
Abstract
Approximately 10% of all cases of deep vein thrombosis (DVT) occur in the upper extremities. The most common secondary cause of upper-extremity DVT (UEDVT) is the presence of a venous catheter. Primary UEDVT is far less common and usually occurs in patients with anatomic abnormalities of the costoclavicular space causing compression of the subclavian vein, called venous thoracic outlet syndrome (VTOS). Subsequently, movement of the arm results in repetitive microtrauma to the vein and its surrounding structures causing apparent ‘spontaneous’ thrombosis, or Paget-Schrötter syndrome. Treatment of UEDVT aims at elimination of the thrombus, thereby relieving acute symptoms, and preventing recurrence. Initial management for all UEDVT patients consists of anticoagulant therapy. In patients with Paget-Schrötter syndrome the underlying VTOS necessitates a more aggressive management strategy. Several therapeutic options exist, including catheter-directed thrombolysis, surgical decompression through first rib resection, and percutaneous transluminal angioplasty of the vein. However, several controversies exist regarding their indication and timing.
Introduction
Approximately 10% of all cases of deep vein thrombosis (DVT) occur in the upper extremities, adding up to a yearly incidence of 0.4–1 cases per 10,000 individuals. 1 Upper-extremity deep vein thrombosis (UEDVT) is classified as either primary or secondary based on aetiology. ‘Secondary’ UEDVT refers to the presence of a predisposing factor such as malignancy, central venous lines, and pacemaker or defibrillator leads. Catheter-associated UEDVT accounts for the majority of secondary UEDVT cases. 2 The overall incidence of UEDVT is rising, mainly due to the increasing use of central venous catheters (CVCs), peripherally inserted central catheters in particular. 3
Primary UEDVT is far less common than secondary UEDVT, comprising 20% of all UEDVT cases. It often occurs after strenuous activity of the arm, thus primary UEDVT is commonly referred to as ‘effort(-related) thrombosis’. 2 Most patients with primary UEDVT have underlying anatomic abnormalities of the costoclavicular space, causing compression of the subclavian vein. This is also known as the thoracic outlet syndrome (TOS), yet for venous obstruction a more logical denomination would be thoracic inlet syndrome. The resultant repetitive microtrauma to the vein intima leads to apparent ‘spontaneous’ thrombosis. James Paget first described this clinical entity in 1875. 4 Subsequently, Von Schrötter was the first to explore the role of vascular trauma as a pathogenic factor. 5 In the 20th century the term Paget–Schrötter syndrome was coined for this condition. Despite differences in pathogenesis, the clinical manifestations of both primary and secondary forms are similar.
This chapter will cover both primary and secondary UEDVT. Diagnosis and treatment strategies will be discussed, as well as controversies around the management of this condition.
Diagnosis
The clinical manifestations of UEDVT include unilateral swelling, discomfort, and discoloration of the affected arm. Furthermore, prominent superficial (collateral) veins, low-grade fever and, although rare, development of superior vena cava syndrome can be present. 3 Occasionally, a pulmonary embolism is the first clinical manifestation. While these manifestations may raise suspicion of UEDVT, diagnosis should be confirmed by additional diagnostic testing, as clinical manifestations alone carry low specificity. 3
The diagnostic strategy for UEDVT is under debate, as no validated approach exists. Contemporary guidelines, proposed by Bates et al., 6 are largely consensus based. Plasma D-dimer levels are commonly used to rule out DVT of the lower extremities. However, many patients with suspected UEDVT have comorbid conditions associated with elevated D-dimer levels limiting its use in the diagnostic workup. 7 Duplex ultrasonography is most commonly used as initial test for suspected UEDVT. A duplex ultrasound may reveal abnormal Doppler patterns indicating absence of venous flow. This is suggestive of the presence of DVT, especially in a vein that cannot be compressed. 3 When duplex ultrasound is inconclusive, while clinical symptoms strongly indicate UEDVT, either contrast-enhanced computed tomography or magnetic resonance imaging (MRI) can be performed. However, data on their diagnostic accuracy is scarce. 7 Nonetheless, these diagnostic modalities help provide visualisation of the proximal veins in the arm, a region where the diagnostic capacity of ultrasound is limited. 3 Concurrently, MRI can be useful in the diagnosis of underlying pathology including malignancy or anatomic abnormalities at the level of the thoracic outlet. Phlebography (also called venography) is generally not required for the diagnosis of UEDVT. While it provides adequate imaging of the venous anatomy, phlebography requires cannulation of the veins of the affected arm. Therefore, we only use it in conjunction with catheter-directed thrombolysis.
