
Abstract
Catheter-directed thrombolysis for deep venous thrombosis is considered the basic treatment modality for intrathrombus removal. This method is preferably used in patients with iliofemoral deep venous thrombosis due to poor spontaneous recanalization in this segment, especially on the left side. The method was published almost 25 years ago and has gained ground in the treatment because of poor results from systemic thrombolysis and because of the possibility of stenting any underlying iliac obstruction during the procedure. However, the publications of catheter-directed thrombolysis reveal a great heterogeneity concerning catheter-directed thrombolysis technique and the lack of high quality evidence about monitoring as a tool to minimize the risk of bleeding and pulmonary embolism. Strict inclusion and exclusion criteria, correct composition and infusion of thrombolysis agent, imaging thrombus clearance during catheter-directed thrombolysis, ensuring flow enhancement during the bedridden situation, careful evaluation of indication for stenting based on imaging, and sufficient conversion to anticoagulation treatment following catheter-directed thrombolysis are essential. The aim of this paper is to discuss different treatment aspects of catheter-directed thrombolysis for iliofemoral thrombosis and to suggest a monitoring model for future treatment.
Introduction
Success rates and complication rates are the most important indicators for optimal care in catheter-directed thrombolysis (CDT) for iliofemoral deep venous thrombosis (DVT). Therefore, several practical, technical, and observational aspects need consideration in obtaining optimal results. Safety of the patients is of great concern with measures to reduce bleeding complications and prevent pulmonary embolism (PE). One key question is where to observe the patient during treatment: in an intensive care unit (ICU) or in a vascular ward. Achieving patency with normal valve function is the treatment goal. Thus, this article will focus on different aspects to be considered during CDT for iliofemoral DVT and suggests a monitoring model for future treatment. Terms, definitions, and recommendations are in this article based on reporting standards in newly updated Quality Improvement Guidelines for The Treatment of Lower-extremity Deep Vein Thrombosis with Use of Endovascular Thrombus Removal based from a broad platform of interventional experts published in 2014. 1 Relevant articles are added to further clarify some aspects.
Inclusion criteria, exclusion criteria, and pretreatment laboratory parameters
In- and exclusion criteria and pretreatment measurements.

APTT: activated partial thromboplastin time; DVT: deep venous thrombosis; INR: international normalized ratio.
In practice, the patient should present normal values of INR, activated partial thromboplastin time (APTT), antithrombin, hemoglobin, fibrinogen, creatinine, platelet account, and a negative pregnancy test prior to CDT. 3 The test for thrombophilia does not influence the indication for CDT; however, it has major impact on the duration of anticoagulation treatment following CDT. A positive test for lupus anticoagulants falsely increases APTT. In the Department of Vascular Surgery in Copenhagen, females on contraceptive pills continued the medication during the procedure in order to avoid severe menstrual bleeding during CDT. Unfortunately, no specific data on this management exist.3,4
Age limitations are not mentioned in the quality improvement guidelines. 1 No restrictions appear to be necessary when it comes to the age of the patient.4,5
Drugs and prevention of bleeding
Recombinant tissue plasminogen activator (rt-PA) is the most used lytic drug, but urokinase is used in some trials. Rt-PA is safe in the sense, that the clearance of this drug is more than 90% effective in the first pass via the liver, and the half-life is 3½ min, whereas urokinase has fourfold longer half-life. A short half-life is of great importance to reduce the risk of systemic thrombolysis, and in case of bleeding complications leading to discontinuation of thrombolytic infusion. Varied levels are used in the different trials from <1.0 up to 3 mg/h,3,6,7 and even a total maximum per day or for the entire treatment is used in some publications.5,7,8 According to an international advisory board, rt-PA should not exceed 2 mg/h. 9 The preferable interval is 1–2 mg/h. 1
Only few studies with CDT have compared t-PA with urokinase. Therapy with t-PA (1 mg/h) in 24 limbs compared with urokinase (120.000 U/h) in 30 limbs showed significantly shorter treatment time (24 h contra 33 h, p = 0.011) using t-PA. 10 However, another study with t-PA (only ½ mg/h) in 32 limbs and urokinase (120.000 U/h) in 38 limbs showed no difference concerning infusion time, success rate, complication rate, but t-PA was less expensive. 11
Heparin given simultaneously is mandatory; otherwise, the opened vein segment will occlude immediately due to an extremely thrombogenic surface. The infusion acts therefore optimally in combination with heparin either as unfractionated heparin or low molecular weight heparin (LMWH). Given unfractionated heparin, the APTT is monitored frequently during CDT aiming a prolongation of 1.5–2.5 times, corresponding to 50–60 s up to 90 s.3,4,7 LMWH is dosed weight adjusted according to general recommendations. The total volume of the lytic infusion (rt-PA and heparin or LMWH diluted in 0.9% saline) varies from 50 to 120 ml/h.4,7 It is important to check the access site to ensure that the lytic fluid actually is injected intravenously without leakage to the bandage.
