
Abstract
Aim
Self-application of properly performed compression bandages is generally considered as problematic. Therefore, the aim of this study was to measure the pressure of self-applied short stretch adjustable compression wrap compression systems (Juxta fit™) and to compare the results with the pressure achieved by bandaging other legs using the same material.
Methods
In the two training courses for nurses, specifically interested in leg ulcer treatment, the new bandage type of adjustable compression wrap was explained and workshops were organized, in which the interface pressure achieved by Juxta fit™ was measured. In the first course, the nurses applied the compression system to each other, and in the second course, another group did it on their own legs. Bandagers were instructed to apply the system strongly, with a target range of more than 50–60 mmHg.
Results
In the first course with mutual application (n = 34), the median pressure at the medial lower leg was 58.5 mmHg (minimal 31, maximal value 137 mmHg), in the second course in which self-application was tested (n = 36), the corresponding values were 61.5 mmHg (minimum 35, maximum 102 mmHg). No pressures less than 30 mmHg were seen on the distal calf in either group.
Conclusions
In contrast to short stretch bandages that are frequently applied by bandagers with too low pressure, the adjustable compression wrap devices handled by the patients themselves produce more appropriate and more consistent pressure.
Introduction
Flexible “elastic” textiles (long stretch bandages, compression hosiery) are distinguished from more rigid, inelastic materials (zinc paste bandages, short stretch bandages) according to the elasticity of the compression material.
1
Strongly applied “inelastic,” short stretch materials, exerting a resting pressure of more than 50 mmHg, produce even higher pressures in the erect, standing position and a massage effect when walking, and are more effective in hemodynamic terms than elastic. Such materials2,3 are therefore recommended for serious clinical conditions (venous leg ulcers, symptoms of severe venous congestion, lymphoedema). However, their use in clinical practice is limited by two main factors. In general, most bandages are applied too loosely. The resulting reduction in edema causes a rapid loss of pressure so that the inelastic compression bandages need to be re-applied frequently, especially in the initial phase of treatment. Adjustable compression wrap (ACW) compression systems, such as those first developed in the USA (CircAid Medical Products), are an effective alternative to short stretch bandages, with the advantage that these two mentioned limitations to an effective treatment are avoided:
They can be applied by patients themselves, When they become loose, patients can re-tighten ACW themselves.
In both cases, adjustments can be made according to the subjective sensation of the pressure exerted, and the patient can check whether the desired compression range has been achieved with a supplied pressure-measuring card.
Aim of the study
The rationale of this experimental study was to answer the question if inelastic ACW compression wraps can be properly handled by ambitious first-time users after short theoretical instruction and to proof the prespecified hypothesis that the compression would be stronger and that the variability of the achieved pressures with the new devices would be smaller in comparison with the conventional inelastic bandages reported in the literature.
Material and methods
This is a report of pressure measurements performed under a new inelastic compression system (ACW) at the occasion of two hands-on workshops in the Netherlands in 2012 and 2014.
Following the detailed instruction at the demonstration course, 34 nurses were invited to apply lower leg compression exerting strong, but not painful pressure to each other using Juxta fit™. The pressure achieved was measured with a flat, air-filled probe (Picopress Microlab Italia) at point B1 (the transition between the muscular and the tendinous portion of the medial gastrocnemius muscle) and at the widest section of the calf (Point C) (Figure 1).
