
Abstract
Background
There are opinions that telangiectasis and reticular veins are asymptomatic and constitute a cosmetic problem only. However, it has been proven that telangiectasis and reticular veins also affect the quality of life and are symptomatic.
Methods
Ninety consecutive female patients who were admitted to our outpatient clinic and did not have insufficiency in deep, superficial and perforating veins were included in this study. All participants were divided into three groups as the compression group (Group 1), medical treatment group (Group 2), and sclerotherapy group (Group 3). The initial complaint severities of all patients were noted. Except for patient compliance assessment, baseline, 1st month (T1), 3rd month (T2) and 6th month (T3) evaluation records were kept in all three groups.
Results
The study began with a total of 90 patients, 30 patients in each group. The mean ages of Groups 1, 2 and 3 were 39.73 ± 8.51 years, 39.30 ± 8.67 years, and 40.77 ± 9.45 years, respectively. The rates of decrease in pain, itching, restless leg, and muscle cramps were similar among the patient groups at all times (P > 0.05). The rate of reduction in swelling was similar between the groups at T1 and T2 (P > 0.05), while there was a significant difference between the groups at T3 (P = 0.009). The groups significantly differed in terms of appearance concern at all times (P = 0.002 for T1, P < 0.001 for T2 and T3).
Conclusion
We showed that symptoms such as swelling and heaviness in leg can be improved with medical treatment, but the patient's cosmetic satisfaction can increase with sclerotherapy.
Introduction
Chronic venous disease (CVD) is a common disease, detected in 25-50% of the adult population. 1 The visible varicose formations, which can significantly affect the quality of life, are the subject of complaints in half of the patients. This may cause psychological problems in patients as well as loss of workforce. 2 The most common complaints related to the disease are pain in the legs, edema, cramping and cosmetic problems. Insufficiency can affect deep, superficial, or perforating veins.3,4
There are also opinions that telangiectasis and reticular veins are asymptomatic and constitute a cosmetic problem only. However, it has been proven that telangiectasis and reticular veins also affect the quality of life and are symptomatic. 5 The referral of patients to the outpatient clinics with complaints of pain, tingling, edema, and leg restlessness, despite lack of insufficiency in the superficial, deep and perforator veins in doppler ultrasonography (DUSG) examinations, are quite high. In these patients, the symptoms regress with sclerotherapy applied to isolated skin varices. 6 A treatment modality should be used in patients with isolated telangiectasia. Thus, we aimed to compare the effectiveness of sclerotherapy, compression, and medical treatments in patients with isolated telangiectasis in our prospective randomized study.
Methods
Ninety consecutive female patients who were admitted to our outpatient clinic and did not have sufficiency in deep, superficial (great and small saphenous vein) and perforating veins were included in this study. Ethics committee approval was obtained before starting the study, which was conducted per the Helsinki Declaration criteria. The study procedures were explained by interviewing the patients one by one, their signed informed consents were obtained, and telephone numbers were recorded. Patients with comorbid diseases which may cause extremity symptoms, hypertension, chronic diseases such as renal failure and diabetes mellitus, muscle diseases, patients under the age of 20 years, those indicating that they cannot comply with 6-month follow-up period and those with a body mass index (BMI) of >30 kg/m2 were excluded.
Study design
The study was a randomized prospective clinical trial. Participants were randomly assigned 1:1:1 to the compression, medical therapy, and sclerotherapy group (Figure 1). Block randomization according to the admission date to the outpatient clinic. An independent statistician generated the allocation sequence, and the independent investigator assigned the participants to treatments in chronological order as the participants enrolled. Data were analyzed by an independent statistical expert.