Treatment is preferably monitored during CDT 1–2 times every 24 h with APTT, fibrinogen, fibrin
Fibrinogen is often elevated in the acute phase, and a minor decrease in the fibrinogen level generally occurs during CDT. However, a marked decrease in fibrinogen level might indicate systemic fibrinolysis and a risk of bleeding and should lead to careful examination of the patient.
Flow facilitation
Intermittent pneumatic compression (IPC) is commonly used as prophylaxis for DVT and in the treatment of chronic venous edema and lymphedema, but infrequently used in connection with CDT. In a comprehensive review on CDT from 1998, only three of 15 publications have reported use of IPC. 12 A small Japanese prospective study from 2005 compared a group of 10 patients treated with CDT and IPC with 14 patients treated with CDT alone and included mainly patients with iliofemoral involvement. 13 In the IPC group a temporary IVC filter was inserted. The IPC device consisted of a foot cuff and a calf cuff inflated to 80 mmHg in a sequential way maintained for 6 s with 1 min to next inflation during the entire bedridden position, thus more accurately called sequential intermittent compression. The results demonstrated better initial thrombolysis with IPC (p = 0.0037) and less occurrence of postthrombotic syndrome (PTS) in the IPC group (p = 0.01) after median follow-up period of 22 months for the group without IPC and 14 months for the other group. A logic rationale seems to be a benefit of a flow-enhancing procedure to keep the lysed vein segments open in interaction with heparin imitating the calf pump function. This assumption may support a benefit of a great infusion volume rather than a minor volume. No increased risk of symptomatic PE was demonstrated based on no trapped thrombus in the filters. Even though IPC is not mentioned in the quality improvement guidelines, the flow-enhancing device might be of use during CDT. 4
Thrombus clearance and D- dimer
Avoiding PE
Occurrence of PE during CDT can, of course, finishes the treatment prematurely, but is in fact very seldom. In two recently published large-scale studies with 90 and101 patients, respectively, undergoing CDT, no procedure-related PE occurred. In these studies, only eight patients had IVC filters inserted.4,7 Same findings were seen in a publication with 69 patients managed with CDT and additional mechanical procedures without filter. 15 No symptomatic PE occurred in 87 patients treated with ultrasound (US)-assisted CDT without filter. 5 The reason for this negligible risk is the use of AC before, during, and after the procedure. Another observation is that the iliofemoral DVT most often is located on the left side due to an underlying May–Thurner lesion. However, one quite recently published article showed an incidence of 4.9% with symptomatic PE during CDT in 266 patients without IVC filter. They concluded that the risk of PE was markedly increased in patients with previous silent PE and heart disease, found in almost 1/3 with heart disease and 1/2 with previous silent PE. IVC filters are recommended in such a category of patients. 16 Usually patients with any restricted cardiopulmonary function are not candidates for CDT. Routinely insertion of a retrievable IVC filter is not recommended but can be justified in patients with a flagellating thrombus configuration. 1
Imaging for visualization of patency
Imaging of the thrombus removal is another helpful principle in achieving the best results. Daily venograms perfectly illustrate the progress of the treatment. Furthermore, in some cases it is necessary to replace or move the lysis catheter in order to maximize the instillation of the lytic fluid directly into the remaining thrombus formation. Multiple venograms at the end of the procedure are mandatory to visualize the flow in the iliac lumen. Uncovered obstructions at this level have to be carefully evaluated in order to make decision for a stenting procedure. Intravascular ultrasound (IVUS) for this part of the treatment is only described in one article, in which visualization of any residual thrombus resulted in further lysis. 17
Observation unit: ICU or vascular ward?
