
Abstract
Aneurysms of the inferior vena cava (IVC) are exceedingly rare; less than 50 cases have been reported in the world literature. Owing to the paucity of data regarding the natural history of IVC aneurysms, there is no consensus on their treatment. This case report describes the evaluation of an IVC aneurysm in a 56-year-old male, briefly discusses the embryologic development of the IVC, and revisits the question of whether surgical intervention is indicated in these patients.
The first report of an inferior vena cava (IVC) aneurysm was published in 1973. 1 This report described a case of a varix of the cardiac segment of the inferior vena cava in a child that was described as an enlarging “soft-tissue density in the right cardiophrenic angle.” The varix was diagnosed on “angiocardiogram.” A Medline search resulted in 26 additional cases that have been published in the English literature since then. A wide range of presenting signs and symptoms have been described, as well as a variety of approaches to the management of this rare entity. We report a case of a relatively asymptomatic IVC aneurysm that highlights the importance of considering this diagnosis in the differential diagnosis of a retroperitoneal mass.
Case Report
A 56-year-old, previously healthy man presented with complaints of mild lower extremity edema associated with nonspecific abdominal pain for several months. His past medical history and past surgical history were unremarkable. The patient had no signs or symptoms suggestive of pulmonary embolism. Physical examination revealed very mild bilateral lower extremity edema without ulcerations or skin changes. A bilateral lower extremity venous duplex sonogram was negative for deep venous thrombosis.
To further evaluate the abdominal pain, computed tomography (CT) of the abdomen and pelvis was performed. The CT scan demonstrated a 4.4 × 5 cm right-sided retroperitoneal mass that was associated with the IVC at the level of the renal veins (Figure 1). This mass was initially felt to be a neoplasm, and percutaneous needle biopsy of the mass was considered. However, owing to the close association of the mass with the IVC, there was concern regarding this approach. Subsequently, magnetic resonance imaging and magnetic resonance angiography of the abdomen were performed, which again showed a 4 cm minimally enhancing mass versus an aneurysm that caused obstruction of the IVC at the level of the renal hilum with the development of significant collateral circulation.

Computed tomographic scan of an inferior vena cava aneurysm (arrow).
Based on the imaging studies, the diagnosis of aneurysm was a consideration, and we decided to proceed with an inferior vena cavogram to further delineate the anatomy. The inferior vena cavogram revealed a large venous varix in the upper IVC below the level of the liver (Figure 2). The IVC appeared to terminate at the level of the varix with more cephalad drainage through a markedly enlarged azygos vein and retroperitoneal collaterals. A catheter was passed easily through the varix into the draining azygos vein, and pressures were measured across the varix. No pressure gradient was present across this varix. There was also no suggestion of intraluminal thrombus based on the appearance of the venogram.

Venogram of an inferior vena cava aneurysm draining into a dilated tortuous azygous vein.
Owing to the lack of pressure gradient across the varix and the paucity of symptoms, no intervention was performed. Nine months following this evaluation, the patient had not developed any new symptoms. The patient will be followed with an annual CT scan.
Discussion
