
Abstract
Objectives
Chronic venous disease (CVD) is a progressive condition affecting the lower limb venous system, leading to venous hypertension, muscle dysfunction, and gait alterations. Patients with CVD often experience muscle weakness, reduced ankle mobility, and impaired gait biomechanics. However, the impact of CVD severity on spatiotemporal gait parameters and plantar flexor strength remains little explored. The present study aimed to compare gait biomechanics, plantar flexor strength, dorsiflexion ankle range of motion, and functional performance among patients with mild, moderate, and severe CVD, classified according to the CEAP system.
Methods
A cross-sectional study was conducted in two phases. Phase 1 compared gait parameters between healthy individuals and patients with CVD. Phase 2 examined variations in movement patterns across CVD severity groups, classified according to CEAP class into mild CVD (CEAP 1; n = 11), moderate CVD (CEAP 2–3; n = 12), and severe CVD (CEAP 4–6; n = 6). Gait parameters, including speed, stride length, and stance time, were assessed using a motion capture system. Plantar flexor strength was measured with a handheld dynamometer. Ankle dorsiflexion range of motion was assessed using the Weight-Bearing Lunge Test (WBLT), and functional performance was evaluated using the Human Activity Profile (HAP) questionnaire.
Results
No significant differences were observed in spatiotemporal gait parameters between healthy individuals and patients with CVD or across disease severity groups. In contrast, normalized plantar flexor strength differed significantly among groups (p = .041). Ankle dorsiflexion range of motion was also reduced with increasing disease severity (p = .005), particularly in the severe group. No significant differences were found for HAP scores.
Conclusion
CVD severity was associated with reduced plantar flexor strength and ankle dorsiflexion range of motion, while spatiotemporal gait parameters remained unchanged. These findings suggest that musculoskeletal impairments may precede detectable alterations in gait, highlighting the importance of early assessment and targeted rehabilitation strategies in patients with CVD.
Introduction
Chronic venous disease (CVD) is a heterogeneous clinical condition involving multiple morphological and functional alterations of the venous system. The disease is a consequence of venous hypertension caused by valvular abnormalities associated with calf pump dysfunction.1–3 The primary classification for the disease is based on the Clinical Etiological Anatomical Pathophysiological (CEAP) classification. The CEAP classification ranges from CEAP 0, indicating no visible or detectable signs of venous disease, to CEAP 6, signifying an active venous ulcer. This classification encompasses the spectrum of CVD from CEAP 0 to CEAP 6, including telangiectasias and reticular veins (CEAP 1), varicose veins (CEAP 2), and edema (CEAP 3). The more advanced stages of the disease, corresponding to CEAP classes 4 to 6, are characterized by chronic venous insufficiency (CVI), which includes trophic skin changes (CEAP 4), healed venous ulcers (CEAP 5), and active ulcers (CEAP 6).3–5 A significant portion of the global population is affected by CVD. A systematic review demonstrated that the overall pooled prevalence was 9% for CEAP 0, 26% for CEAP 1, 19% for CEAP 2, 8% for CEAP 3, 4% for CEAP 4, 1% for CEAP 5, and 0.4% for CEAP 6. 6
In addition to clinical changes, patients often experience functional changes. 7 Pain and edema, typically perimalleolar, can trigger the main modifications in functionality. 8 One of the main changes is in range of motion (ROM), with a reduction in ROM detected in both dorsiflexion and plantar flexion in patients with CVD without venous ulcers compared to healthy individuals.9–11 In addition, a systematic review with meta-analysis demonstrated a reduction in the strength of the dorsiflexors and plantar flexors from the early stages of CVD. 12 It is possible to identify structural and metabolic abnormalities in the skeletal muscle cells of the calf in this population, 13 which justifies these findings.
Finally, van Uden et al. 14 also identified changes in balance and gait speed. Patients with venous leg ulcers (active or healed) exhibited lower gait speed and a broader base of support compared to healthy individuals, possibly due to instability or discomfort, which may reduce muscle activity and impair venous blood flow. The slower walking speed and broader base of support could be related to decreased overall mobility and fear of falling, creating a vicious cycle that impairs venous circulation. Additionally, the patients exhibited fewer heel rises, indicating reduced muscle endurance. However, the authors compared only patients with venous ulcers and healthy individuals, without establishing the stage at which gait and strength disturbances can be detected. In elderly individuals with CVD, de Moura et al. 11 found that those with CVD had lower gait speed than healthy individuals, highlighting the functional limitations associated with advanced CVD (CEAP 5 and 6). However, only gait speed was evaluated in the analysis.