The major concern for patients treated with thrombolysis is the risk of bleeding. In many countries, the patients have to stay in an ICU in order to give the patients the most optimal control during the CDT procedure. In Copenhagen, the patients from the beginning in 1999 have been admitted in the vascular ward with educated and trained nurses checking up on the patients at least 1–2 times every 8 h. Checklists for the patients at bed rest should be followed, including pulse rate, blood pressure, inspection for bleeding, and to ensure a correct placement of the catheter at the access site. Arterial punctures and intramuscular injections are not allowed prior to or during thrombolysis. Pericatheter oozing, sometimes epistaxis and hematuria can occur despite maximal precautions, and is described as minor bleeding. Major bleeding is defined as intracranial bleeding, large hematoma, need for blood transfusion, evacuation by surgery, or need to discontinue the treatment.1,4
The recent publication on the aforementioned improvement guidelines does not take any position concerning ICU contra ward, but underline all the monitoring precautions mentioned above. 1 However, it is a fact, that the stay in ICU is much more expensive compared to a stay in an ordinary ward. This fact has over the years accentuated the need for methods using less amount of lytic infusion in a shorter period in an attempt to reduce the risk for bleeding.
Conversion to AC
Shift from cessation of the lytic infusion to anticoagulation treatment poses a minimal risk of bleeding, but a major risk of rethrombosis. Weight-adjusted LMWH is given immediately after end of the last infusion of thrombolytic agent and is considered safer than unfractionated heparin, though controlled with APTT. Some centers recommend bridging with LMWH in therapeutic doses for at least 14 days to ensure a safe overlap, while initiating treatment with vitamin K antagonists.3,4 The none vitamin K oral anticoagulants have not found their place in this field. The duration of AC treatment varies from months to years and depends on the causes of the DVT, including massive thrombophilia. However, evidence is weak. Lifelong AC is reported in patients with cava atresia and CDT. 18
Control at discharge
The patients are mobilized 2 h after removal of the CDT catheter. US before discharge is mandatory to verify the patency of the treated segments, including the adjoining veins. In case of reocclusion, retreatment is mandatory if possible. It is absolutely necessary to inform the patient about this possibility before CDT. The patients are discharged wearing short elastic compression stockings (ECS). However, the benefit of ECS after CDT is not tested in any study. A consultation about the continued AC is important. Many papers have included US controls after six weeks, three, six, and 12 months and yearly hereafter. Any deviation from the recovery status should be promptly reported and assessed. The publications give no information of a benefit for more aggressive posttreatment controls. In our experience from Copenhagen, the failures with either stenosis, occlusion, or reflux occur gradually over the years. 4 The patients are encouraged to maintain a relatively high level of physical activity.
Discussion
The impact of institutional volume increases in a six-year period (2005–2010) in the United States has recently been published and compared centers with <6 CDT procedures a year contra centers with more procedures. 19 In-hospital mortality rate was significantly lower in high-volume centers (0.6% versus 1.5%, p = 0.04), and a trend toward lower rate of intracranial hemorrhage without difference concerning blood transfusions, PE, and gastrointestinal bleeding was observed. A direct implication of these findings indicates a professional decision to concentrate this category of patients in big-scale institutions. It is worth mentioning, that based on the same nationwide sample of 90,618 patients with DVT, of which 3649 patients were offered CDT, no difference in mortality was encountered between the CDT group and the AC group. 20
Death occurred as well in the national multicenter registry from US 1999. 21 Of 473 patients only two patients died (0.4%): One from intracranial hemorrhage, and one from PE. PE was seen in 1%. Ten years later no death or PE occurred in the large-scale studies with 90 + 101 patients, respectively, from the Scandinavian groups.4,7 A suggested threshold suggests < 1% occurrence of intracranial bleeding and < 2% occurrence for symptomatic PE. 1 These goals will only be achieved following a strict monitoring management to keep the mortality rate as close to zero as possible.