Pressure gauge attached to the inner surface of the Juxta fit™ in the two measuring points B1 and C.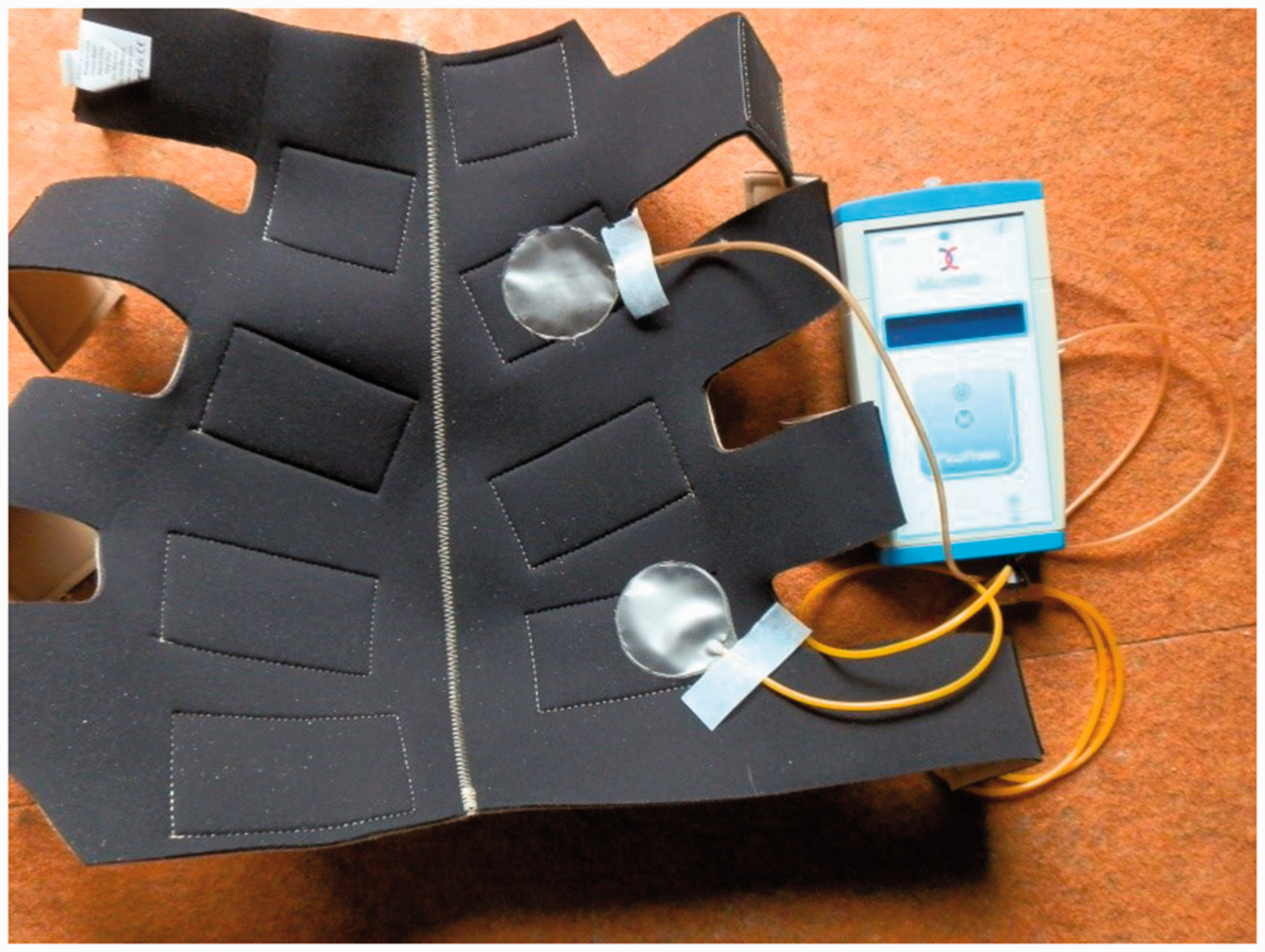
At a second training course two years later, after a theoretical instruction, 36 new participants applied Juxta fit™ to their own legs and the pressures achieved were registered.
Outcome was the interface pressure in mmHg, measured by a reliable instrument.
The course participants were mainly nurses whose main interest was the treatment of venous leg ulcers, but who had no prior knowledge of ACW materials. A total of 59 women and 11 men in CEAP classes C0–C2 agreed to participate. A more detailed analysis was not undertaken, because the clinical manifestations of the subjects were irrelevant for the pressures measured.
In the introductory instruction, the participants were informed about the intended measurements and agreed to participate as a part of the practical hands-on workshop, in accordance with the declaration of Helsinki of the World Medical Association.
They were recommended to apply compression as firmly as possible, but without causing pain, with a tentative range of more than 50 mmHg.
Pressures were measured in a semi-recumbent position (knee slightly bent and rotated outwards, ankle relaxed). Measurements were then made after a maximum of 10 dorsiflexion and after standing up (Figure 2).
Self-applied Juxta fit™. Resting pressure 56 mmHg, pressure peaks on dorsiflexion of up to 65 mmHg. After standing up, the pressure increases to 71 mmHg.
Study design and statistics
Two independent groups of compression pressure values were compared: one after application of ACW to foreign legs in a first training course and the other after self-application in another hand on workshop for new trainees.
Variability was assessed by calculating the coefficient of variation (standard deviation relative to the mean).
