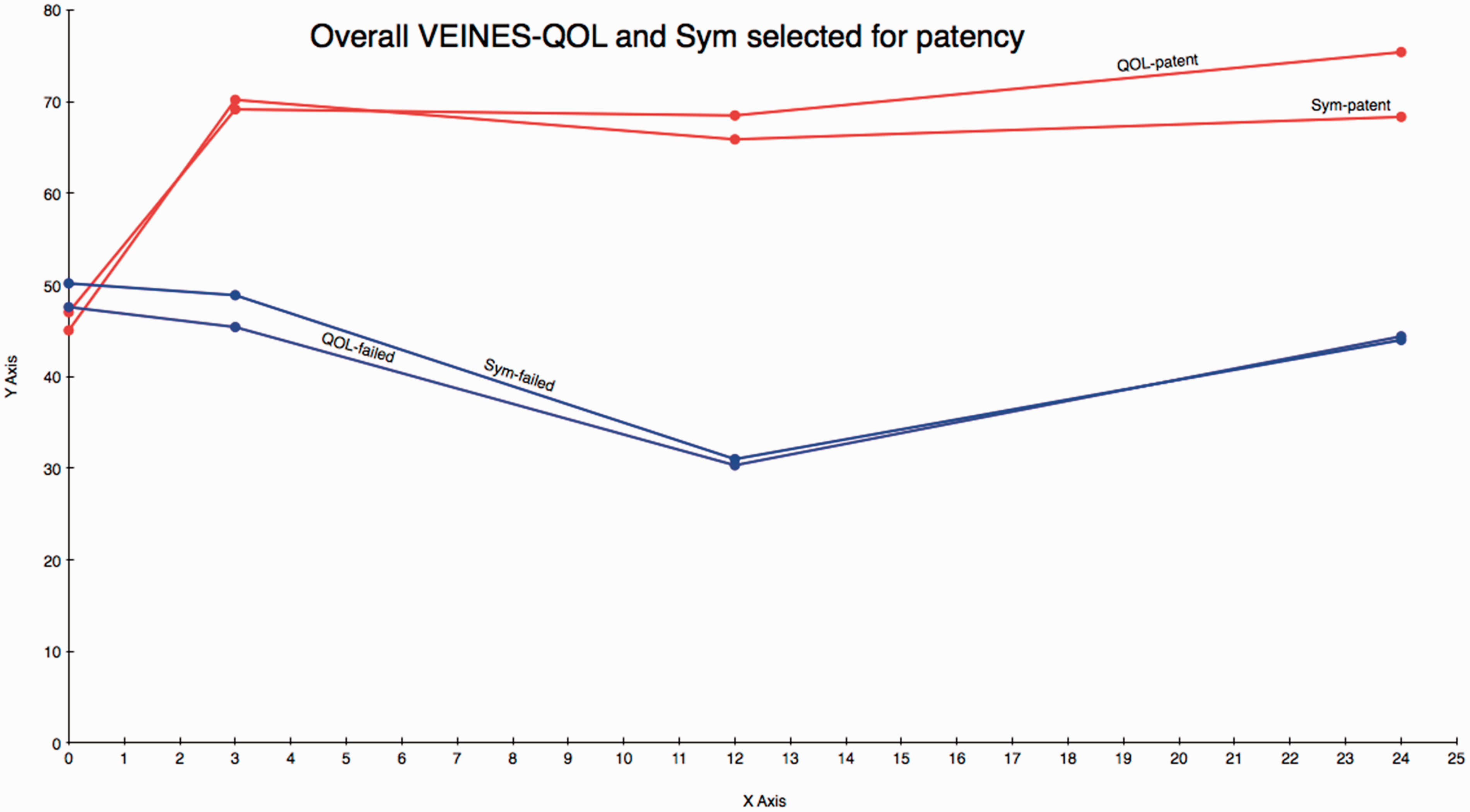
Finally, a repeated measure ANOVA was done for three of the eight SF-36 scales, which we know from a previous publication 9 to be responsive to DVO: physical functioning (PF), BP and RP. Controlled for age the one-year linear progression of the PF and RP was statistically significantly improved (respectively p = 0.004 and p = −0.004), whilst the BP VAS-scale was not (BP, p = 0.074).
Discussion
Patency is considered a surrogate outcome for treatment success. The two year patency rates as shown are much better than anticipated years ago.
