
Abstract
Objective
To assess the potential of multidetector-row computed tomography imaging and its reformations in the evaluation of the superior and inferior vena cava normal anatomy and their anatomical variants, and to make a brief review of caval embryogenesis and developmental errors.
Methods
We retrospectively reviewed a total of 1000 whole-body computed tomography scans performed between January 2010 and December 2016 to assess the normal superior and inferior vena cava anatomy and their variants.
Results
The normal superior and inferior vena cava anatomy was found in 88.9% of patients, whereas multiple variants were found, ranging from the superior or inferior vena cava duplication, to the azygos continuation of the inferior vena cava.
Conclusions
Computed tomography is a powerful tool to analyse superior and inferior vena cava anatomical variants. The knowledge and assessment of normal caval anatomy and of its anatomical variants is mandatory in the correct pre-operative planning in surgical and radiological interventions. Knowledge of caval variants is helpful in the differential diagnosis of abdominal or mediastinal masses, to avoid misdiagnosis, as well as in the screening of associated congenital pathologic conditions.
Introduction
Anatomical variants of superior and inferior vena cava are congenital anomalies sustained by an incorrect development of one or more components of the embryonal venous system. These variants, usually asymptomatic, represent an incidental finding in patients undergoing computed tomography (CT) examination, and can be misdiagnosed as mass-like lesions, leading to an incorrect treatment. Knowledge of those aberrations, some of which can be associated with cardiac anomalies, is mandatory in the planning of surgical and radiological interventions, in order to reduce procedural complications. Especially, the success of mediastinal surgery as well as fashioning renal transplantations is strictly dependent on an adequate pre-operative vascular planning; furthermore, the knowledge of caval anatomy has also consequences on the correct positioning of a central venous catheter or on inferior vena cava filter placement. Therefore, surgeons, interventional radiologists and diagnostic radiologists should be familiar with the full bouquet of common and uncommon caval variants.
Materials and methods
Study design – Study population
We performed a literature search in PubMed using keywords as superior vena cava, inferior vena cava, embryology and anatomical variants. Each abstract found was reviewed to choose the pertinent studies; article references were also used to select all other relevant articles. Studies were defined as pertinent for inclusion if they covered the topic of vena cava embryology and/or of its anatomical variants. The most pertinent studies were included in this analysis, including case reports. We performed an internal CT database search to identify all the patients who underwent a whole-body multi-detector CT (MDCT) in our department between January 2006 and December 2016, irrespective of their disease; we selected CT examinations which had both the unenhanced and portal-venous-enhanced scans. A total of 1000 consecutive MDCT were included and retrospectively reviewed to evaluate the clear visibility of the superior and inferior vena cava. All technically inadequate CT examinations were excluded. For each CT examination, a written informed consent was obtained. The study was waived by our Institutional Review Board and was performed in agreement with the 1990 Declaration of Helsinki and subsequent amendments.
Imaging technique
CT exam acquisition
All CT studies were performed on a 64-channel multidetector-row CT system (Lightspeed VCT XT, GE, USA). The unenhanced scan was obtained from the pulmonary apices to the symphysis pubis with 4 × 2.5 mm slice collimation, a pitch of 6, 2.5 mm slice width and reconstruction interval, a table speed of 15 mm/rotation and a 0.5 s gantry rotation time; the same acquisition volume was obtained for the contrast-enhanced scan, but with 4 × 1 mm collimation, a pitch of 6, 1.25 mm slice width, and 1 mm reconstruction interval, a table speed of 15 mm/rotation, and a 0.5 s gantry rotation time, using 130 mAs and 120 kV.
Contrast medium administration
In all patients, 0.5 gI/kg of iodinate low-osmolar non-ionic contrast medium (Iopromide, 370 mgI/mL, Ultravist; Bayer Healthcare, Germany), followed by 60 mL of saline, were injected into the brachial vein with a power injector at a flow rate of 3 mL/s. Scan delay for portal-venous phase was standardized between 60 and 80 s for each patient, based on our experience.
Image post-processing
MDCT scans were retrospectively evaluated and processed on dedicated workstations (Advantage Workstation 4.1, GE, USA) in order to visualize the vascular structures from every point of view, using 3D reconstructions (maximum-intensity projection (MIP); multiplanar reconstruction (MPR)) in order to enhance the detection of normal anatomy, anatomical variants and pathologies.
Embryogenesis
We reviewed all SVC and IVC configurations, both normal and variant, based on the work of Kellman et al. 1 The final caval venous system derives from the persistence or the regression of multiple sets of veins; among these, the cardinal veins, which drain deoxygenated blood from the embryo, can be identified from the fourth to fifth week of embryonic development: these are divided into anterior cardinal veins (ACVs, draining the cephalic portion of the embryo), posterior cardinal veins (PCVs, draining the rest of the embryo) and common cardinal veins (CCVs, originating from the confluence of the first two and draining in the sinus venosus, which forms part of the right atrium).
Normal development of SVC
The right ACV, the right CCV and the right horn of the sinus venosus normally give birth to the SVC. The right and left ACVs anastomize to form the left brachiocephalic (innominate) vein, whereas the rest of the left ACV regresses (forming the ligament of Marshall), except for a small, terminal portion, that persists as the left superior intercostal vein.
Normal development of IVC
PCVs are dominant until the sixth week, and then regress. During the seventh week, a pair of subcardinal veins (SubCVs) develops, located ventro-medially to the PCVs; anastomosis develops between the right and left SubCVs (intersubcardinal anastomosis), anteriorly to the aorta and between SubCVs and PCVs. In the eighth week, a third pair of veins develops, the supracardinal veins (SupCVs), located dorso-medially to the PCVs, becoming the dominant venous system; anastomosis develop between the right and left SupCVs (intersupracardinal anastomosis), posteriorly to the aorta and between SupCVs and SubCVs (subcardinal-supracardinal anastomosis). SupCVs extend above the diaphragm, forming the azygos and hemiazygos veins, while caudally give birth to the lumbar veins. The right SubCV gives birth to the suprarenal segment of IVC and, anastomizing with the post-hepatic segment of IVC – derived from the right vitelline vein (subcardinal-hepatic anastomosis), gives birth to the hepatic segment of IVC. The renal segment of IVC derives from the right subcardinal–supracardinal anastomosis. The infrarenal segment of IVC derives from the right SupCV, with regression or fusion of the left one; caudally, it anastomizes with the iliac veins derived from the caudal portion of the PCVs. The renal, gonadal and adrenal veins derive from both the SubCVs.
