
Abstract
Chronic upper extremity venous outflow occlusion (UEVOO) occurs frequently among hospitalized patients as a result of various anatomical or pathological etiologies. This includes venous thoracic outlet syndrome, catheter-related injury, malignancy, and hypercoagulable states. While open surgical and endovascular therapies have increasingly been utilized in managing UEVOO, many patients can still be successfully managed with non-invasive therapies. In this review, we will discuss how conservative measures such as anticoagulation and compression therapy can be applied to different causes of UEVOO. The optimal treatment of patients with chronic upper extremity occlusion can be accomplished by deciding which patients will be most likely to benefit from conservative management.
Introduction
Upper extremity deep venous thrombosis (DVT) is a common condition diagnosed among patients hospitalized with comorbid medical conditions. It is estimated that nearly 10% of the acute DVT occur in the upper extremity deep veins, which equates to an annual incidence of between 0.5 to 1 cases per 10,000 people in westernized nations.1,2 When central venous thrombosis occurs, it may involve one or more segments of the axillary, subclavian, or innominate veins, as well as extension into the superior vena cava (SVC). Chronic upper extremity venous outflow occlusion (UEVOO) occurs when these thrombosed venous segments fail to re-canalize. This typically is the result of fibrous conversion of the thrombus within the vein following the initial DVT. The chronicity of upper extremity venous occlusion is evidenced by ample venous collateralization, which is usually found across the entire thoracic outlet (Figure 1(a) and (b)).
Venography demonstrating chronic upper extremity venous outflow occlusion in patients with (A) prior indwelling catheter for hemodialysis; and (B) implantable leads for cardiac pacemaker. Arrows show robust network of collateral veins that have developed in the thoracic outlet of these patients to achieve adequate venous outflow.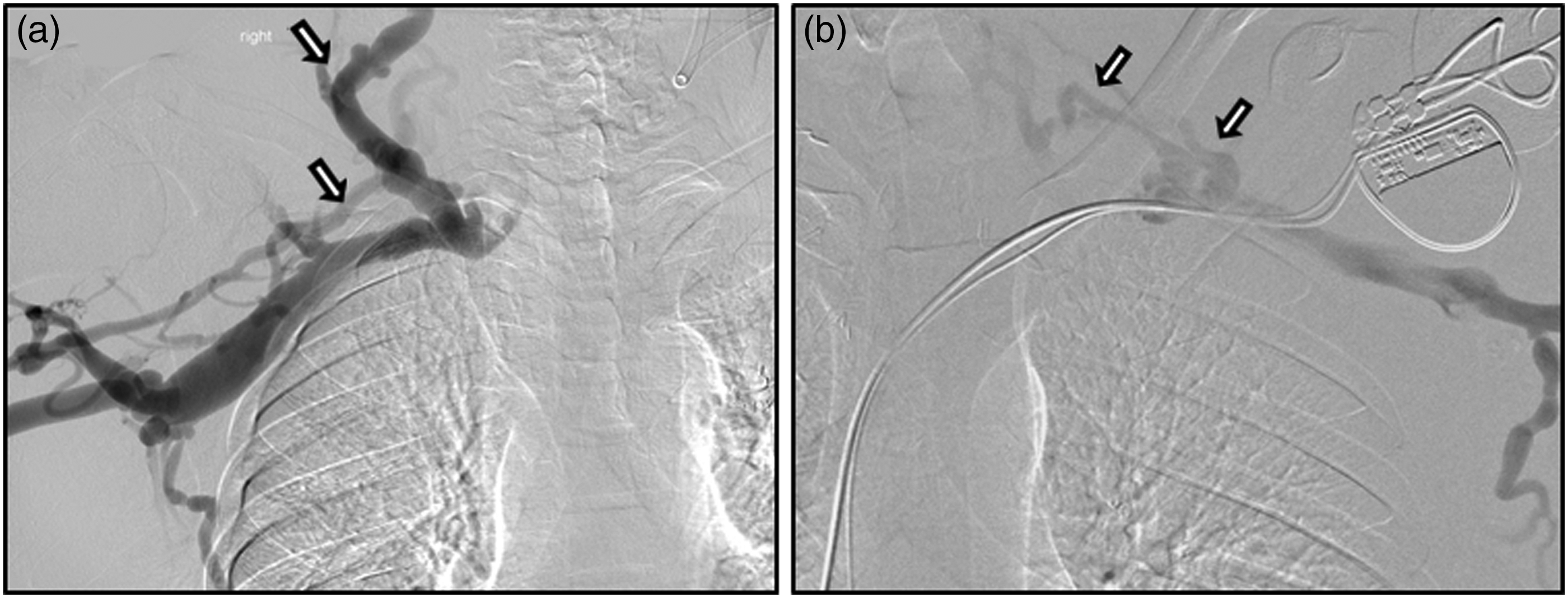
While some patients with UEVOO remain asymptomatic and do not seek treatment, a significant proportion of patients will develop post-thrombotic obstructive symptoms or complications that require management and treatment. The incidence of post-thrombotic syndrome in the upper extremities has been reported to range between 7% and 46% of patients depending on etiology. 3 Patients are also known to at risk of recurrent thrombosis of collateral and re-canalized upper extremity veins. It is important to understand what treatment options are available for patients that present with UEVOO.
