
Abstract
Background
Breast reconstruction is associated with multiple risk factors for venous thromboembolism. However, the incidence of deep vein thrombosis in patients undergoing breast reconstruction is uncertain.
Objective
The aim of this study was to prospectively evaluate the incidence of deep vein thrombosis in patients undergoing breast reconstruction using autologous tissue transfer and to identify potential risk factors for deep vein thrombosis.
Methods
Thirty-five patients undergoing breast reconstruction were enrolled. We measured patients’ preoperative characteristics including age, body mass index (kg/m2), and risk factors for deep vein thrombosis. The preoperative diameter of each venous segment in the deep veins was measured using duplex ultrasound. All patients received intermittent pneumatic pump and elastic compression stockings for postoperative thromboprophylaxis.
Results
Among the 35 patients evaluated, 11 (31.4%) were found to have deep vein thrombosis postoperatively, and one patient was found to have pulmonary embolism postoperatively. All instances of deep vein thrombosis developed in the calf and were asymptomatic. Ten of 11 patients underwent free flap transfer, and the remaining one patient received a latissimus dorsi pedicled flap. Deep vein thrombosis incidence did not significantly differ between patients with a free flap or pedicled flap (P = 0.13). Documented risk factors for deep vein thrombosis demonstrated no significant differences between patients with and without deep vein thrombosis. The diameter of the common femoral vein was significantly larger in patients who developed postoperative deep vein thrombosis than in those who did not (P < 0.05).
Conclusions
The morbidity of deep vein thrombosis in patients who underwent breast reconstruction using autologous tissue transfer was relatively high. Since only the diameter of the common femoral vein was predictive of developing postoperative deep vein thrombosis, postoperative pharmacological thromboprophylaxis should be considered for all patients undergoing breast reconstruction regardless of operative procedure.
Introduction
In recent decades, venous thromboembolism (VTE) has been highly discussed in the USA and Europe because it brings about death during operation. Major breast reconstruction warrants additional prophylaxis considerations, and it has been generally accepted that surgical cases included in the orthopedic and general surgery literature were sufficiently similar in their anatomical location, degree of invasiveness, and patient population to make them comparable from a VTE risk perspective. 1 By contrast, less emphasis has been placed on the risk of VTE in Japan because Japanese plastic surgeons do not pay much attention to the risk of VTE at present.
Recently, several reports concerning chemoprophylaxis for VTE after plastic surgery have discussed that the practice was effective without increasing problematic bleeding-related complications.1–4 The guidelines of the American College of Chest Physicians for the prevention of VTE recommend that plastic surgery patients should be stratified using the Caprini’s risk assessment models. 5 Incidence in plastic surgery category has been reported by Pannucci et al. 6 They stratified plastic surgery patients without chemoprophylaxis by Caprini’s risk assessment model. They showed that the Caprini’s risk assessment model effectively stratified plastic and reconstructive surgery patients for perioperative VTE risk. 0.61% in patients in Caprini score 3–4, 1.27% in patients in Caprini score 5–6, 2.69% in patients in Caprini score 7–8, and 11.3% in patients in Caprini score over 8 had VTE event between postoperative days 0 and 60. The higher patients had its score, the more they suffered from VTE events. However, they collected data not by ultrasound but from medical records. They missed asymptomatic VTE. Deep vein thrombosis (DVT) was detected at a rate of 10–40% in patients without chemoprophylaxis after general surgery. 7 However, accurate incidence of DVT after plastic surgery is uncertain. 1 Although the risks of VTE are significant, there is a reluctance to use prophylaxis because of bleeding concern. 4 In Japan, chemoprophylaxis for VTE has not been widely adopted. At our institute, we have not used any chemoprophylaxis agent to prevent VTE in plastic surgery patients to date. Therefore, the current study sought to evaluate the incidence of DVT in patients undergoing autologous tissue transfer and to identify potential risk factors for DVT.
