
Abstract
Introduction
To date, there are limited descriptive data on the ultrasonographic characteristics of reticular and perforator veins associated with telangiectasias of the thigh.
Objectives
Evaluate the prevalence, anatomic correlations of reticular and perforator veins associated with lateral thigh telangiectasias.
Methods
This was a cohort study performed between June and December of 2014. Twenty-four female patients (43 limbs) with telangiectasias of the lateral thigh were evaluated by duplex ultrasound. Reticular and perforator veins were characterized according to valvular competency, vein diameter and connection with perforator veins at the thigh. Body mass index, current use of oral contraceptive, and history of pregnancy correlation data were also collected. A non-parametric Kruskal-Wallis test and a Student's t-test test were used for analysis.
Results
All 43 limbs had incompetent reticular veins underlying telangiectasias sites. A total of 20 incompetent perforator veins were found to be connected to the reticular veins. Obese and overweight patients had a higher prevalence of incompetent perforator veins and larger reticular veins when compared to those with normal weight (P < 0.05). Lower extremities with telangiectasias had a higher frequency of total perforator veins (n = 33) and incompetent perforator veins (n = 16) than extremities without telangiectasias (p = 0.001).
Conclusion
Lateral thigh telangiectasias were associated with both incompetent reticular and perforator veins. Obese and overweight patients were especially affected.
Introduction
Lower extremity telangiectasia affects millions of people worldwide, causing significant cosmetic embarrassment, and ultimately leading to the search for medical care. 1 Although sclerotherapy is considered effective, its etiology and pathogenesis is still unclear. 2 Weiss and Weiss demonstrated a possible association between telangiectasias and insufficient reticular veins. 3 Although some reports suggested the role of insufficient reticular and perforator veins, especially associated with telangiectasias refractory to treatment,4,5 there were limited descriptive data on the ultrasonographic characteristics of the associated reticular and perforator veins of the thigh. The aim of this study was to evaluate the prevalence, anatomic correlations and ultrasonographic characteristics of reticular and perforator veins associated with lateral thigh telangiectasias.
Methods
A cohort study was conducted between June and December of 2014. Twenty-four asymptomatic patients (43 limbs) with telangiectasia of the lateral thigh were evaluated by duplex ultrasonography with linear transducer of 5–7 MHz (Philips HD 11 XE Ultrasound System, Andover, MA) in standing position. We measured body mass index (BMI), current use of oral contraceptive, and history of pregnancy. All reticular and perforator veins were characterized according to (1) valvular competency defined as the presence or absence of reflux time greater than 0.5 s, (2) vein diameter (mm), and (3) connection with perforator veins at the level of the thigh or leg. A comparison was performed with a group of 20 limbs (14 patients) without telangiectasia.
The study was approved by the Institutional Review Committee, with all participants receiving and signing an informed consent. A non-parametric Kruskal-Wallis test was used for the analysis of anthropometric baseline characteristics, while a Student's t-test test was used for the evaluation of numeric variables. A P value < 0.05 indicated statistical significance.
Results
Perforator vein distribution and competence, reticular vein diameter (mm) in obese and non-obese individuals.
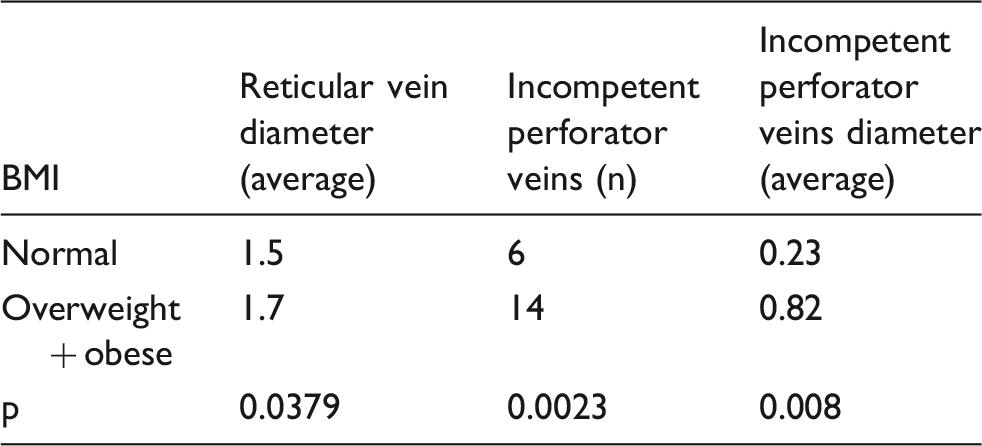
BMI: body mass index.
Conclusion
Lateral thigh telangiectasias were associated with both incompetent reticular and perforator veins. Obese and overweight patients were associated with a higher frequency of incompetent perforator veins, along with reticular veins of larger diameters.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Clinica do Esporte Hospital Ethics Comittee (REC number: 0032014), with all participants receiving and signing an informed consent.
Guarantor
FRS.
Contributorship
FRS: Conception and design of study, analysis and interpretation of results, drafting and reviewing of the manuscript, and final approval of the manuscript. YWC: Analysis and interpretation of results, drafting and reviewing of the manuscript, and final approval of the manuscript. MP: Analysis and interpretation of results and final approval of the manuscript.