Patients with UEVOO have historically been treated with conservative measures such as arm elevation, heat, and oral anticoagulation during the acute phase.4,5 But over the past 40 years, a number of contemporary open surgical and endovascular treatments have been introduced and advanced for the treatment of acute venous outflow thrombosis and the development of chronic occlusion.6,7 This includes catheter-based endovascular therapies as well as thoracic outlet decompression surgery. While these different invasive therapies have significantly improved management options and outcomes for patients with UEVOO, they also carry a significant risk of complications and morbidity. Complications from open and endovascular treatments occur in up to 20% of patients and include wound hematomas, bleeding complications, nerve injuries, pneumothorax, chylothorax, pulmonary embolism, and chronic postoperative pain syndromes. 8 Moreover, a recent systematic review showed that 30% of patients undergoing surgical intervention for upper extremity thrombosis and occlusive disease had no improvement in symptoms following therapy. 5 While it is recognized that open and endovascular treatments are necessary and beneficial for many patients with UEVOO, there are no published evidence-based guidelines to help direct management and a significant number of selected patients may benefit from established conservative measures and not need to be subjected to the risk of invasive therapies.
In this review, we will discuss the etiology of chronic upper extremity outflow occlusion and provide an algorithm for how to select appropriate conservative management as compared to invasive treatment. The different primary and secondary causes of UEVOO each mandate consideration of different management strategies that may be tailored to each individual patient. The optimal management of UEVOO can be accomplished by deciding which patients will be most likely to benefit from conservative measures.
Clinical presentation of chronic upper extremity venous occlusion
When patients are diagnosed with UEVOO, the first step in the management algorithm is to assess the clinical presentation along with severity and chronicity of symptoms (Figure 2). Up to three-quarters of individuals diagnosed with UEVOO are hospitalized patients with comorbid conditions and may present with a wide spectrum of signs and symptoms. The diagnosis of UEVOO may be an incidental finding when a computed tomography, angiogram, or ultrasound study is performed for another indication. Between 5% and 10% of patients are asymptomatic and do not seek treatment.
1
Asymptomatic patients are usually found to have a robust network of collateral vessels in the thoracic outlet that provide sufficient venous outflow. A chronic occlusion in the subclavian vein may lead to large collaterals to the internal jugular vein, which can be seen on this venography (Figure 1(a)).