Materials and methods
Patients
This study was approved by Tokyo Women’s Medical University Research Ethics Committee. Consecutive referral patients undergoing autologous breast reconstruction between April 2011 and June 2014 were eligible for the study. The patients’ preoperative characteristics, including age, body mass index (BMI, kg/m2), congestive heart disease, hormone replacement therapy, inflammatory bowel disease, central venous catheter placement, previous history of DVT, and renal failure were all evaluated. Based on these data, we calculated Caprini score preoperatively. D-dimer testing was done preoperative and postoperative day 3. All patients used graduated compression stockings, and pneumatic compression devices were applied intermittently while patients were confined to bed. Although patients were encouraged to walk on postoperative day 1, most of them were unable to walk on postoperative day 3. In this study, chemical thromboprophylaxis was not performed.
Preoperative venous duplex ultrasound
The presence of DVT was diagnosed using compression ultrasound. A color duplex scanner (LOGIQ 7 PRO, and LOGIQ S8 PRO, GE Health Care Japan, Tokyo, Japan) with a 10 MHz transducer was used. Initially, each patient was placed supine in the reverse Trendelenburg position at 15°. Examinations began at the common femoral vein (CFV) and then moved to the femoral vein at the adductor canal. The anterior and posterior tibial veins (ATV and PTV, respectively) were also recorded. Afterward, the patient was placed prone with the knee flexed at 30°, and the residual popliteal, peroneal, gastrocnemius, and soleus veins were evaluated. The diameter (cm) of each venous segment was also measured before surgery.
Operative procedure
In this study, we used four different types of flaps to reconstruct after mastectomy. Donor sites for our breast reconstruction are roughly divided into two groups, using a flap from the abdomen and from the back. The choice of technique depends on patients’ breast size, habitus, and availability of donor flap sites.
8
A flap from the abdomen has three types of flaps, superficial inferior epigastric artery flap (SIEA flap), deep inferior epigastric artery perforator flap (DIEAP flap), and transverse recutus abdominal myocutaneous flap (TRAM flap). These flaps have a large amount of skin and adipose tissue. Therefore, it is a good option for patients who require moderate to large breast reconstruction. Another option for patients who have relatively small breast mounds is latissimus dorsi myocutaneous flap.
9
Formerly TRAM flaps were commonly used for breast reconstruction as an abdominal flap. TRAM flap is nourished by superior epigastric artery (SEA) and vein (SEV), and deep inferior epigastric artery (DIEA) and vein (DIEV). On the one hand, SEA and SEV are used when the pedicled TRAM flap is raised. On the other hand, DIEA and DIEV are used when the free TRAM flap is raised. However, the most common complication of the use of after TRAM flaps for breast reconstruction was abdominal wall hernia due to lack of rectus abdominis muscles. To avoid this disadvantage, plastic surgeons have tried to preserve the rectus abdominis as much as possible. Consequently, muscle sparing-TRAM flap was introduced. Finally, DIEAP flap was introduced. This flap doesn’t contain the rectus abdominis muscles.
10
Using the DIEAP flap has reduced postoperative complication more than using TRAM flap. For these reasons, DIEAP flap was widely used despite its lengthy operation. Concerning the SIEA flaps, the blood supply to the adipocutaneous layer is derived from the superficial inferior epigastric vessels. Thus, the use of SIEA flap results in minimum abdominal donor site morbidity.
11
One of the disadvantage of the use of superficial inferior epigastric vessels, however, was that they are often very small and short.
12
To detect sufficient nutrient vessels in the planning of free flap operations, computed tomography angiography (CTA) was routinely used. If large superficial epigastric vessels were identified on CTA, SIEA flap was preferred. Flowchart of the selection of autologous breast reconstruction is shown in Figure 1.
Flowchart of the selection of autologous breast reconstruction.
Study outcome
The primary study outcome was the development of DVT on postoperative day 3 and day 7. Postoperative DVT was defined as the presence of a noncompressible segment of the vein in B-mode and lack of spontaneous flow on color Doppler imaging.
Statistical analysis
All data were analyzed using the SPSS software package (Version 20.0; SPSS Inc., Chicago, IL, USA). Comparisons of numerical data between groups of patients were made using Wilcoxon rank sum test. Fisher’s exact test and chi-square test were used to evaluate differences between proportions. Continuous data were expressed as mean ± standard deviation (SD). P values < 0.05 were considered to indicate statistical significance.
Results
Patient characteristics
Distribution of postoperative VTE.