The Mann–Whitney U test was used to compare the two independent treatment groups. The intragroup comparison between semi-recumbent (lying), dorsiflexion and standing up was carried out with the Friedman test. For comparing frequencies, the Chi square test was used. p-values of less than 0.05 were considered statistically significant.
Results
Amazingly, people who apply ACW for the first time are able to achieve satisfactory compression pressures after short theoretical instructions. It is demonstrated that self-application leads to a lower degree of variability.
Figure 2 shows the example of a pressure trace recorded at B1 under a self-applied Juxta fit™.
Pressure values (mmHg) measured after self-application (left) versus application of ACW by another person (right).
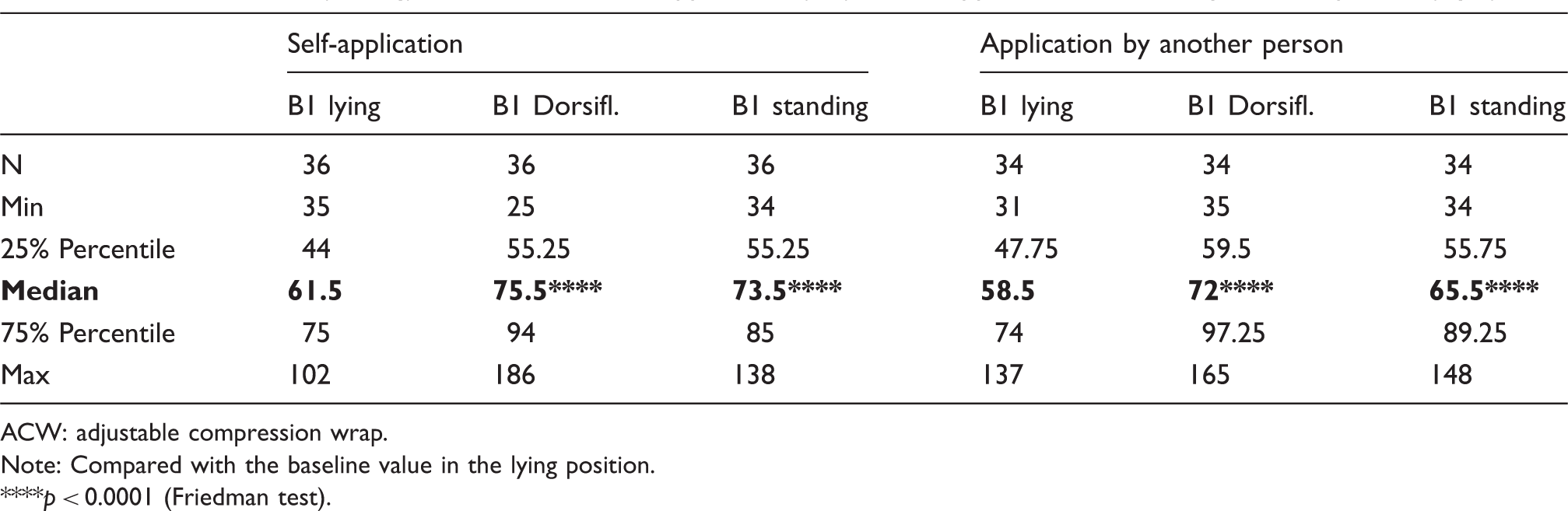
ACW: adjustable compression wrap.
Note: Compared with the baseline value in the lying position.
p < 0.0001 (Friedman test).
Significant increases in pressure occurred after dorsiflexion and after standing up in both the groups, but there were no significant differences in pressures in the various positions between the two groups.
Figure 3 shows the individual pressures at B1 and C in the lying position after self-application of Juxta fit™ and after application by the nurse.
Left half of figure: Comparison of resting pressures measured at B1 between self-application and application by another person. Right half of figure: the same for Point C. Self-application shows a lower coefficient of variation (VC).
There is a greater scatter of pressures after application by another person, and the coefficients of variation (CV) are higher.
The pressure gradient between the two measuring points is shown in Figure 4. Higher pressures over the calf than at the distal lower leg were measured in 3 from 36 persons with self-application (8%), but in 9 from 34 (26%) when the device was mutually applied (Chi square 4.0496, p = .044182).