Algorithm for selecting appropriate conservative and invasive management of patients with different etiologies for chronic upper extremity venous outflow occlusion.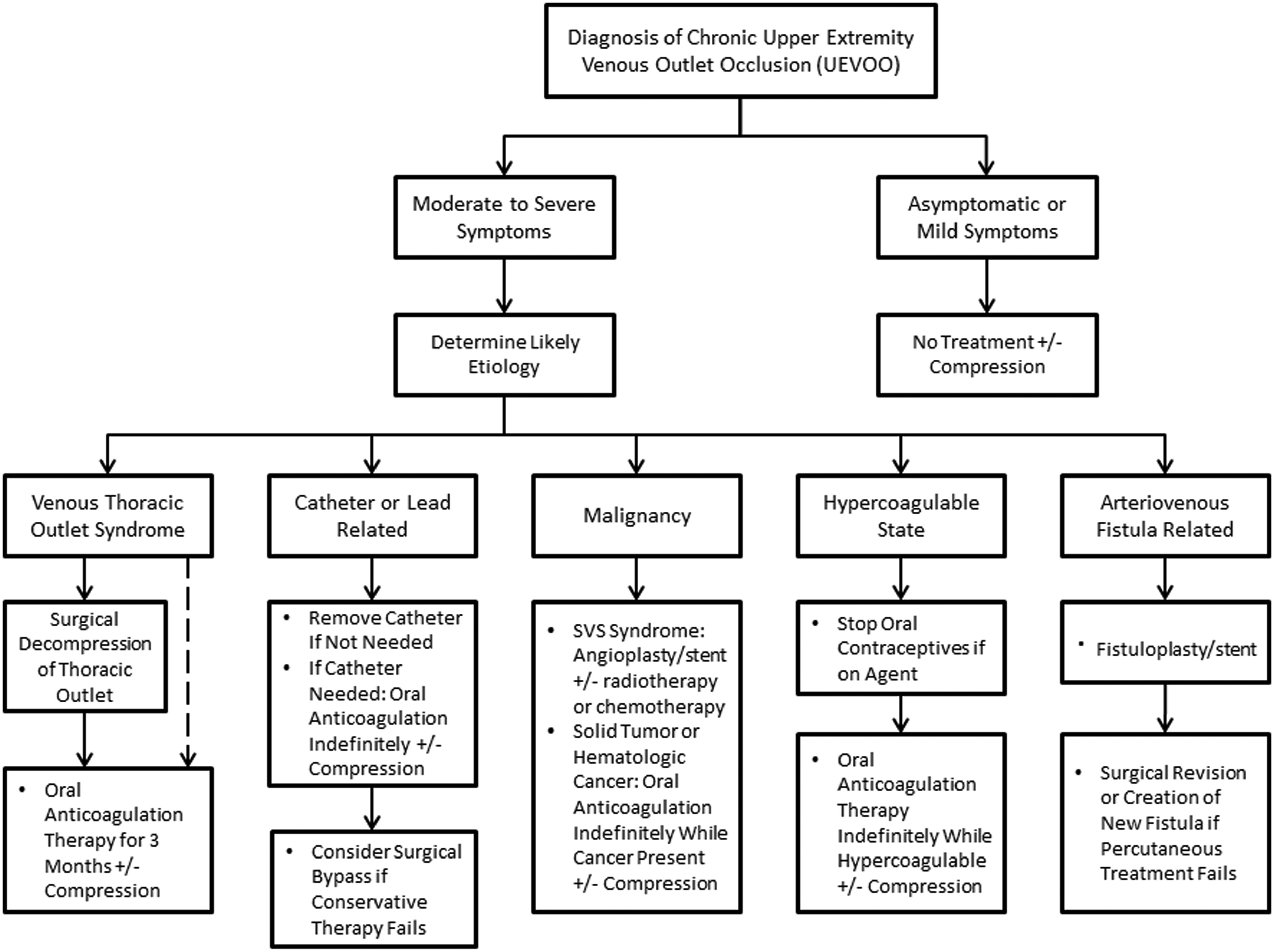
While some patients with UEVOO are asymptomatic, the vast majority of patients will present with some degree of symptoms that vary with chronicity. The incidence of post-thrombotic syndrome in the upper extremity ranges from 7% to 46%, which is similar to the lower extremity. 3 Establishing the duration and severity of symptoms is important for determining what type of treatment is needed. The most common symptoms are arm swelling in approximately 80% of patients and pain in 30% to 50% of patients. 9 Swelling may involve the entire arm and hand, which may be disabling in many cases. Patients may also frequently complain of heaviness, supraclavicular fullness, jugular venous distention, cyanosis, and dilated subcutaneous veins around the shoulder girdle. However, chronic venous insufficiency leading to venous ulcers in the upper extremity is very rare. 10
Etiology and pathogenesis of chronic upper extremity venous occlusion
If patients diagnosed with UEVOO have moderate to severe lifestyle limiting complications, the next step is to establish the likely etiology (Figure 2). The etiology of UEVOO can be divided into primary and secondary causes. Primary causes include venous thoracic outlet syndrome or effort thrombosis, and idiopathic thrombosis without any defined risk factors. 7 Secondary causes of UEVOO are more common than primary, and account for 80% of upper extremity DVT. 9 The most frequent secondary causes of UEVOO are related to indwelling catheters or leads, including central venous catheters, peripherally inserted central catheters, pacemakers, or defibrillators. 11 The presence of an arteriovenous (AV) fistula also increases the risk of UEVOO in the ipsilateral arm. Other secondary causes are the presence of cancer, history of coagulation disorders, trauma, and other conditions that are known to lead to a hypercoagulable state. We will review each of these etiologies and their management in more detail below.
