
Abstract
I ntroduction
This is a single-center clinical study for the evaluation of safety, efficacy, and performance of endovenous cyanoacrylate (Sapheon Venaseal Closure System, now Medtronic Medical) for the treatment of great saphenous vein (GSV) reflux.
M ethods
Primary outcome measures included the GSV obliteration, with clinical recurrence on follow up as detected by serial clinical and duplex examinations of patients at 1 week, 1 month, 6 months, and 1 year. Venous clinical severity score (VCSS), Aberdeen varicose vein questionnaire (AVVQ), Short Form Health Survey 36 Item (SF-36) questionnaires were used at clinical follow up. Diameter of the GSV, treatment length of the GSV, and pretreatment clinical severity of the varicose vein were analyzed to predict recanalization using Cox regression analysis.
R esults
Fifty-seven legs in 29 patients with primary varicose veins were included. One week follow-up duplex showed successful obliteration of the GSV in all except one of the legs. Two legs had minimal extension of thrombus to deep vein. None of the patients had deep venous thrombosis. All the patients were discharged the same day of operation. Median time to return to work was 1 day (range 1–16 days). Our VCSS, AVVQ, and the SF-36 physical and mental scores changed from a mean of 6.91, 23.66, 44.24, 54.26 at baseline to 2.43, 6.10, 43.85, 52.50 at 1 month post operation, respectively. Kaplan–Meier analysis showed that the GSV closure rates were 98.2%, 94.3%, 89.7%, and 78.5% at post-op 1 week, 1 month, 6 months, and 1 year, respectively. With median follow-up period of 9 months (range 1–13 months), no clinical recurrence of varicosity was observed. Mean GSV diameter ≥8 mm was a significant predictor for recanalization (hazard ratio 6.92, 95%CI 1.34–35.67, p = 0.021).
C onclusion
This study showed that the use of endovenous cyanoacrylate in the treatment of the GSV reflux was safe. All patients had symptomatic improvement as shown by the VCSS and AVVQ.
Keywords
Introduction
Whilst endovenous therapy is minimally invasive without the necessity of open surgical wounds in the groin, the multiple perivenous needle injection for tumescence anesthesia may result in periprocedural pain and ecchymosis.1,2 Recently, there are nonthermal endovenous treatment modalities which do not require tumescence anesthesia, namely mechanochemical ablation (Clarivein) and cyanoacrylate glue. Cyanoacrylate glue is a liquid adhesive that has been used in humans in the treatment of arteriovenous malformations and peptic varicosities.3–5 The mechanism of the cyanoacrylate glue is simple: plasma and blood stimulates its polymerization and leads to closure of the target veins. 6 The use of this commercially available endovenous cyanoacylate glue (Venaseal™ Sapheon Closure System, Sapheon Inc. (Santa Rosa, California, USA; now Medtronic, Gorway, Ireland) for trunkal ablation of great saphenous reflux is a new modality for treating the varicose veins. The recently published VeClose Study showed that in 108 legs treated with VenaSeal Sapheon Closure System (Sapheon, Inc, Morrisville, NC), the 3-month closure rates was 99%, and that this treatment modality was proven to be effective. 7
The aim of this paper is to report our single-center, prospective study for the evaluation of safety, efficacy, and performance of endovenous cyanoacrylate (sapheon venaseal closure system) for the treatment of primary great saphenous reflux.
Patients and methods
Study population
These were nonrandomized consecutive patients with varicose veins (mainly bilateral) who presented to our tertiary vascular center. Inclusion criteria included fully consenting adult patients aged more than 18 years, who had primary varicose veins with pre-operative duplex ultrasound proven incompetence of saphenofemoral junction (SFJ) and/or reflux in the great saphenous vein (GSV).