Pressure gradients between distal (B1) and proximal (C) calf. Self-application shows a more consistent distribution of pressures.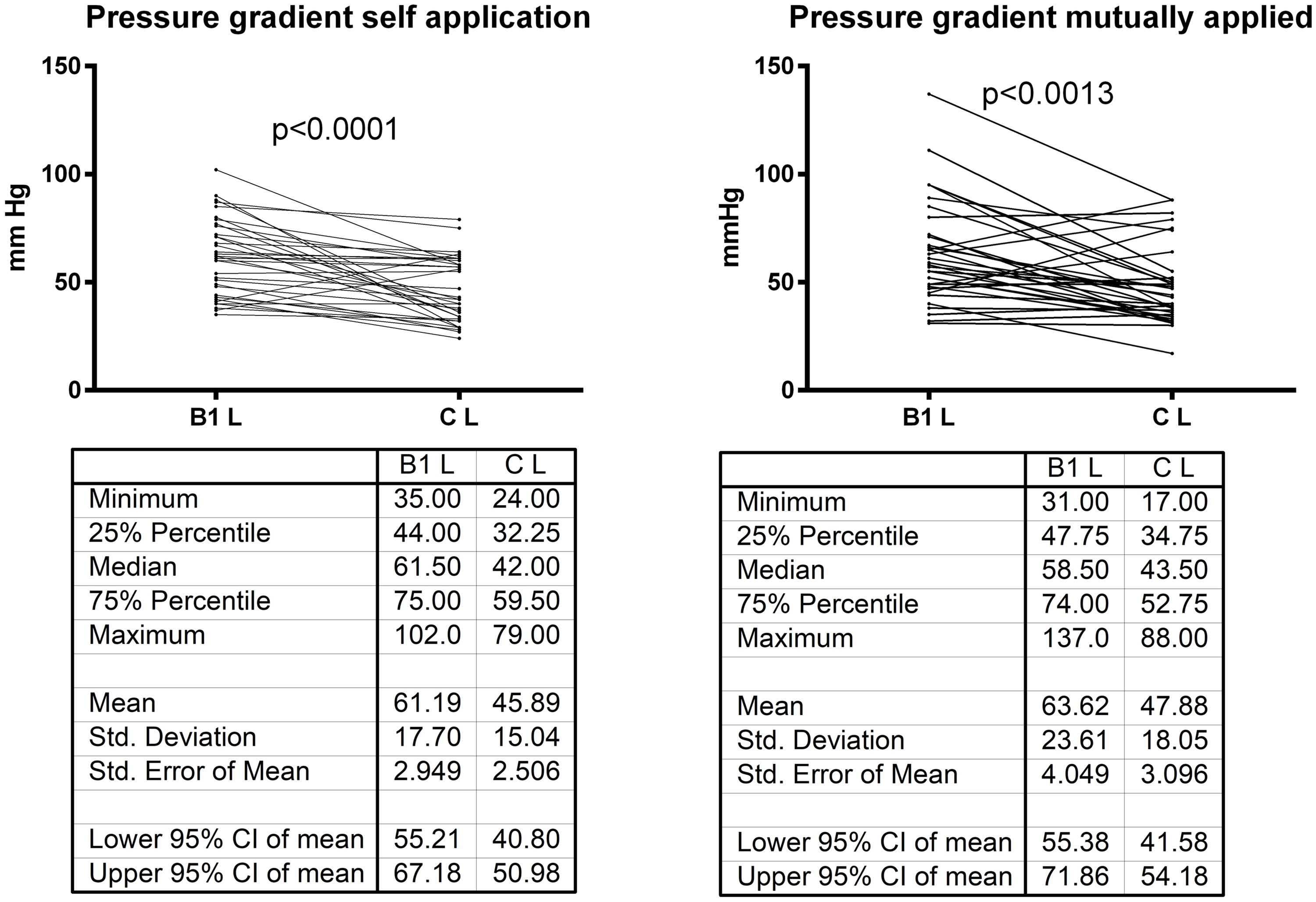
Discussion
The presented data show that self-application of the tested ACW system achieves pressure ranges that are in average not different from those obtained by application to another leg, but show minor variation.
Only one test person applied the system on his own leg with a pressure of 102 mmHg, while values over 100 mmHg were reached five times in the group of mutual bandaging. Also regarding a pressure gradient, self-application produced more consistent results than mutual application. No pressure measured at B1 was lower than 30 mmHg. This shows quite clearly that the subjective feeling is a reliable guide during the application of the ACW device and that subjects can produce proper, strong compression when they are told that the system should be firm, but not painful.
In daily practice, Juxta fit™ is coming with a pressure measuring card to guide the patient in applying the system in a certain pressure range. Comparisons with sub bandage pressure measurements are still lacking.