Venous thoracic outlet syndrome
The most common primary etiology of UEVOO is associated with venous thoracic outlet syndrome (vTOS), which is also known as effort thrombosis or Paget-Schroetter syndrome. About 80% of cases occur in the dominant arm of young otherwise healthy adults who participate in activities involving repetitive upper limb motion or exercise. 12 This typically involves repetitive ipsilateral abduction and external rotation of the arm. Patients with vTOS are commonly are found to have an anatomic abnormality that causes external compression of the subclavian vein as it travels through the thoracic outlet. 13 This anatomic space is defined by the intersection of the clavicle, first rib, and costoclavicular ligament anteromedially and the anterior scalene muscle posterolaterally. Repeated micro-trauma to the subclavian vein caused by anatomic compression in the thoracic outlet induces subsequent endothelial damage and stenosis with intraluminal fibrosis. During surgical exploration, scarring is also typically found around the subclavian vein where it courses between the clavicle, first rib, and anterior scalene muscle. Ultimately, this combination of external compression, internal fibrosis and venous stasis leads to effort-thrombosis and occlusion of the subclavian vein.
Symptoms related to chronic vTOS are variable, and most patients typically present with position-dependent arm swelling and some degree of cyanosis. 7 In some patients, symptoms may be brought on during provocative tests such as those elicited by the Wright maneuver or Eden’s test, although the diagnostic accuracy of these maneuvers is marginal. 7 Patients may also present with concomitant neurological symptoms due to compression of the brachial plexus.
The severity of symptoms along with a patient’s age and comorbid status are important factors to weigh when deciding to pursue operative versus conservative management in UEVOO related to vTOS. Young healthy patients with lifestyle-limiting symptoms associated with chronic vTOS have been shown to benefit from surgical decompression of the thoracic outlet, consisting of first rib resection with anterior scalenectomy. Following surgical decompression of the thoracic outlet, treatment with post-operative anticoagulation has been shown to be successful in luminal re-canalization of the subclavian vein on average after seven months of therapy. 13 Anticoagulation can be stopped after symptoms resolve and patency of the upper extremity veins are confirmed.
On the other hand, the evidence for surgical decompression in older patients with chronic vTOS is less clear. In fact, several studies have demonstrated that a large proportion of patients with vTOS can be managed with anticoagulation therapy, particularly if symptoms are mild. In a study by Lee et al., 8 it was shown that 41% of patients with Paget-Schroetter were successfully managed with conservative therapy and did not need to undergo surgery. Another group supported these findings showing that 77% remained symptom free at a median follow-up of 55 month with only a short 3-month period of anticoagulation. 14 Patients that failed non-operative treatment in this study were younger and more likely to be athletes. These findings suggest that non-operative management is another viable option for selected patients with UEVOO associated with vTOS.
Indwelling catheter and leads
Indwelling catheter and implantable leads account for the majority of secondary causes of UEVOO. Approximately 25% of patients who undergo prolonged central venous cannulation will experience deep venous thrombus or venous occlusive disease, although it is not recognized in many patients. This includes chronic indwelling central lines, port systems, or dialysis catheters in the subclavian and axillary veins. Implanted pacemaker or defibrillator leads within the central veins may also result in DVT and occlusion. Catheters with multiple or large lumens are thought to have the highest risk of causing thrombosis. Peripherally inserted central catheters (e.g. PICC lines) also pose a risk for UEVOO, with nearly 5% of patients developing a DVT after insertion. 15 How the device is used also influences the risk of complications, with catheters used for bolus chemotherapy and total parenteral nutrition known to be at a higher risk of thrombosis and occlusion.