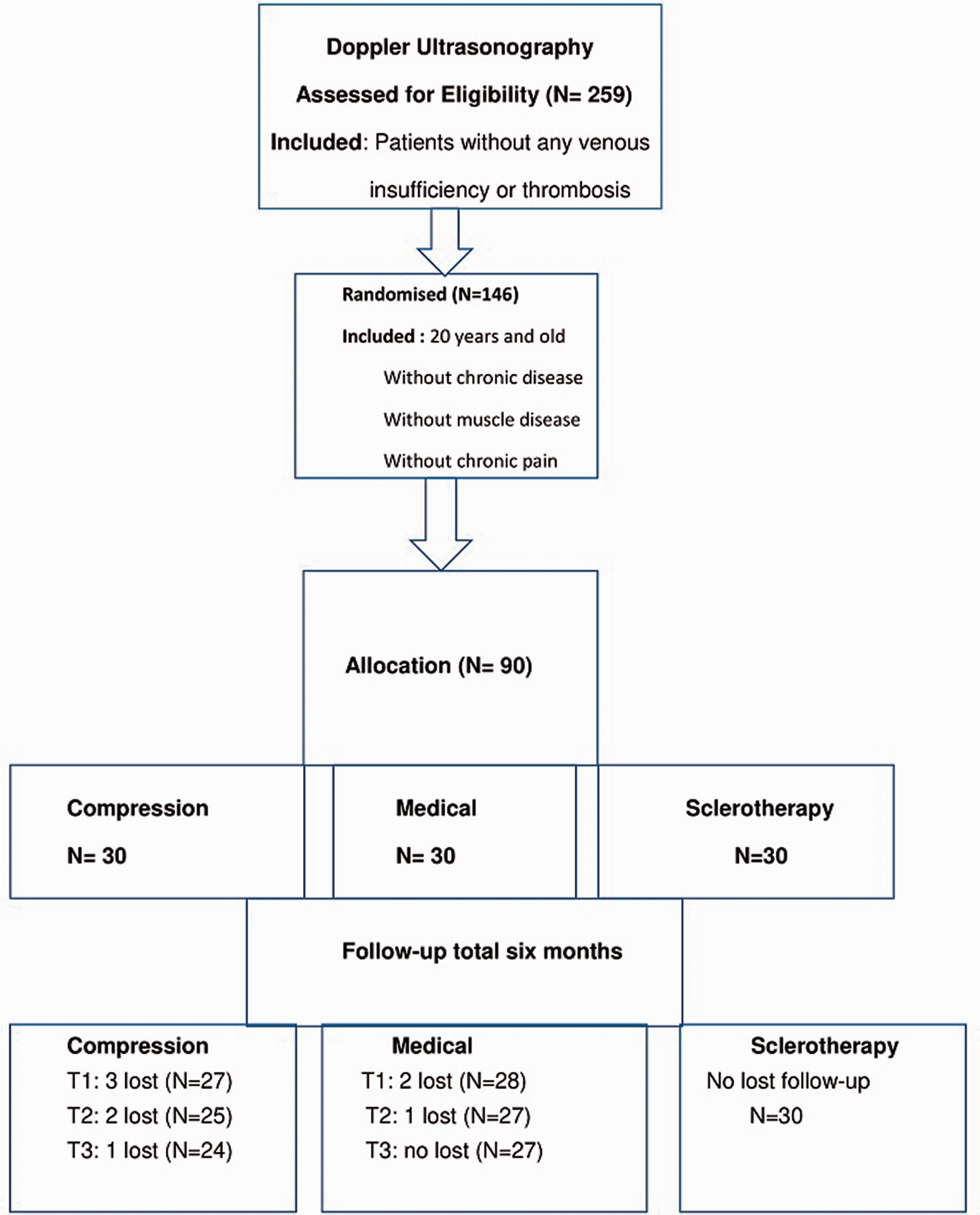
CONSORT diagram showing flow through the study.
Doppler ultrasonography evaluation
All Doppler ultrasonography (DUSG) evaluations were made by the same radiologist, and re-evaluation was performed by us with the DUSG device in the cardiovascular surgery clinic. All patients were assessed in supine position with gray- scale and color DUSG for deep venous thrombosis of the lower extremity and/or thrombosis sequelae in the lumens and walls. During the examination, the cranial segment of the femoral vein, the popliteal vein, the cranial segment of great saphenous vein close to the saphenofemoral junction, along with its caudal segment medial to the knee were investigated for reflux by spectral doppler imaging. Reflux was investigated in the above-mentioned vascular segments during the sudden release of the distal compression. 7
Procedures performed
All participants were divided into three groups as the compression group (Group 1), medical treatment group (Group 2), and sclerotherapy group (Group 3). In the compression group, patients were administered 20-28 mmHg medium-high pressure compression stockings above the knee. They were trained for the use of stockings, which were recommended to be worn during the day and removed at night, and incompliant patients (3 patients) were excluded from the study after evaluating patient compliance during follow-ups. In the medical group, calcium dobesilate was administered in the morning and evening as two oral tablets (1000 mg in total). No other analgesics were given to the patients, and those taking analgesics in all groups were excluded from the study. In the sclerotherapy group, lauromacrogol 0.5% and 1% vials were administered weekly without dilution. The concentration and dose applied were decided according to the vessel size and type. Sclerotherapy application started proximally, primarily from reticular veins, and moved on to distal segments.