All the pre-procedural duplex ultrasound scans were performed by certified vascular sonographers using the Sequoia 512 (Siemens, CA, USA) or Philips iU22 (Philips Healthcare Solutions, WA, USA) devices in our vascular laboratory. Saphenous vein reflux was defined by the presence of retrograde flow detected in the duplex ultrasound scan over the SFJ, with the patient examined in the standing position (more than or equal to half a second). 8 The diameter of GSV was measured, while patient supine, at three levels (proximal thigh near SFJ, mid thigh, and distal thigh above knee). Mean diameter of GSV was defined as the average of the above three measurements. All our patients gave written consent.
This study had local Institutional Review Board approval (reference UW 15-212). There was no deliberate selection bias by the authors to only perform the operation with favorable lesions, and all patients followed a fixed protocol of follow up.
Study procedure
All the endovenous procedures were performed in our Minimally Invasive Surgical Center under local anesthesia with the use of standard sterile technique. Since this was an IRB-approved project with a very new treatment modality in our region, we preferred to perform these procedures in the presence of an anesthetist.
The endovenous technique has been described previously. 9 In summary, after injection of local anesthesia in puncture site, percutaneous ultrasound-guided (uSmart 3200T, Terason, Burlington, USA) puncture of the GSV at the knee level was done using micro-puncture set (Angiodynamics, Queensbury, New York, USA). The 0.035 propriety guidewire was passed to the SFJ, and then exchanged to the propriety 5Fr long sheath. The cyanoacrylate adhesive was prepared and attached to the delivery catheter. Patient was then put in head-down position. The tip of the 5Fr introducer sheath/cyanoacylate catheter was advanced to the SFJ and positioned 4 cm distal to the SFJ, as measured on the ultrasound screen. There was no need for peri-venous tumescence anesthesia. With proximal compression by the ultrasound probe, the cyanoacylate was injected intravenously as per protocol, with two injections of approximately 0.09 mm were given 1 cm apart at this location, followed by a 3-min period of local compression, and then repeated 3 cm spaced injections and 30 s ultrasound probe compression sequences until the entire length of the target vein was treated. Treatment length of GSV was defined as the length of GSV that received cyanoacrylate adhesive treatment. GSV occlusion and the lack of deep vein thrombosis (with compressibility) were confirmed by duplex ultrasound intraoperatively. Small stab avulsions of varicosities under local anesthesia were performed in the same operative setting.
Patients were discharged same-day post procedure from the vascular ward. Post-procedure compression stockings were used in view of avulsions and the small wounds dressed by community nurses.
Peri-procedure assessment and follow up
All the patients underwent serial clinical and duplex ultrasound examination at 1 week, 1 month, 6 months, and 1 year. The primary endpoint was procedural success rate with obliteration of the GSV, lack of deep vein thrombosis, and lack of clinical recurrence of varicose veins. The complete closure of the saphenous vein was defined as duplex ultrasound noncompressibility/absence of flow signal along the entire treated saphenous vein segment with no discrete segments of patency exceeding 5 cm as read by a qualified specialist vascular ultrasonographers. 10
We also looked at postoperative pain score, ecchymosis at site of puncture and avulsion, side-effects and serious adverse events possibly related to the treatment at discharge time and follow up, time to return to work, improvement in disease specific, and general quality of life scores. The perioperative pain score will be recorded with the patient being asked to rate pain experienced immediate postoperatively on a 0 to 10 numeric rating scale. The ecchymosis at site of puncture and avulsion will be recorded at 1 week and rated as minimal, mild, moderate, or severe. The venous clinical severity score (VCSS) is a well-recognized system in recording venous severity.11,12 To avoid confusion with the CEAP scale and to generate a dynamic score, the categories of the VCSS are presented on an elemental basis to add emphasis to the most severe sequelae of venous disease that are likely to show the greatest change in response to therapy. 13 The VCSS was measured for every leg sequentially preoperatively, at 1 month, 3 months, 6 months, 1 year, and 2 years postoperatively. The Aberdeen varicose vein questionnaire (AVVQ) was developed and validated by Garratt et al. 14 for measuring quality of life in patients with lower limb varicose veins. The AVVQ was asked for every patient preoperatively, at 1 month, 3 months, 6 months, 1 year, and 2 years postoperatively. The Short Form Health Survey 36 Item (SF-36) is a widely-used and well-validated generic quality-of-life instrument.15,16 It assesses two domains: physical health (assessed as the patient’s level of functioning) and mental health (assessed as an indication of well-being). When complete, the survey generates a score ranging from 0 to 100, with higher scores indicating better general health perception. The SF-36 was measured for every patient preoperatively, at 1 month, 3 months, 6 months, 1 year, and 2 years postoperatively. All data were entered prospectively into our departmental computerized database.
