
Abstract
Objective
The aim of this study was to observe the change of the ankle joint range of motion, the muscle strength values measured with an isokinetic dynamometer, pain scores, quality of life scale, and venous return time in chronic venous insufficiency diagnosed patients by prospective follow-up after 12-week exercise program including isokinetic exercises.
Methods
The patient group of this study comprised 27 patients (23 female, 4 male) who were diagnosed with chronic venous insufficiency. An exercise program including isokinetic exercise for the calf muscle was given to patients three days per week for 12 weeks. At the end of 12 weeks, five of the patients left the study due to inadequate compliance with the exercise program. As a result, control data of 22 patients were included. Ankle joint range of active motion, isokinetic muscle strength, pain, quality of life, and photoplethysmography measurements were assessed before starting and after the exercise program.
Results
Evaluating changes of the starting and control data depending on time showed that all isokinetic muscle strength measurement parameters, range of motion, and overall quality of life values of patients improved. Venous return time values have also increased significantly (p < 0.05).
Conclusion
In conclusion, increase in muscle strength has been provided with exercise therapy in patients with chronic venous insufficiency. It has been determined that the increase in muscle strength affected the venous pump and this ensured improvement in venous function and range of motion of the ankle. In addition, it has been detected that pain reduced and quality of life improved after the exercise program.
Introduction
Functional disability of muscle pump due to impaired muscle strength plays an important role in the pathophysiology of chronic venous insufficiency (CVI). Exercise therapy is recommended to eliminate the problem of muscle pump dysfunction.1,2
In the study of De Moura et al., 3 it has been reported that walking speed, range of motion (ROM), strength, and functional capacities of patients with CVI were worse than those of normal individuals. Yang et al.4,5 have found that calf muscle strength and endurance of patients with CVI were insufficient compared to the control group of healthy individuals.
Cetin et al. 1 have reported that calf muscle function as well as thigh muscle function are significantly impaired, and exercise programs to improve the lower extremity strength will be useful in the treatment of CVI.
Other researchers have also reported that decline in venous compliance can be improved by ROM, strength, and endurance exercises and by compression therapy.2,6,7
ROM exercises and isometric and isotonic strengthening exercises for the ankle muscles are the exercises that can be recommended. 8 In the literature, ROM exercises and isometric strengthening exercises have been applied to patients, and significant results were obtained. However, there is no study investigating the effectiveness of isokinetic muscle strength exercises.
We made the design of our study on this deficiency in the literature. ROM exercises, resistance training with Theraband, isokinetic exercises at angular speeds of 60°/s, 90°/s, 120°/s, stability exercises, walking exercises, and intermittent pneumatic compression pump was applied to patients with CVI three days a week for 12 weeks under physician supervision.
The aim of this study was to observe the change of the ankle joint ROM, the muscle strength values of plantar flexion (PF) and dorsiflexion (DF) measured with an isokinetic dynamometer, Visual Analog Scale (VAS) scores, EQ-5D quality of life scale, and venous return time (VRT) in CVI-diagnosed patients by prospective follow-up after giving calf muscle strength enhancing (exercise) workout programs.
Methods
The patient group of this study comprised 27 patients (23 female, 4 male) who were diagnosed with stage C3–C4 CVI by the CEAP (Clinical signs (C), etiology (E), anatomical features (A), underlying pathophysiological cause (P)) classification according to patients’ history, the findings of the physical examination, doppler ultrasonography and photoplethysmography (PPG) tests at the Cardiac and Vascular Surgery Clinic of Süleyman Demirel University Medical Faculty.
Risk factors for CVI among the study group were determined as prolonged standing in 13 patients, pregnancy in 9 patients, obesity in 4 patients, and history of thrombophlebitis in 1 patient. In addition, eight patients got the history of CVI in family members displaying genetic tendency to CVI. Informed consent was obtained from all the patients in the study group in accordance with the Helsinki Declaration, and the approval for the study was granted by the Local Ethics Committee of Süleyman Demirel University with Decision No. 90 at meeting on 27 March 2013.
Summary of exercise program.
