
Abstract
Introduction
Quality-of-life and severity scores are both popular measures in medicine. For deep venous obstruction, the VEINES-QOL/Sym and venous clinical severity score (VCSS) are widely used. Combining a patient-reported outcome with a clinical severity score should give a more sensitive outcome for treatment results. To establish and compare their suitability for deep venous disease, we compared the outcomes of both scores in a group of patients who were interventionally treated for deep venous disease.
Methods
The venous clinical severity scores and VEINES-QOL/Sym scores of a group of patients who had received interventional treatment for deep venous obstruction more than 12 months ago were compared at T0 and T12.
Results
Both the Spearman’s rho and Pearson’s r show a very weak, negative correlation (statistically significant (p ≤ 0.05)), between the venous clinical severity score and VEINES-QOL at T12 and between the venous clinical severity score and the VEINES-SYM at both T0 and T12. T0 VCSS-VSYM: rho = −0.219 (p = 0.052), r = −0.236 (p = 0.037), T12 VCSS-VQOL: rho = −0.459 (p = 0.007), r = −0.379 (p = 0.030), T12 VCSS-VSYM: rho = −0.463 (p = 0.007), r = −0.432 (p = 0.012). This negative correlation was not statistically (p ≥ 0.05) confirmed for T0 VCSS-VSYM.
Conclusion
The physician-scored venous clinical severity score of patients treated for deep venous obstruction does not correlate well with their self-reported quality-of-life and symptom scores.
Keywords
Introduction
Quality-of-Life (QoL) is an increasingly popular outcome measure in modern medicine. Although the concept of QoL has been known for several decades, an uprising of QoL instruments and their application in medicine can be seen only in the last 20 years. QoL is usually measured by means of standardized questionnaires, also often referred to as ‘Patient Reported Outcome Measures’ (PROMs). These questionnaires result in one or more scores, depending on the specific instrument used. A distinction is made between disease-specific and generic QoL, where the first one only applies to specific domains influenced by the targeted disease and the latter targets the overall wellbeing of the patient. Venous pathology can have a large negative impact on the QoL of patients. Comparisons between congestive heart failure and chronic venous insufficiency have been established. 1 A multitude of venous disease-specific QoL instruments is available. 2
The most important aspect of a QoL instrument is the ability to detect treatment-related changes. These changes are determined by a combination of treatment success or failure and the extent of the pathology but can also be influenced other case mix variables, such as age, sex and comorbidity. Ideally, QoL outcomes are objective and universal, but in practice, they are influenced by a myriad of confounders.
Examples of commonly used specific QoL instruments are the VEINES-QOL/Sym (VQS), 3 the CIVIQ-20 4 and the AVVQ. 5
Only looking at the patient’s perspective of treatment effects is just one side; the professional perception of the physician is another. A physician will judge treatment success or failure based on his/her clinical opinion and theoretically objective assessment of the patient’s condition. The outcome is an improvement, status quo or a decline of health. In order to facilitate and structure clinical assessment, various instruments are created. For venous disease, the venous clinical severity score (VCSS) 6 is often used and it is considered a gold standard. This measurement instrument tries to capture clinical symptoms and findings in a single score which objectifies the severity of the disease. A successful treatment should have a beneficial effect on the VCSS score.
Theoretically, both types of measurement, (1) patient-reported disease-specific QoL (VQS) and (2) clinician-reported severity (VCSS), should be able to distinguish treatment effects, whether positive or negative. To establish and compare their suitability for deep venous disease, we compared the outcomes of both scores in a group of patients who were interventionally treated for deep venous disease.