SVC variants
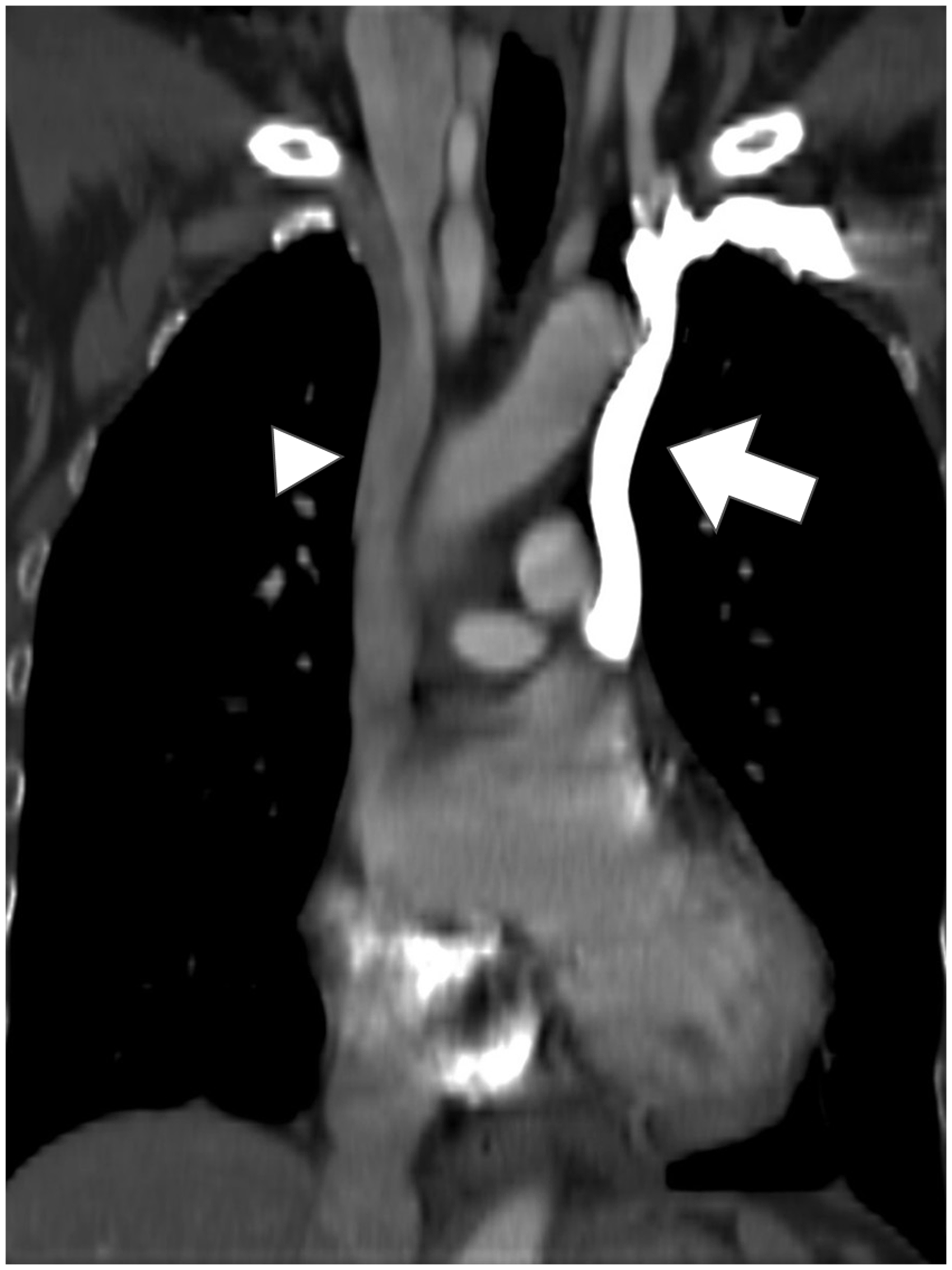
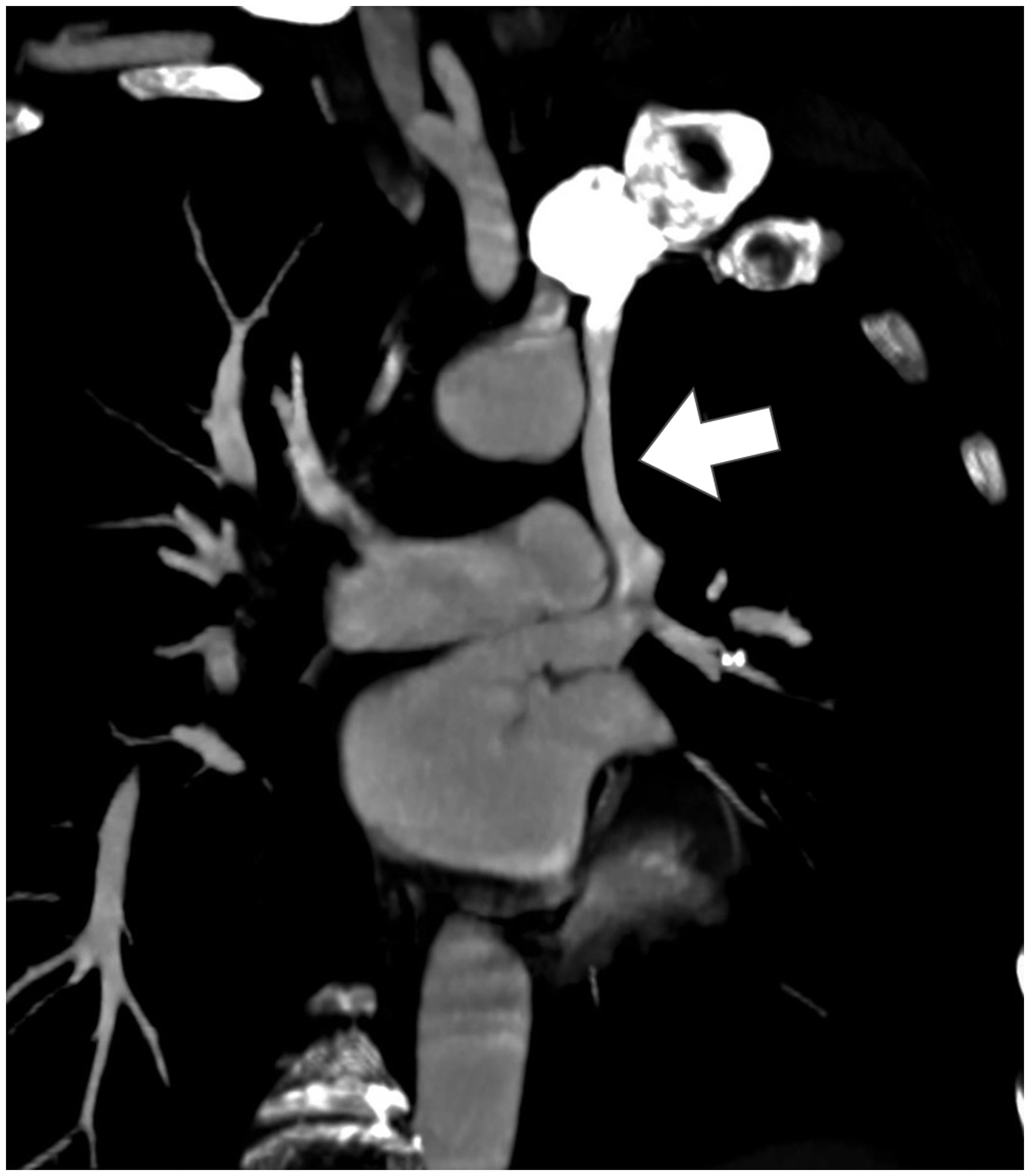
Left-sided SVC1–5 (Figure 1): it origins from the confluence of the left subclavian and jugular veins and travels laterally to the aortic arch. Its presence is due to the persistence of the left ACV, left CCV and the left horn of the sinus venosus. Its prevalence is up to 10% in patients with associated coronary syndromes – an association which increases in case of absence of the right SVC. In 90% of cases, it is associated to the persistence of the right SVC (SVC duplication) (Figure 2). The left SVC can drain into the right atrium via the coronary sinus (92%) or into the left atrium (8%, with a non-clinically significant right-to-left shunt, usually as a part of a developmental complex going under the name of Raghib syndrome)