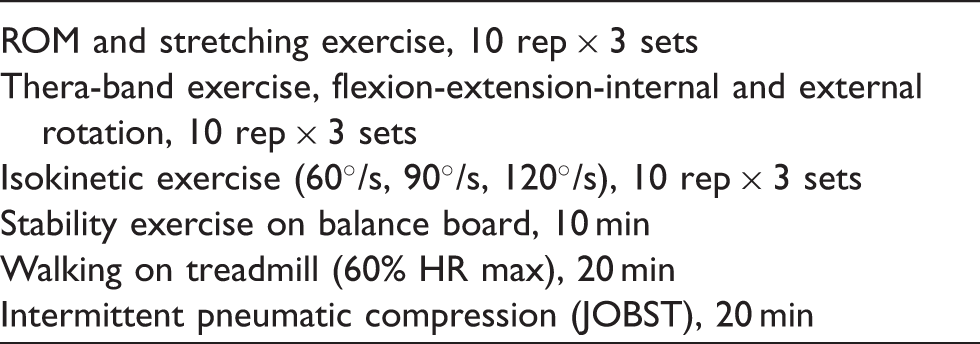
ROM: range of motion; rep: repetition; s: second; HR: heart rate; max: maximum; min: minute.
Patients’ ankle joint ROM, isokinetic muscle strength, pain, quality of life, and PPG measurements were assessed before starting and after the exercise program.
The presence of painful venous ulceration, active local infections, the patient incompatibility during the test, non-compensatory heart and lung failure, peripheral arterial disease, diabetes, vasodilator treatment, orthopedic disorders of the ankle, and any systemic disease which would prevent the working on the isokinetic dynamometer was defined as exclusion criteria.
PPG device (ELCAT Vasoquant VQ1000 D-PPG®, Germany) was used for VRT measurement and CVI grading, while isokinetic dynamometer (HUMAC® NORM™ Testing & Rehabilitation System, USA) was used for isokinetic muscle strength measurements and exercises.
PPG measurements of the patients whose history and physical examination findings were compatible with stage C3–C4 CVI were carried out by the cardiovascular surgeon. According to results of PPG, patients who have VRT values below 25 s and who do not have the exclusion criteria were included in the study. The grade of CVI was recorded as mild insufficiency if the VRT was 20–24 s, moderate if VRT was 10–19 s, and severe if VRT was <10 s. Patients were directed to the sports medicine physician after diagnosis and staging.
VAS scoring was used to define the severity of the complaints of the CVI patients, and EQ-5D quality of life scale was used in order to determine the effect of CVI on the overall quality of life.
The ankle joint range of active motion was measured by the metal goniometer (Baseline Stainless, USA) before isokinetic muscle strength measurements of patients.
Submaximal warming exercise was performed on the cycle ergometer for 10 min before muscle strength test, and stretching exercises were performed for 5 min before and after muscle strength test. Peak torque (PT) and total work values of ankle PF and DF have been detected with isokinetic tests.
The ankle PF and DF muscle strength tests were applied at speeds of 60–120°/s in concentric/concentric mode. The tests were applied in prone position at a ROM of 15°DF and 40°PF.
After the tests, patients were included in the exercise program. Exercises continued three days a week for 12 weeks (60 min per session and 20 min JOBST for recovery). Patients did not use varsity socks and did not receive any medical treatment during this period.
The data of patients with treatment compliance over 90% were included in the study and were analyzed.
Statistical Analyses
Statistical analysis was performed with SPSS version 22 software. The frequency distribution of data was investigated. Descriptive statistical data were given as mean ± standard deviation. Accordance of the group with normal distribution was determined with Kolmogorov–Smirnov test. Changes of the starting and control data depending on time were evaluated with Dependent samples t test. The evaluation of the test statistics was made at a significance level of alpha = 0.05.
Results
Initially 27 patients were included in the study. At the end of 12 weeks, five of the patients left the study due to inadequate compliance with the exercise program. As a result, control data of 22 patients were included.
Twenty patients were female and two were male (mean age: 48 ± 9 years, mean height: 159 ± 7 cm, and mean body weight: 72 ± 13 kg).
According to lower extremity PPG measurements, CVI was observed in a total of 39 lower extremities, consisting of 17 right side and 22 left side. Thirty-three of them were determined as stage C3 CVI while six were stage C4 CVI.
Of the 17 right lower extremities, CVI was determined as mild in 4, moderate in 9, and severe in 4, while of 22 left extremities, CVI was determined as mild in 3, moderate in 17, and severe in 2.
