
Abstract
BACKGROUND:
Reconstructive surgery is established as a standard treatment option after mastectomy due to cancer. It is crucial to patients to achieve a natural and symmetric looking breast through reconstruction. Anthropometric measurements are used to assess the objective symmetry of the breast, which are prone to errors and difficult to reproduce.
OBJECTIVE:
The aim of this work is to validate breast volumetry using three-dimensional surface imaging.
METHODS:
We compared preoperatively analog and digitally evaluated volume of the breast with our gold standard, direct water displacement measurement of the mastectomy specimen. We examined 34 breast specimens in total.
RESULTS:
Each measurement method (Breast Sculptor, VAM, Breast-V) for breast volume/mass determination demonstrates acceptable agreement ranges when compared with resected volumes and masses. The strongest volumetry instrument is Breast Sculptor (digital), the weakest is Breast-V (analog).
CONCLUSIONS:
3D surface imaging is a quick, effective, and convenient method to evaluate breast shape and volume. The accuracy, reproducibility, and reliability of 3D surface imaging were comparable with MRI in our study.
This takes us a step closer to the long-term goal of establishing robust instruments to plan breast reconstructive surgery, achieve better surgical results, and contribute to quality assurance in breast surgery.
Introduction
With about 69,000 new cases in Germany every year, breast cancer is by far the most common cancer in women. In addition, more than 6,000 women are diagnosed with an in-situ tumor annually. Based on the current incidence rates, approximately one in eight women will develop breast cancer during their lifetime. Furthermore, nearly three out of ten affected women are younger than 55 years of age on diagnosis [1, 2]. Reconstructive surgery after mastectomy is now established as a standard treatment option. Many patients consider the symbolic loss of the breast as an abandonment of their sexual identity. In addition to functional advantages in everyday life, the restoration of the breast is a fundamental coping strategy for many patients in dealing with their disease [3]. It is therefore crucial to achieve a natural-looking breast through reconstruction. A study into patients after breast reconstruction was able to reveal that both patients and the attending surgeons strive for breast symmetry [4]. Previous studies have already demonstrated the decisive psychosocial importance of visual breast symmetry for patients [5–7]. The objective symmetry of the breast in the context of reconstructive breast surgery is often assessed using anthropometric measurements. In clinical practice, these are usually obtained manually with the aid of a measuring tape directly on the patient. The necessary measurement points (so-called landmarks) are typically determined by palpation. This method is easy to use; however, the measurements obtained are subject to error and are difficult to reproduce. Moreover, the determination of landmarks is subjective and dependent on the experience of the examiner. Finally, this method is time-consuming and uncomfortable for the patient [8].
Thanks to rapid technological advances, three-dimensional (3D) surface imaging and volume evaluation using digital anthropometry has become possible [9–12].
The aim of this work is to validate breast volumetry using three-dimensional surface imaging. We compare the preoperatively evaluated volume of the breast with our gold standard, the volume of the mastectomy specimen measured during surgery. Our aim is to answer the questions as to which preoperative measurement method is the most accurate; whether 3D volumetry is more accurate than the conventional analog method; and whether it is comparable to the accuracy of MRI volumetry.
Patients and methods
A total of 25 patients undergoing planned mastectomy were included in our prospective study. Of these 25 patients, nine underwent bilateral mastectomies and 16 unilateral mastectomies. We examined 34 mastectomy specimens in total. Data were collected from June to October 2020 and the study was approved by the Ethics Committee of the University Hospital of Regensburg (20-1653-101 and amendment 20-1653_1-101). The metadata of our participated patients are summarized in Table 1. It should be noted that one patient (n = 1) was underweight at the time of data collection with a body mass index (BMI) of less than 18.5 kg/m2. Normal body mass with a BMI of 18.5 to 24.9 kg/m2 was recorded in 17 patients (n = 17). Overweight with a BMI of 25 to 29.9 kg/m2 was presented by three patients (n = 3). Three further patients presented grade I obesity with a BMI of 30 to 34.9 kg/m2 (n = 3). Finally, one patient (n = 1) suffered from grade II obesity with a BMI of 35 to 39.9 kg/m2. None of the patients in the study population was determined as grade III obese with a BMI of greater than 40 kg/m2.
Summary of study cohort demographics and description
Summary of study cohort demographics and description
The indication for mastectomy was either carcinoma, carcinoma in situ, or prophylaxis. Depending on the indication, we performed either a modified radical mastectomy (MRM) (n = 17) or subcutaneous mastectomy (n = 17).