Therefore, as the disease progresses through its various clinical stages, disturbances in gait movement patterns and changes in the strength parameters of the muscles involved in walking may occur. Analyzing spatiotemporal gait variables in patients with CVD and associating them with plantar flexor torque and peak force is crucial for understanding the functional impairments caused by the disease. Given the key role of the calf muscle pump in venous return, 15 any deficits in strength and gait mechanics could further compromise circulation, exacerbating symptoms and disease progression. Identifying changes in gait patterns, such as stride length and stance time, alongside reductions in plantar flexor strength, may provide insights into early functional decline and help define targeted rehabilitation strategies.
A deeper understanding of these variables could lead to the development of more effective interventions to improve mobility, enhance muscle function, and potentially slow disease progression in patients with CVD. Thus, the present study aimed to compare the movement patterns in different levels of CVD severity during gait, as well as the strength of the plantar flexors, ankle mobility, and performance of daily activities.
Methods
Study design
A cross-sectional observational study was conducted in patients with CVD to assess gait and plantar flexor muscle strength. The present study was conducted in two phases. Phase 1 investigated differences in spatiotemporal gait parameters between healthy individuals and patients with CVD, whereas Phase 2 examined differences in muscle strength, dorsiflexion ROM, and activities of daily living across levels of CVD severity. The research was approved by the local ethics committee (CAAE 31695520.5.0000.5108), and the study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. All patients were evaluated in the Laboratório de Análise do Movimento (LAM) of Universidade Federal dos Vales do Jequitinhonha e Mucuri (UFVJM) from June 2023 to 2024. Patients were informed of the study’s purpose and signed a consent form to participate.
Patients with CVD were consecutively recruited from a specialized outpatient vascular clinic. All patients who met the predefined inclusion criteria underwent thorough evaluation through anamnesis and physical examination and were invited to participate in the study. The most affected limb was defined as the one with the greater symptom burden, as reported by the patient, and confirmed by duplex ultrasonography findings indicating more significant venous reflux or obstruction. In cases where both limbs were affected, the limb with the more severe duplex findings was selected for analysis. Subjects aged between 50 and 80 years and with a medical diagnosis and signs or symptoms of CVD were included. Patients with musculoskeletal or neurological limitations, or any other condition that affected gait or other evaluation procedures in the study, were excluded. Healthy subjects were selected from the community, had normal Doppler ultrasound, had no comorbidities affecting gait, and were within the same age range.
The sample calculation was performed using the Sigma Stat 9.0 and with the results reported by the study by van Uden et al. 14 Considering the difference in the Stance phase between healthy subjects and patients with CVD of 3.23, a standard deviation of 1.89, alpha error of 5%, and statistical power of 0.80, a minimum of 18 participants was obtained for three groups (6 per group).
In the present study, participants were classified according to the CEAP system. For analytical purposes and to facilitate interpretation of the results, CEAP classes were grouped into three categories: CEAP 1, CEAP 2–3, and CEAP 4–6, which are referred to in the manuscript as mild, moderate, and severe stages, respectively. This subdivision was adopted solely to simplify group comparisons and does not imply a redefinition of current nosological terminology.
Procedures
Gait analysis
The gait analysis was conducted in a Tridimensional Motion Capture Laboratory (Figure 1). Data during walking were recorded using a system of 9 Oqus 3+/5+ cameras at a sampling rate of 200 Hz (Qualisys Medical AB, Sweden). Tridimensional Motion Capture Laboratory, where the gait analysis was conducted.
A scale and a measuring tape were used to measure body mass and height, respectively. The same experienced examiner assessed body mass and height. Passive retroreflective markers were placed on the volunteers (Figure 2). All segments were modeled using the Calibrated Anatomical System Technique.