Methods
Patient group
In order to measure the effect of treatment on the QoL and severity scores, we selected a group of patients who had received interventional treatment for deep venous obstruction (DVO) more than 12 months ago. Only patients with VCSS scores for a single limb were chosen. DVO was confirmed by previously described diagnostic procedures. 7 Treatment consisted of percutaneous transluminal angioplasty (PTA) and stenting. In some cases, additional endophlebectomy and an arteriovenous (AV) fistula were required in order to regain a patent venous flow. The exact treatment protocols have been described previously.8–10
Scoring instruments
In order to assess the clinical severity score of the patients before and after treatment, we used the VCSS. The VCSS was created in 2000 by an American Venous Forum (AVF) committee consisting of a group of experts in the field of venous disease. The initial goal of the VCSS was replacing the clinical part in the CEAP classification with something more longitudinal and less static.6,11 It was revised and updated in 2010 in order to update some terminology, simplify the instrument and provide clarification of some ambiguities. 12 The VCSS is a score based on expert opinion, and although statistical validation (intra-observer, inter-observer, etc.) has been performed, no studies validating the VCSS specifically for DVO could be found. 13 Even so, it is routinely used as an outcome in various studies and treatment evaluations. The most important reason for using the VCSS is to establish a standardized and uniform way of reporting clinical outcomes. A 30-point scale is used to provide longitudinal measurement of treatment outcomes. A lower score means less severe disease. The VCSS is generated by the physician during the clinical exam and is meant to be usable for the whole spectrum of venous disease. QoL instruments and the VCSS are considered complementary to each other by many, including the creators of the VCSS. 12
In addition to clinical outcomes, we use the VQS in our practice for disease-specific QoL. The VQS is a rigorously validated QoL instrument, specifically made for venous disease. 3 The VQS consists of 26 items, of which 10 are symptom-related, 9 assess limitations in daily activities, 1 assesses which time of day has the greatest symptom intensity, 1 assesses changes during the past year and 5 cover the psychological impact of venous disease. Two scores are