6
(Figure 3). The anastomosis between the right and left ACVs (left brachiocephalic or innominate-vein) persists in 35% of cases.
Coronal contrast-enhanced CT MPR and MIP projection showing a left-sided SVC. Coronal contrast-enhanced CT MPR and MIP projection showing an SVC duplication; the left-sided SVC (arrow) is more hyperdense than the right-sided IVC (arrowhead) due to the preferential flow during contrast-media injection from the left arm. Coronal-oblique contrast-enhanced CT MPR and MIP projection showing a left-sided SVC draining in the left atrium.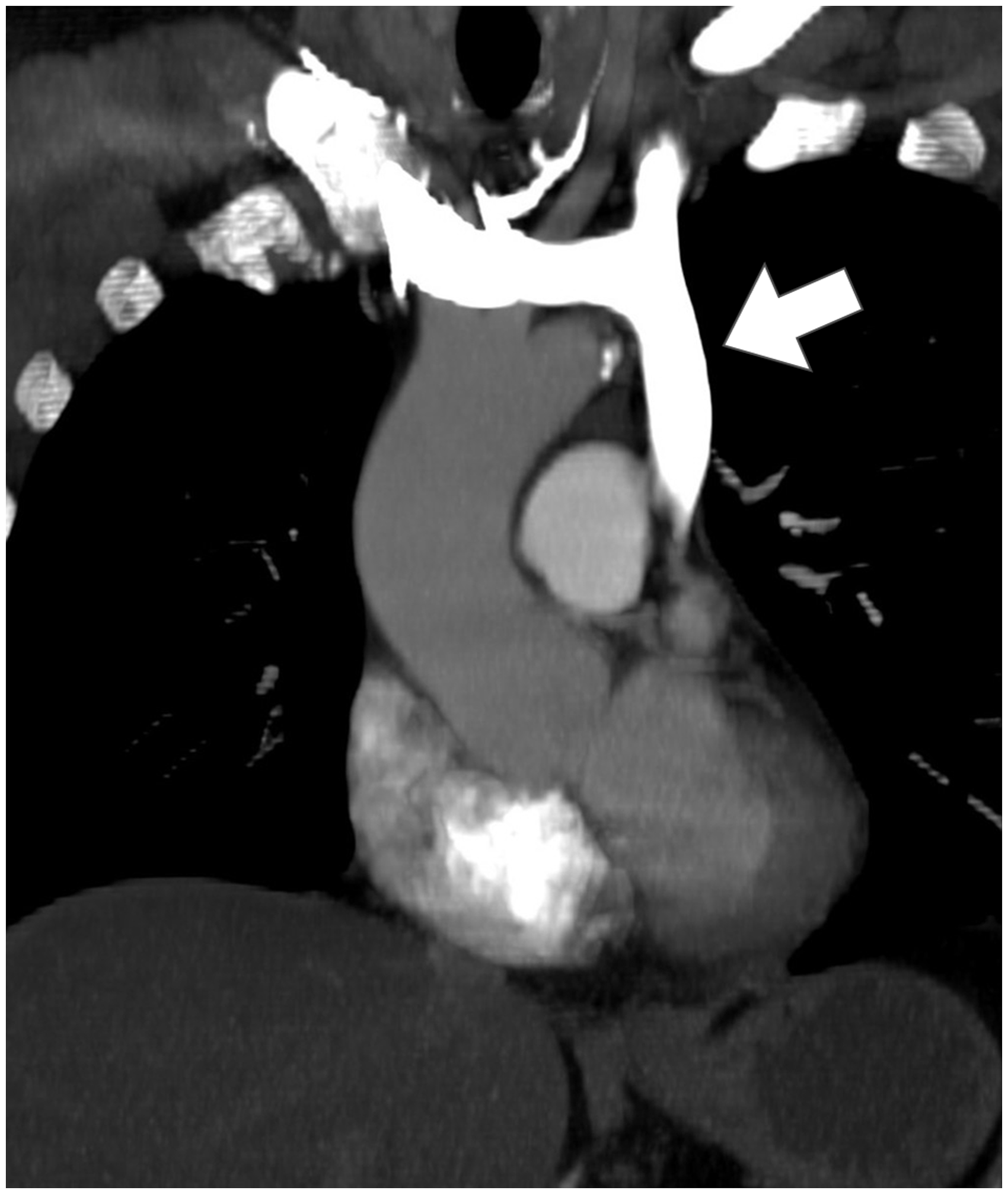
IVC variants7
IVC variants are divided into infra-renal, renal and supra-renal, based on the location of the anomaly.