16
Initially, a static test was performed with the participants. Before data collection, participants walked for approximately 1 minute to familiarize themselves with the laboratory setup. Then, seven walking trials were recorded at a self-selected speed on a 12-m walkway. Placement of fourteen-mm passive retroreflective markers on the right lower limb, with anatomical markers on the femur, malleolus, and foot, and clusters on the shank.
Fourteen-millimeter passive retroreflective markers were placed on the shank and foot of the right lower limb. Specifically, anatomical markers were positioned on the medial and lateral epicondyles of the femur and the medial and lateral malleolus. For the foot, markers were attached over the base of the 5th metatarsal base and the 1st and 5th metatarsal heads. 17 In addition, clusters of four non-collinear markers were attached to the shank.
Kinematic data were processed using Visual 3D software (version 6, C-motion, USA). Marker trajectories were low-pass filtered using a 4th-order Butterworth filter at 6 Hz. 18 The data were time-normalized to 101 points within the gait cycle, i.e., from heel contact to the next heel contact of the same foot. 19
Nine spatiotemporal variables were extracted, including gait speed, stride length (distance from the initial contact of one foot to the next initial contact of the same foot), strides per minute, step length (distance from the initial contact of one foot to the initial contact of the contralateral foot), steps per minute, cycle time (time to complete one gait cycle with the affected leg), double support time (both feet in contact with the ground), time in stance phase (time of affected leg in stance phase), and time in swing phase of affected leg.
Portable dynamometry – Microfet2
To assess the plantar flexion strength of the affected limb, the individual was placed in a prone position on a stretcher with the lower limbs (feet) extending beyond the edge against the wall. The Microfet2 was positioned on the plantar surface of the foot. 20 Each procedure was performed four times, with the first trial serving only for movement familiarization, during which the peak force was not considered valid; the measurements became valid from the second trial onwards. The command was given to the individual, followed by verbal encouragement from the evaluator: “1,2,3 go… force, force, force.” The variables of interest were the average of the three valid measurements.
Weight-Bearing Lunge Test
Ankle dorsiflexion range of motion was assessed using the Weight-Bearing Lunge test (WBLT). Participants were positioned standing, facing a wall, with the limb to be tested anteriorly and the heel firmly in contact with the floor. They were instructed to move the trunk and the knee of the tested limb forward toward the wall until the knee touched the surface, while keeping the heel in contact with the ground. The contralateral limb was positioned behind the body to assist with balance, and participants were allowed to support themselves on the wall if necessary, 21 lightly.
Whenever the knee contacted the wall without heel lift, the foot was progressively moved backward in small increments until the knee just barely touched the wall, with the heel still in firm contact with the floor, thereby positioning the ankle joint in maximal weight-bearing dorsiflexion. The angle formed in this dorsiflexed position is measured, with the result expressed in degrees. The procedure was conducted by a trained researcher following a standardized protocol, and the highest value obtained from valid trials was used for analysis. 21
Human Activity Profile (HAP)
Physical activity level and performance in daily activities were assessed using the Human Activity Profile (HAP), a 94-item questionnaire validated for patients with CVD, 22 which ranks daily activities according to their energy demand. A trained researcher administered the instrument in an interviewer-based format, and participants classified each activity as “I never did this,” “I stopped doing this,” or “I still do this.” The total HAP score was considered the primary measure of habitual physical activity. 23
Statistical analysis
Statistical analysis was performed using SPSS software version 22.0 (SPSS Inc., Chicago, IL, USA). The Kolmogorov-Smirnov test was used to analyze the distribution of variables. Descriptive variables were presented as mean and standard deviation, median and interquartile range, or absolute number and percentage, as appropriate.
The values obtained were compared across healthy subjects and patients with different disease severity levels. Differences in the evaluated variables were assessed using ANOVA or the Kruskal-Wallis test, as appropriate. When global differences were detected, post hoc comparisons between disease severity levels were performed using the independent-samples t-test or the Mann-Whitney test, with Bonferroni correction to adjust for multiple comparisons. A significance level of 5% was adopted.
Results
Clinical and spatiotemporal gait parameters in healthy individuals and patients with chronic venous disease stratified by severity.