calculated from the completed questionnaire: the QOL score (25 items), which measures the overall impact of venous disease on the patient’s QoL, and the Sym score (10 items), which measures symptom severity. It has been validated for DVO and post-thrombotic syndrome (PTS).3,14,15 Here, a higher score constitutes a better QoL.
In principle, both the VQS and the VCSS scores are assessed at every visit to our outpatient clinic. In this comparative study, we used data on the pre-treatment VEINES-QOL, Sym and the VCSS scores, and the 12 months post-treatment VEINES-QOL, Sym and VCSS scores.
Statistics
At pre-treatment and at 12 months post-treatment separately, both Spearman’s rank correlation (rho) and Pearson’s correlation (r) coefficient were used to assess the relationship between the VCSS, the overall VEINES-QOL and VEINES-Sym. Given the definitions of the scales, there should be a high, negative (rank) correlation between the professional instrument and the patient-provided one. The p value and number of patients are also given. A p value of less than 0.05 is considered to be statistically significant. Data analysis was performed by SPSS-version 23.
Results
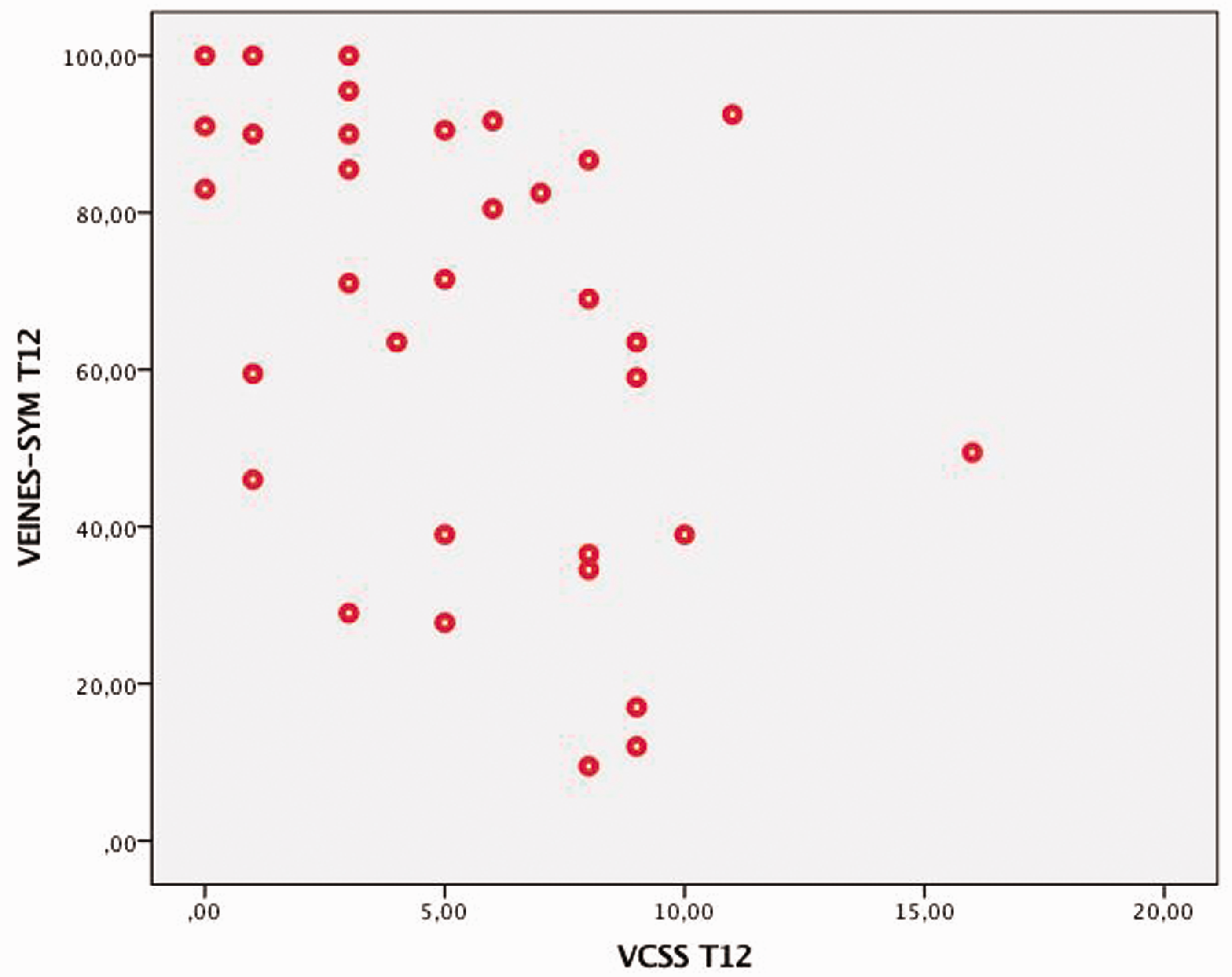