Individual therapy courses (neoadjuvant chemotherapy, radiotherapy, trastuzumab therapy, and many more) and histopathological findings of the resected specimens (receptor status, tumor size, grading, mammary tumor stages, and many more) of the study participants were researched and compiled to better classify the results. Relevant metadata of the oncological findings are displayed in Table 2.
Summary of the oncological findings for all 25 patients
All patients were measured manually using a standard tape measure along the skin surface. Pre-operative breast volume was calculated using the Breast-V formula, as proposed by Longo et al. [13] for ptotic breasts and extended by Huang et al. [14] for non-ptotic breasts. Both formulae have been employed in several studies previously [15, 16]. Breast-V is a tool to determine volume, it actually calculates in grams in direct comparison of mastectomy specimens during surgery. An assumption of 1g = 1 ml is used by the Breast-V app such that the calculated mass is the estimated volume. In our study, we preferred to avoid this approximation and compared the calculated mass with the actual mass of the specimen.
Digitally assessed volumetry of the female breast
In addition, we measured breast volumes and various breast dimensions using the portable Vectra® H2 (Canfield Scientific, USA) photogrammetry scanning system. This system allows us to reproduce the total surface information for an individual patient. The system is supplied with Vectra Breast Sculptor (Canfield Scientific, USA) software for point cloud processing and mesh generation and with Vectra Analysis Module (VAM). Both applications allow analysis of the 3D model in terms of breast volume and various breast dimensions, as previously demonstrated in a number of studies [7, 17–19]. Thus, 14 points were marked on the patient and subsequently selected in Breast Sculptor and in VAM (See Fig. 1). Subsequently, the volume was output for both programs. All measurements were performed three times and then averaged. The operator was blinded to reduce bias.
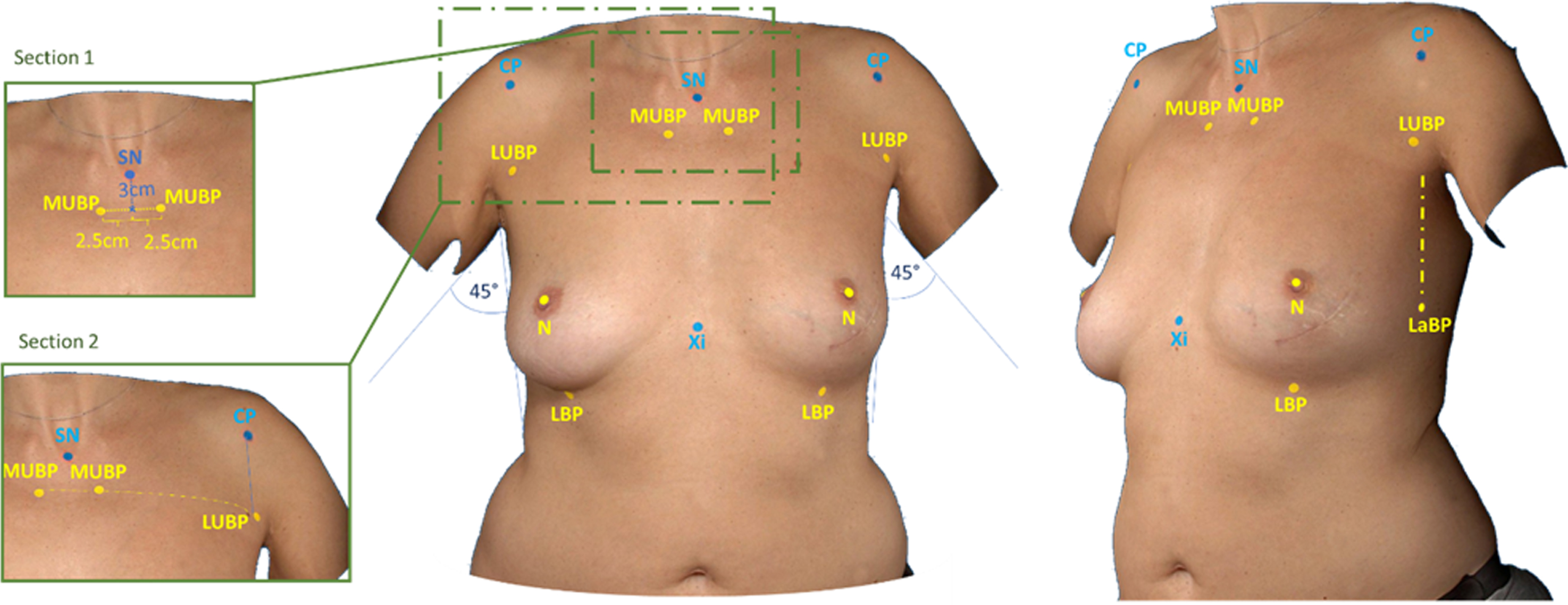
Standard landmarks for 3D imaging with palpation of the CP (coracoid process), SN (sternal notch), and Xi (Processus xiphoideus), measurement of MUBP (medial upper breast pole) and LUBP (lateral upper breast pole) (Sections 1 and 2), and spotting of N (nipples) and LBP (lower breast pole).