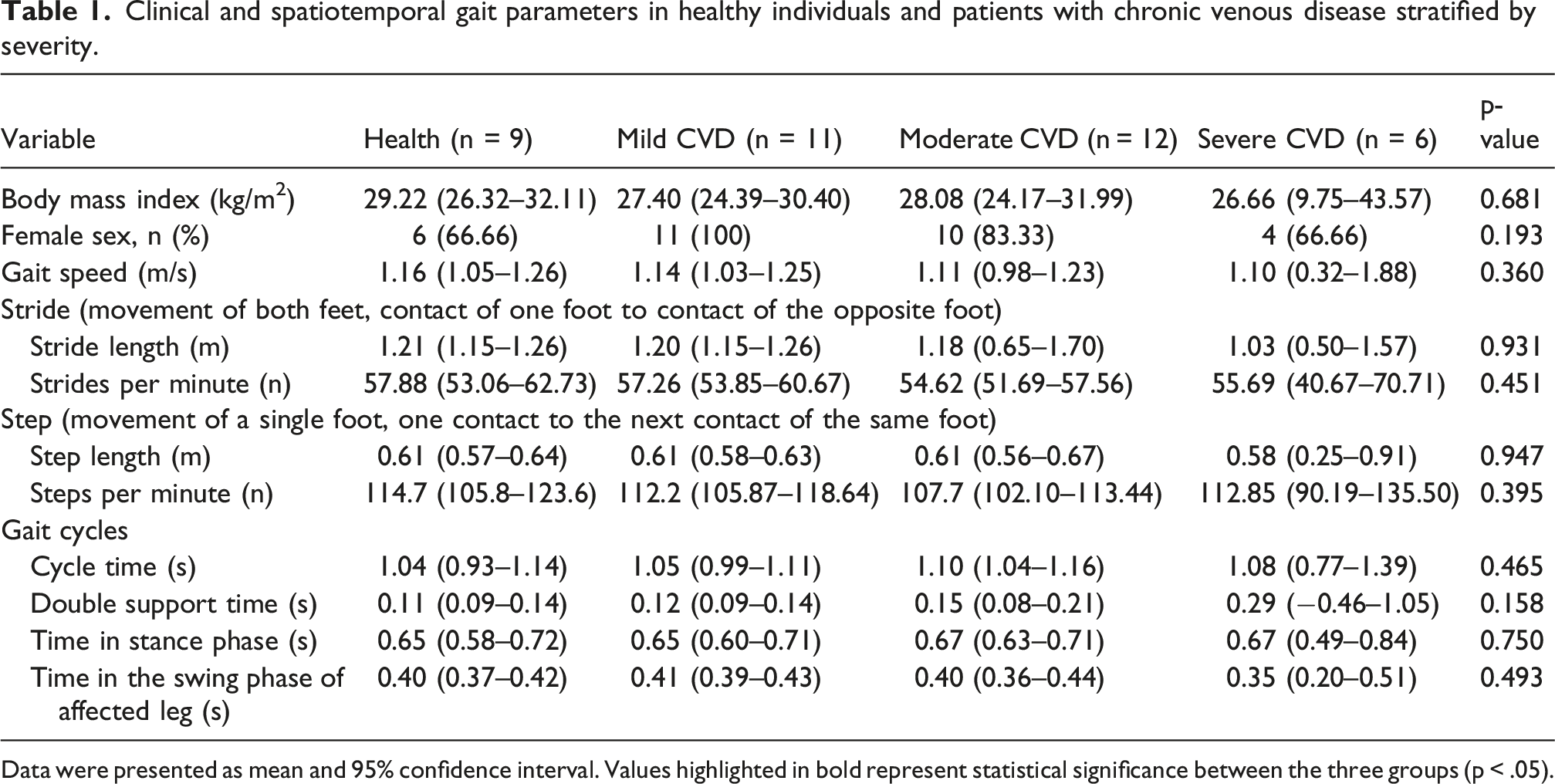
Data were presented as mean and 95% confidence interval. Values highlighted in bold represent statistical significance between the three groups (p < .05).
Differences in plantar flexor strength and torque in the sample stratified by the severity of CVD.
