
Abstract
Venous leg ulcer (VLU) is one of the most common lower extremity ulcerated wound, and is a significant healthcare problem with implications that affect social, economic, and the well-being of a patient. VLU can have debilitating related problems which require weekly medical care and may take months to years to heal. The pathophysiology of VLU is complex, and healing is delayed in many patients due to a persistent inflammatory condition. Patient genetic and environmental factors predispose individuals to chronic venous diseases including VLU. Changes in shear stress affecting the glycocalyx are likely initiating events, leading to activation of adhesion molecules on endothelial cells, and leukocyte activation with attachment and migration into vein wall, microcirculation, and in the interstitial space. Multiple chemokines, cytokines, growth factors, proteases and matrix metalloproteinases are produced. The pathology of VLU involves an imbalance of inflammation, inflammatory modulators, oxidative stress, and proteinase activity. Understanding the cellular and biochemical events that lead to the progression of VLU is critical. With further understanding of inflammatory pathways and potential mechanisms, certain biomarkers could be revealed and studied as both involvement in the pathophysiology of VLU but also as therapeutic targets for VLU healing.
Keywords
Introduction
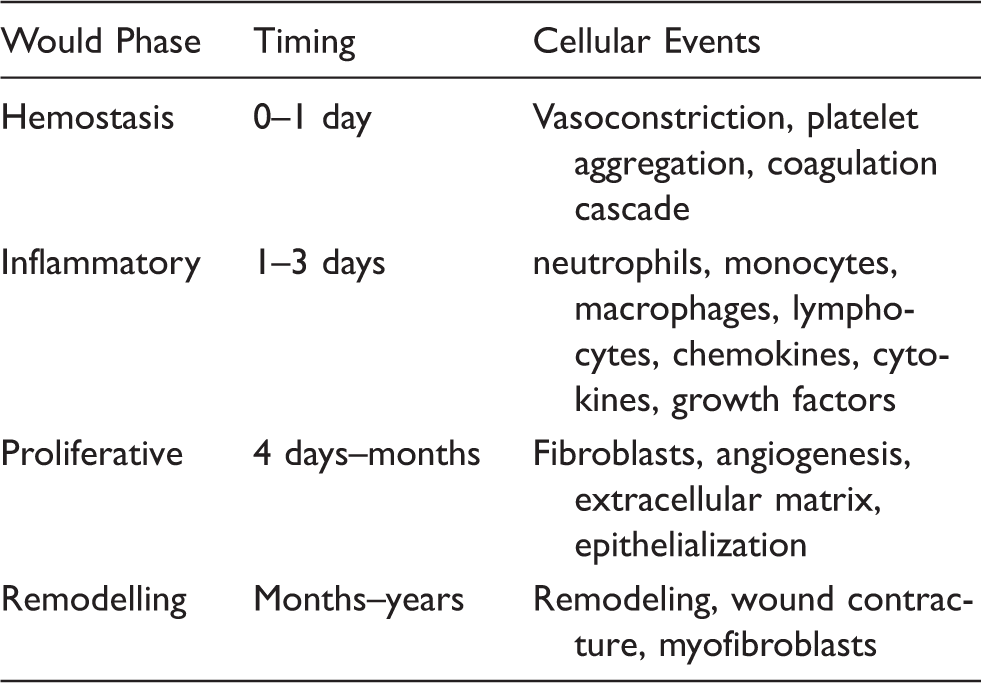
Chronic venous disease (CVD) is a spectrum that clinically includes patients presenting with varicose veins, edema, skin changes and venous leg ulceration (VLU). Chronic venous insufficiency (CVI) is associated with increased ambulatory venous pressure and is usually seen with advanced forms of CVD (edema, skin changes, VLU). CVI affects 10–35% of US adults. Primary (chronic venous disease resulting in venous hypertension from varicose veins with idiopathic valvular insufficiency) CVD is more common than secondary (chronic venous disease resulting in venous hypertension usually from venous thrombosis and valvular insufficiency and/or obstruction) with the latter responsible for about 18% to 28% of limbs with CVD. In the Western population skin changes and ulceration affects 2–5% of Western population. Importantly, VLU wounds occur in up to 5% of the population over 65 years of age.1,2 Wound healing is a complex process that involves hemostasis with platelet function and coagulation cascade within the first day, this is followed by an inflammatory phase involving neutrophils and macrophages that last several days, a proliferative phase which begins after 3 to 4 days and progresses for months involving growth factors, angiogenesis, fibroblast activity with collagen and extracellular matrix deposition, keratinocytes for epithelialization, and finally a remodeling phase, which begins at several months from the inciting event and progresses for months to years, leading to wound contracture (Table 1).3,4 A fundamental principle in chronic VLU is that an inflammatory condition exist that persists leading to disease presentation and progression. The important steps in inflammation involves leukocytes, particular macrophages and monocytes as well as T-lymphocytes, changes in shear stress on the endothelium and glycocalyx alterations, inflammatory modulators and chemokines, cytokine expression, growth factors, and matrix metalloproteinase activity. There are genetic and environmental conditions that predispose individuals to CVD likely leading to altered shear stress on the endothelial cells, causing endothelial cells to release vasoactive agents, express E-selectin, inflammatory molecules, chemokines, and prothrombotic precursors.4–6 