The UEVOO symptoms caused by indwelling catheters and leads are typically less severe than other etiologies associated with this condition. Some patients with catheter-related UEVOO may not have any symptoms and the inability to aspirate the catheter may be the first sign of venous occlusion. Given that venous occlusion typically occurs over a more gradual time span, many patients are able to develop a robust network of collaterals across the occluded segments in the thoracic outlet (Figure 1(a) and (b)). This likely explains why the post-thrombotic syndrome occurs less frequently in patients with catheter and lead-associated thrombosis and occlusion. 10
If patients develop symptomatic UEVOO while indwelling catheters are in place, a decision has to be made whether the catheter is still needed (Figure 2). If the indwelling catheter is not actively being used and other options for venous access remain, it should be removed and the decision to start anticoagulation made depending on the severity of patient symptoms. Many patients may not need anticoagulation after the catheter is removed, particularly if their symptoms are mild. On the other hand, a trial of anticoagulation should be initiated if an indwelling catheter is still being actively used for intravenous administration of medications or blood sampling. If symptoms resolve with anticoagulation therapy alone, this should be continued indefinitely while the indwelling catheter is in place. If symptoms do not resolve with anticoagulation alone, a decision must be made to remove the catheter and other sites for catheter placement should be considered. All patients with persistent UEVOO symptoms related to catheter use may also be considered for compression therapy with or without the use of concurrent oral anticoagulation.
Malignancy
Malignancy is another common secondary cause of UEVOO, which is found in nearly 40% of patients who are diagnosed with an upper extremity DVT. 11 Cancer may induce a pro-thrombotic state in the upper extremity deep venous system through several different mechanisms. 6 This includes thrombophilia associated with tumors such as lung adenocarcinoma, non-Hodgkin’s lymphoma, breast tumors, and ovarian cancer. Chemotherapy regimens used to treat these various tumors are also known to induce coagulation abnormalities and commonly require the use of chronic indwelling central venous catheters that independently increase the risk of UEVOO as described above. Finally, thoracic tumors may infiltrate or compress the central veins or SVC leading to SVC syndrome.
The management of patients with UEVOO related to malignancy depends on the mechanism of tumor involvement and severity of symptoms (Figure 2). For SVC syndrome, the severity of symptoms depends on the recruitment of central collaterals, which typically come from the azygous and hemi-azygous veins. Patients with moderate to severe symptoms related to SVC syndrome may require endovascular treatment with angioplasty and stenting, along with radiation or chemotherapy to palliate symptoms. In the absence of SVC syndrome, most symptomatic patients with UEVOO related to malignancy can be successfully treated with anticoagulation therapy with or without compression therapy. This is particularly true for cancer patients who need a central venous catheter for chemotherapy or total parenteral nutrition, where anticoagulation will decreases the risk of progressive thrombosis. In general, anticoagulation therapy should be continued in patients as long as the malignancy is thought to remain active.
Hypercoagulable state
There are a number of different pathological and physiological conditions that create a hypercoagulable state and contribute to secondary causes of UEVOO. This includes recognized congenital thrombophilia or acquired coagulation defects. 9 A prospective registry of patients with thrombosis showed that 35% of patients with upper extremity DVT was diagnosed with at least one known hereditary thrombophilia, including factor V Leiden mutation, prothrombin G20210A mutation, anti-phospholipid antibodies, protein C deficiency, protein S deficiency, or anti-thrombin deficiency. 16 Other conditions that may create hormone-induced coagulation abnormalities include pregnancy, use of oral contraceptives, and the ovarian hyper-stimulation syndrome. 6 Finally, surgery or trauma to the upper extremity may stimulate a hypercoagulable state that is exacerbated by venous stasis from arm or shoulder immobilization and/or casting.
Among patients with UEVOO who are identified as having a hypercoagulable state, the first step in management is to identify if any hypercoagulable risk factors are modifiable. If patients are taking oral contraceptive therapy, this agent should be stopped if possible (Figure 2). Otherwise, anticoagulation therapy should be started and maintained as long as a known hypercoagulable state is present. Patients diagnosed with a hereditary thrombophilia may benefit from consultation with a Hematologist or thrombosis specialist in order to help select the most appropriate long-term anticoagulation therapy agent.
AV fistula
Among patients with end stage renal disease, the presence of an AV fistula in the upper extremity for hemodialysis is another secondary cause of UEVOO in the ipsilateral limb. The pathogenesis of this condition is thought to be related to impaired vasodilation and endothelial dysfunction in the outflow veins brought on by uremic factors that deplete nitric oxide. In addition, many patients with end stage renal disease have had a history of prior subclavian cannulation for vascular catheter access. 15 The development of central venous stenosis from indwelling catheters as described above may remain asymptomatic until creation of an AV fistula in the ipsilateral arm. Clinical factors during hemodialysis that suggest UEVOO may include increased venous pressures with backflow into the arterial needle, prolonged bleeding times, and inefficient or inadequate dialysis.