Vectra provides an intuitive user interface (see Fig. 2).
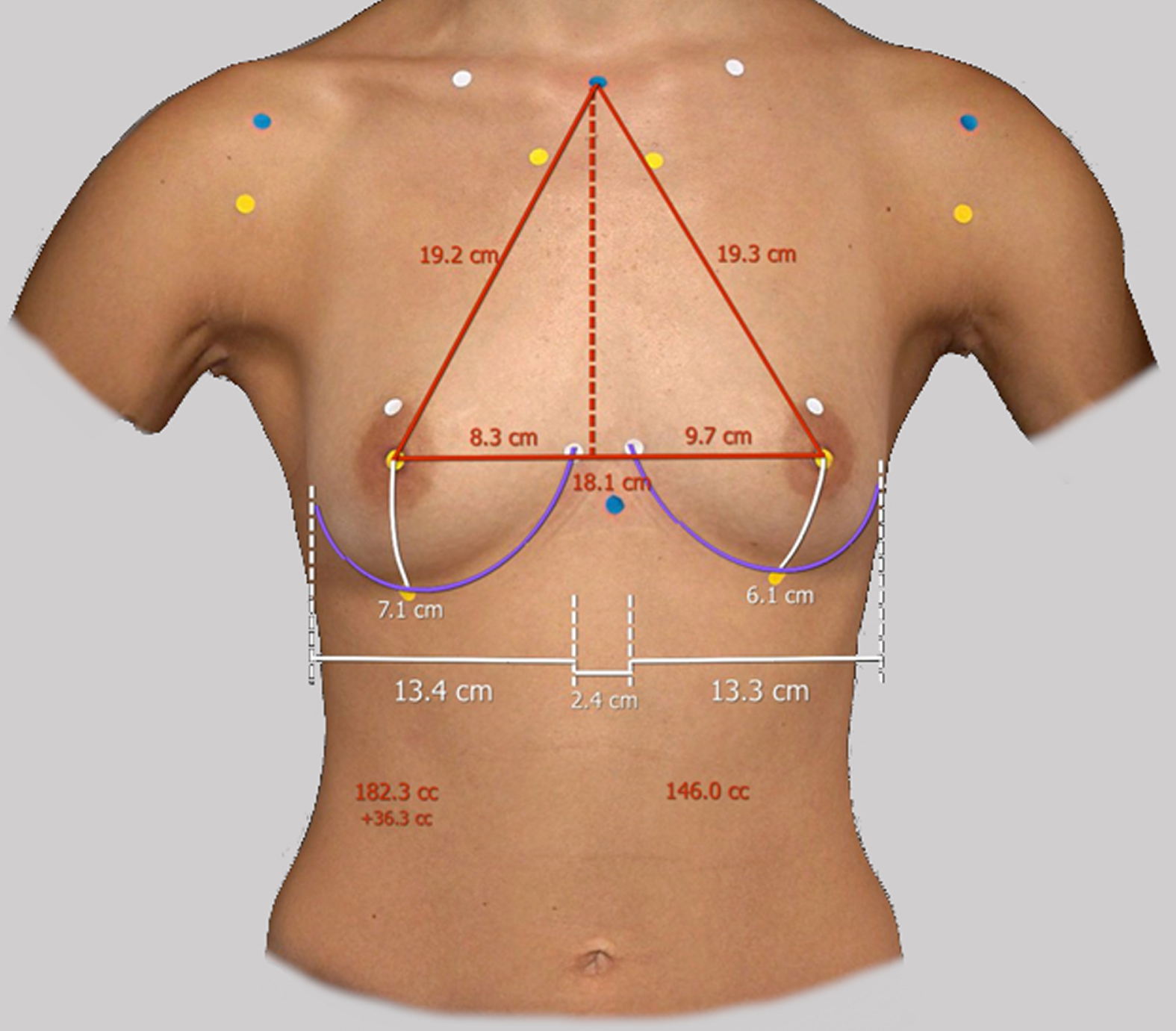
Vectra H2 3D Imaging and VAM calculation.
Each breast volume measurement was performed three times in succession for the same breast (n = 50) by one examiner. A mean value was calculated from this, which served as the measured value for further evaluation. How reliable this mean value is concerning the intra-observer reliability could be illustrated with the intraclass correlation coefficient (ICC), a descriptive statistic to evaluate the reliability and reproducibility of quantitative measurements. This was performed for both Breast Sculptor and VAM measurements.