Mechanical forces, low shear stress, and endothelial-smooth muscle stretch are sensed by the endothelial cells via intercellular adhesion molecule-1 (ICAM-1, CD54) and the mechano-sensitive transient receptor potential vanilloid channels (TRPVs) that are present in the endothelium.2,7 It is well known that patient with CVD have increased expression of ICAM-1, which is expressed on endothelial cells, and activate the recruitment of leukocytes and initiate endothelial transmigration, setting up an inflammatory cascade. Initiating events likely involve altered shear stress and mechanical stress forces on the endothelium and its glycocalyx (a glycosaminoglycan on the surface of endothelial cells), with perturbations on nitric oxide production, vasoactive substance release, expression of monocyte chemoattractant protein-1 (MCP-1) and vascular cell adhesion molecule-1 (VCAM-1, CD106), expression of L-selectins and E-selectins, ICAM-1, with recruitment of leukocytes leading to leukocyte transmigration into the vein wall and interstitial tissue space, setting up an inflammatory cascade and production of several cytokines (transforming growth factor-β1 (TGF-β1), tumor necrosis factor-α (TNF-α), interferon-γ (IFN-γ), interleukin-1 IL-1)) and increased expression of matrix metalloproteinases (MMPs).7,8 As a result of persistent inflammation the venous wall and valves are affected and venous hypertension ensues, propagating the disturbances on the endothelium, microcirculation, and inflammatory response (Figure 1).
Schematic flow diagram of the pathophysiologic events in chronic venous disease. Genetic and environmental conditions predispose individuals to venous disease. Early changes likely involve low shear stress on the endothelium with glyococalyx disruption, and activation of endothelium and leukocytes by a variety of adhesions molecules (ICAM-1, VCAM-1, TRPV-1) and leukocyte chemoattractants (chemokines, MCP-1, MIP-1α,β). Macrophages (MP), mast cells (MC), and t-lymphocytes (TL), infiltrate the venous wall and the interstitial tissue and around the postcapillary venules. Inflammation persist, matrix metalloproteinases are expressed and begin tissue degradation of collagen, elastin, extracellular proteins, and glycosaminoglycans, leading to venous wall and valvular injury producing venous hypertension. This cycle perpetuates as the inflammatory response continue leading to eventual skin changes and venous leg ulcer. Phases of wound healing. There are four phases to wound healing. It begins with hemostasis involving vasoconstriction and platelet activation and aggregation, followed by an inflammatory phase with neutrophils acting within the first 24 hours and then replaced by macrophages with lymphocytes having a role later in the phase. There are many chemokines, cytokines, growth factors, and proteases that are produced during the inflammatory phase. The proliferative phase is begins the structural repair of the tissue with fibroblasts producing collagen, elastin, and extracellular matrix proteins. Angiogenesis and epithelialization are characteristic of this phase and occur within the first week and continue for months. The final phase involves remodeling which involves myofibroblasts and is the wound continues to gain tensile strength over months to years.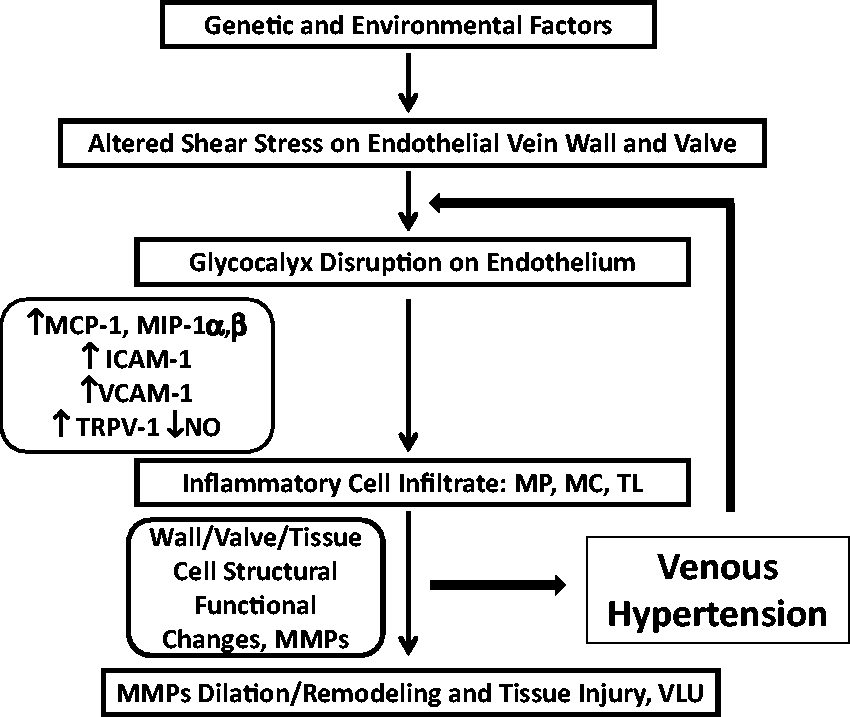
VLU have several areas of activated pathways due to the persistent inflammatory response that include oxidative stress with iron overload, cytokine and chemokine expression, alteration in collagen turnover, and overexpression of MMPs leading to tissues destruction of the dermis with eventual skin changes and ulcer formation. This review will cover some important aspects of general wound healing, and then discuss the important aspect of the pathophysiology of wound healing in VLU, differentiate VLU that heal versus VLU that are classified as non-healing with respect to the biochemical properties of the wound.