The management of UEVOO in the ipsilateral arm of a patient with a functional AV fistula nearly always requires open or endovascular treatment to maintain patency. A fistulogram may be performed to confirm the UEVOO followed by balloon angioplasty or stenting of the venous outflow occlusive disease as needed (Figure 2). Restenosis remains a major problem after percutaneous treatment of UEVOO and commonly requires multiple repeat endovascular interventions or surgical revision to maintain a functioning AV fistula.
Options for conservative management of upper extremity venous occlusion
Anticoagulation
Anticoagulation therapy is the cornerstone of conservative management for patients with UEVOO across the spectrum of etiologies (Figure 2). Symptomatic patients with chronic upper extremity venous occlusion benefit from anticoagulation through a number of different mechanisms, including prevention of thrombus propagation, maintenance of venous collaterals, and promotion of luminal re-canalization. These therapeutic effects may in turn help prevent the long-term sequelae of chronic venous insufficiency and post-thrombotic syndrome in patients with UEVOO.
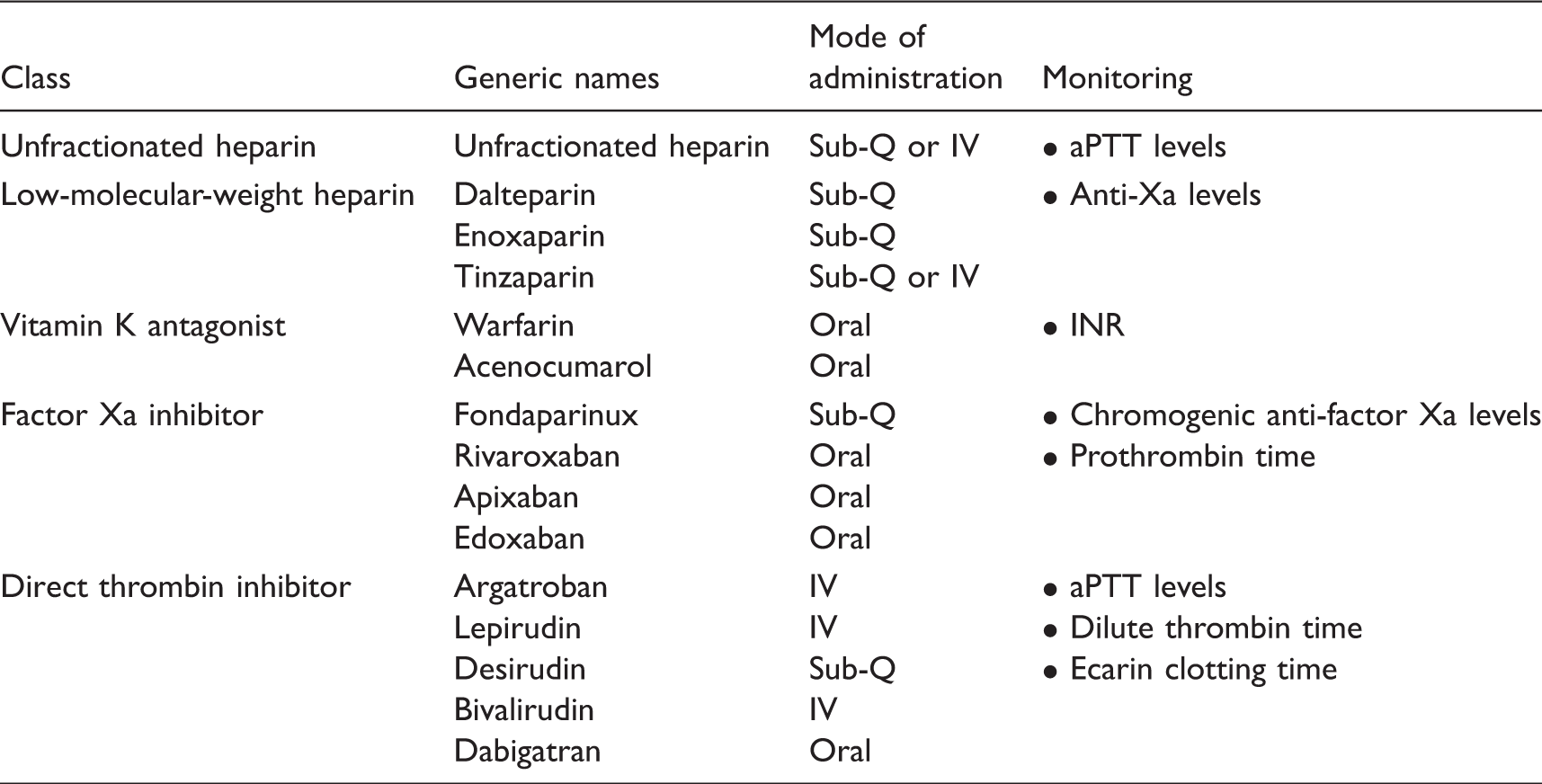
Pharmacological options for systemic anticoagulation.