Infra-renal
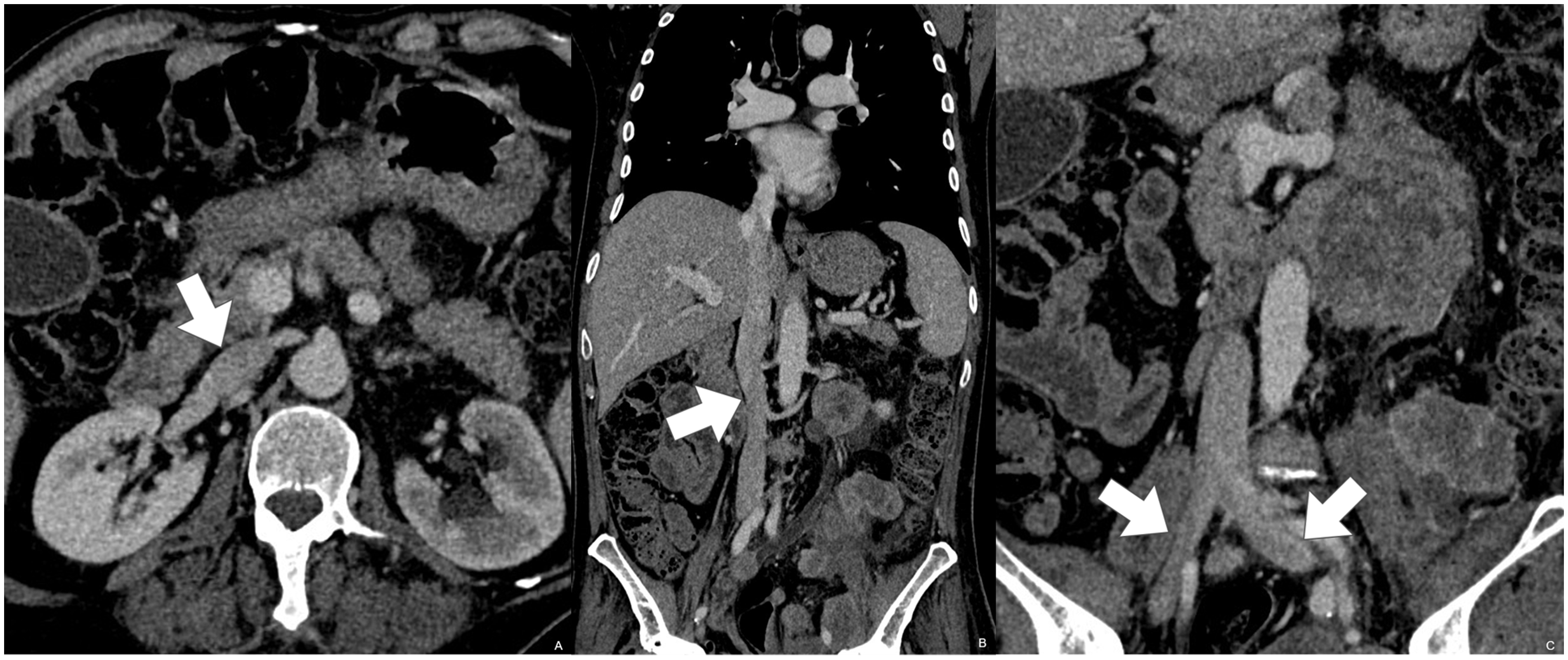
IVC duplication8–11 (Figure 4): it is the result of the persistence of both the right and left SupCVs. It travels left to the abdominal aorta, and typically crosses over anteriorly to join the right IVC, at the level of the left renal vein (LRV) (Figure 5); it can, however, cross posteriorly to the aorta. The calibre of the right and left IVCs can be greatly different. The left IVC usually continues caudally into the left common iliac vein, whereas the right IVC usually continues into the right common iliac vein; anastomosis between the right and left iliac veins are described. The association between the IVC duplication and other congenital anomalies, both vascular (circumaortic venous collar, retroaortic left renal vein, retrocaval ureter, see below) and non-vascular (horseshoe kidney, crossed fused ectopia, pelvi-ureteric junction anomalies) is known.
Axial contrast-enhanced CT showing an IVC duplication, on both sides of the abdominal aorta. Coronal contrast-enhanced CT MPR and MIP projection showing an IVC duplication with the left-sided IVC crossing anteriorly to the abdominal Aorta to join the right-sided IVC.

Left-sided IVC8,9,11–13 (Figure 6): it derives from the persistence of the left SupCV and the regression of the right one. As in the IVC duplication, usually it joins the infrarenal tract of the right IVC at the level of the LRV, anteriorly to the abdominal aorta, even though this anastomosis can happen more caudally and/or posteriorly to the aorta. The left IVC usually bifurcates caudally into the right and left common iliac veins.
Coronal contrast-enhanced CT MPR and MIP projection showing a left-sided IVC which crosses posteriorly to the abdominal aorta to drain in the intrahepatic portion of the IVC.
Retrocaval/circumcaval urether 14 : it is present in 0.07% of population, and is 2.8–4 times more frequent in men. It results from the persistence of the right PCV and the right SupCV regression, which forms the infrarenal segment of the IVC. The ureter usually travels anteriorly to the right SupCV and posteriorly to the right PCV; in this anomaly, the persistent right PCV migrates medially to form the infrarenal segment of the IVC, carrying and dislocating medially the ureter, which can determine various grades of ureteral obstruction and/or urinary tract infections. Usually (99%) this anomaly occurs on the right side.
Renal: The LRV is normally derived from the intersubcardinal anastomosis, which passes anteriorly to the aorta.
Retroaortic LRV10,15–17 (Figure 7): it results from the regression of the intersubcardinal anastomosis and the persistence of the intersupracardinal one. The LRV crosses posteriorly to the aorta, and drains in the IVC at the same level of the right renal vein, but more often caudally.