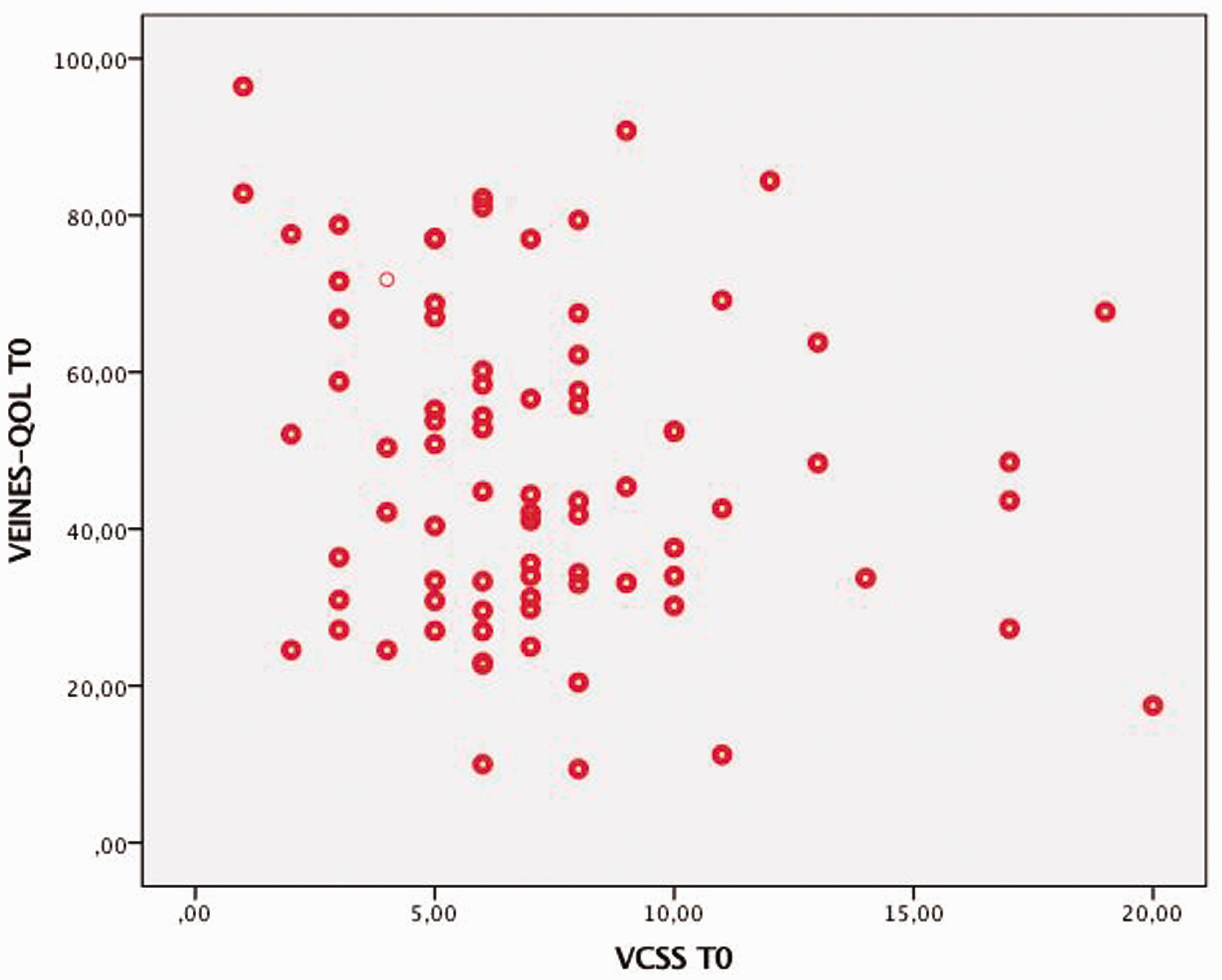
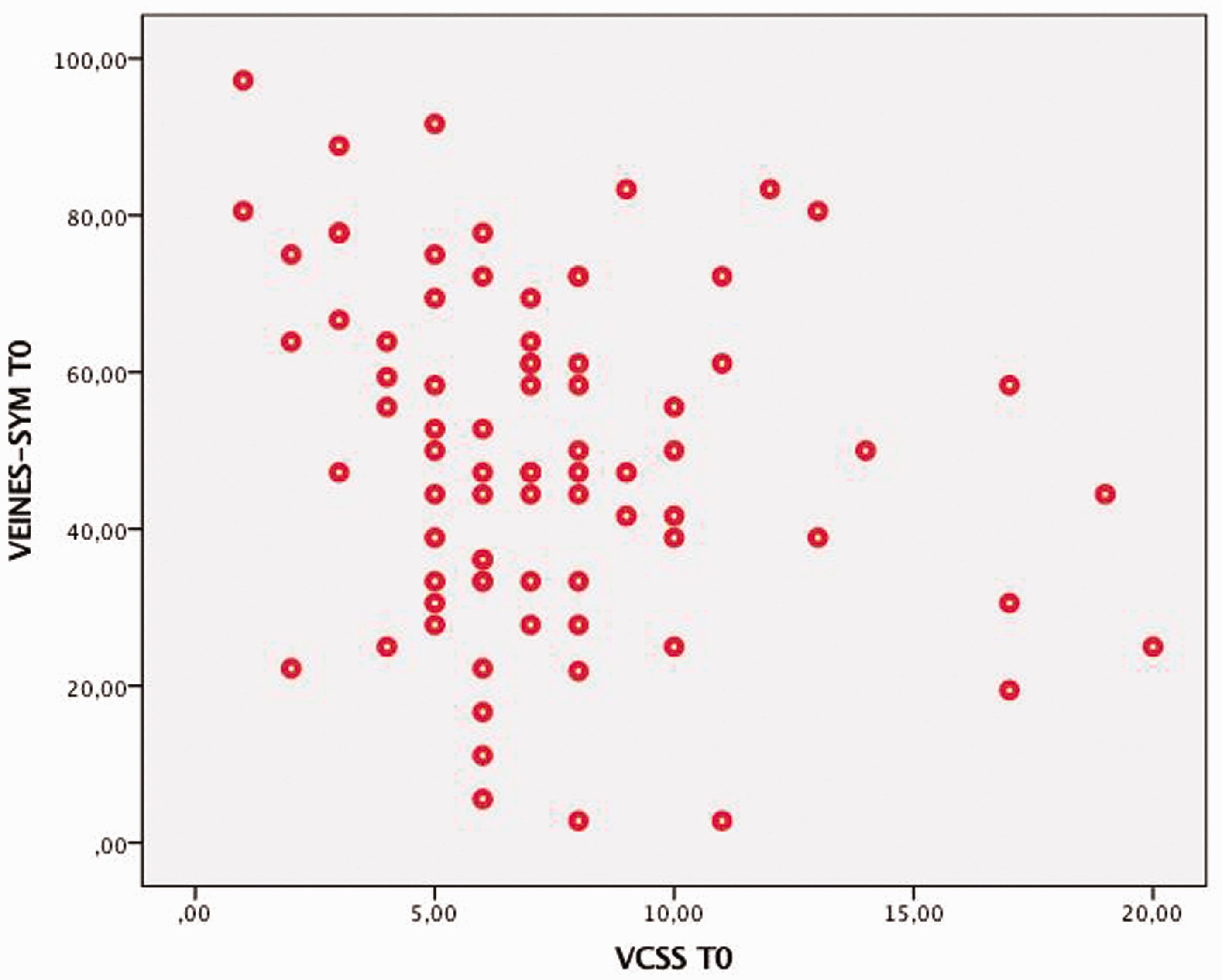
Table 1 shows numbers, means, differences in means and standard deviations at pre-treatment (T0) and at 12 months post-treatment (T12) of the 191 patients used in this study. Because of missing values, the number of completed VQS scores declines at T12 and only about 42% of the corresponding VCSS scores could be traced from patient care. This leads to different patient numbers per measurement, ranging from 73 to 188 patients. Table 2 shows the correlations between the VCSS scores and the VQS scores at T0 and T12. Both the Spearman’s rho and Pearson’s r show a very weak, negative correlation (statistically significant (p ≤ 0.05)), between the VCSS and VEINES-QOL at T12 and between the VCSS and the VEINES-SYM at both T0 and T12. This negative correlation was not statististically (p ≥ 0.05) confirmed for VCSS and VEINES-SYM at T0. Figures 1 to 4 show the scatterplots of the four relationships examined. The points in the scatterplot show the measured VCSS score and its corresponding VEINES-QOL or -SYM for the same patient. The form of the shown scatterplots is indicative for the absence of a strong correlation between the two measurements.