Wound Healing
Wound healing has four phases that overlap as one phase regresses and the next phase initiates (Table 1). Following the development of a wound, an immediate event occurs called the hemostasis phase. This phase begins with vasoconstriction by released vasoactive substances (thromboxane A2, serotonin, adrenalin). Platelets are rapidly recruited to the injured area and activation by the injured blood vessel exposing collagen leads to ADP and glycoprotein adhesion molecules (fibrinogen, fibronectin, vitronectin, thrombospondin, and von Willebrand’s factor) release and aggregation. Prothrombin is activated by platelets and forms thrombin, which catalyzes the formation of fibrin from fibrinogen making a thrombus and acting as a provisional matrix. An important protein is fibronectin which contains several integrin receptors and will be important in stimulating the migration and adhesion of fibroblasts, keratinocytes, and endothelial cells. Platelets also have integrin receptors and add further aggregation to thrombus and secrete growth factors (platelet derived growth factor (PDGF), transforming growth factor-α (TGF-α), TGF-β, basic fibroblast growth factor (bFGF), insulin-like growth factor-1 (IGF-1) and vascular endothelial growth factor (VEGF)), which are necessary compounds to recruit inflammatory cells. The second phase begins at 1 to 3 days of wounding involves the inflammatory response which initiates the recruitment of neutrophils and monocytes/macrophages. The cells release a host of inflammatory chemokines and cytokines, as well as growth factors. Neutrophils are recruited by several chemokines including thrombin, leukotrienes, PDGF, TGF-β, and bacteria as well as complement, initiate the defensive mechanisms to infection. Further cytokines are released and after 24 hours neutrophils undergo apoptosis with the insurgence of monocyte/macrophages leading to further inflammation and phagocytosis. Macrophages produce cytokines, MMPs, and growth factors (IL-1, IL-6, IL-8, and TNF-α, TGF-β, PDGF, TGF-α, bFGF, heparin-binding epidermal growth factor-like growth factor (HB-EGF), IL-1, IL-6, and a variety of MMPs 1,2,3,9,10) needed to both clear cellular debris and initiate the process of recruiting fibroblasts for collagen and matrix deposition. Further initiation of angiogenesis is initiated by the direction of VEGF, epidermal growth factor (EGF) and PDGF. Lymphocytes also participate in the later stages of inflammation. The proliferative phase follows and is dominated by fibroblast function with collagen deposition and further extracellular matrix proteins that takes place within the first week and progresses for months. The provisional fibrin matrix is now replaced with collagen, elastin, proteoglycans, glycosaminoglycans, and noncollagenous glycoproteins. Fibroblasts are under the regulation of a number of growth factors (PDGF, epidermal growth factor (EGF), IGF-1, and TGF-β). Collagen deposition (type I and III) increases up to the third week and then begins to decline. Epithelialization comes from the wound edge and skin appendages (sweat glands, hair follicles), and requires the detachment of keratinocytes to migrate, proliferate and cover the collagen rich matrix. This is regulated by growth factors (TGF-α, EGF, keratinocyte growth factor (KGF), and TGF-β) as well as MMP-2, MMP-9 which are important in degrading type IV collagen for cellular detachment and