Axial contrast-enhanced CT showing a retroaortic LRV, which drains in the right-sided IVC.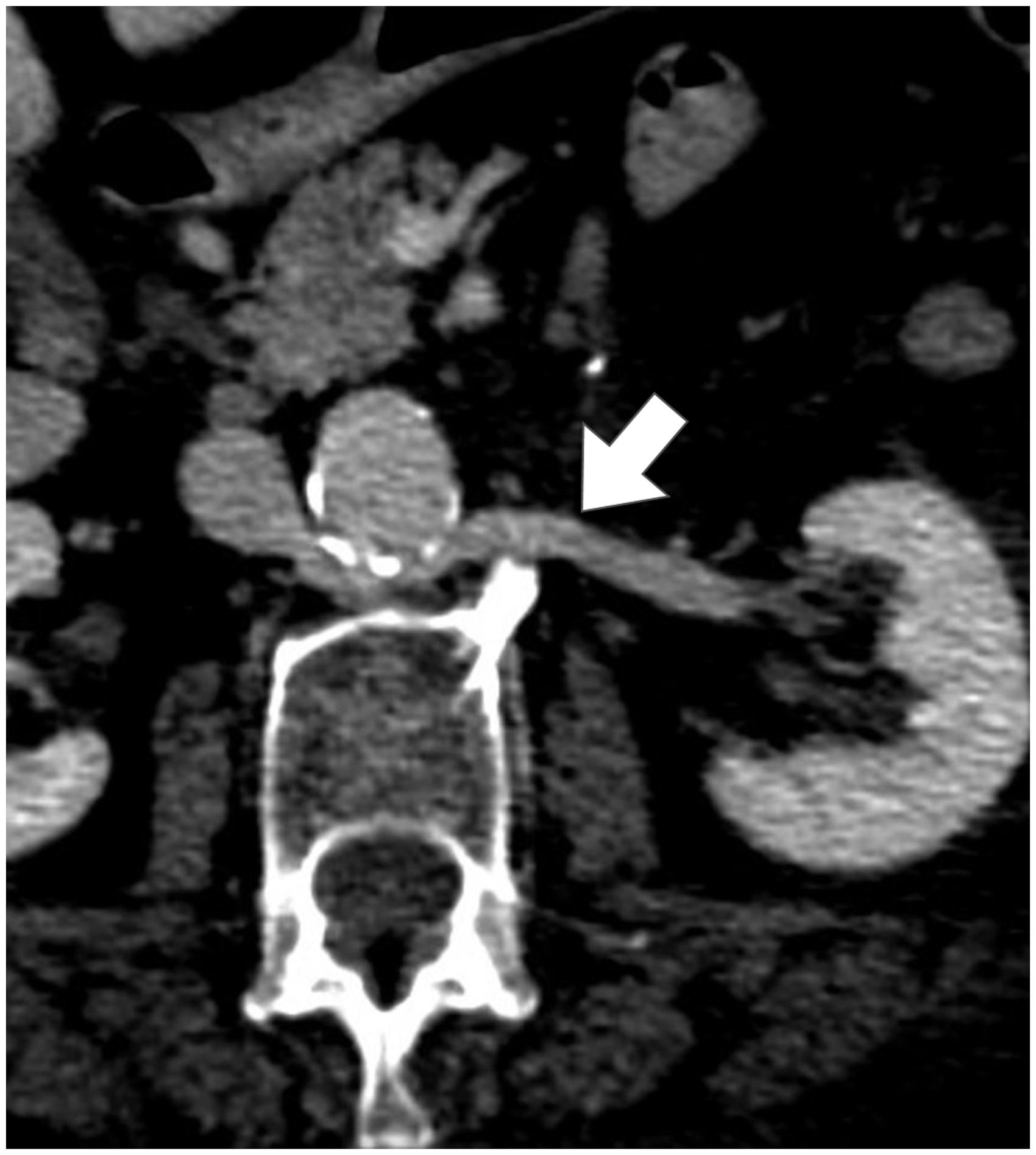
Circumaortic LRV10,15–18 (Figure 8): it is a venous collar which encircles the aorta, with the right and left branches that can cross at the same level of the right renal vein, or caudally. It results from the persistence of the intersubcardinal anastomosis, anteriorly to the aorta, and of the intersupracardinal anastomosis, posteriorly. Usually, the anterior branch drains the left adrenal vein, whereas the posterior branch drains the left gonadal vein.
Axial contrast-enhanced CT MIP reconstruction showing a circumaortic LRV, which drains in the right-sided IVC; the retroaortic vein is identified by the arrowhead.
Supra-renal
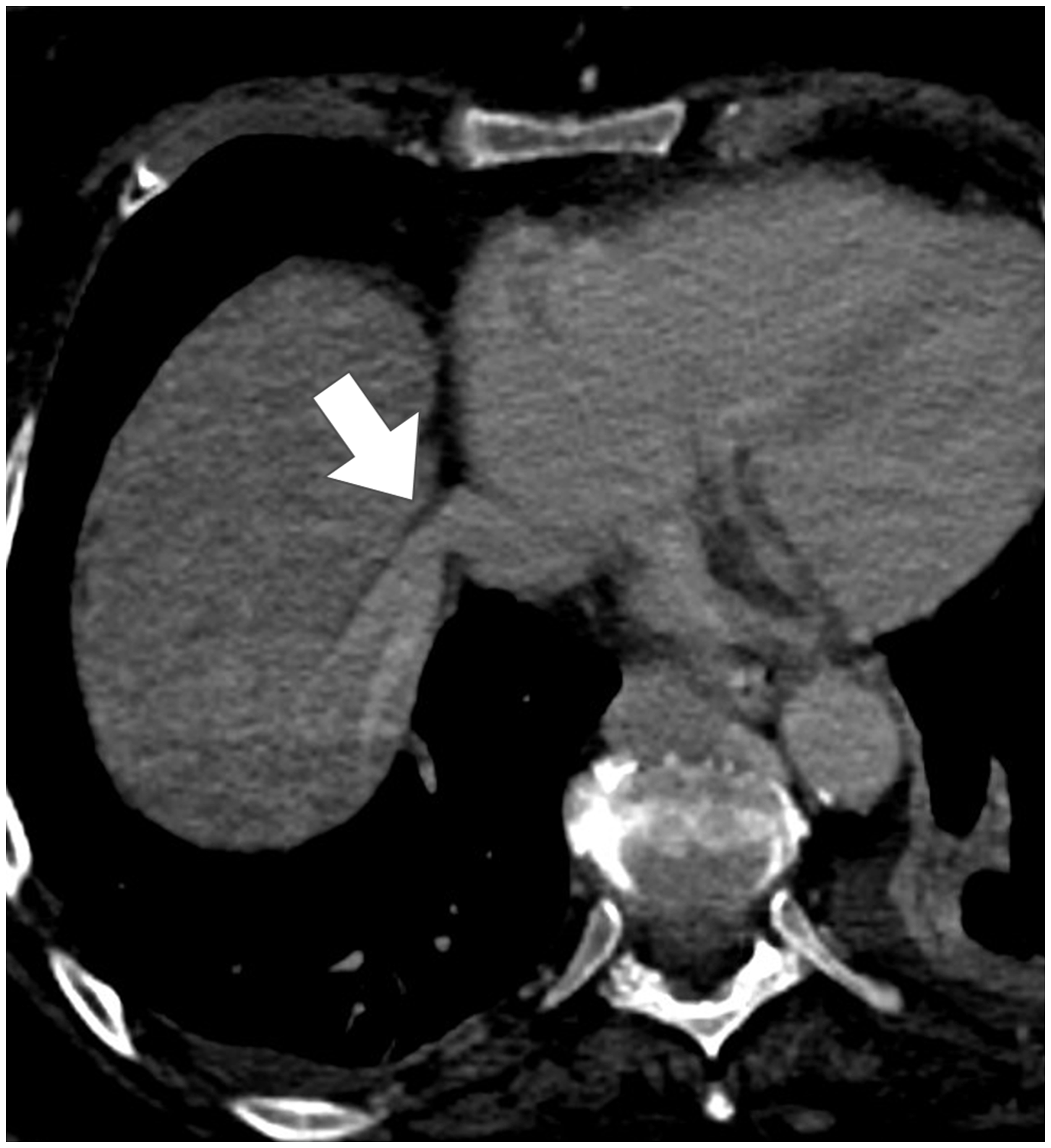
Azygos continuation (AC) of IVC9,10,19 (Figure 9): it is characterized by the absence of the hepatic segment of the IVC, with the blood flow reaching the SVC through the azygos vein. It results from the failure of the formation of the hepatic segment of the IVC (subcardino-hepatic anastomosis) and from the atrophy of the right SubCV. The blood flow is directed into the SupCVs via the subcardinal–supracardinal anastomosis and reaches the SVC through the azygos vein (derived from the right SupCV). The hepatic veins drain directly into the right atrium via the post-hepatic segment of the IVC derived from the right vitelline vein (Figure 10). This anomaly is commonly associated with congenital heart disease, polysplenia and asplenia. Hemiazygos continuation of the IVC can also occur, usually in presence of a left IVC; the hemiazygos vein and the azygos arch are markedly enlarged due to the increased blood flow.
Coronal contrast-enhanced CT MPR and MIP projection showing the AC of the IVC. Axial-oblique contrast-enhanced CT MPR and MIP projection showing the autonomous drainage of the hepatic veins in the right atrium.
All the abovementioned anomalies can be associated to each other, as in the case of the presence of an IVC duplication, an azygos/hemiazygos continuation of the IVC and a retroaortic left (or right) renal vein. In particular, the hemiazygos vein can drain into the azygos vein, can join the coronary sinus via a persistent left SVC, or can drain into the left brachiocephalic vein.
Absence of the entire IVC or of the infrarenal IVC (with preservation of the suprarenal segment)20,21: Absence of the entire IVC (IVC agenesis, aplasia, atresia) is present in 0.005–1% of the population and is due to the failure in the development of the embryonic venous system, or can be determined by an IVC thrombosis in the intrauterine or perinatal period. Absence of the infrarenal segment of IVC is due to the failure in