Nonfatal major bleeding occurred in 11% in the US registry study and later reported in 1.5% of the cases.21,22 A threshold is suggested to be < 7%. 1 Minor bleeding rates, which all are without any influence of the outcome, vary from 3 to 26%.7,22 No threshold value is mentioned of this complication, which should be as minimal as possible. 1
Patients with more than 50% residual thrombus in the treated vein segment had significantly higher CEAP grades and more severe PTS judged by the Villalta score. The incidence of PTS was lowest in patients with complete thrombus removal, emphasizing the importance of clearing as much thrombus mass as possible. 23 Residual thrombus material after CDT was also a predictor of increased rate of PTS shown in the CaVenT study. Both reflux and lack of patency at six months were independent predictors for development of PTS after 24 months. 24 A recent paper including 93 patients concluded that lysis of less than 50% was strongly predictable for DVT recurrence (HR 5,83, p < 0.001) and PTS. 25 These observations might—among other factors—strengthen the use of D-dimer control and IPC to increase the efficacy of CDT.
The article is not intended to be a systematic review, which gives certain limitations. According to existing guidelines for optimal care during CDT we have emphasized some of the most important elements in the treatment.
Future research
One of the main challenges is the problem concerning the amount of remaining residual thrombus. Rapid and efficient removal of blood clots reduces the risk of PTS. The question is what amount of residual thrombus can be accepted? It definitely depends on the age of the thrombus, the duration of treatment, and the concentration of rt-PA. It is the authors’ belief that studying the D-dimer fluctuations during the therapy and particularly at the end of thrombolysis in conjunction with diagnostic imaging might help to plan when to end the lytic infusion. IVUS can be helpful too. Another issue is about the use of IPC. It is the authors’ belief that flow stimulation during CDT is important as well as efficient anticoagulant treatment and follow up after discharge. Conclusively, the area of CDT needs more studies with protocols on subelements during treatment.
Conclusion
The summarized factors in the table are suggestions to monitor CDT, while not all are scientifically proven.
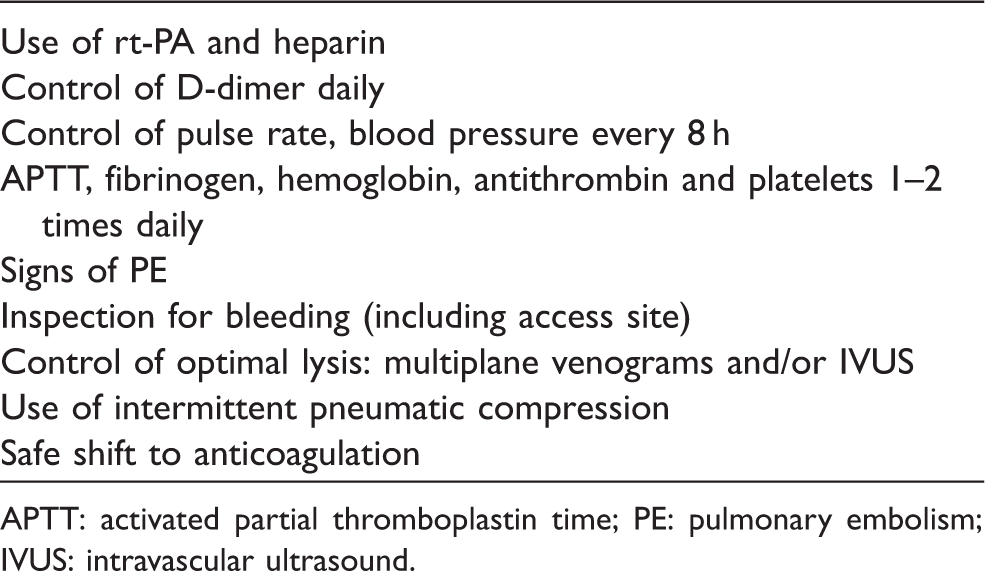
APTT: activated partial thromboplastin time; PE: pulmonary embolism; IVUS: intravascular ultrasound.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.