Statistical analysis
Incomplete closure or recanalization of the GSVs would be detected by duplex ultrasound. Closure rates over time were analyzed using Kaplan–Meier analysis. Risk factors of mean diameter of GSV, treatment length of GSV, and preoperative clinical score of CEAP were tested for prediction of recanalization using Cox proportional hazard regression analysis. All analyses were performed using SPSS (version 22.0). A p-value of <0.05 was regarded as statistically significant.
Results
Patients and disease characteristics
Baseline characteristics.

The average diameter of the great saphenous vein in the treatment zone as determined by pre-operative duplex ultrasound with the patient supine was 7.1 mm (range 3.9–11.4 mm). The median treatment length of GSV was 27 cm (range 17–33 cm) (Table 1).
Operating procedures
There was no deviation of the protocol: all the GSVs were successfully punctured percutaneously, cannulated according to protocol, and all the cyanoacrylate injections were at precisely 4 cm from the SFJ. All the patients had immediate on-table completion duplex ultrasound to document successful obliteration of the GSV in the treatment segment, and lack of deep vein thrombosis as shown by calf squeeze and compressibility in the common femoral vein. The mean procedural time from aseptic prepping and draping to completion of all avulsions and application of support stockings was 64 min (range 28–99 min).
Postoperative results
The mean pain ratings were low at 0.86 (range 0–3) at immediate postoperative period. All the patients walked home independently. The severity of the ecchymosis at the puncture and avulsion sites as assessed at postoperative day 7 was low: no bruises in 40 legs, mild in 16 legs, and moderate in 1 leg. All the bruises were from avulsion phlebectomy sites and not from the GSV puncture sites.
Post operation, the median time of return to work or normal life was 1 day, ranging from 1 to 16 days. Most of the delay was due to dressings of wounds for the avulsion sites. All of the patients resumed normal daily activities on discharge. Operative complications included two minimal extension of thrombus to deep vein. Both required treatment of subcutaneous low molecular weight heparin injection for 1 week. Reassessment duplex ultrasound afterwards showed completion resolution of the deep vein thrombus. Other operative complications were minor with one minor wound infection over an avulsion surgical site which resolved with wound dressings. One patient had mild paraesthesia over dorsum of the foot which improved upon follow up. With a mean follow-up period 9 months (range 1–13 months), there was no clinical varicose vein recurrence.