This report just presents the pressures achieved immediately after application of Juxta fit™® in nurses’ legs and does not give any information on the practicability, tolerability, efficacy or side effects in the longer run. It needs to be underlined 4 that the study participants who applied the compression device were nurses specialized in ulcer treatment, so that it may be problematic to generalize the findings to patients. However, this fact allows comparisons with reported data in the literature.
Also, Heyer et al. 4 measured pressures under short stretch bandages during nursing training courses, made up of participants like ours. Their study showed that of 551 bandages applied, only 51 (10%) achieved the target pressure range of 50–60 mmHg. In 77%, the bandages were applied too loosely (<30 mmHg) and the range of variation was between 6 and 143 mmHg. From the data given in a more recently published extension of this study, reporting pressure measurements under inelastic bandages applied by a total of 972 experienced bandagers a variation coefficient of 54.7% could be calculated, and of 58.1% for a group of 135 non-experts. The pressures in this study ranged between less than 10 and more than 170 mmHg. 5 As shown in Figure 3, the variation of our data is much smaller when Juxta fit™ is used, especially after self-application. In a recent Danish study, pressures between 11 and 80 mm were measured in compression courses and it was concluded that three-quarters of all bandages applied by the healthcare professionals were too loose. 6 These studies clearly demonstrate that most of the conventional compression bandages are applied incorrectly. Earlier studies came to analogous conclusions. For example, Keller et al. 7 showed that it was particularly nurses with many years of experience, who applied bandages too loosely and that refresher courses are helpful for improving the quality of bandaging.
It could be argued that the results obtained here with the healthcare professionals might differ from those to be expected when untrained patients would self-apply the ACW-system.
A previous study in lymphoedema patients showed us that Juxta fit™ can be self-applied highly satisfactorily by untrained patients even after a single demonstration and that the subjective sensation of firmly applied compression is apparently more informative than a bandage optimally applied according to the objective criteria. 8 In this study, Juxta fit™ was first applied to the lower leg by specialized nurses and then removed 2 h later and re-applied by the lymphedema patients themselves. The median pressure at B1 after application by the nurses was 53 mmHg (minimum 27 mmHg, maximum 74 mmHg); the analogous values after self-application by patients 2 h later were 52 mmHg (minimum 35 mm, maximum 69 mmHg). The coefficients of variation were clearly lower with self-application (20%) than after application by the healthcare professional (27.3%). In common with other investigations, the presented data showed that self-application resulted in far fewer excessively low or excessively high values. These results suggest that patients feel the required firmness themselves and avoid pressures that are too loose or too great. Another study performed in patients with chronic edema of the legs showed that the ACW was superior to a short stretch bandage in terms of edema reduction after 24 h. This was probably due to the smaller loss of compression of the ACW material because of readjustment by the patients. 9
The significantly higher pressures recorded on dorsiflexion and on standing compared to the lying position reflect the stiffness of the textile material used.
Stiffness plays a role in patients regarding a more intense hemodynamic and massaging effect and should therefore also be considered in the future studies with other ACW-products. 10 The present study focused on the question whether untrained patients are capable of self-applying ACW systems, with a resting pressure range comparable to that achieved with bandages applied by the healthcare professionals and did not emphasize stiffness, which might be of interest in future studies, comparing different brands of ACW devices.
Conclusions
The pressures recorded under Juxta fit™ suggest that without special prior training, this short stretch material can be self-applied according to the subjective sensation and can achieve a satisfactory range of pressure, which is stronger compared to the reported pressure values from inelastic bandages. Following the brief instruction by a doctor or specialist healthcare professional, patients can provide themselves with highly effective compression.
Footnotes
Acknowledgment
I would like to thank Mrs. Els Brouwer, Medi Netherlands, for her help regarding the pressure measurements and all the hands-on trainees in the courses for their cooperation. Measurements were done at courses organized by Medi, Holland to which the author has been invited as a presenter, advocating inelastic compression material, at that time without practical experience in ACW devices. The study was planned, performed and evaluated by the author without any support from a company.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: HP received travel costs for the courses in Holland where the investigation was carried out, but no honorarium.
Ethical approval
The participating nurses agreed that compression pressure measurements were performed on their own legs as one part of the practical training.
Guarantor
Medi Company, producer of CircAid, Bayreuth, Germany.
Contributorship
The author was responsible for the idea of the study, the pressure measurements, data evaluation and for writing the text of the submitted manuscript.