IVC aneurysms are rare. The etiology of these aneurysms is unknown but may be related to abnormalities of the complex embryologic development of the IVC. For the IVC to develop normally, three paired sets of veins must develop, form anastomoses, and regress in a very precise fashion (Figure 3). Briefly, the normal IVC is composed of four segments: infrarenal, renal, suprarenal, and hepatic. The infrarenal portion is derived from the supracardinal veins. The renal segment is derived from the subsupracardinal anastomoses. The suprarenal segment is derived from the subcardinal veins and the hepatic portion from the vitelline vein.
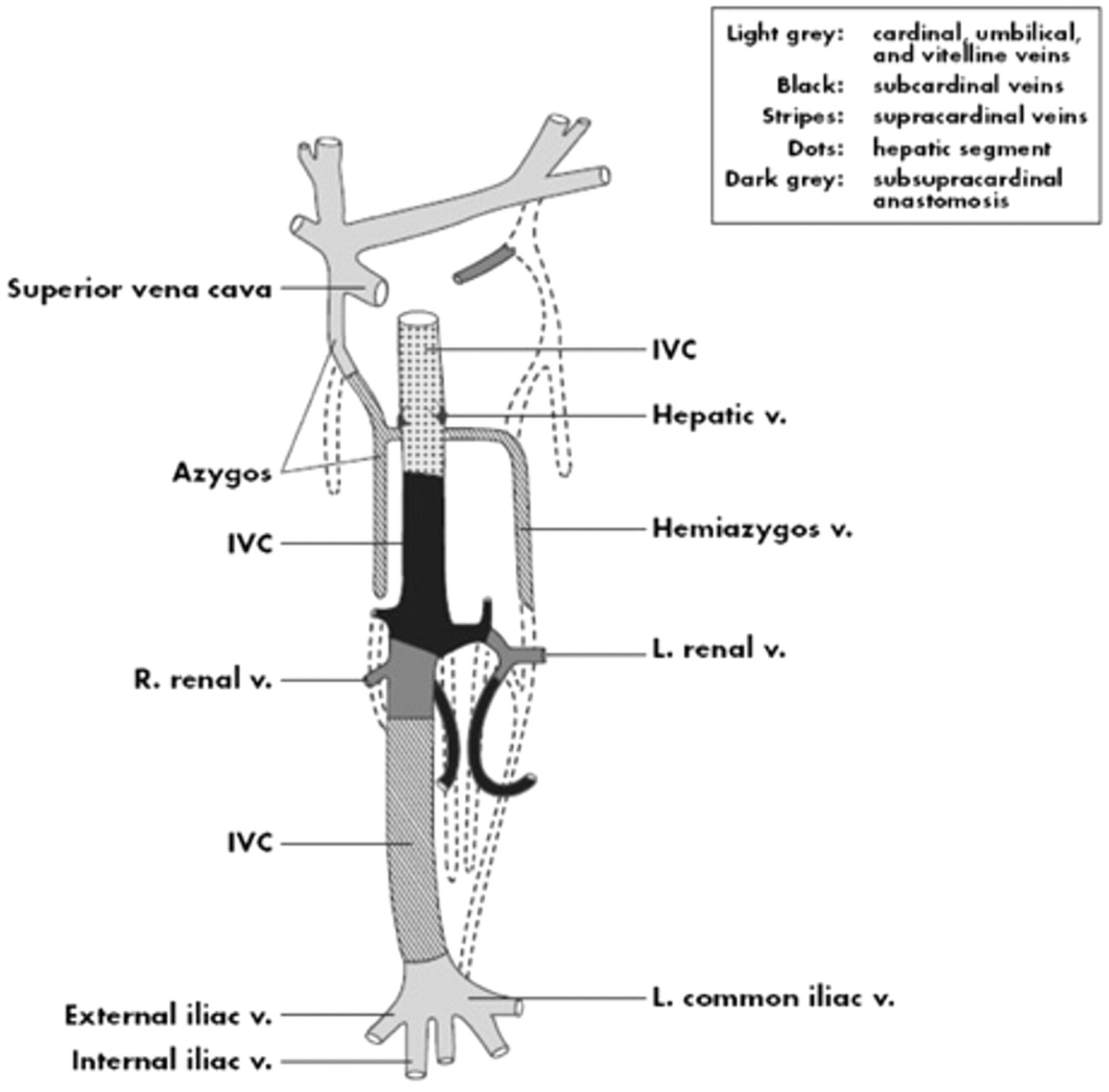
Embryologic origins of the segments of the vena cava. The dashed lines represent segments that have regressed in normal venous development. IVC = inferior vena cava.
The clinical presentation of IVC aneurysms varies in the literature (Table 1). 1–25 The age at presentation ranges from 5 to 77 years. Many IVC aneurysms are discovered incidentally on imaging studies performed for unrelated reasons. 2,7,18,19 The most common presenting symptoms are vague abdominal pain 20,24 and leg swelling associated with lower extremity deep venous thrombosis with or without associated pulmonary embolism. 6,8,10,13,25 Other, more unusual presenting signs and symptoms include massive penile bleeding 5 and an enlarging epigastric mass. 11
Summary of Cases Published in the English Literature
DVT = deep venous thrombosis; IVC = inferior vena cava; LE = lower extremity; NA = not applicable; NR = not reported; PE = pulmonary embolus.
Two different classification systems have been described in the literature for IVC aneurysms. The Thompson and Lindenauer classification describes three types: type I, congenital; type II, acquired; and type III, secondary to arteriovenous fistula. 26 The current patient would be considered type I in this classification. Gradman and Steinberg classified IVC aneurysms into four types based on anatomic variations: type I is an aneurysm of the suprahepatic IVC with no venous obstruction; type II is associated with interruption of the IVC above or below the hepatic veins; type III describes aneurysms confined to the infrarenal IVC without an associated venous anomaly; and type IV is a miscellaneous group. 8 By the Gradman and Steinberg classification, the current patient would be considered a type II.
Owing to the rarity of this condition, little is known about the natural history; thus, there is no consensus about the technical aspects of treatment of IVC aneurysms or even the indications for treatment. Many cases were initially mistaken for neoplasms. 10,18 Thus, the diagnosis of IVC aneurysms should be considered in the differential diagnosis of retroperitoneal neoplasms. If the diagnosis is equivocal, a cavogram should be performed to delineate the venous anatomy. Another useful adjunct that may be considered is intravascular ultrasonography to evaluate intraluminal thrombus.
Several of the asymptomatic cases in the literature were followed with serial CT scans. 18,24 Others were resected owing to thrombosis with associated lower extremity deep venous thrombosis with or without pulmonary embolism. 8,13 Some authors believe that IVC aneurysms should be resected to prevent the complications of deep venous thrombosis and pulmonary embolism. 2,24 At the same time, one case of IVC aneurysm with associated deep venous thrombosis was successfully treated with thrombolysis and warfarin anticoagulation. 6
Conclusion
Clearly, there is no consensus on the indications for treatment or the treatment modalities for IVC aneurysm. As a result, cases need to be managed on an individual case by case basis. The majority of cases in the literature that underwent surgical resection were symptomatic. We suggest that in the case of asymptomatic IVC aneurysms, observation with serial imaging studies is an acceptable treatment option.
Footnotes
Acknowledgment
Financial disclosure of authors and reviewers: None reported.