MMP-1, MMP-3, and MMP-10 promoting new epithelial cells to migrate along fibronectin and the extracellular matrix components. Throughout the process of proliferation phase, angiogenesis is taking place to restore new blood vessels in the injured area now enveloped by connective tissues and extracellular matrix, and under the regulation of angiogenic factors (VEGF, PDGF, MMPs), which brings in endothelial cells forming new capillaries for oxygen and carbon dioxide transport and nutrients. The final phase involves remodeling and begins within months and may continue for several years. This phase involves wound contracture and is performed by myofibroblasts differentiated from fibroblast. The characteristics of this phase is the progressive increase in wound tensile strength, increase of total collagen especially type I, increased cross-linking of collagen, where the strength of the tissue reaches 80% of that of unwounded tissue.3,9,10
Pathophysiology in Venous Leg Ulcer Wound Healing
Chronic VLU are characterized by perpetual inflammatory phase, with provisional matrix but inability to continue to the proliferative and remodeling phases of wound healing. The appearance of wound ulcer that have an inflammatory state is characterized by open wounds which have drainage, have necrotic tissue overlying the wound bed, have pain as well as induration around the surrounding irregular borders (Figure 2). The characteristics leading to VLU are multifactorial, and the biologic environment is a complex interplay of imbalances in a number of biomolecules and processes which include: inflammatory cells, chemokines and cytokines, inflammatory modulators, extracellular matrix proteins, collagen turnover, oxidative stress, and protease activity especially MMP2- and MMP-9.
11
It is important to discuss cellular and biochemical properties of the wound which differentiate VLU that heal versus VLU that are non-healing, that could provide insight into the mechanisms and potential treatments of VLU (Table 2).
Large chronic venous leg ulcer. There venous leg ulcer is characterized by significant inflammation surrounding the ulcer, irregular ulcer border, and unhealthy wound bed containing necrotic tissue and poor granulating matrix. There is excess drainage from the venous leg ulcer termed wound fluid which is rich in cytokines and proteinases that exacerbate a condition of inflammation. Important pathophysiologic events in venous leg ulcers. There are a number of cellular and biochemical events involved in the pathophysiology of venous leg ulcer. These events have a pathology that is associated with the ulcer, and how the wound environment changes the condition of the cellular components or biomolecules can predict if healing of the venous leg ulcer will occur.

Inflammatory Cells
Inflammatory cells have been demonstrated in patient with CVD. In a study evaluating the number of white blood cells in tissue biopsies of patients with CVI, it was determined that the number of leukocytes was highest in the dermis of patients with a history of ulceration followed by tissues with lipodermatosclerosis, and lowest in CVI patients with no evidence of skin changes. In a careful histological study using immunohistochemistry in patients with severe lipodermatosclerotic skin changes, the predominant cell types were found to be T-lymphocytes and macrophages. 12 In another study the type of leukocyte was defined in a morphometric analysis. Biopsies from patients with severe lipodermatosclerosis and healed ulcers contained significant numbers of mast cells around arterioles and postcapillary venules, and in active VLU macrophages were predominantly located in the postcapillary venules.