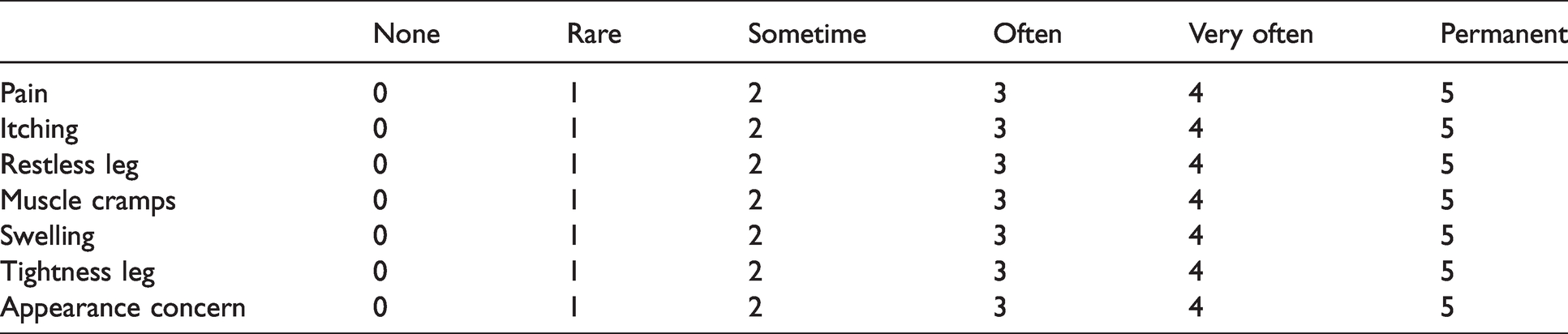
Baseline, 1st month (T1), 3rd month (T2) and 6th month (T3) evaluation records were kept in all three groups. A modified venous clinical severity classification (mVCSC) was created using the venous clinical parameters in the Aberdeen varicose vein scoring 8 and the Bonn vein study. 9 Accordingly complaints of pain, tingling sensation, restless leg, cramp, edema, heaviness in leg and dissatisfaction with the appearance of the legs were graded and recorded (Table 1). The initial complaint severities of all patients were noted. During follow-up, the differences between the groups were investigated for all complaints, based on whether they were in same, better or worse condition than the initial evaluation.
Modified venous clinic severity score.
Statistical analysis
Variables in the study were expressed as mean ± standard deviation, median (minimum-maximum) and n (%). One Way ANOVA and Kruskal Wallis tests were used for comparisons between the groups. The differences of the 1st, 3rd and 6th month scores from baseline were evaluated and the decrease rates were obtained, which were compared between the groups using Fisher-Freeman-Halton, Pearson Chi-Square, and Fisher's Exact tests. Analyses of the study were made in SPSS v.21 (IBM Corp. Released 2012. IBM SPSS Statistics for Windows, Version 21.0. Armonk, NY: IBM Corp.) and p < 0.05 was considered statistically significant.
Results
The study began with a total of 90 patients, 30 patients in each group. The mean ages of Groups 1, 2 and 3 were 39.73 ± 8.51 years, 39.30 ± 8.67 years, and 40.77 ± 9.45 years, respectively, which were similar. The severity of first complaints, such as pain, itching, restless leg, muscle cramps, swelling, heaviness in leg and cosmetic concern were recorded before the treatment, all of which were similar between the three groups (Table 2).
Demographic data and initial complaint levels of the patients.