Follow-up duplex ultrasound and questionnaire results
Duplex ultrasound follow up
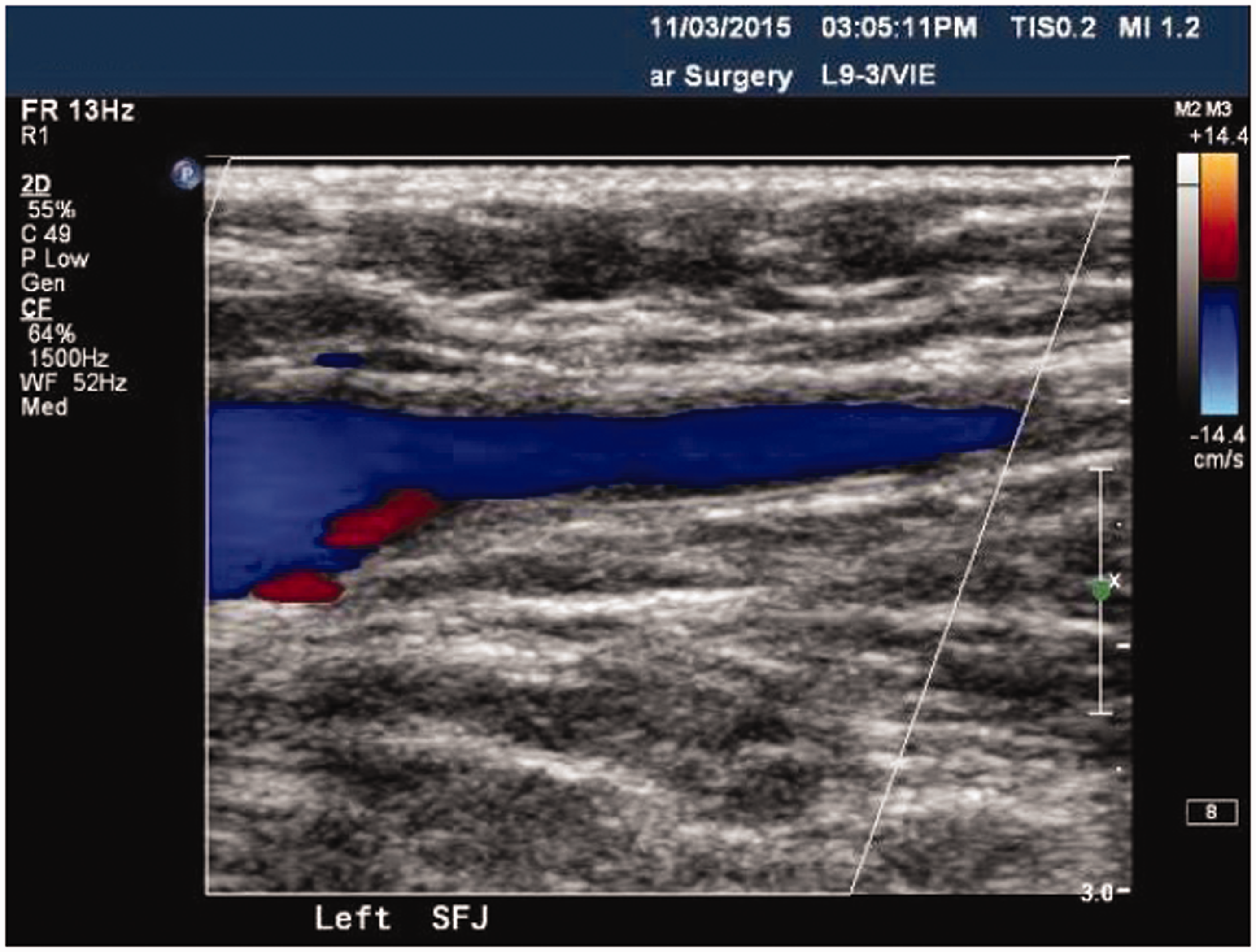
The mean follow-up period of this cohort of patients was 9 months (range 1–13 months). Fifty-seven (100%), fifty-three (75%), and seventeen (30%) legs had passed the 3, 6, and 12 months follow-up points, respectively. None of our patients defaulted follow-up visits. On day 7, all the GSVs in the intended treatment segments were successfully obliterated. At post-op 1 week, 1 month, 6 months, and 12 months, the closure rates were 100%, 95.3%, 90.3%, and 78.5%, respectively (Figure 1). There were no total recanalization. Partial recanalization (defined as any further recanalization compared to previous scans) occurred in seven legs, with one, two, two, and two recanalizations of the proximal GSVs noticed in 1 week, 1 month, 6 months, and 1 year respectively during the follow up (Figure 2). None of the recannalized GSVs resulted in clinical recurrence or deterioration of the CEAP score.