Chemokines and Cytokines and Growth Factors
Chemokines are a family of cytokines, or signaling proteins secreted by leukocytes and other cells. Chemokines, or chemotactic cytokines, have the ability to produce chemotaxis in nearby responsive cells. The classification and nomenclature of chemokine families are divided into four groups depending on the spacing of their first two cysteine residues, and named as: α-chemokine (CXC), β-chemokine (CC), γ-chemokine (C or XC) and δ-chemokine (CX3C). All of these proteins exert their biological effects by interacting with G protein-linked transmembrane receptors called chemokine receptors that are selectively found on the surfaces of their target cells. The major role of chemokines is to act as a chemoattractant to guide the migration of leukocytes and recruiting monocytes during cytokine activation and inflammation. 8 In a very interesting study analyzing cytokine levels and venous ulcer healing in 29 patients who underwent ulcer edge biopsy before and after 4 weeks of four layer compression bandaging. The study determined that untreated ulcers typically display high levels of chemokines (IL-8), pro-inflammatory cytokines including several interleukins (IL-1, IL-6, IL-12), TNF-α, and interferon-γ (IFN-γ), and granulocyte-macrophage colony stimulating factors. After 4 weeks of compression therapy, the levels of pro-inflammatory cytokines decreased significantly and the wounds began to heal. After compression, levels of TGF-β1 increased significantly as the ulcers improved. When specific cytokine levels were related to the percentage of healing, it was found that those with higher levels of pro-inflammatory cytokines including IL-1 and IFN-γ healed significantly better than those with lower levels of these cytokines prior to compression. Treatment with compression therapy resulted in healing that was coupled with reduced pro-inflammatory cytokine levels and higher levels of the anti-inflammatory cytokine interleukin-1 receptor antagonist (IL-1 Ra). 13 The role of TGF-β1 in VLU healing was investigated in a study of 80 patients treated with multilayer compression bandaging. In the wound fluid and serum, cytokines and factors reflecting the processes of inflammation (IL-1, TNF-α), proteolysis (proMMP-2 and proMMP-9), angiogenesis (bFGF, VEGF), and matrix deposition/proliferation/fibrosis (TGF-β1) were measured. Interestingly, ulcer healing at 5 weeks only correlated significantly with increased concentrations of TGF-β1 in the VLU wound fluid. 14 In a study of 40 patients with healing versus non-healing VLU of greater than 8 weeks duration, patients had tissue biopsy at the VLU edge and wound fluid at initial visit. Evaluation of VLU healing was assessed after 8 weeks. In healing VLU there was significantly higher (P < 0.001) levels of PDGF-AA in the perivascular region, and in the wound fluid healing VLU had significantly increased levels of PDGF-AA and decreased ratio of MMP-2:TIMP-2 (tissue inhibitor of metalloproteinases) (P = 0.0001). 15
Inflammatory Modulators
Regulation of the inflammatory response is complex and has many biomolecules that are involved. In a landmark study of proteomics and degradomics, VLU patients with healing wounds (n = 9) and non-healing wound (n = 19) were evaluated. The VLU wound fluid was collected and proteins separated by sodium dodecyl sulfate polyacrylamide gel electrophoresis (SDS-PAGE) and analyzed by liquid chromatography and mass spectroscopy. Differential detection Identified 149 proteins and 23 were unique to healing VLU and 26 unique to non-healing VLU. Three proteins were analyzed for proof of concept and identified significantly increased levels in non-healing VLU of lactotransferrin, S100A9, and annexin A1. The importance of these proteins is their function: Lactotransferrin has strong antimicrobial activity is thought to be mediated by diverse mechanisms, including its iron scavenging property, its proteolytic activity, and its inhibition of bacterial biofilm formation. Furthermore, several studies emphasize lactotransferrin role in regulating cellular signaling pathways, which control inflammation, cytokine expression, and cell cycle arrest. Annexin A1 is a calcium dependent phospholipid binding protein can affect many pathways of the inflammatory response (e.g. leukocytes extravasation and inflammatory cytokine secretion), and suppresses the inflammatory reaction involved with nitric oxide synthase and cyclo-oxygenase pathways. S100A9 is a calcium binding and modulating protein important in cell growth and differentiation, and in wound healing.11,16 Further work will be required to determine the actual function of these inflammatory modulators have in VLU pathology, and if these are markers of chronic inflammatory response or actual targets for therapeutic intervention.