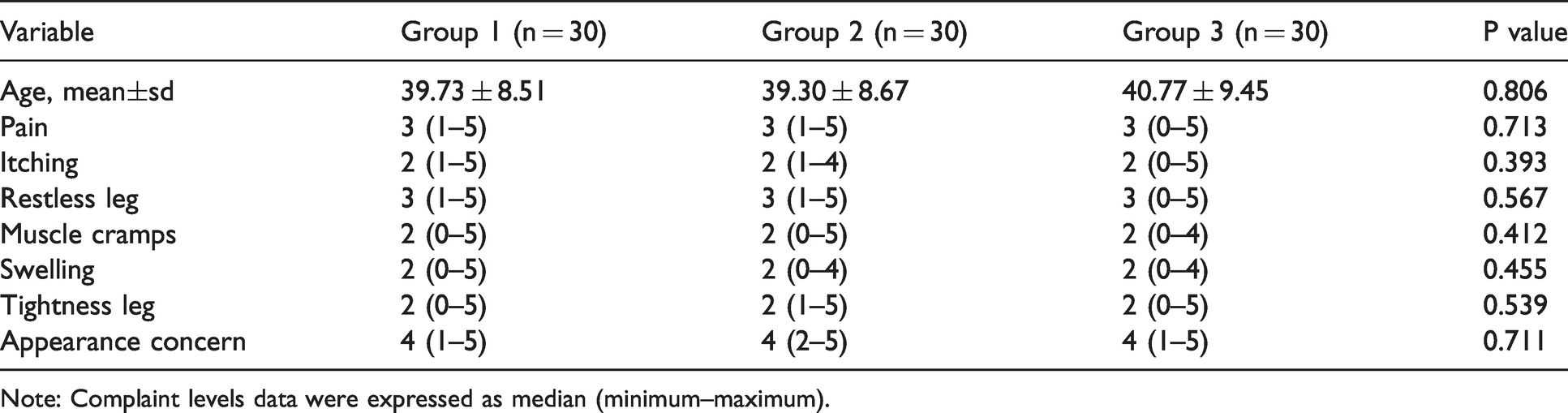
Note: Complaint levels data were expressed as median (minimum–maximum).
Six patients in the compression group (three patients at 1 month, two patients at 2 months, one patient at 3 months) were excluded from the study: Four due to incompliance with compression, one due to communication problems and one due to analgesic use. In the medical therapy group, three patients (two patients at 1 month, one patient at 2 months) were excluded from the study, among which two could not be reached, and one used analgesics. All patients in the sclerotherapy group completed the study. The rates of reduction of first clinical complaints in the patient groups were compared at T1, T2 and T3 (Table 3).
Comparison of decrease rates of patients' clinical complaints according to baseline values.
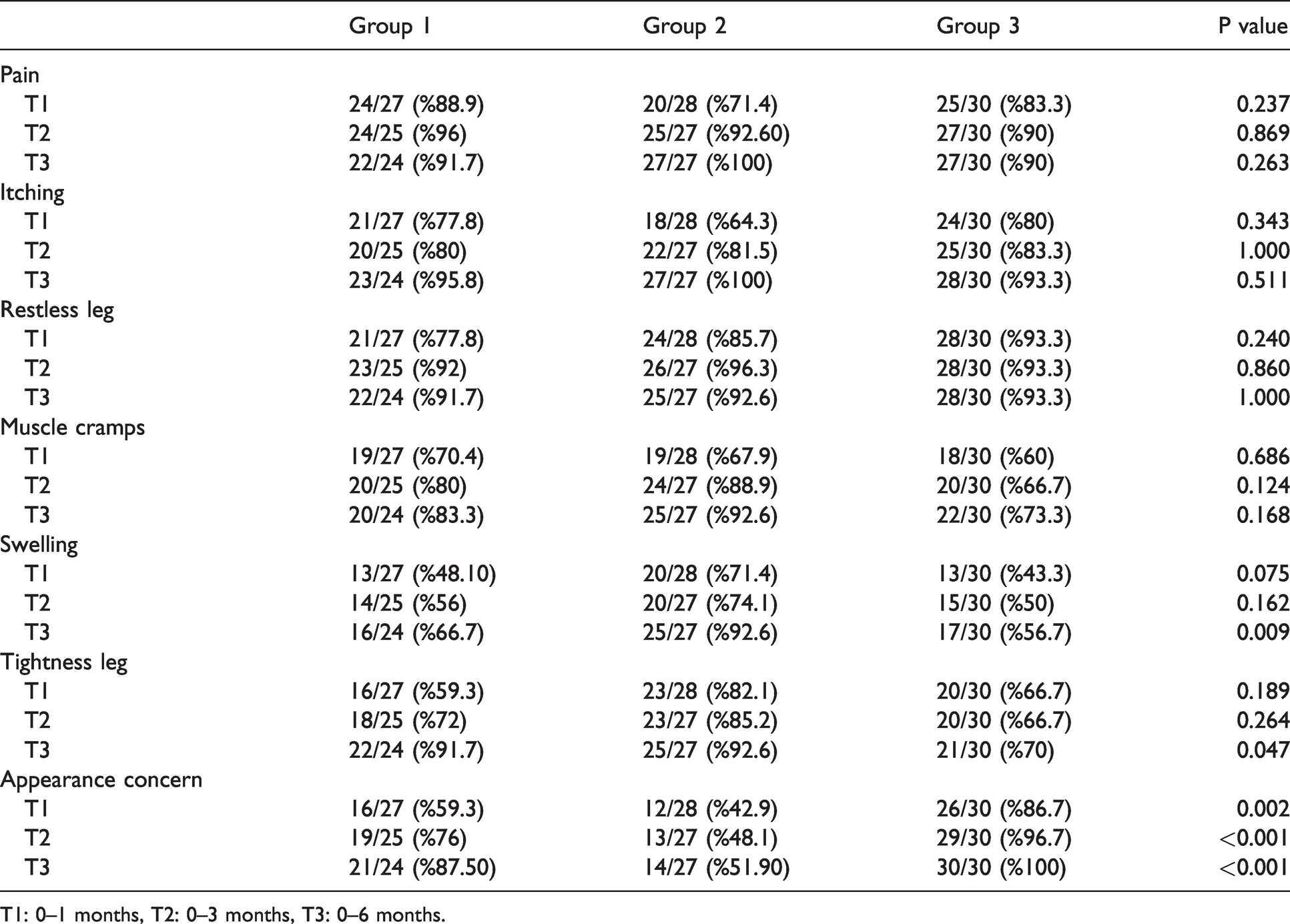
T1: 0–1 months, T2: 0–3 months, T3: 0–6 months.
The rates of decrease in pain, itching, restless leg, and muscle cramps were similar among the patient groups at all times (P > 0.05). The rate of reduction in swelling was similar between the groups at T1 and T2 (P > 0.05), while there was a significant difference between the groups at T3 (P = 0.009). In subgroup analyses, there were significant differences between Groups 1 and 2 (P = 0.033), and Groups 3 and 2 (P = 0.002), while Groups 1 and 3 were similar (P = 0.454). There was no significant difference in T1 and T2 between the groups in terms of heaviness in leg, but the decrease was significant at T3 (P = 0.047). Subgroup analysis revealed that this significant difference occurred between Groups 2 and 3 (P = 0.031) (Table 3).
The groups significantly differed in terms of appearance concern at all times (P = 0.002 for T1, P < 0.001 for T2 and T3). Groups 1 and 2 (P = 0.224) were similar at T1, while Groups 1 and 3 (p = 0.019), and Groups 2 and 3 (P < 0.001) differed. At T2, significant differences were found between Groups 1 and 2 (P = 0.039), 1 and 3 (P = 0.039), and 2 and 3 (P < 0.001). Groups 1 and 2 (P = 0.006), and 2 and 3 (P < 0.001) were different at T3 in subgroup analyses, while Groups 1 and 3 (P = 0.082) were similar (Table 3).