The diagnostic process for primary UEDVT is similar to the algorithm for secondary UEDVT. However, we perform an additional chest x-ray to reveal possible anatomical abnormalities. Namely cervical ribs, although these are rarely associated with venous TOS (VTOS), and callus induced by a medial clavicular fracture.
Management of secondary UEDVT
With the growing use of CVCs, secondary UEDVT is increasingly common.3,8 Patient-related risk factors for catheter-associated UEDVT are the presence of cancer and a history of DVT. Variables accompanying the insertion of the catheter are related to the development of an UEDVT as well (i.e. number of insertion attempts, catheter size and type, vein selection, depth of insertion, operator).8,9 In the absence of a CVC other causes include paraneoplastic syndrome, surgery, or trauma of the arm or shoulder, pregnancy, oral contraceptive use, and hereditary or acquired thrombophilia. 2
Treatment of UEDVT aims at elimination of the thrombus, thereby relieving acute symptoms, and preventing recurrence. Additionally, complications such as pulmonary embolism and post-thrombotic syndrome (PTS) should be prevented. Our therapeutic algorithm is depicted in Figure 1 and will be elucidated in the following sections. Initial management for all UEDVT patients consists of anticoagulant therapy. Low-molecular weight heparin (LMWH) in a therapeutic dosage as first-line treatment, immediately followed by vitamin K antagonists, is most commonly used. We aim for an international normalised ratio (INR) of 2.5–3.5. The use of LMWH over unfractioned heparin is based on data from studies investigating lower extremity DVT.
2
Accordingly, studies on the optimal duration of anticoagulant therapy in patients with UEDVT are lacking. In our centre we follow the guideline from the American College of Chest Physicians (ACCP), arbitrarily recommending anticoagulation for at least three months.
10
Long-term use of anticoagulation for more than six months may be indicated in case of recurrent thrombosis or when the underlying cause for the secondary UEDVT is ongoing (i.e. malignancy).