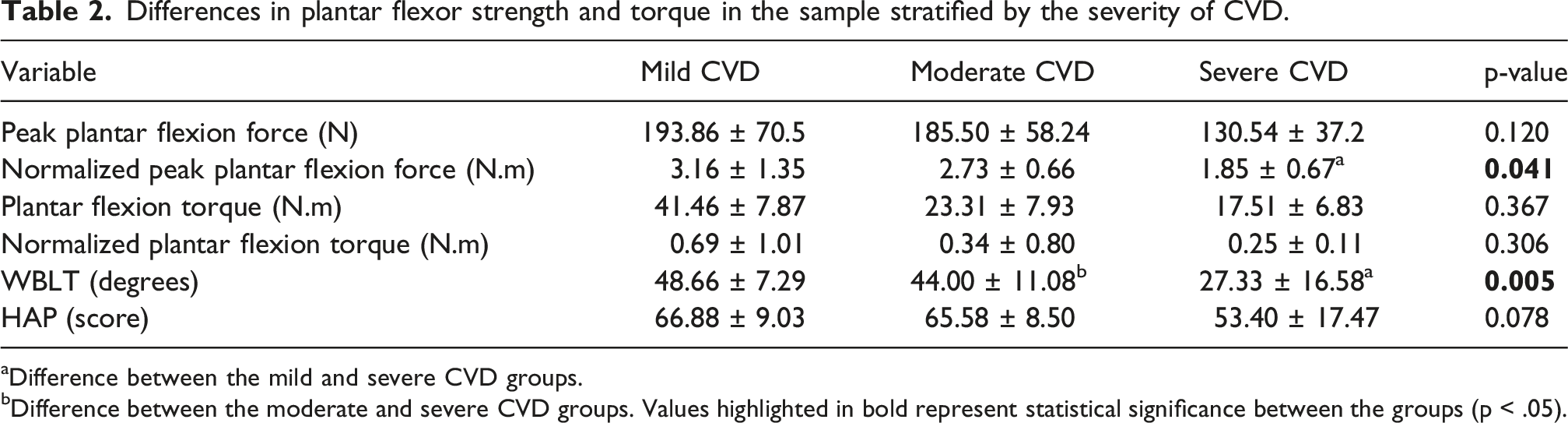
aDifference between the mild and severe CVD groups.
bDifference between the moderate and severe CVD groups. Values highlighted in bold represent statistical significance between the groups (p < .05).
For the WBLT, CEAP classification showed a statistically significant effect (p = .005). Bonferroni-adjusted pairwise comparisons revealed significant differences between the mild and severe CVD groups (p = .005) and between the moderate and severe CVD groups (p = .023). In contrast, no significant difference was observed between the mild and moderate CVD groups. The HAP was not different among the CEAP class (p = .078).
Discussion
This study investigated the impact of CVD severity on gait, muscle strength, and ankle mobility. The main findings indicate that spatiotemporal gait parameters did not differ between groups, whereas plantar flexor strength (when normalized) and ankle dorsiflexion range of motion were significantly reduced with increasing disease severity. These results suggest that impairments in muscle function and joint mobility may emerge before detectable changes in global gait performance, indicating that early functional deficits in CVD may not be captured by conventional gait parameters.
Although no differences in spatiotemporal gait parameters were observed across groups, this finding warrants careful interpretation. Gait is a complex, highly adaptable motor task that is often preserved through compensatory mechanisms despite underlying neuromuscular impairments. 24 It is possible that patients with CVD maintain stable gait patterns despite reductions in muscle strength and joint mobility, particularly at a self-selected walking speed. Additionally, the relatively small sample size in the severe group and the use of global spatiotemporal variables may have limited sensitivity to detect subtle alterations. Taken together, these observations suggest that spatiotemporal gait analysis alone may be insufficient to detect early functional decline in CVD, and that its use as a primary outcome in this population warrants careful reconsideration.