Discussion
Chronic venous disease is an important clinical condition that can affect the quality of life, as well as lead to psychological problems. Although it can affect deep, superficial, and perforating systems, only telangiectatic vein formations can be seen in some patients. It has been shown that isolated telangiectatic veins can cause various symptoms in individuals and should be treated. The main symptoms associated with venous disease are pain, itching, muscle cramps, and swelling. These symptoms may not always be associated with elevated venous pressure. In other words, telangiectatic veins may also cause symptoms in patients without superficial and deep venous insufficiency. These symptoms appear with the release of inflammatory mediators as a result of the interaction of leukocytes with the endothelium. As the inflammatory response increases, macro findings such as venous valve damage may occur. This situation causes an increase in venous pressure and high venous pressure can exacerbate this clinic. 3 Dermal complex reflux (telangiectatic and reticular veins) causes symptoms by the same mechanism. This reflux can be reduced by obliteration with sclerotherapy and compression treatments. Also, medical treatment can reduce reflux with its venoprotective effects. Thus, these symptoms may regress. 10
In this current randomized controlled prospective study, we compared the efficacy of three methods in the treatment of telangiectatic varicose veins for the first time in the literature. We found no difference in treatment results in the 0–6-month range in terms of pain, itching, restless leg, and muscle cramps. There was a significant decrease in swelling in patients who received medical treatment at the 6th month compared to the other two groups. In terms of heaviness in leg, there was a significant decrease only in the medical group compared to the sclerotherapy group at the 6th month. Cosmetic concern reduction was higher in the sclerotherapy group at all times. We can state that symptoms such as swelling and heaviness in leg can be improved with medical treatment, but the patient's cosmetic satisfaction can increase with sclerotherapy.