ATV: anterior tibial vein; DVT: deep vein thrombosis; PTV: posterior tibial vein; PV: peroneal vein; SV: soleus vein; VTE: venous thromboembolism.
In terms of risk factors for VTE, one patient had renal failure and four patients received hormone replacement therapy before operation. In this study, no patients had congestive heart disease, inflammatory bowel disease, central venous catheter placement, or previous history of DVT. Only one of four patients receiving hormone replacement therapy developed DVT.
Baseline characteristics.

BMI: body mass index; DVT: deep vein thrombosis.
Values are expressed as mean ± SD. P values determined by Wilcoxon rank sum test.
Caprini’s risk assessment model.

DVT: deep vein thrombosis.
Ultrasound-derived parameters
Preoperative ultrasound-derived parameters.
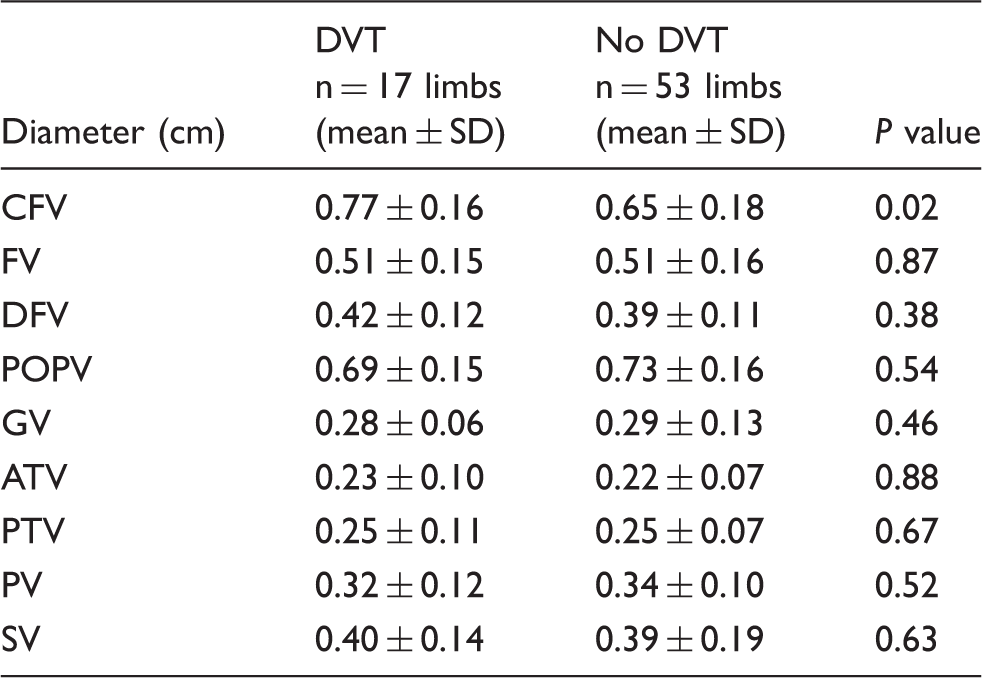
ATV: anterior tibial vein; CFV: common femoral vein; DFV: deep femoral vein; DVT: deep vein thrombosis; FV: femoral vein; GV: gastrocnemius vein; POPV: popliteal vein; PTV: posterior tibial vein; PV: peroneal vein; SV: soleus vein.
Values are expressed as mean ± SD. P values determined by Wilcoxon rank sum test.
Operative methods
Comparison of operative methods.