Scatterplot of the relationship between the VCSS score (X-axis) and VEINES-QOL score (Y-axis) at T0. Scatterplot of the relationship between the VCSS score (X-axis) and VEINES-SYM score (Y-axis) at T0. Scatterplot of the relationship between the VCSS score (X-axis) and VEINES-QOL score (Y-axis) at T12. Scatterplot of the relationship between the VCSS score (X-axis) and VEINES-SYM score (Y-axis) at T12. Means, standard deviations and mean differences between VCSS scores and VEINES-QOL/Sym scores at T0 and T12. VCSS: venous clinical severity score. Correlations between VCSS scores and VEINES-QOL/Sym scores at T0 and T12. (Significant P values in bold). VCSS: venous clinical severity score.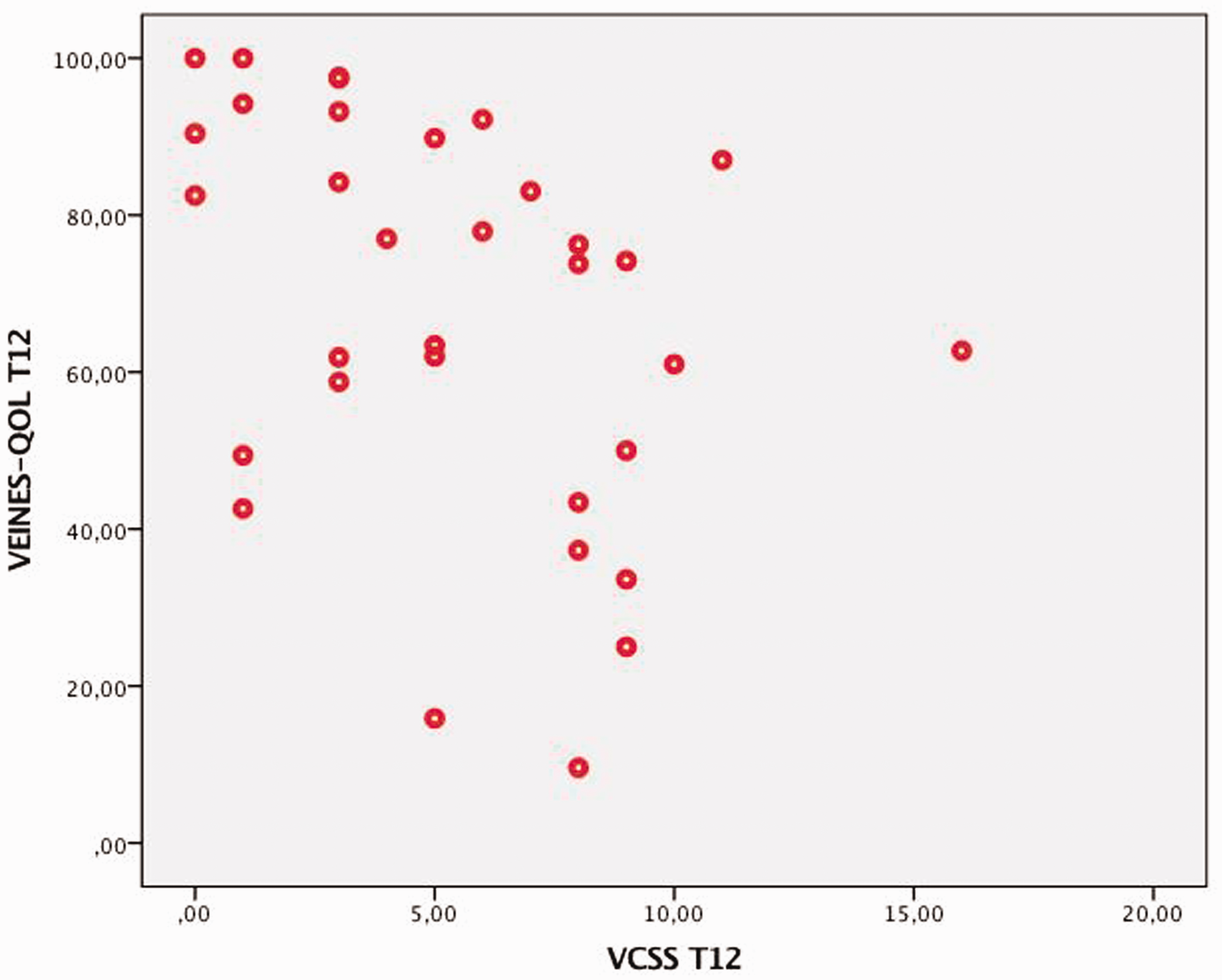


Discussion
The reason for this comparison is to establish whether the VCSS is a valid and sensitive score, responsive for treatment effect when used in deep venous pathology. The VQS is already known to correlate well with outcomes such as patency and the extent of pathology. 16 Failed interventions show less improvement and sometimes even a decrease in VQS scores. Also the extent of the pathology correlates with the VQS, prolonged extended pathology results in lower (worse) scores.7,16 Thus a responsive and specific severity score should be expected to follow suitable disease-specific QoL measurements such as the VQS. A combination of a physician reported severity score, patient-reported QoL and symptom score should in theory give a more objective measurement of disease progression and treatment outcome.