Standard therapeutic algorithm for UEDVT in our hospital. LMWH: low-molecular weight heparin; UEDVT: upper extremity deep venous thrombosis.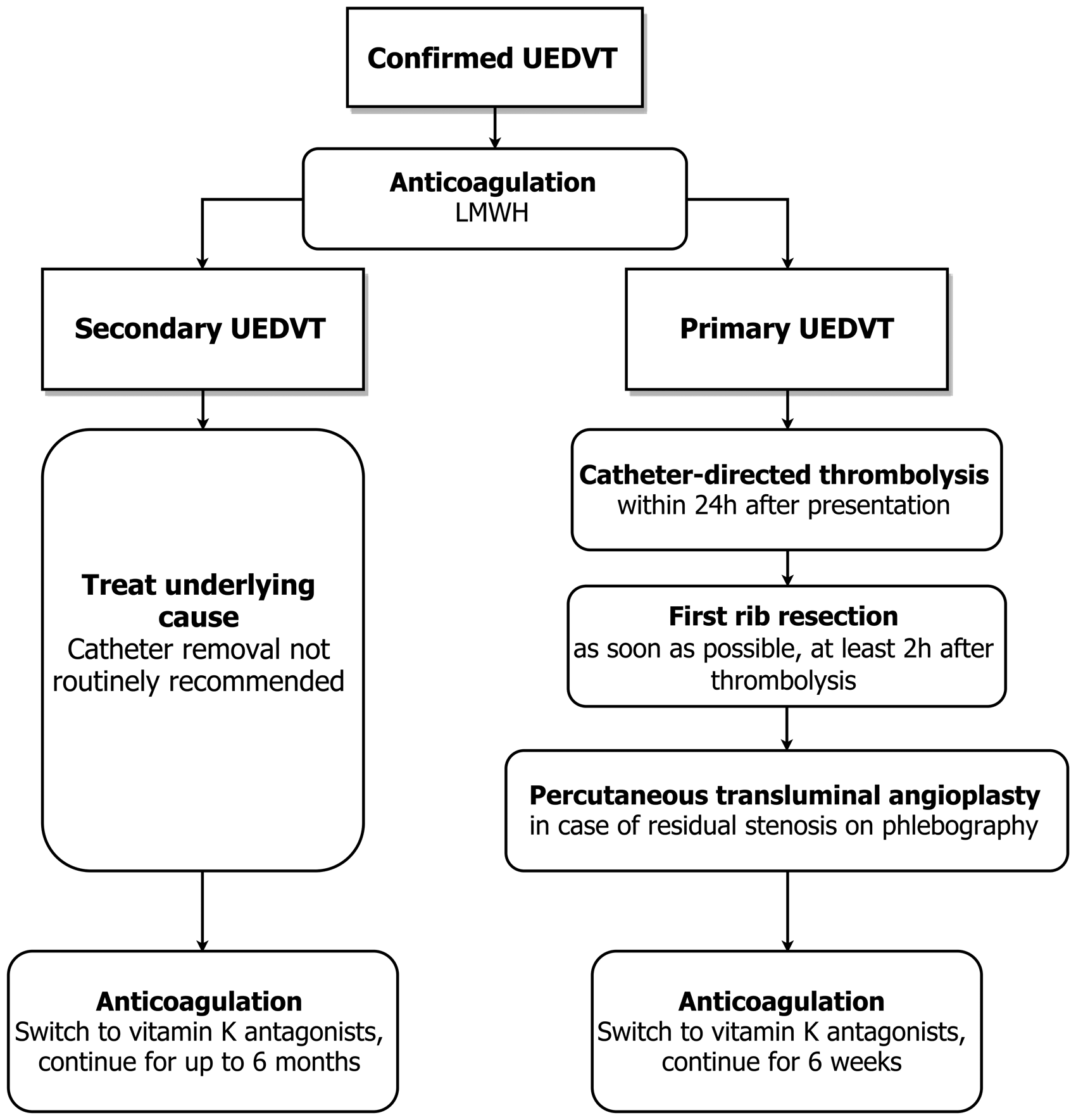
Apart from anticoagulation, the management of secondary UEDVT consists of eliminating the cause whenever possible. However, when this cause is a catheter, routine removal is not recommended: a functional, well placed catheter is safe to maintain.2,6 In some cases the catheter induces progression of the thrombus, or provokes infection, necessitating removal. Removal is also warranted when symptoms of DVT persist despite treatment with anticoagulants, when the catheter malfunctions, or when there is a contraindication to anticoagulation therapy. Unfortunately, studies on optimal timing of removal are lacking. 7
Catheter-directed thrombolysis may remove the thrombus and restore vein patency. However, most of the common causes of secondary UEDVT (i.e. CVCs, malignancy) are a relative contraindication to thrombolytic therapy. Patients with chronic symptoms or PTS are offered compression bandages or sleeves. These may provide some comfort, yet due to lacking evidence on their use in UEDVT they are not routinely recommended in the ACCP guideline. 10 In lower extremity DVT compression therapy is of proven benefit, evidenced by a meta-analysis showing a reduction in the occurrence rate of PTS. 11 Thus, the same might be true in the arm, though compliance with upper extremity compression bandages or sleeves appears to be low.
Management of primary EUDVT
The most common primary form of UEDVT is effort-related thrombosis or Paget–Schrötter syndrome. Underlying VTOS is present in most of these patients. In VTOS, there is a narrowing or occlusion of the subclavian vein, caused by anatomical abnormalities in the thoracic inlet. These abnormalities lead to repetitive microtrauma to the subclavian vein and its surrounding structures with movement of the arm. Subsequently, resultant inflammation, venous intima hyperplasia, and fibrosis may occur, leading to narrowing of the vein and the formation of a thrombus. 7 These pathogenic factors have implications for the diagnostic workup and management of Paget–Schrötter syndrome, as described below.