Clinical analyses values.
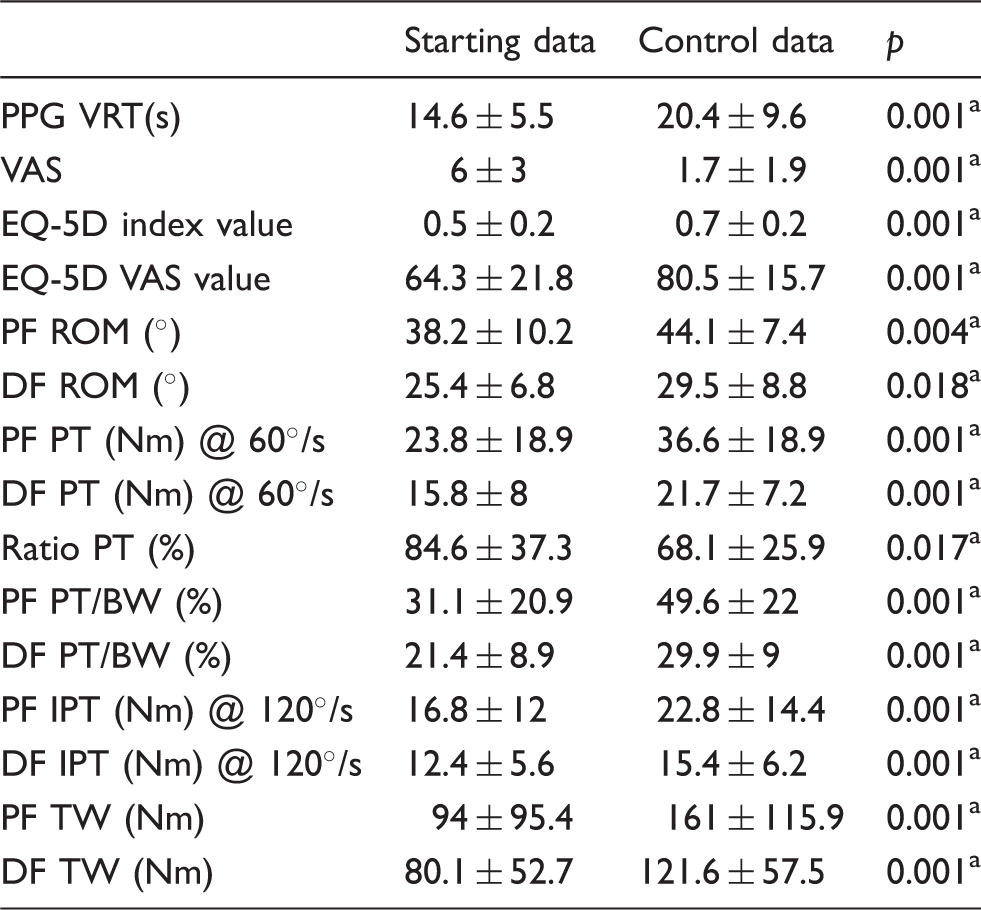
Note: Data are given as mean ± standard variation. PPG: photoplethysmography; VRT: venous return time; s: second; VAS: Visual Analog Scale; PF: plantar flexion; DF: dorsiflexion; ROM: range of motion; Nm: Newton meter; PT: peak torque; BW: body weight; IPT: initial peak torque (mean of first three repetition); TW: total work.
Statistically significant difference.
Discussion
At the end of our study, all isokinetic muscle strength measurement parameters, ROM, and overall quality of life values of patients improved. VRT values have also increased. These data showed that calf muscle exercise program for 12 weeks improved the ankle joint ROM, muscle strength, overall quality of life, and the VRT and reduced pain in CVI patients.
Failure in the calf muscle pump function with venous reflux is the basis of pathophysiology in CVI. In previous studies, severity of venous ulceration which is the final stage of CVI has been found as being associated with pump function failure. 9 Therefore, it is important to determine the degree of muscle pump and venous function insufficiency.
It was emphasized that when the effect of exercise on muscle strength is released, decline in disease or improved venous function will be detected. In our case series, time-dependent VRT increase with increase in muscle strength was detected after exercise application. These findings also support the positive effects of exercise in the treatment of patients with venous insufficiency.