the development of the PCVs and SupCVs. The common iliac veins can also be absent, with the internal and external iliac veins which can join together and drain into the enlarged lumbar veins, conveying the blood flow into the azygos and hemiazygos veins, through collateral paravertebral veins. The suprarenal segment of the IVC is formed by the confluence of the renal veins. Patients may present with symptoms of lower extremity venous insufficiency or idiopathic deep venous thrombosis.
Results
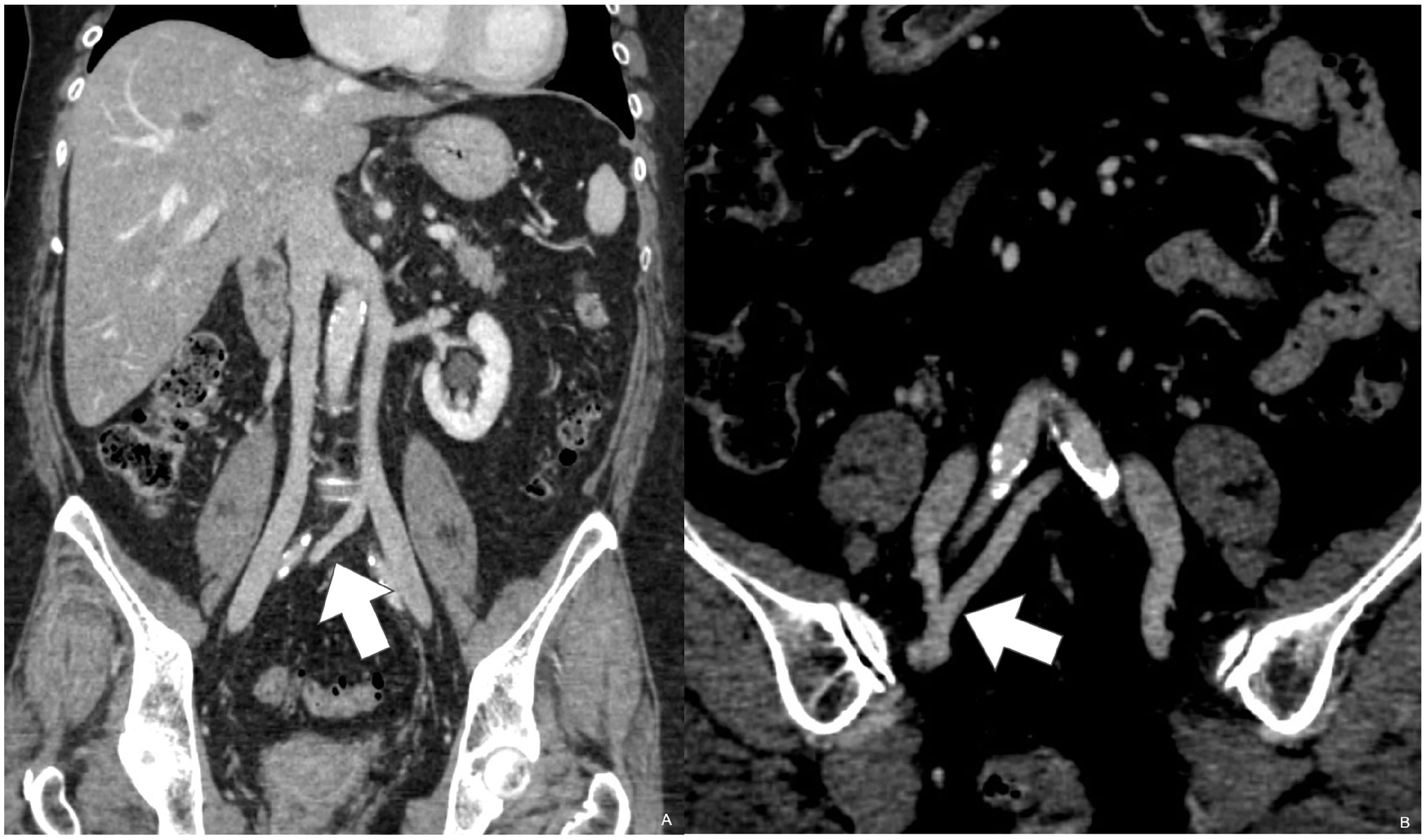
One-hundred MDCT exams were considered technically inadequate (10%) due to bad enhancement of the venous system (60/1000), artefact movements (20/1000) and beam-hardening artefacts due to contrast medium persistence in the anonymous vein or due to the presence of a central venous catheter (30/1000). A total of 900 MDCT whole-body examinations were retrospectively reviewed. Normal anatomy of SVC (Figure 11) and IVC (Figure 12) was present in 800 patients (88.9%). Among the anatomical variants, we found a left-sided SVC (Figure 1) in three patients (0.3%), which in 0.8% of cases was associated to the presence of the right SVC (SVC duplication) (Figure 2); in one case (0.1%), the left SVC drained into the left atrium, determining a minimal, non-clinically significant, right-to-left shunt (Figure 3). A left-sided IVC (Figure 6) was detected in one patient (0.1%), and in 0.2% of cases, it was associated to the presence of the right IVC (IVC duplication) (Figures 4 and 5); in two cases, the IVC duplication was associated with the absence of the left common iliac vein and the origin of the right internal iliac vein from the contralateral vena cava (crossing internal iliac vein), also with a connection to the right common iliac vein (Figure 13). A circumaortic LRV (Figure 8) was detected in 31 patients (3.4%), whereas a retroaortic LRV (Figure 7) was found in 5.8% of patients. The AC of IVC (Figures 9 and 14) was detected in three patients (0.3%); it was associated with an IVC duplication with retroaortic cross-over in 2/900 patients (0.2%), whereas in one case (0.1%), it was associated with hemiazygos continuation of LRV, asplenia and left gonadal vein drainage in internal iliac vein (Figure 15).
Axial (a) and coronal (b) contrast-enhanced CT MPR projections showing a right-sided SVC. Axial (a) and coronal (b-c) contrast-enhanced CT MPR projections showing a right-sided IVC (a-b) and the origin of common iliac veins (c). Coronal contrast-enhanced CT MPR and MIP projections showing an IVC duplication with a crossing left internal iliac vein originating from the left-sided IVC (a) which joins the internal iliac vein originating from the right-sided IVC (b). Coronal contrast-enhanced CT MPR and MIP projection showing the AC of the IVC with a thin segment of the intrahepatic portion of the IVC. Axial (a) and 3D (b-d) contrast-enhanced CT images showing the AC of the IVC (a-b), the hemiazygos continuation of the LRV and the asplenia (*) (c), and the drainage of the right gonadal vein in the right internal iliac vein (d).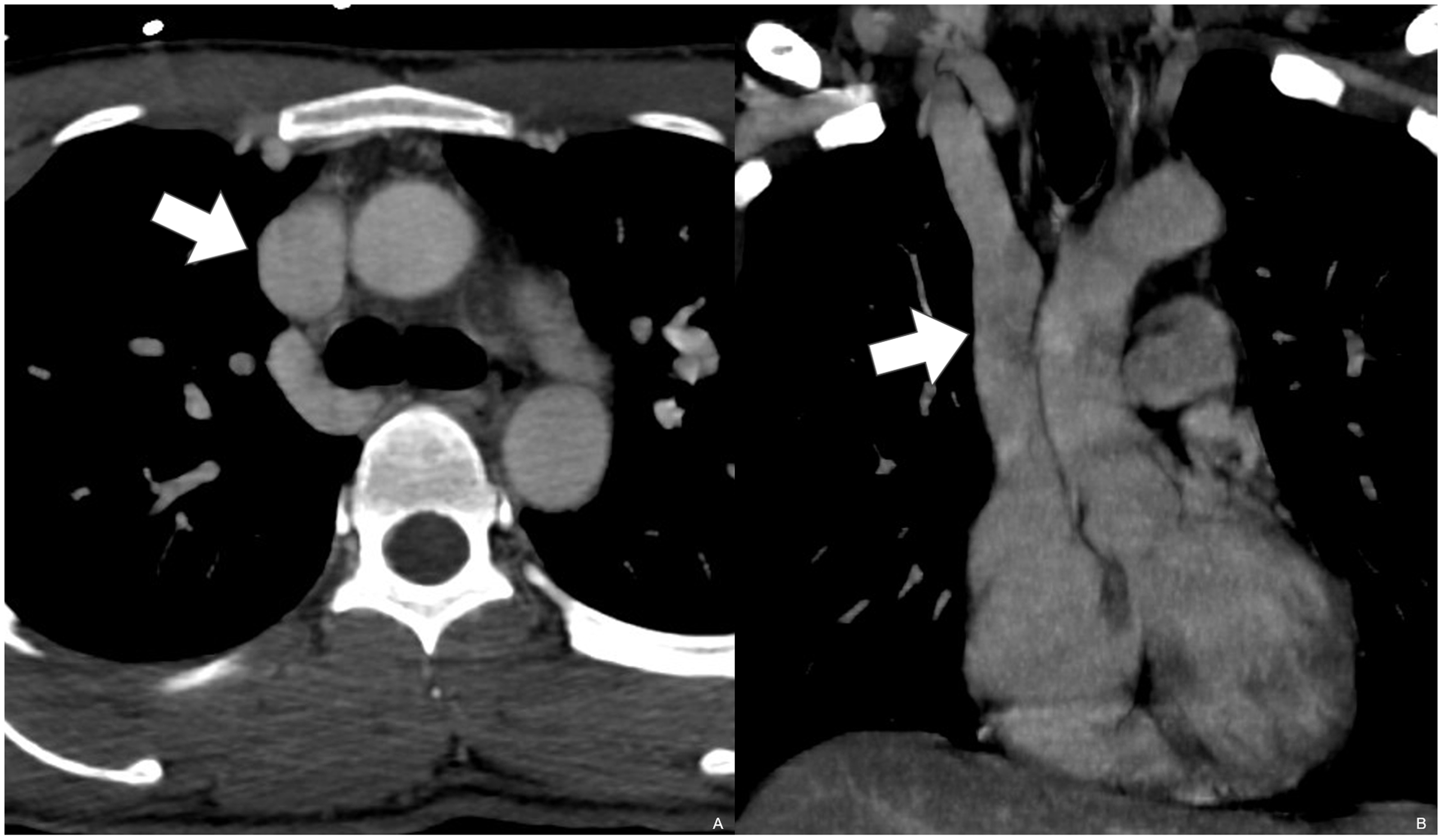