QoL is considered to be a true outcome for defining treatment success. The QoL measures used in this series (VEINES-QOL/Sym) to evaluate the interventions for DVO proved again to be responsive and the outcomes are in line with the clinical observations. When the QoL outcomes are selected for patency all failed recanalizations corresponded with lower QoL scores and successful interventions showed a dramatic increase of disease specific QoL scores. This proves that patency is also an important outcome when evaluating the success of deep venous interventions.
The QoL improvements seem to last up to 24 months, something which was also observed in the clinical follow-up of the patients. Because of the decreasing number of patients, when selecting on both treatment type (IVCS, PTS and EPTS) and patency, we were not able to analyse the combined effect of the separate treatment groups and patency. This combined effect is yet to be analysed when the dataset expands in order to prevent a type 2 error. The expected effect of the treatment type will most probably depend on the extent and nature of the treatment, e.g. the more complex treatment (EPTS) will show a slower recovery whilst the relative simple IVCS intervention shows a faster and larger increase in QoL.
The overall QoL improvements shown in this series reach up to 20 points and higher on a VAS scale. Changes in VEINES-QOL/Sym scores of this magnitude are already known to correspond with significant clinical improvement when compared to generic QoL instruments such as the SF-36v2. 10
Norman et al. conducted a large systematic review 14 in order to estimate the minimally important difference (MID) for HR-QoL instruments. They concluded that roughly one half of the standard deviation (SD) of the QoL baseline measure will correspond with the MID. 14 The number of response items and type of instrument (disease specific / generic) did not influence this value. 14 When selected for patency the corresponding VEINES-QOL/Sym VAS scores show differences of up to 28 points, with a SD ranging between 19 and 25.
When we compare the conclusions of Norman et al. to the results all successful procedures show highly clinically important improvements (difference between measurements > one half of the SD) in QoL scores. The failed procedures show a much larger SD, which means their difference in QoL scores during the follow-up period is most likely not clinically relevant. Larger numbers are needed though, to prove the true statistical significance of these findings.
It can be concluded that patency is the dominant factor related to the significant improvement in QoL scores, this is true for both generic and disease specific QoL. Failed procedures, i.e. procedures where we were unable to restore sufficient drainage of the deep venous system, show no specific QoL improvement, but there also seems to be no reduction in clinically relevant QoL measures. This can be explained by the persistence of venous hypertension, impaired back-flow and thus symptoms and complaints such as varicose veins, pain, heaviness and restless legs. The result of a failed procedure is identical to the situation before treatment, such as obstruction and decreased venous outflow with corresponding symptoms. Therefore, a decrease in QoL compared to baseline for failed procedures was not anticipated because the hemodynamics returned to the situation as before the intervention.
Successful procedures, where patent and adequate flow are reached primarily, or even secondary, correspond with a large disease specific QoL increase, which is also clinically relevant with less symptoms of venous obstructive disease, something also observed in clinical exams and outpatient clinic visits. This is also reflected in the improved two generic QoL scales (PF, RP).
The patency numbers reached in this series have exceeded the expectations and continue to improve with the evolution of techniques and materials. When our numbers are large enough to statistically differentiate between the different treatment groups we expect the patency numbers to be higher for the IVCS treatment group and lower for the more complex and extensive disease.
Longer follow-up is required to see if the beneficial effects of restoring venous flow in the lower limbs will persist, especially in more complex cases. Eventually the model regarding the QoL data need to be combined and correlated to clinical scoring instruments, such as the Villalta scale 15 and VCSS score. 16 Some of these clinical instruments might require adaptation to adequately register the clinical relevant improvements by these new treatment modalities.
Since there is no consensus on how to classify DVO disease, it is important to incorporate new scores for diagnostic and radiological imaging such as the LET score and LOVE classification in guidelines and treatment protocols.8,17 This way, combined with improved clinical scoring systems, one can strive to set a benchmark for treatment indication and follow-up for DVO and perform comparisons between different techniques, centres and physicians.
Conclusions
The overall patencies of interventions for deep venous pathology are exceptionally good after two years. Concomitantly the VEINES-Sym and VEINES-QOL scores improve significantly for 3, 12 and 24 months when compared to the baseline (T0) after treatment.
Successful interventions showed, as expected, a significantly greater QoL improvement between T0 and T3,12,24 for both VEINES-QOL and VEINES-Sym scores when compared to the failed interventions. The one-year linear improvement of two SF-36 scales (PF and RP) is also significant.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.