Thrombolysis
Both primary and secondary UEDVT patients will initially be treated with anticoagulant therapy. The results of anticoagulation alone, however, are unfavourable with high rates of residual venous obstruction and persistence of symptoms, 12 as well as the development of PTS in up to 75% of cases. 13 Thus, for patients with primary UEDVT, catheter-directed thrombolysis should be added to the therapeutic arsenal. Previous research suggests favourable primary patency rates of the vein after catheter-directed thrombolysis, compared with anticoagulation alone. 7 Thrombolysis is feasible when the onset of thrombosis was recent and the patient carries a low risk of bleeding complications. One study assessed the use of thrombolysis in a UEDVT population and showed a rate of complete or partial recanalisation of 97%. 2 Thus, catheter-directed thrombolysis seems highly effective in the elimination of an acute thrombus thereby providing rapid symptom relief. However, with no level 1 evidence available it is unclear whether catheter-based therapy, as compared with anticoagulation alone, actually reduces the risk of recurrence, pulmonary embolism, or PTS in UEDVT. 7 The CaVenT trial (Catheter-Directed Venous Thrombolysis in Acute Iliofemoral Vein Thrombosis) showed a reduction in occurrence of PTS after catheter-directed thrombolysis in lower extremity DVT. 14 These long-term benefits will possibly be substantiated further by upcoming results from the ATTRACT trial (Acute Venous Thrombosis: Thrombus Removal With Adjunctive Catheter-Directed Thrombolysis). 15 The outcomes of a more aggressive approach in the lower extremities add to the retrospective series supporting thrombolysis in UEDVT, despite the absence of a randomised trial in these patients. In our experience, catheter-directed thrombolysis provides excellent results in terms of recanalisation and almost immediate symptom relief. For this reason we try to accomplish thrombolysis within 24 h after presentation for all patients with recent onset of primary UEDVT. An arbitrary time limit of 14 days or less is maintained for this interventional strategy as the outcome of thrombolysis is said to be less favourable after two weeks. 10 However, we have successfully performed thrombolysis up to four weeks after duplex-confirmed UEDVT. Notably, the discrepancy between time of clinical onset of UEDVT and pre-existent subclinical thrombosis in the vein complicates the discussion about the initiation and timing of thrombolysis.
Surgical therapy
Anticoagulant therapy with catheter-directed thrombolysis adequately establishes removal of the thrombus in almost all patients with primary UEDVT. Yet, vein patency is in most cases severely compromised by venous stenosis at the level of the costoclavicular space, caused by mechanical compression and repetitive trauma of the subclavian vein. Adequate decompression of the venous thoracic inlet involves resection of the first rib, the costoclavicular ligament, and the anterior and medial scalene muscle.2,7 Furthermore, resection of fibrotic tissue surrounding the vein, so-called venolysis, is an important part of the procedure. 12 We prefer the most commonly used transaxillary approach to resection. Yet, alternative techniques exist including various combinations of supra-, para-, and infraclavicular approaches, some enabling the addition of open endophlebectomy with vein patch plasty. Also, others suggest sternal disarticulation or medial claviculectomy with first rib resection (FRR).12,16 Complications include hemopneumothorax, nerve injury, hematoma requiring reoperation, and recurrence of thrombosis. 7 Chronically occluded veins, often challenging due to extensive fibrosis, require a tailored approach to surgery depending on lesion characteristics. Surgical options span from endophlebectomy to autologous venous interposition bypass graft but there is little guidance from published series.
Unfortunately, no randomised controlled trial exists to evaluate this approach of FRR. Lee et al. 17 suggest, based on a small series of 35 patients, that FRR should be preserved for patients with persistent complaints after thrombolysis and one to three months of outpatient anticoagulation therapy. They conclude that with this more cautious approach some patients may be spared surgery, with acceptable long-term results. However, the results of a recent review of retrospective case series by Lugo et al. 18 suggest that the addition of immediate FRR to the management of acute effort thrombosis is associated with considerably higher rates of immediate symptom relief, as well as vein patency at follow up. 18 Additionally, in their review, up to 40% of patients who did not receive surgical decompression eventually required surgery for recurrent symptoms. Also, long-term results are favourable, as Urschel and Razzuk 19 report a 95% rate of excellent or good outcomes over 20 years. In accordance with these results other authors state, as we do, that with acute primary UEDVT full recovery is best established by a combination of anticoagulation, thrombolysis, and surgical decompression (FRR) within the first 14 days after onset of UEDVT symptoms.12,20,21 Initial concerns with surgery soon after thrombolysis have led to the propagation of delayed surgery by some authors. Yet this means deferment of definitive correction of the underlying problem while multiple reports have shown immediate decompression to be safe and highly effective. 12
After FRR a phlebography is performed again and in case of significant residual stenosis, as found in the majority if not all cases, a percutaneous transluminal angioplasty (PTA) is carried out. Again, evidence on this approach is limited, and alternative suggested approaches are either delayed phlebography or observation only. 12 Immediate post-decompression balloon angioplasty showed 100% patency and no residual symptoms after four years in a small sample of patients, while stenting of the subclavian vein seemed to have a worse long-term outcomes (64% patency and 43% residual symptoms at 3.5 years). 22 These results were possibly biased as additional stents were placed when lesions were insufficiently responsive to angioplasty alone. Therefore, we do not use stents for patients with Paget–Schrötter syndrome. When haemodynamically significant lesions persist despite thrombolysis, FRR and PTA, surgical reconstruction of the vein may be feasible; however, reports on this procedure are scarce. 12
Our experience combined with the available literature has led to the following recommendations. In our centre, all patients with a primary UEDVT of less than 14 days receive thrombolysis within 24 h after diagnosis. When an open vein is re-established we conduct a phlebography, during which the arm is moved in several provocative positions. In case of an underlying anatomical substrate for the development of effort-related thrombosis, surgical decompression after thrombolysis is required. Thus, patients eligible for surgery receive a FRR as soon as possible, but not earlier than 2 h after termination of thrombolysis. In case of significant residual stenosis after FRR and venolysis, a PTA is carried out. Subsequently, anticoagulant therapy is continued for up to six weeks from diagnosis.