MRI volumetry
MRI examinations of both breasts were already digitally available for three patients. Retrospectively, the volume measurement was performed using a 1.5 Tesla MRI scanner (Siemens Avanto fit, Siemens Healthcare, Erlangen). Patients underwent a routine standard MRI protocol performed in the prone position using a bilateral dedicated 18-element breast coil. It was ensured that the patient was lying in the prone position with both breasts hanging freely in the bilateral openings of the breast coil.
The standard breast MRI protocol comprises the following scans: a T2 STIR (Short-Tau Inversion Recovery), a T2 without fat suppression and a DWI (diffusion-weighted MRI; b = 50, 800 s/mm2). Subsequently a dynamic perfusion study with an intravenous injection of 0,1 mmol/kg of Gadovist (Bayer Vital GmbH, Germany) is performed, which is followed by flushing with 20 ml of saline solution at 1 ml/s. Examinations covered the entire breast in the axial and sagittal planes. Two blinded examiners performed the breast measurements.
The volume analysis was performed on the T2 STIR sequence in the axial plane. Sequence parameters were as follows: TR (repetition time) = 5000 ms, TE (echo time) = 83 ms, slice thickness = 5 mm with 0.5 mm intersections gap, field of view 340×340 mm; matrix 320×224. The breast boundary was drawn manually using the vendor-specific “freehand ROI” tool (syngo MR E11, Siemens Healthcare, Erlangen) [19]. MRI scanning consistently demonstrated the highest accuracy [22].
Water displacement volumetry
The mastectomy specimen volume was measured using water displacement. A graduated water vessel with a capacity of two liters was prepared in the operating room and filled with 800 ml 0.9% saline solution. The excised breast specimen was placed inside the vessel, and the displacement volume of the mastectomy specimen could be read off the scale. (See Fig. 3)
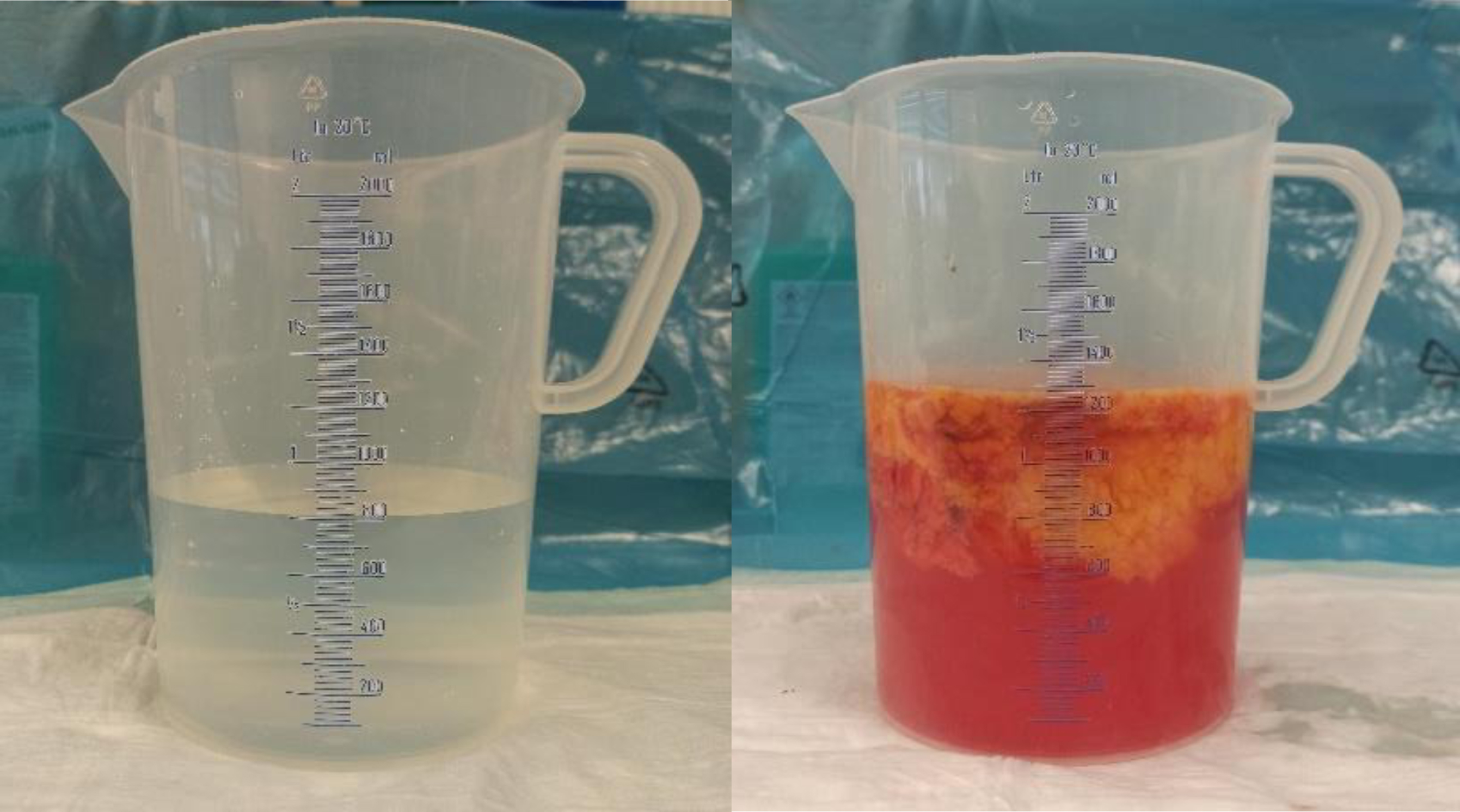
Graduated vessel for water displacement volumetry.