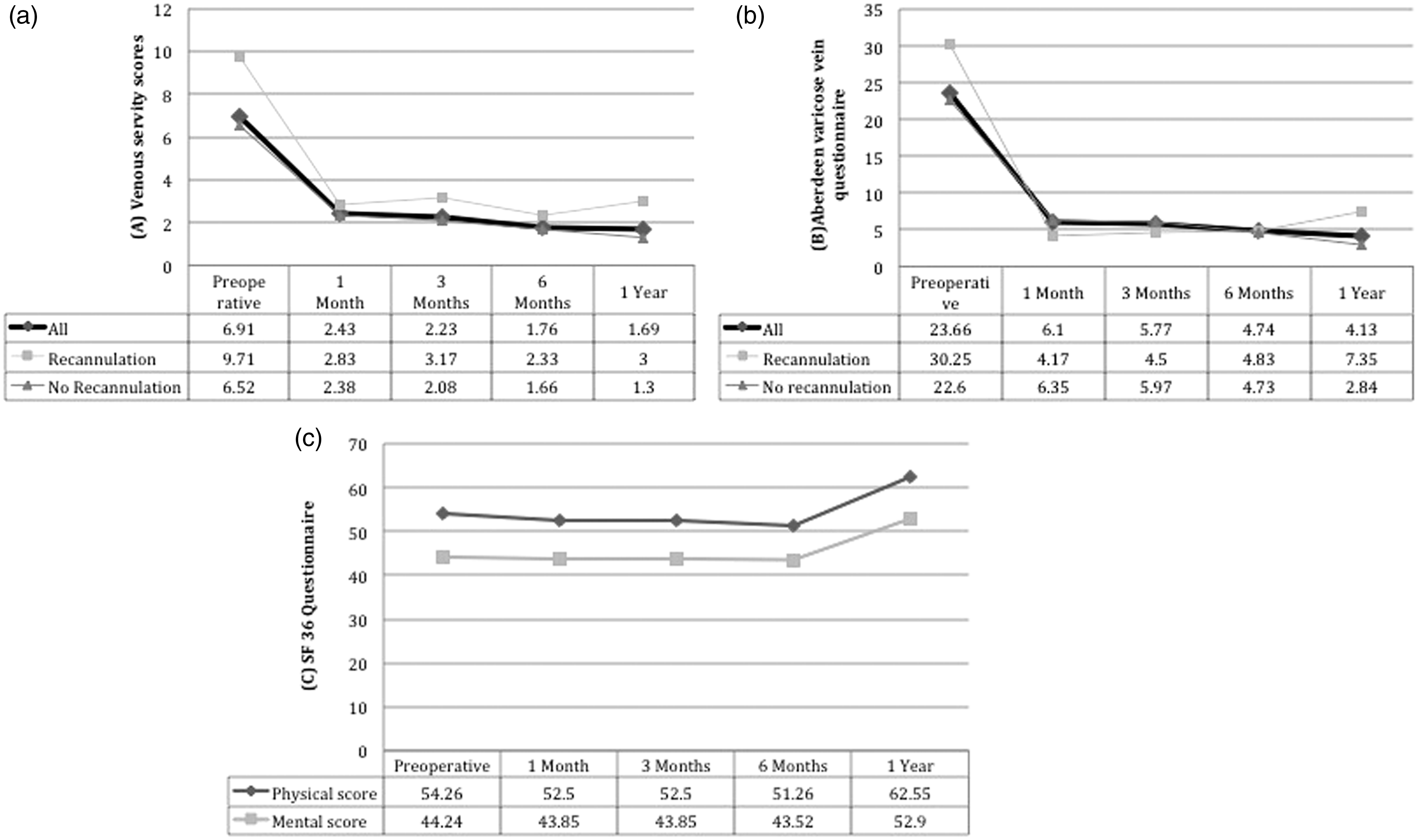
(a) Kaplan–Meier curve showing successful closure of great saphenous veins over time. (b) Comparing closure rates in GSV size <8 mm and ≥8 mm (mean diameter of GSV ≥8 mm, hazard ratio 6.92, 95%CI 1.34–35.67, p = 0.021). Example of a 6-month follow-up duplex showing recanalization of the previously obliterated proximal great saphenous vein. Graphical representation of the venous severity scores (a), Aberdeen varicose vein questionnaires (b), and SF 36 questionnaires (c).