Collagen Turnover
Collagen turnover and remodeling is an important function of healing VLU. In a proteomics study evaluating VLU wound fluid collagen substrate types α-I and III chains were only demonstrated in healing VLU. 16 In a study evaluating VLU biopsies in healed patients (n = 12) and not healed patients (n = 15), as well as controls (n = 15), after applying compression bandaging for 12 months, the degradation products of collagen and collagen turnover were determined. Healed VLU had significantly (P < 0.001) elevated levels of degraded collagen and type III collagen (P = 0.005, as measured by collagen III N-terminal propeptide, indicating increase collagen deposition and turnover), and elevated levels of MMP-1 (P < 0.001, MMP-1 is important in tissue remodeling during healing). 17
Oxidative stress
Iron overload has been found in the serum and dermis of limbs of patients with venous ulcer compared with control subjects. A concomitant elevation in MMP-9 activity was also present in patients with VLU. The importance of iron overload in venous ulcer tissue is that it can cause oxidative stress and production of free radicals or reactive oxygen species (superoxide, nitric oxide, hydrogen peroxide, peroxynitrite). It is suggested that elevated iron deposits in the limbs is released into the serum with activation of MMPs and reactive oxygen species, and impaired ulcer healing. 18 Other investigators have also found increased ferritin and overall oxidative stress as measured by 8-isoprostane (measure of lipid peroxidation) and total antioxidant status in VLU wound fluid. Importantly the levels of ferritin and oxidative stress as measured by total antioxidant status (a measure of oxidative stress) were significantly lower (P < 0.05) in patients with healing VLU versus those that had non-healing VLU. 19 These studies support the concept that VLU have an environment of oxidative stress and oxidative-induced cellular damage that may result from the presence of higher levels of iron, and in particular increase oxidative stress in non-healing VLU.
Matrix Metalloproteinase Activity
A variety of MMPs have been identified in VLU both by biopsy and in the VLU wound fluid. Because MMPs are important in the pathogenesis of VLU, it is important to examine data that has evaluated MMPs in the VLU wound fluid and in biopsies. The collagenase activity of venous ulcer wound fluid was found to be 116-fold higher than in normal acute wound fluid. Importantly, the collagenase activity decreases in VLU demonstrating healing at 2 weeks. 20 In another study evaluating MMPs in VLU wound fluid, MPP-1 and MMP-8, as well as TIMP-1 and TIMP-2 (tissue inhibitors of MMPs) were present. Collagenase was 2–3 fold higher in VLU wound fluid compared to acute wound fluid. Of interest there was a 10-fold increase of gelatinase (MMP-2 and MMP-9) levels and activity in VLU wound fluid.21,22 These studies indicate that there is significant proteolytic activity in VLU, indicating a chronic state of inflammation and tissue destruction of collagen and extracellular matrix proteins leading to impaired wound healing. However, there are also responses to treatment with changes in MMP profiles within the wounds that support VLU healing. In a study of patients with VLU, tissue biopsies obtained at initial visit and after four weeks of compression therapy were evaluated for MMPs. At four weeks, significant decrease (P < 0.05) in both mRNA and protein were seen for MMP-3 (stromelysin-1) and MMP-9 (gelatinase-B). In addition, in those patients that had greater than 40 % healing of the VLU versus those that had less than 40% healing, significant decreases (P < 0.05) in MMP-1, MMP-2 and MMP-3 were identified. 23 In another interesting study VLU wound fluid was compared to acute wound fluid and assessed for MMP-9 and neutrophil gelatinase-associated lipocalin (NGAL). NGAL binds covalently to MMP-9 inhibiting deactivation of MMP-9 and increasing its activity. As expected MMP-9 and NGAL were significantly elevated in VLU wound fluid compared to controls. Interestingly, the levels of MMP-9 and NGAL in VLU wound fluid decreased at 4 and 8 weeks in VLU that healed, and remained elevated in VLU that did not heal. 24
Conclusions
VLU have a complex pathophysiology, and have reduced wound healing due to a persistent inflammatory state. There are many inflammatory pathways that are activated within the VLU environment. Genetic and environmental factors predispose patients to CVD and changes on the endothelial surface and protective glycocalyx are likely early initiating events. The inflammatory cells are activated by activation of endothelial cells and adhesion molecules, which results in the expression of many cytokines, inflammatory modulators, MMPs, and oxidative stressors. There is clinical and scientific evidence in the literature that modulation of cytokines by compression leads to VLU healing. In addition, favorable changes in the proteolytic, collagen turnover, and oxidative environment of the VLU, leads to increased healing. This would suggest that these pathways, when dysregulated and unopposed, are important in development of VLU, and that further research in the inflammatory and proteolytic mechanism of VLU should be pursued to determine appropriate biomolecules that are involved in VLU development, but also as potential markers for prognosis and targeted therapy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.