Discussion
Nowadays, due to the development of new interventional radiology and surgical techniques to treat both primary and metastatic tumours, and the increasing availability of transplantation-related interventions, both in donors and receiving patients, the accurate depiction and definition of SVC and IVC anatomy are mandatory. Conventional contrast-enhanced multi-detector CT venography (MDCTV) is an accurate and minimally invasive procedure that requires cannulation of a small vein, non-ionic iodinated contrast injection and use of ionizing radiation; non-ionic contrast medium is the most effective mean to increase the overall safety of contrast media studies, traditionally being characterized by lower incidence of nephrotoxicity and lower risk of adverse reactions in comparison to ionic contrast medium.22,23 MDCTV is useful for evaluation of thoracic and abdominal venous system’s normal anatomy as well as anatomical variants; it is also more accurate than duplex ultrasound (excellent in the study of superficial veins, especially in the limbs, but largely limited in the study of vena cava), and more available and less expensive than venous MRI; on the other hand, MRI technology continuously evolves, providing more advanced equipment and complex software, which is faster and provides increase of image quality. MR sequences like phase-contrast MRI and time-of-flight MRI also allow a good quality of the vascular anatomy without contrast administration. Compared to CT, vascular MRI images are also characterized by an increased signal-to-noise ratio and easier 3D postprocessing. 24 MDCTV is useful in a large number of situations, both in surgical and interventional radiology settings, granting a roadmap for further treatments.25,26 The best reconstruction to provide a panoramic view of the superior and inferior vena cava anomalies, suitable for a proper discussion and confrontation with surgeons and interventional radiologists, especially in case of underlying pathology, usually is made on the coronal or coronal/oblique plane. However, it is mandatory to remember that the acquisitions on the axial plane are always helpful, to better understand the relationship between the veins and the other mediastinal and abdominal structures.
Prevalence of SVC and IVC variants in our study and in literature.
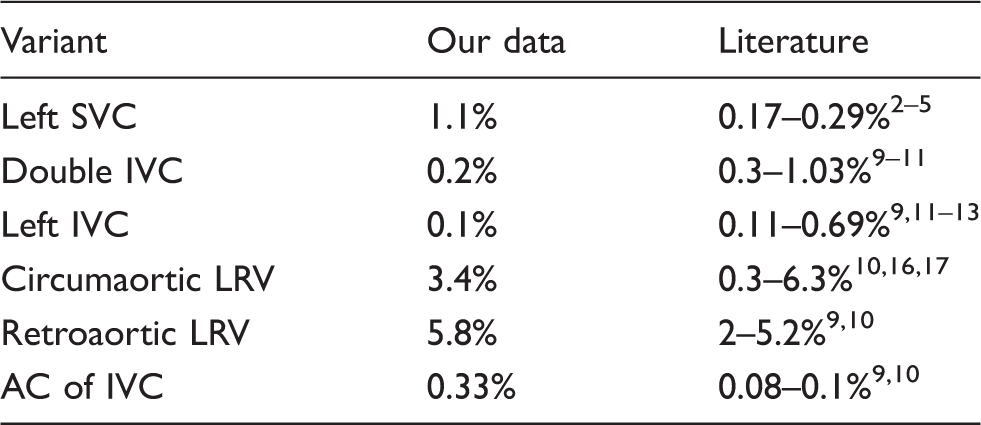