The investigator performing the water displacement volumetry had not been informed of the result of the preoperative evaluation of the breast volume (either analog or digitally); we thus accepted them as a blinded examiner.
SPSS Statistics version 25.0.0. (IBM, Armonk; New York) was used to carry out the statistical analysis. We answered the question of agreement and thus the question of the clinical suitability of the new measurement with Bland-Altman plots (BAPs). These were generated using MedCalc Software (Version 20.113, MedCalc Software Ltd, Belgium). BAPs illustrate the extent of agreement between the measurement methods. Our gold standard was set as the water displacement volumetry of the specimen and the mass of the specimen.
Results
Breast density
The volume and the mass of the resected tissue were measured intraoperatively. Figure 4 portrays the scatter plot of specimen volumes and masses. Pearson’s correlation coefficient r between the measurements is 0.99 (95% CI 0.9798 to 0.9950, p < 0.0001). The plotted measured values are distributed symmetrically around the regression line. The regression line does not align with the angle bisector y = x. Thus, we cannot assume absolute equality of the measured values.
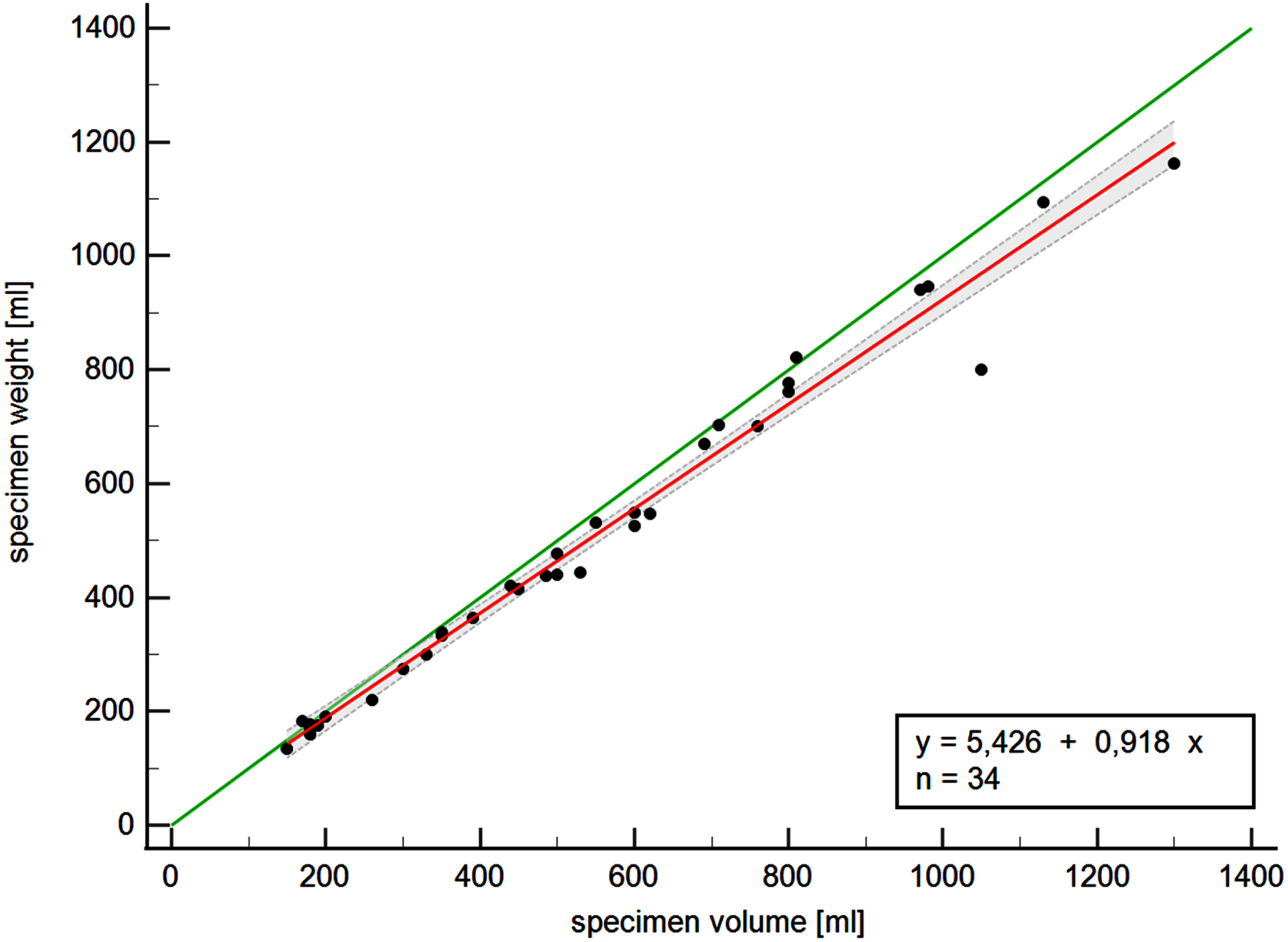
Scatter plot of specimen volumes and masses with angle bisector (green) and regression line (red).
The density of breast tissue is calculated as the quotient of specimen mass and volume. Table 3 summarizes the breast densities of the subcutaneous mastectomies (n = 17), the MRM (n = 17), and for all 34 mastectomy resections.
Density of the resected tissue