Case
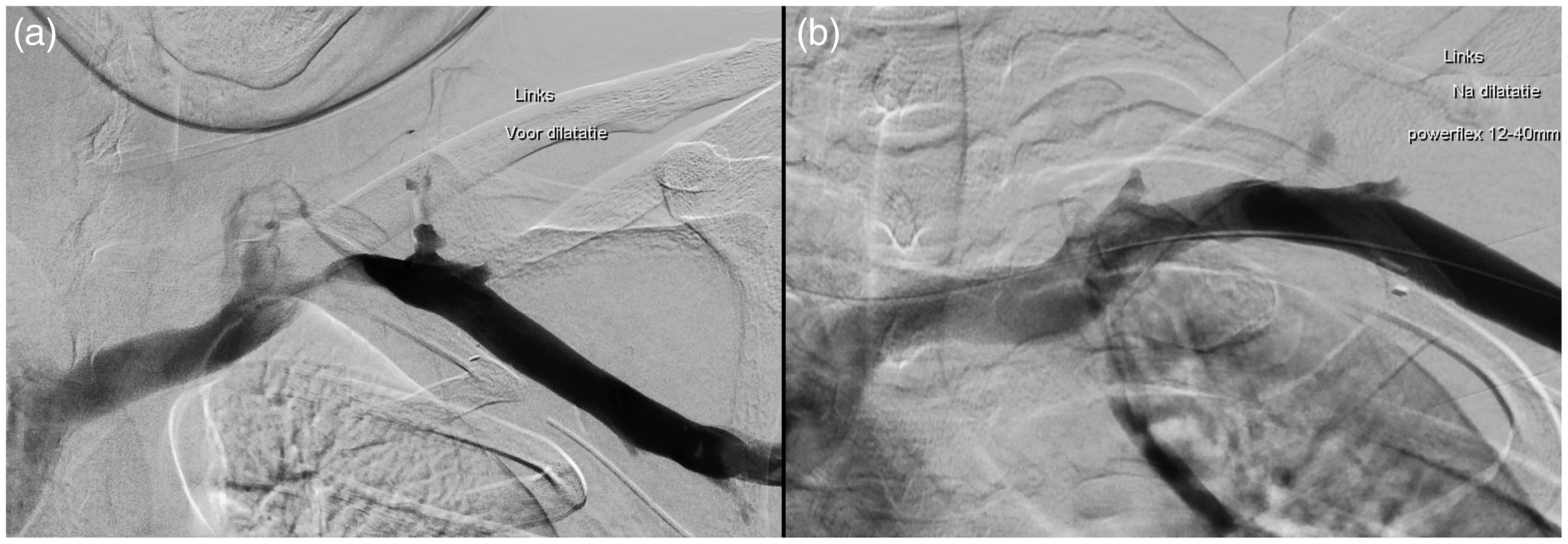
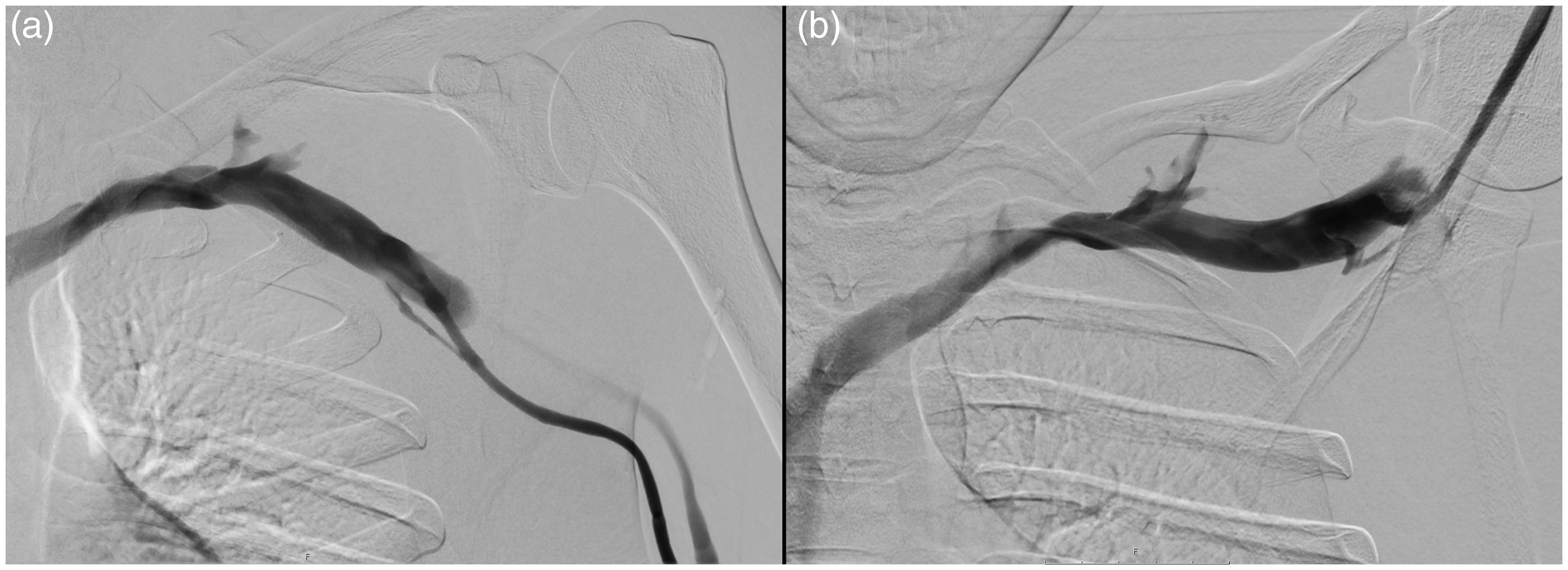
A 25-year-old, previously healthy, male was admitted to our hospital with a diffusely swollen, erythematous, and painful left arm with paraesthesia. The complaint had first occurred acutely after overhead working on a ceiling a couple of days earlier. Ultrasound revealed a thrombus in the subclavian and axillary vein of the left arm. UEDVT was confirmed by phlebography (Figure 2). Catheter-directed thrombolysis with regular interval phlebography was performed with intra-clot delivery of urokinase (Medacinase®, medac GmbH, Hamburg, Germany) for 43 h. At that time, control phlebography revealed complete lysis of the thrombus (Figure 3(a)), with total occlusion of the subclavian vein in abduction of the arm (Figure 3(b)). Evidently, the anatomy of the thoracic inlet caused compression of the vein, thereby inducing DVT. FRR was performed approximately 6 h after thrombolysis had ended. Post-surgery phlebography revealed residual stenosis of the vein (Figure 4(a)), which was subsequently dilated via PTA (Powerflex (Cordis) 10/40 mm and Powerflex (Cordis) 12/40 mm balloons) providing near-complete recanalisation (Figure 4(b)). Anticoagulation using vitamin K antagonists was started (target INR: 2.5–3.5) and continued for six weeks. At four-month follow-up control phlebography revealed vein patency in neutral position (Figure 5(a)), and only slight compression with maximal abduction of the left arm (Figure 5(b)). His symptoms had dissipated.
Phlebography before thrombolysis showing complete occlusion of the subclavian vein with extensive collaterals. (a) Phlebography after thrombolysis showing complete lysis with residual stenosis, (b) provocation by maximal abduction of the left arm results in full compression of the subclavian vein. (a) Phlebography after first rib resection, with the left arm in neutral position, showing residual stenosis, and (b) after subsequent percutaneous transluminal angioplasty, showing slight remaining stenosis. (a) Phlebography showing a patent subclavian vein in neutral position at four-month follow-up. (b) Maximal abduction induces slight compression of the vein, yet there is a significant reduction of visible collaterals compared to findings at time of diagnosis.

Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.