LRV: left renal vein; IVC: inferior vena cava; SVC: superior vena cava; AC: azygos continuation.
Anatomical variants of SVC – all due to the persistence of left common cardinal vein – can be classified into two main groups, based on the regression or persistence of the right common cardinal vein. On the other hand, the IVC anatomical variants can be divided based on the location into supra-renal, renal and infra-renal, a clearer division than the one in pre- and post-renal, bypassing these confounding prefixes. However, in literature there is little or no consensus on the classification of SVC and IVC anatomical variants.27–29 In addition, it is not yet clear which is the underlying cause of these variations; it is, however, well known that, sometimes, more than one variation can occur at the same time. In our experience, we found a few of those variant associations, some of which were similar to some already depicted by other authors; in particular, the case of the IVC duplication associated with the crossing internal iliac vein identified in our search (Figure 13) was similar to the one described by Ogul et al. 30 Another interesting finding, similar to the one described by Ahmetoglu et al., was that of two patients with double IVC with retro-aortic cross-over, and azygos continuation of the IVC: one of the two presented a persistence of a thin intrahepatic IVC segment, which drained the right renal vein, whereas the azygos vein was enlarged due to the collection of the venous blood flow from both the right and left IVCs (Figure 14). 31 On the other side, regarding our case of AC of IVC associated with hemiazygos continuation of LRV, asplenia and left gonadal vein drainage in internal iliac vein, we did not find any already described association like this in literature (Figure 15).
In conclusion, MDCT is a powerful tool to analyse superior and inferior vena cava anomalies. Understanding of caval anatomy and frequent and infrequent variants is helpful for a correct pre-operative planning of interventional radiological as well as surgical procedures. MDCT provides high-quality 3D-reconstructed images and allows minimally invasive assessment of normal anatomy and anatomic variants of superior and inferior vena cava.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The Institutional Review Board waived consent for this study.
Ethical approval
Our Institutional Review Board (Fondazione Policlinico Universitario A. Gemelli Università Cattolica del S. Cuore) waived this study.
Guarantor
RM.
Contributorship
RI and AP designed the study and wrote the manuscript. AP and FC performed literature and internal database research, and collected images. RI and RM critically reviewed the draft.