For our comparison, intraoperative volume measurement by the water displacement method is used as the gold standard. Each method was compared to this standard using BAPs. As an example, Fig. 5 portrays the BAP between the standard (Y-axis) and the value measured by Breast Sculptor.
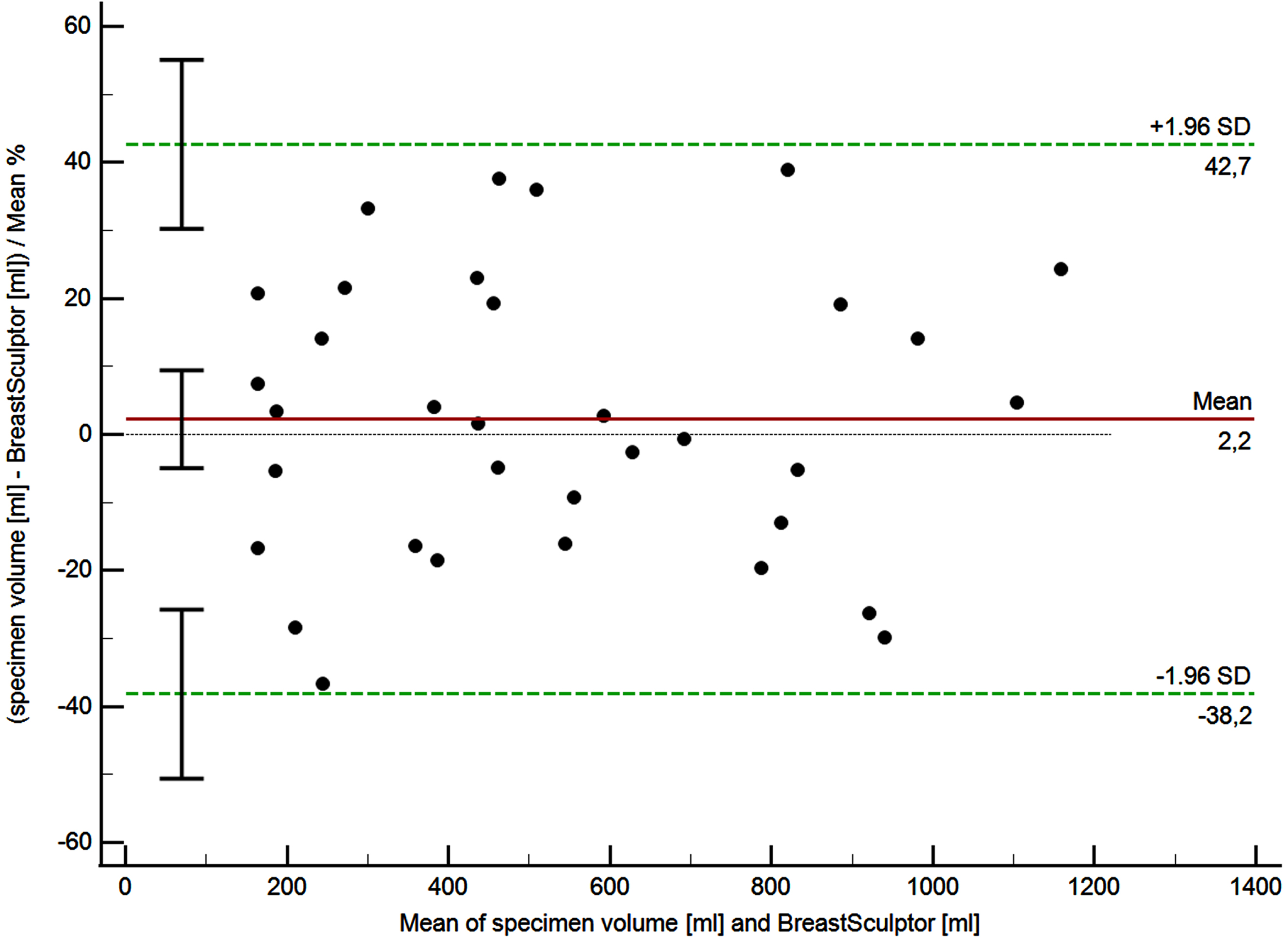
Bland-Altman plot of agreement between resection volume and breast volume measurements with Breast Sculptor. The figure depicts the percentage measurement differences.
All results are summarized in Table 4 and graphically illustrated in Fig. 6. It should be noted that this is not a boxplot.
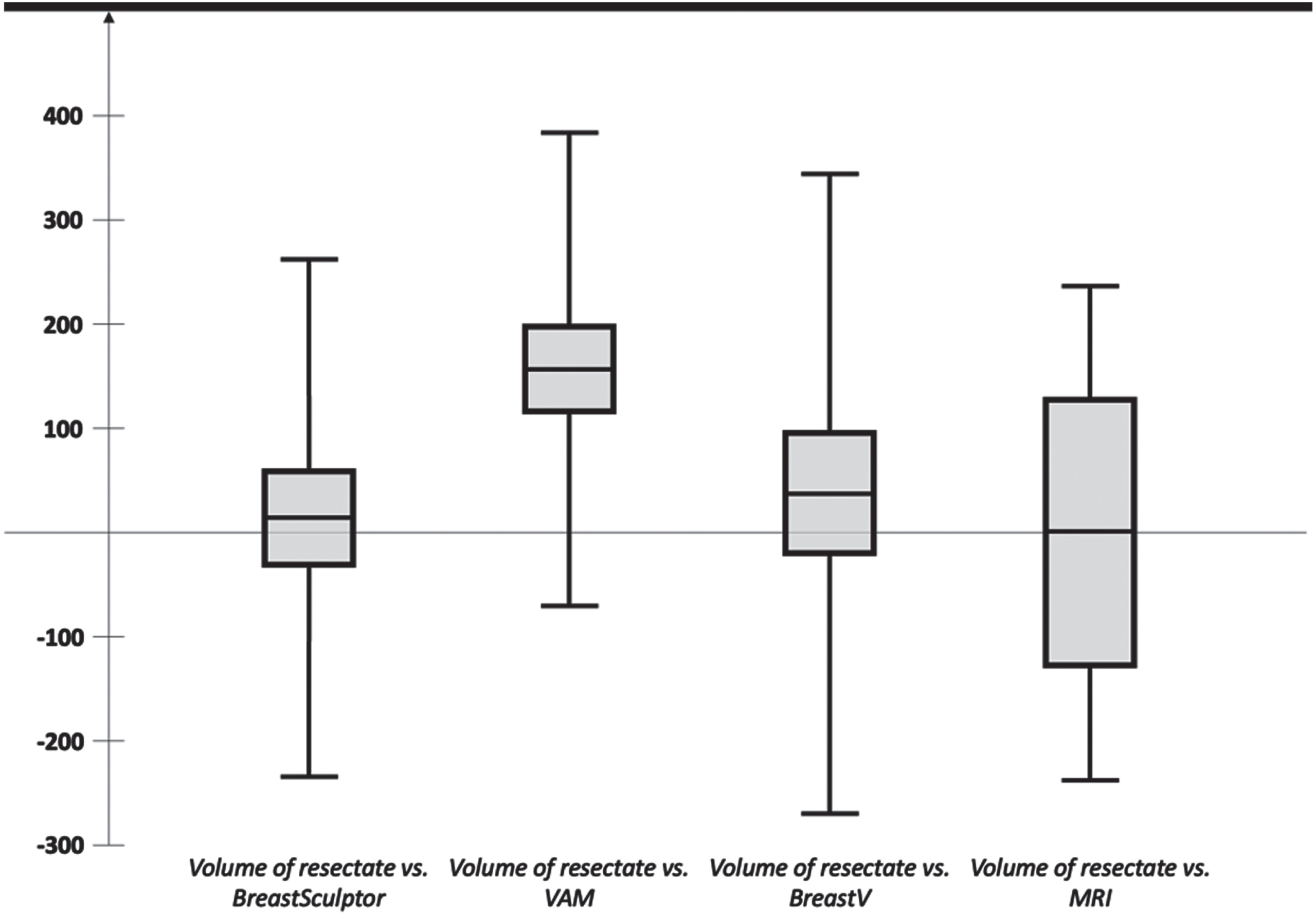
Graphical representation of the absolute results of Bland-Altman plots. Mean measurement difference is in the center of each box. The box represents the confidence interval of the mean measurement difference. The lower and upper limits of agreement are given as the limits of the plots (no boxplot).