Prediction of recanalization
Predictors for recanalization.

GSV: great saphenous vein.
Closure rates of those GSV <8 mm remained high at 100%, 93.1%, 93.1%, and 93.1% at post-op 1 week, 1 month, 6 months, and 12 months, respectively; whilst that for GSV ≥8 mm, closure rates were 90.9%, 90.9%, 68.2%, and 34.1% at post-op 1 week, 1 month, 6 months, and 12 months, respectively (log-rank test, p = 0.006) (Figure 1(b)).
On the other hand, treatment length of the GSV (hazard ratio 2.59, 95%CI 0.34–19.81, p = 0.359) and preoperative clinical score of the CEAP (hazard ratio 2.29, 95%CI 0.51–10.23, p = 0.280) were not predictive of recanalization (Table 2).
Questionnaire follow up
The results of the VCSS, AVVQ, and the SF-36 surveys are tabulated in Figure 3. Our VCSS scores decreased from a mean ± standard deviation of 6.91 ± 3.45 at baseline to 2.43 ± 1.49, 2.23 ± 1.60, 1.76 ± 1.71, and 1.69 ± 0.95 at 1 month, 3 months, 6 months, and 1 year of follow up, respectively. Those with partial recanalizations presented higher baseline and subsequent scores (Figure 3(a)).
The AVVQ scores decreased from a mean ± standard deviation of 23.66 ± 11.10 at baseline to 6.10 ± 5.55, 5.77 ± 5.88, 4.74 ± 5.46, and 4.13 ± 2.80 at 1 month, 3 months, 6 months, and 1 year of follow up, respectively. The patients with partial recanalizations presented higher baseline and subsequent scores (Figure 3(b)).
Physical scores of the SF-36 questionnaire remained similar from a mean ± standard deviation of 44.24 ± 7.50 at baseline to 43.85 ± 8.22, 43.85 ± 8.22, 43.52 ± 11.08, and 52.90 ± 4.30 at 1 month, 3 months, 6 months, and 1 year of follow up, respectively. Similarly, mental scores of the SF-36 questionnaire remained similar from a mean ± standard deviation of 54.26 ± 9.56 at baseline to 52.50 ± 10.16, 52.50 ± 10.16, 51.26 ± 12.88, and 62.55 ± 1.15 at 1 month, 3 months, 6 months, and 1 year of follow up, respectively (Figure 3(c)).
Discussion
This is a study to show early results with a mean follow-up period of 9 months in the use of commercially available endovenous cyanoacylate glue for trunkal ablation of reflux in the great saphenous veins. We have in this cohort of patients shown successful obliteration of GSVs in the treated segment, with no clinical or duplex evidence of deep vein thrombosis in the common femoral vein. We also showed that this treatment modality is effective and safe in simultaneous treatment of bilateral GSVs (57 limbs in 29 patients) and that one propriety bottle of the cyanoacrylate could be used for both legs in the same clinical session. We have found that one bottle of cyanoacrylate glue is more than enough volume for treatment of both legs, with the median treatment length of GSV of 27 cm (range 17–33 cm). All of the patients had symptomatic improvements post procedure, despite the fact that there were seven cases of partial recanalization on follow-up duplex.