A prospective randomized controlled study by Schul et al. (most similar to our work) compared medium pressure (20-30 mmHg) compression stockings (N = 29) and sclerotherapy (N = 29) in patients with isolated reticular/telangiectatic veins. The clinical conditions of the patients at the beginning and during their follow-up were evaluated with the modified Aberdeen Varicose Vein Questionnaire and the patients were followed up for one year. At the end of the study, the authors found that compression therapy improved patients' itching, cramping, and restless leg symptoms. They also found that sclerotherapy applied to telangiectatic veins is more effective for pain complaints. In this study, it was emphasized that especially reticular and telangiectatic veins do not constitute a cosmetic problem only, rather, they should be treated effectively. 10 Unlike this study, we compared three treatment methods. Our follow-up period was six months. We also believe that isolated telangiectatic veins should also be treated.
In a prospective study conducted by Kanter, the effectiveness of sclerotherapy treatment in patients with restless leg syndrome was investigated on 113 patients, among which 98% who underwent sclerotherapy had regression of their initial symptoms. This rate was 92% in the first year and 72% in the second year, as found by follow ups. At the end of the study, it was emphasized that patients with restless leg syndrome should also be evaluated phlebologically. 11 In our study, one of our treatment options was sclerotherapy. Although there was no statistically significant difference, the clinical improvement in patients who underwent sclerotherapy was better than those who received medical therapy and compression therapy at all follow-up times.
The main treatment options of telangiectatic lower extremity veins, decided by the patients’ complaints, include compression therapy, venoprotective drug therapy and sclerotherapy. Compression therapy, which can be used in all clinical stages of CVD, reduces venous pressure by enabling the lower extremity muscles to pump venous blood effectively, thus, preventing stasis. 12 The main challenge of this treatment is the compliance problems of the patients. 13 In our study, Group 1 completed the study with the least number of patients due to incompliance. Venoprotective drugs, on the other hand, are often used and recommended in patients with venous insufficiency due to their venotonic, anti-inflammatory, and capillary leak-reducing effects. 14 In sclerotherapy, the sclerosing agent is injected intravenously, so the vessel becomes sclerosed due to transmural damage in the endothelia. This method is recommended in the treatment of telangiectatic varices. 15
Clinical benefits can be obtained with the concurrent use of these treatment methods. A multicenter study conducted by Bogachev et al. included 1150 patients, 93% of whom were females, at C1s stage according to the CEAP classification. In this study, clinical efficacy of venoprotective drug treatment administered concurrently with sclerotherapy was investigated with visual analog scale (VAS) and quality-of-life (CIVIQ-14) evaluations. In the assessments made one month later, they found that the medical treatment added to the sclerotherapy significantly reduced the complaints. 16 In this study, no information was given on whether the patients had great saphenous vein, small saphenous vein and perforator vein insufficiency, which is a critical point affecting the results. Unlike this study, we investigated the effectiveness of three treatment methods, and our patients had isolated telangiectatic veins. In addition, although the number of our patients was sparse, our follow-up period was six months.
Pain, restless leg, and dissatisfaction with appearance are the main symptoms of telangiectatic varicose veins. In our study, we developed a scoring of common complaints related to this disease (Table 1) and recorded the baseline complaints of all patients. The stimulation of subcutaneous nerve endings due to venous dilatation17,18 results in various symptoms occurring in different degrees.
The sparse number of patients and the single center design of the study are its main limitations. Our study needs to be supported by novel studies in larger multi-center patient series, in which various treatment combinations are used.
Conclusion
Venous insufficiency is a common condition which sometimes manifests with isolated telangiectatic venous structures. In this study, we investigated the efficacy of three treatment methods in the treatment of isolated telangiectasia and reticular veins and showed that they should be treated. These three methods can also be combined.
Footnotes
Acknowledgement
None.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the local ethic committee (Approval number: KAEK-152012)
Guarantor
None.
Contributorship
UA: design and execution of the methodology described in this article, manuscript writing and final editing of the paper. ME: literature research, manuscript writing and final editing of the paper. TT: literature research, manuscript writing and final editing of the paper. YA: literature research, manuscript writing and final editing of the paper.