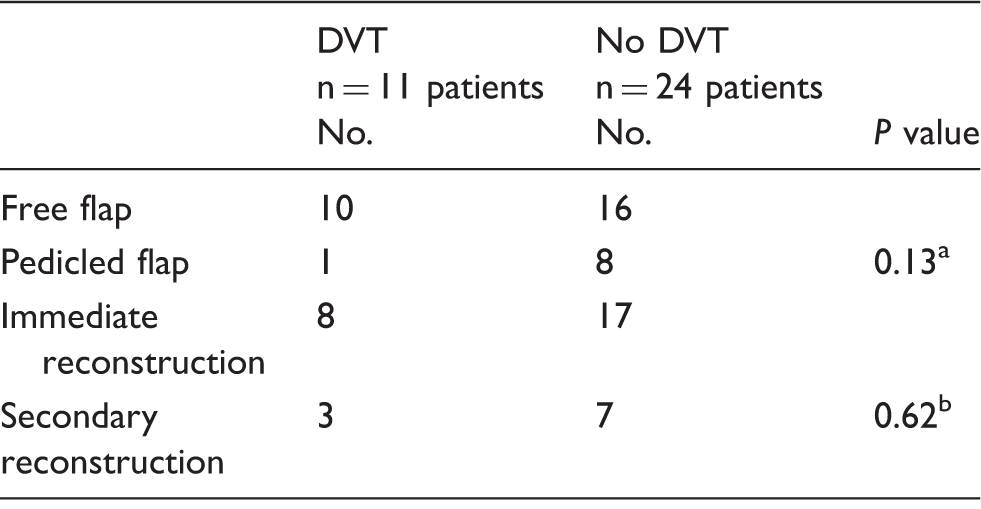
DVT: deep vein thrombosis.
Chi-square test.
Fisher’s exact test.
Frequency of autologous breast reconstruction type and VTE.
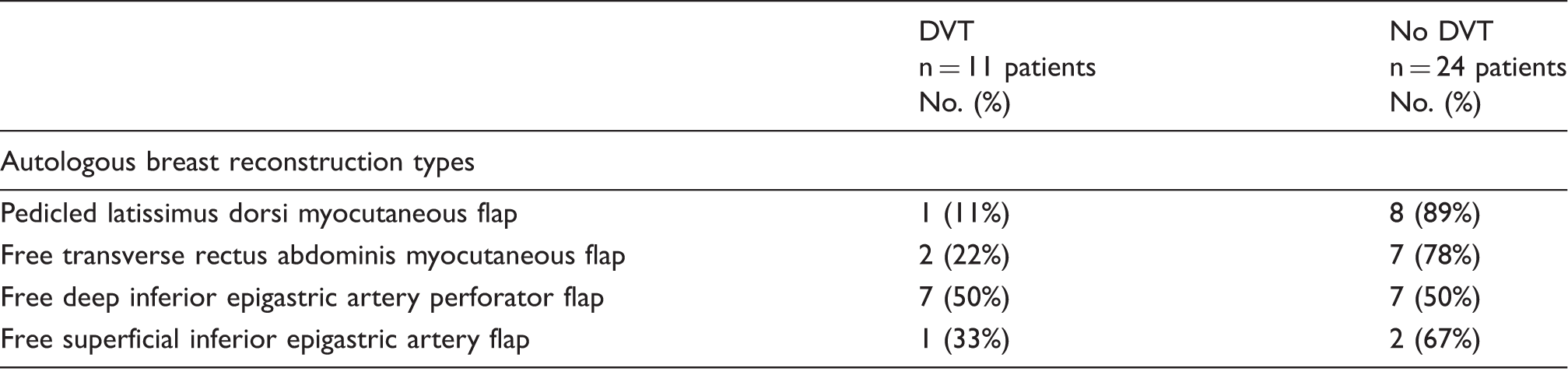
DVT: deep vein thrombosis; VTE: venous thromboembolism.