The endovenous cyanoacylate glue (Venaseal™ Sapheon Closure, now Medtronic Medical) system gained Conformité Européene (CE) mark in 2011 and FDA approval in February 2015, and has now been extended to South East Asia with Hong Kong being the only territory where this product could be used. The initial human pilot study was performed by Jose Almeida on eight patients with incompetent GSVs in the Dominican Republic. 17 All the veins were successfully obliterated at 1 month’s follow up and 1-year results were published in abstract form, and all the treated patients experienced clinical improvements with a complete closure rate of >94% after 1 year. 18 Proebstle et al. 19 further reported that all the veins were closed at 24 to 72 h; and there were no significant side-effects or complications and the patients did not have any deep vein thrombosis or pulmonary embolism, but the first 8 of 38 (21%) patients had post ablation thrombus extension through the SFJ. Almeida et al. 20 also reported 2 years’ results of 38 patients, and showed that complete occlusion of the treated GSVs was achieved in all the patients except for one complete and two partial recanalizations observed at 1, 3, and 6 months of follow up, respectively. 20 The Sapheon Closure System Feasibility Study, conducted in the Dominican Republic with 38 patients, completed enrolment in July 2011, and showed a 3-year closure rate of 94.7%.21,22
In a prospective multicenter study conducted in seven European centers between 2011 and 2012, 69 unilateral GSVs were treated, and with a median follow up of 3 months, with complete occlusion rates of 95% and 90% at 3 and 6 months, respectively. 23 To date, there is only one published, randomized controlled prospective multicenter study. The VeClose Study reported early results of a randomized trial of cyanoacrylate versus radiofrequency ablation. 7 A total of 108 patients received cyanoacrylate, and 114 had radiofrequency ablation with the ClosureFast system (Covidien, Mass). The follow-up period was relatively short, with a 3 months’ closure rates being 99% for cyanoacrylate and 96% for radiofrequency ablation. Pain experienced during the procedure was mild and similar between the two treatment groups, and the authors concluded that cyanoacrylate was noninferior to radiofrequency ablation for the treatment of incompetent GSV. 24
The European Sapheon Closure System Observational Prospective (eSCOPE) Study is an on-going study involving three venous centers in the United Kingdom to assess the role of the cyanoacrylate in the closure of incompetent GSV. 24 In this study, the efficacy and safety will be compared to appropriate literature reports to determine if the results of the treatment of reflux disease with the Sapheon Closure System are consistent with or better than the expectations. Additional comparison points may include measurements of pain and/or length of time to return to work. Incomplete occlusion and recanalization appeared to be caused by continued flow of blood from venous tributaries into the treated long saphenous vein resulting in areas of failed closure. 24 In this study, we found that GSV diameter of >8 mm were more likely to be associated with proximal recanalizations on follow up.
Recently, Toonder et al. 25 has shown that cyanoacrylate can also be used to obliterate perforator incompetence under ultrasound guidance, in a technique called cyanoacrylate adhesive perforator embolization (CAPE). In a small series, it was shown that cyanoacrylate adhesive perforator embolization could be used effectively with up to 76% occlusion rate of incompetent perforating veins without serious complications.
There are limitations to our study. This study is a single-center nonrandomized series. However, in view of the prospective data collection and the many bilateral cases, it is anticipated that that this may be a pilot study platform for planning a further randomized controlled trial for simultaneous treatment of both legs, which may be an interesting addition to the VeClose Study.
Conclusion
Our early results showed that simultaneous treatment of bilateral incompetent GSVs can be performed using one bottle of cyanoacrylate glue and, thus, may make the procedures more cost-effective than treating one leg at a time. Our analyses for recanalization showed that GSVs >8 mm were more likely to have recanalization on follow up, although the precise mechanism for this is unclear.
Contributions
Study design: YC
Data collection: YC, YL, GC.
Data analysis: YC, YL, GC.
Writing: YC
Critical review of paper: YC, AT, SC.
Revision of paper: YC, YL, GC.
Ultimate responsibility: YC.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Division of Vascular & Endovascular Surgery, Department of Surgery, University of Hong Kong Medical Centre, Hong Kong.