There are several different methods for the evaluation of venous function in many other studies. In the study of O’Brien et al., 10 calf muscle pump function measurements were made with the use of air plethysmography after a 12-week home-based progressive resistance exercise program, and the authors have reported that the ejection fraction has increased and the residual volume fraction has reduced. Padberg et al. 2 have investigated the hemodynamic effects of exercise by duplex ultrasound scanning and air plethysmography and reported that after six months of exercise, the calf muscle pump parameters returned to normal, but there was no change in the degree of reflux and the stage of the disease. In addition, Yang et al.4,5 have not detected any change in the venous reflux although there was an increase in ejection fraction and decrease in residual fraction in the air plethysmography measurements after six-week intensive exercise program. These studies show an improvement in the calf muscle pump function as in our study, but it is not obvious whether there is a significant change in the VRT.
Several theories regarding the pathophysiology of pain in CVI patients have been presented. One of these theories points at the change in the sensory innervation of venous wall, the other points at the increase in endoneurial venous pressure and microangiopathic venous ischemia. 11
Pain levels in patients with CVI show correlation with the stage of the disease. 11 VAS is a commonly used method in the determination of the level of pain or in the comparison of pre and post treatment pain levels of CVI patients.1,11,12 In this study, we also used VAS for the definition of pain levels in the CVI patients. VAS scores of our case series were decreased in the 12th week of control.
Calf pain caused by insufficiency of calf pump is frequently seen in the 60- to 65-year-old people. Subhedar et al. 13 have observed that VAS scores of the patients reduced by the strength exercises for quadriceps and calf muscles.
Pain is not the most important symptom in all cases. Feeling of heaviness, itching, cramps, and other symptoms can also be detected which can make the diagnosis difficult. The degree of clinical symptoms and progression of the disease is correlated with the overall quality of life of patients. 11
“EQ-5D quality of life scale” used in our study is a general health scale. Turkish validity and reliability studies of the scale are made. 14 Statistically significant increase was detected between our patients start and control EQ-5D scale values.
Regular contraction of the calf muscles is an essential factor for lower extremity venous return. 15 The calf muscle pump is called as “peripheral heart” owing to its role in venous return from the lower extremities. 16 A long-term weakness in the calf muscles leads to the slowing down of lower extremity blood flow and increased risk of deep venous thrombosis. 15 It has been indicated that exercises to rehabilitate the muscle pump function, in addition to medical or surgical treatment, may be useful as supportive therapy in patients with severe CVI.1,2,4,17,18
As it is shown in various researches, calf muscle strength and endurance are lower in patients with CVI.6,19 Changes in muscle structure can be shown both morphologically and pathophysiologically. Investigations performed on muscle biopsies of CVI patients have shown type 2 myofibrillary atrophy in the gastrocnemius muscle, muscle necrosis, regeneration, denervation, ischemic muscle cells denaturation, inflammatory cell proliferation, and interfascicular vein dilatation damage.18,20
Muscle performance is traditionally evaluated by manual muscle testing. However, manual muscle testing determines just the force which occurs at a certain point of the width of movement; therefore, it does not provide accurate and reliable results. Furthermore, parameters such as work, force, and endurance can not be obtained by manual muscle testing, and it has been reported that the rate of 23%–31% deficit was determined in isokinetic knee test applied to patients who displayed normal results by manual muscle testing.
Isokinetic test provides a quantitative measurement of the musculoskeletal system performance. Acquired objective parameters provide possibility to save the patient’s follow-up data and to evaluate the disease improvement. Isokinetic testing allows the kinematic analysis of the movement by the comparison of the two sides in the extremity segments, by determining the rate of agonist/antagonist muscle strength rates and by the measurement of the work capacity and endurance of muscles movement. Feedback may be given to the patient during the test and exercise by showing his own performance graphics or numerical results on a monitor. 21 Ankle isokinetic muscle strength evaluations are used safely in researches with all these positive aspects.22,23 In this study, isokinetic dynamometer has been used in the ankle muscle strength measurements and treatment programs of CVI patients.
ROM in which the measurement will be made is of great importance in terms of standardization of the isokinetic muscle strength measurement tests. Koutsioras et al. 24 have carried out the isokinetic muscle strength measurements on the ankle muscles of the running long jump athletes in the prone position at 15°DF, 40°PF, and 55°ROM. 24 Considering the earlier studies done, we performed isokinetic muscle strength measurements and isokinetic exercises at a ROM of 15°DF and 40°PF in our study.