The two measures (Pearson’s r and Spearman’s rho) used to determine the correlation between the VCSS and VQS scores show a statistically proven (p ≤ 0.05) weak negative correlation between −0.2 and −0.4. This means that roughly 20% to 40% of the data points are on the same line, which is very weak for a correlation. For this cohort of patients, the VCSS and the VQS apparently disagree on the disease impact and/or treatment response.
This negative correlation did not reach statistical significance for the VEINES-QOL and VCSS at T0, probably because of a type II error caused by missing VCSS scores. This illustrates the importance of registering clinical scores.
The described cohort of patients suffered from various degrees of DVO and was treated with angioplasty, stenting and optionally with an endophlebectomy. Beside imaging and per-procedure confirmation of pathology, most of these patients suffered from severe venous claudication. The VQS scores show trends accordingly. We have made no selection in specific treatment and/or pathology because it is already established the VQS is responsive for these differences. Thus, VQS improvement should correlate to a decrease in VCSS scores and vice versa. But unfortunately this was found not to be true, the VCSS scores do not seem to relate at all with the VQS scores.
There are multiple theories for this discrepancy. First of all, the VCSS was developed with varicose veins in mind. Varicose veins have a different disease profile when compared to deep venous obstructive disease. Varicose vein symptoms tend to focus more on skin problems such as redness, itching and discoloration. Also, varicose veins affect mainly the superficial venous anatomy of the lower extremities, resulting in visible varicosities, ulceration and restless legs. As such, the VCSS focuses specifically on these symptoms and lacks a number of symptoms more prevalent in deep venous pathology, such as venous claudication, deep venous thrombosis, groin and pelvic discomfort and/or pain after exercise. Some symptoms, such as pain, varicosities and leg swelling, occur in both types of disease. The main goal of interventional treatment in DVO is different from varicose veins though, focusing more on debilitating symptoms such as venous claudication and pelvic pain after exercise. This can explain why the VQS score changes are much more consistent with disease and treatment results than the compared VCSS scores.
An alternative theory is that the severity perceived by the physician differs from the true impact of the disease on the QoL as perceived by the patient. The most debilitating symptoms in our patient population are mostly invisible and not detected during routine physical examination. It might very well be possible that this results in an underestimated disease burden from the perception of the physician.
Nevertheless, this cohort of patients with DVO shows that in order to accurately assess the severity on their disease and the effect of treatment in a standardized way the VCSS does not suffice. In order to identify if this is the result of underestimation by the physician or caused by non applicable items in the score is hard to tell. Further research and perhaps some experimentation with VCSS variants are warranted.
Conclusion
Both the Spearman’s rho and Pearson’s r show a very weak, negative correlation (statistically significant (p ≤ 0.05)), between the VCSS and VEINES-QOL at T12 and between the VCSS and the VEINES-SYM at both T0 and T12. Therefore, the physician scored VCSS of patients treated for deep venous obstructive disease do not correlate well with their self-reported QoL and symptom scores.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.