Compression therapy
Compression bandages and sleeves have traditionally been used to treat patients with upper extremity lymphedema. But there also may be a practical application for this type of treatment in UEVOO.18,19 In comparison to compression sleeves for lymphedema, however, graduated compression must start in the hand (Figure 3). The use of compression therapy is not recommended in the acute phase of UEVOO, although many patients with chronic upper extremity venous insufficiency or persistent post-thrombotic disorder may benefit from this type of therapy.
17
Example of compression sleeve that could be worn in patients with post-thrombotic symptoms related to chronic upper extremity venous outflow occlusion.
The physical properties of compression therapy rely upon interface pressure and stiffness of the hosiery. 20 The interface pressure is exerted by the compression fabric on the skin area and is calculated using Laplace’s law, which is directly proportional to the tension of the hosiery and inversely proportional to the radius of the limb to which it is applied. The pressure exerted by compression sleeves is typically measured in units of mmHg, and commercially available compression sleeves typically range between 10 and 40 mmHg. The stiffness of the sleeve depends on the elastic properties of the fabric and is defined by the increase in fabric interface pressure induced when muscles are contracting and the circumference of the limb expands.
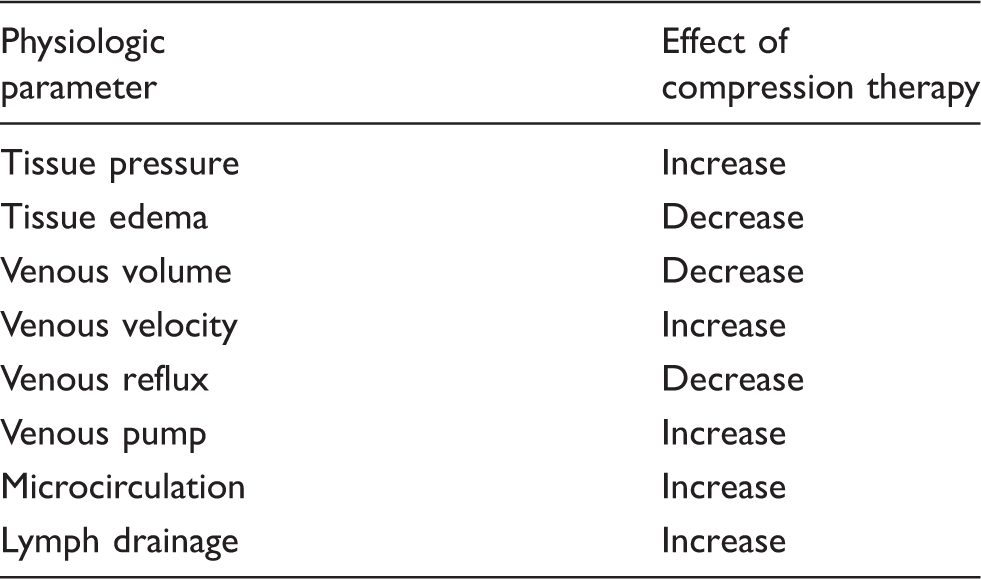
Physiological effects of sleeve compression therapy.
Conclusion
Chronic UEVOO results from a number of diverse anatomical and pathological causes. While some patients remain asymptomatic, the vast majority of patients require some form of treatment. Conservative measures including oral anticoagulation and compression therapy can be applied to large proportion of patients depending on the etiology and the severity of symptoms. We provide an algorithm for helping to select patients for conservative management of UEVOO. With proper selection, a large proportion of patients with UEVOO can avoid the risks associated with undergoing invasive treatments for this condition.
Footnotes
Acknowledgements
I would like to thank Dr. Cees Wittens for the opportunity to prepare this chapter and present work at the 2016 European Venous Course.
Contributorship
BB researched literature and was responsible for all aspects of preparing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Institutional Review Board review or approval was not required for this type of review article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
BB