According to the evaluation of patients beginning and control values, increase in all isokinetic strength measurement parameters and decrease in agonist/antagonist strength ratio were observed (in the aspect of PF and DF). Positive changes from baseline occured in our study.
O’Brien et al. 10 have investigated the efficacy of walking and calf muscle exercise in their study and at the end of 12 weeks, they found an increase in ROM and improvement in walking, balance, and quality of life.
In another study, 49 CVI patients with healed venous ulcers were compared with control group, and difference between groups was found in terms of the ankle PT/BW in the direction of PF and the total work parameters. 25
Kan et al. 17 have applied supervised isotonic calf muscle exercises to 10 patients with venous ulcers for seven consecutive days and detected a significant improvement in venous volume ejection fraction at the end of the exercise period. In this study, it has been shown that calf muscle exercises will provide improved venous function even in such a short period of one week.
Kahn et al. 26 have showed that six-month training program provided an improvement in 95 patients with post-thrombotic syndrome. The applicability of exercise therapy in patients with post-thrombotic syndrome can be evaluated in multicentered clinical trials. Thus, it has also been reported that exercise therapy is important in the lower extremity venous system diseases other than CVI.
Agonist/antagonist ratio, obtained by isokinetic muscle force measurements, gives the rate of muscles which provide opposite movements of the joint. DF/PF muscle ratio must be 33% for the functional capability and stability of the ankle joint. 27 This rate has been found to increase due to the weakness in the calf muscle in patients with CVI. Cetin et al. 1 have reported the rate of 51 ± 14% for DF/PF in CVI patients in their case series. 1
At the beginning of our research, agonist/antagonist ratio of the ankle of patients was higher than healthy individuals. Patients start and control agonist/antagonist ratio values showed a significant decrease.
The slightest change in the ROM of the ankle may cause greater hemodynamic changes. A change of 1.5 cm in ankle rotation axis leads to 8.3% increase in extension PT. 28 Dix et al. 29 have showed that restriction in the ankle ROM was correlated with the stage of venous disease. 29 The ankle exercises are suggested to be beneficial as they help the calf muscle contraction and protect the ROM of the ankle. 30
Back et al. 31 have demonstrated that in patients with CVI, the ROM is lower than in normal individuals and the reflux increases, ROM decreases in correlation with the degree of the disease. In accordance with Back et al., Shiman et al. 32 have also reported that there is a reduction of ROM of patients with venous ulcers, and venous hypertension will decrease with calf strength and ROM exercises.
In our study, we plan to create meaningful change in the ROM values with hemodynamic alterations by adding ROM exercises and stretching workouts to the exercise program. Evaluation of the control data after the 12-week exercise program showed a significant increase in ROM.
In our study, VRT increased by 12 weeks of exercise. While the regulatory impact of exercise on venous function has been demonstrated once more in this study, the effect of isokinetic exercise has been studied for the first time in the literature.
Evaluation of the data obtained in this study led to the following conclusions:
Increase in muscle strength is being provided with exercise therapy in patients with CVI. In addition to the increase in muscle strength, the increase in muscle strength affects the venous pump and this ensures improvement in venous function. Improvement in the ROM of the ankle is provided. Pain reduces and quality of life improves after the exercise program.
Footnotes
Acknowledgements
The authors would like to thank all the participants for graciously donating their time and also like to thank Mustafa Onur Serbest, Aykut Recep Aktas, Yonca Sonmez, and Emel Sesli Cetin for their assistance in this research. The authors also thank Scientific Research Projects Coordination Department of Suleyman Demirel University.
Author contributions
The study design was created by CÇ, SE and TY. SE and TY diagnosed the cases. SE, HMD, and YBA treated the patients. All data were collected by SE, HMD, and YBA. SE and CÇ analyzed the data and wrote the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The approval for the study was granted by the Local Ethics Committee of Suleyman Demirel University with Decision No. 90 at meeting on March 27, 2013.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Scientific Research Projects Coordination Department of Suleyman Demirel University Research Grant 3618-TUI-13.
Guarantor
SE and CÇ.