Reduced normalized plantar flexor strength and ankle dorsiflexion ROM, with increasing CVD severity, indicate progressive musculoskeletal impairment consistent with the underlying venous pathophysiology. 25 Furthermore, chronic venous hypertension induces structural and metabolic alterations in the calf muscles, such as fibrosis, capillary rarefaction, and reduced oxidative capacity,26,27 while periarticular fibrosis and persistent edema may mechanically restrict ankle dorsiflexion, particularly in advanced CEAP stages. 28 These factors interact to impair the calf muscle pump, reducing venous return and potentially sustaining venous hypertension.26,28 These findings align with prior evidence demonstrating deficits in muscle strength and ankle mobility across the CVD spectrum, 25 but refine current understanding by showing that such impairments can occur independently of detectable gait changes. Consequently, musculoskeletal dysfunction should be considered a central component of CVD progression rather than a secondary manifestation, and plantar flexor strength and ankle mobility should be recognized as relevant targets for assessment and rehabilitation, even in the absence of overt gait alterations.25,26
Moreover, the absence of gait alterations in the present study contrasts with findings from van Uden et al., 14 who reported reduced gait speed and altered support patterns in patients with venous ulcers. This discrepancy likely reflects differences in disease severity, as their sample was restricted to advanced stages (CEAP 5–6), whereas severe cases were underrepresented in the present cohort. Importantly, when patients were analyzed across the CEAP spectrum, gait parameters remained intact despite reductions in plantar flexor strength and ankle dorsiflexion range of motion. This suggests that locomotor alterations may emerge only later in the disease course, whereas musculoskeletal impairments occur earlier. Together, these findings indicate a stage-dependent pattern in which musculoskeletal deficits precede detectable gait alterations, helping reconcile differences across studies and reinforcing that preserved gait does not necessarily reflect preserved function in CVD.
Several limitations of this study should be acknowledged. The relatively small sample size, particularly in the severe CVD group, may have reduced statistical power and contributed to the absence of significant differences in variables with greater variability, such as gait speed and HAP score, despite clinically relevant trends. Additionally, gait was assessed at a self-selected speed under controlled laboratory conditions, which may not reflect the challenges of real-world environments and could underestimate the compensatory demands required to maintain performance. Despite these limitations, the study presents important methodological strengths. The integrated assessment of gait biomechanics, plantar flexor strength, ankle mobility, and functional performance provides a comprehensive functional profile that has not been previously explored across CEAP subgroups. Moreover, the use of objective, instrumented measures, three-dimensional motion capture, handheld dynamometry, and the WBLT enhances measurement precision and reduces potential bias. Finally, stratifying participants across the full spectrum of CEAP classification represents a methodological advancement over prior studies that focused primarily on the extreme stages of the disease.
From a clinical perspective, these findings underscore the importance of early assessment and intervention targeting plantar flexor strength and ankle mobility in patients with CVD, even when gait parameters remain within normal limits. The presence of musculoskeletal impairments before observable changes in global gait performance suggests that rehabilitation strategies focused on calf muscle function and joint mobility may play a key role in preserving functional capacity and potentially slowing disease progression. From a scientific standpoint, the results indicate that conventional spatiotemporal gait parameters may lack sensitivity to detect early functional changes in this population, reinforcing the need for more specific and sensitive assessment tools. Future research should explore longitudinal designs and incorporate more comprehensive biomechanical and neuromuscular analyses to better understand the progression of functional impairments across different stages of CVD.
Conclusion
CVD severity was associated with reduced plantar flexor strength and ankle dorsiflexion range of motion, while spatiotemporal gait parameters remained unchanged. These findings suggest that musculoskeletal impairments may precede detectable gait alterations, highlighting the importance of early assessment and targeted rehabilitation strategies in this population.
Footnotes
Acknowledgments
The authors would like to thank the Laboratório de Análise do Movimento (LAM) of Universidade Federal dos Vales do Jequitinhonha e Mucuri (UFVJM).
Ethical considerations
The study was approved by the institutional ethics committee, and all participants provided written informed consent prior to enrollment (protocol CAAE 31695520.5.0000.5108).
Author contributions
Conception and design: VMC, RGTF, HSC; Analysis and interpretation: PHSF, VAM, ACRL; Data collection: NRG, MSR, CMS, YFE, DSLS, SFFO; Writing the article: VMC; Critical revision of the article: GMF, ARSP, KLSS; Final approval of the article: RGTF, HSC; Statistical analysis: LFFO, MRA, WTS; Obtained funding: None. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: VMC was supported by an MSc. Studentship from the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES). This work was partially funded by Fundação de Amparo à Pesquisa do Estado de Minas Gerais (APQ-04955-23).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Guarantor
Dr Henrique Silveira Costa is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.