Discussion
Confirmed DVTs after autologous breast reconstruction have been reported as a complication in some previous reports, and most of them were symptomatic.13,14 The reported rate of symptomatic DVT ranges from 0.5 to 2.2%, and plastic surgeons have demonstrated poor compliance with established guidelines for VTE prophylaxis. 15 Calf DVT is more likely to be asymptomatic 16 and a lower associated risk of PE. 17 Therefore, calf DVT has been widely overlooked. Furthermore, the rate of asymptomatic DVT occurrences without thromboprophylaxis remains uncertain. 18 In other surgery populations, DVT risk without thromboprophylaxis was approximately 10–40%. In this study, we found that patients undergoing breast reconstruction with autologous tissue transfer had a relatively high incidence (31.4%) of postoperative DVT, similar to that reported in other fields of surgery. In those populations, thromboprophylaxis for DVT was recommended. 7
Two previous studies have investigated the efficacy and safety of chemoprophylaxis in breast reconstruction patients, reporting that subcutaneous heparin did not result in a significant increase in bleeding but was associated with a significant reduction in the rate of DVT.19,20 Kim et al. 2 found that the incidence of asymptomatic pulmonary thromboembolism was significantly lower in patients administered low-molecular-weight heparin than in those with no chemoprophylaxis. Lemaine et al. reported that the incidence of postoperative DVT confirmed by duplex ultrasound was 3.4% in patients who received chemoprophylaxis. This DVT rate is approximately one-tenth of that observed in the present study of patients who received no chemoprophylaxis. Free flap surgeries have been reported as a risk factor for VTE.21,22 Our patients only had asymptomatic calf DVT, which is not as severe as proximal DVT. Only 3% of calf DVT cases left untreated and monitored with serial compression ultrasonography developed proximal extension. However, when patients who have undergone breast reconstruction surgery develop calf DVT, they face a considerable number of risk factors (i.e. cancer, major surgeries, and long bed confinement). Among our patients, one (2.9%) had PE. Hofer et al. 23 reported the incidence of PE after autologous breast reconstruction as 3.8%. Kim et al. 2 found that the incidence of PE after autologous breast reconstruction without thromboprophylaxis was 1.8%. Furthermore, after using LMWH, the authors did not observe PE in their patients. They also did not find an increased rate of bleeding complication using thromboprophylaxis.2,23 Accordingly, patients who have undergone breast reconstruction surgery need treatment with antithrombotic therapy to reduce the risk for thromboembolic complications. Antithrombotic therapy is associated with a risk of major hemorrhage of 0.6–1.2% and a risk of fatal bleeding of 0.1–0.4%. 24 With a complete understanding of this condition, we need to introduce chemoprophylaxis in the field of plastic and reconstructive surgery. Patients who are candidates for free flaps already have many risk factors for DVT. They typically suffered from malignant tumors, heavy trauma, and lengthy confinement to bed. Masoomi et al. 25 found that pedicled TRAM flap was associated with the highest VTE rate among autologous breast reconstruction patients. The VTE rate of latissimus dorsi myocutaneous flap was similar to that of the free TRAM flap. Thus, the free flap surgeries themselves may not carry additional risk for DVT. Our study also lacked the statistical power to discriminate a difference in DVT risk between the use of free flap surgeries and pedicled flap surgeries.
We observed a significantly larger CFV diameter in patients who developed postoperative DVT compared to those who did not. Large CVF may result from any obstruction above the CFV. We hypothesized that there would be some obstruction above the CFV in the DVT groups. However, we did not investigate the venous system above the CFV. Therefore, it remains unclear whether a larger CFV is attributable to our hypothesis. Masoomi et al. 25 found that immediate reconstruction after mastectomy compared with delayed reconstruction, age over 65 years, prior chemotherapy, obesity, and chronic lung disease were associated with higher risk of in-hospital VTE in patients undergoing breast reconstruction surgery. In our study, D-dimer levels measured on postoperative day 3 demonstrated had significant power of postoperative DVT after autologous breast reconstructive surgery. However, this did not result in statistically significant difference. On the other hand, patients who developed postoperative DVT had Caprini’s score > 5 preoperatively. Hence, to avoid overtreatment we had to better apply DVT chemoprophylaxis for patients who had Caprini’s score > 5. Overall, candidates for autologous breast reconstruction had a high risk of postoperative DVT. Therefore, routine postoperative VTE chemoprophylaxis is necessary for the postoperative care of autologous breast reconstruction patients with at least over Caprini’s score 5.
This study includes several notable limitations. First, the patient population was small. There were no cases of symptomatic DVT and only one case of symptomatic PE in this study. We were unable to identify any parameters as potential risk factors for DVT. However, the symptomatic VTE rate was similar to previous reports. We believe that this study provides valuable data on the incidence of symptomatic and asymptomatic VTE in this patient population.
Conclusions
Although the incidence of DVT was relatively high in the cohort of patients undergoing breast reconstruction confirmed by ultrasound, the incidence of symptomatic VTE/PE was low. The use of free flaps was not significantly associated with higher DVT incidence. As VTE complications were not noted in patients undergoing breast construction with a Caprini score < 4, postoperative pharmacological thromboprophylaxis should be considered in those patients with a score > 5, regardless of operative procedures.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.