Summary of the absolute results of Bland-Altman plots on breast volume and mass evaluation with Breast Sculptor, VAM, Breast-V, and MRI (Ø MD = mean measurement difference, ↓LoA = lower limit of agreement, ↑LoA = upper limit of agreement)
The ICC of the breast volume measurements with the Breast Sculptor® software from Vectra® resulted in a correlation coefficient of 0.996 (p < 0.001). Since this is greater than 0.9, one can assume excellent reliability of the measurements and thus of the calculated mean. Likewise, the ICC of the breast volume measurements with the VAM resulted in a correlation coefficient of 0.997 (p < 0.001). Since this is greater than 0.9, one can assume excellent reliability of the measurements and thus of the calculated mean.
Discussion
The three measurement methods (Breast Sculptor, VAM, Breast-V) for breast volume/mass determination demonstrate acceptable agreement ranges when compared with resected volumes and masses.
VAM demonstrates the smallest agreement range of±230 ml for predicted breast volume compared to actual specimen volume. However, there is a systematic error with VAM: the program also systematically underestimates breast volume compared to specimen volume by approximately 150 ml.
The Breast Sculptor software demonstrated the smallest mean measurement difference when compared to specimen volumes. No systematic deviation could be detected. The agreement range of±250 ml is acceptable.
The Breast-V and specimen masses revealed no systematic deviation, but the agreement range is the widest at±310 g compared to other measurement methods. Calculation of breast volume using analog anthropometric measurements such as Breast-V may be cost effective but is less accurate than 3D volumetry of the breast.
In our small MRI collective, the agreement range of±237 ml is very comparable to the 3D measurement and Breast Sculptor evaluation.
In our study, the agreement range of the 3D volumetry is very similar to the agreement range of the MRI. The wide confidence interval of the MRI volumetry is certainly a consequence of the small collective, which is the first limitation of our study.
Based on the recording technique, we would have expected 3D volumetry to be more reliable in smaller breast volumes than in large breast volumes, since the underside of the large ptotic breast is hidden. Nevertheless, the agreement between the respective intervals remains satisfactory independent of the actual breast size.
The second limitation of our study is the potential inaccuracy of the water displacement volumetry. We calculated the breast density and compared our data with that found in the literature. We found similar densities of the breast tissue in our study population [23, 24]. Yip et al. even view water displacement volumetry as the gold standard [20]. The fact that all volumetry measurements (analog or digital) were made without knowing the results of other volumetry measurements is a real strength of the study. All examiners were blinded.
Conclusion
Three-dimensional surface imaging is a quick, effective, and convenient method to evaluate breast shape and volume. The accuracy, reproducibility, and reliability of 3D surface imaging were comparable with MRI in our study.
Our study takes us a step closer to the long-term goal of establishing robust instruments to plan breast reconstructive surgery, achieve better surgical results, and contribute to quality assurance in breast surgery. In addition to clinical research, we were able to publish open source the world’s first statistical model of the breast, the “Shape Model of the Breast” [19]. This statistical model will lead us to a simplification of volumetry using hand-held devices or smartphones.
Footnotes
Acknowledgments
This study would not have been possible without the support of Regensburg Medical Image Computing (ReMIC), Ostbayerische Technische Hochschule Regensburg (OTH Regensburg), Regensburg, Germany. Together we have established a multidisciplinary research group with medical informaticists, plastic surgeons and gynecologists, the Digital Plastic Surgery Research Group.