
Abstract
Background
Oral anticoagulation therapy was the mainstay of deep vein thrombosis treatment but recently, catheter-directed thrombolysis has emerged as an alternative.
Objective
To compare the efficacy and safety of the two strategies.
Methods
Medline, Embase and Cochrane CENTRAL were reviewed. Outcomes of interest included post-thrombotic syndrome, thromboembolic events, mortality, bleeding risk and iliofemoral patency. A random effects model meta-analysis was performed. Heterogeneity was assessed with I square.
Results
Four randomized controlled trials (RCTs) including 1005 patients met the inclusion criteria. Catheter-directed thrombolysis was more likely to prevent overall post-thrombotic syndrome compared to anticoagulation only (OR: 0.32; 95% CI: 0.12–0.85; I2=87.2%), and to lead to iliofemoral vein patency (OR: 2.7; 95% CI: 1.08–6.75; I2=55.3%) but no difference was noted in thromboembolic events (OR = 0.5; 95% CI: 0.08–3.02, I2=55.1%), bleeding and mortality rates.
Conclusions
Catheter-directed thrombolysis can decrease post-thrombotic syndrome rates and improve iliofemoral vein patency compared to anticoagulation when used for the treatment of deep vein thrombosis.
Introduction
Although the precise number of people affected by deep vein thrombosis (DVT) and pulmonary embolism (PE) worldwide is unknown, it is estimated that the annual incidence in the United States is close to 900,000 annually.1,2 Venous thromboembolism (VTE) is the cause of death in almost 60,000–100,000 patients. Almost 45% of patients with DVT, will eventually develop long-term complications, mainly related to post-thrombotic syndrome (PTS), which usually develops within two years of the index event. 1 Some PTS cases might be complicated by excess venous stasis ulcers, which can have an additional impact on a patient’s quality of life as well as increase the overall healthcare costs.1–3
While anticoagulation is the standard treatment of DVT and can prevent PE, it is not equally effective in preventing PTS occurrence.4,5 Previous studies have shown that the extent of thrombus burden and anatomic vein changes such as residual vein thrombosis and popliteal valve incontinence may predispose to increased risk of recurrent VTE and PTS.6,7 Given that the persistence of thrombus in the veins has been associated with unfavorable outcomes, clot lysis or removal was also assumed to decrease PTS risk. While systemic thrombolysis has been shown to be effective in increasing decreasing venous patency and clot lysis while decreasing PTS, it has been linked to an increase risk of bleeding complications including potentially devastating intracerebral bleeding. 8 Catheter-directed thrombolysis (CDT) refers to the technique that combines direct administration of a thrombolytic agent to the thrombus with the usage of devices for thrombus microscopic maceration or aspiration. 9 The aim of CDT is to reduce the thrombus burden in patients with DVT by using a smaller amount of fibrinolytic agent while diminishing the risk of bleeding.
Recently, the largest randomized trial to date was published, adding new evidence for CDT therapy for acute DVT. The Acute Venous Thrombosis: Thrombus Removal with Adjunctive Catheter-Directed Thrombolysis (ATTRACT) showed no difference between CDT and anticoagulation for the prevention of PTS, while the CDT group had an increased risk for major bleeding. 10 Herein, we conducted a meta-analysis of available RCT aiming to compare CDT vs. anticoagulation therapy.
Methods
This meta-analysis was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). 11
Literature search
We conducted a comprehensive literature search of the Medline, Cochrane CENTRAL, Embase and Google Scholar for RCTs comparing CDT vs. anticoagulation therapy for DVT without any language restrictions up to 7/31/2018. In addition, we used internet based sources for information (cardiosource.com; clinicaltrials.gov; theheart.org; and tctmd.com). Two investigators (IB and CAP) independently searched for eligible studies. In cases where there was a disagreement for the eligibility of a study a third investigator was involved in order consensus to be reached. The reference list of pertinent reviews and observational studies was also manually searched for further eligible studies. A combination of the following keywords was used to perform our searches: “catheter-directed thrombolysis”, ‘thrombolysis”, “deep vein thrombosis”, “venous thromboembolism”, “post-thrombotic syndrome” and “randomized clinical trial”. The pre-specified inclusion criteria for the studies were: (i) study groups included catheter-directed thrombolysis and anticoagulation vs. anticoagulation only, (ii) randomized clinical trial design and (iii) intention to treat analysis. Pre-specified exclusion criteria were: (i) duplicated data and (ii) ongoing trials without final results.
Data extraction and outcomes
Data extraction was performed based on a pre-defined data extraction form by two independent investigators blinded to each other. The pre-specified efficacy outcomes included overall PTS occurrence, mild vs. moderate to severe PTS, and VTE (DVT or PE) rates. Efficacy outcomes included bleeding rates and all-cause mortality. Regarding the bleeding rates, since the five-year CAVENT trial results did not report any bleeding events, we performed an analysis incorporating the results of the two-year results of the CAVENT study trial.
Risk of bias assessment
Two independent reviewers (IM and LP) assessed the risk of bias of the included studies with the Cochrane risk of bias assessment tool for RCTs. 12 Studies were assessed as having low, high or unclear risk of bias for the following domains: random sequence generation; allocation concealment; selective reporting; blinding of participants and personnel; blinding of outcome assessment; incomplete outcome data; other bias not covered elsewhere among the domains.
Statistical analysis
Studies outcomes were accepted as defined in the original RCTs. When significant discordances between definitions were present, a more liberal definition was followed. For all outcomes, the intention-to-treat analysis was chosen. We estimated the odds Ratios (ORs) and their respective 95% confidence intervals (CIs) using the random effects model according to the method of Der Simonian and Laird. Heterogeneity among trials for each outcome was calculated by means of I-squared test (a p value ≤ 0.1 was considered statistically significant). 11 Values <25% indicated low, 25% to 70% indicated moderate, and >70% indicated severe heterogeneity To accommodate for different follow-up periods in some outcomes a second analysis was performed for bleeding events, using the two-year rates. A sensitivity analysis was performed for studies that used alteplase only; p values were two-tailed and statistical significance level was set at 0.05 with CIs calculated at the 95% level. Stata 14.1 (Stata Corp., College Station, Texas) was used for statistical analysis.
Results
Out of 487 studies from the literature and on-line sources, 5 studies (four RCTs, since two of the studies – CAVENT two-years and CAVENT five-years – were basically different follow-up period studies from the same RCT) met the prespecified criteria for inclusion in the analysis (Figure 1). The follow-up time ranged between 6 and 60 months among eligible trials. The CaVenT trial (Long-Term Outcome After Additional Catheter-Directed Thrombolysis Versus Standard Treatment for Acute Iliofemoral Deep Vein Thrombosis) reported bleeding outcomes only for 24 months follow-up despite five years of total follow-up. The characteristics of these studies are summarized in Table 1. The acronyms of the studies and the inclusion and exclusion criteria are provided in the Supplementary Table A. Overall, all the studies were found to have low risk of bias (Supplementary Figure 1).
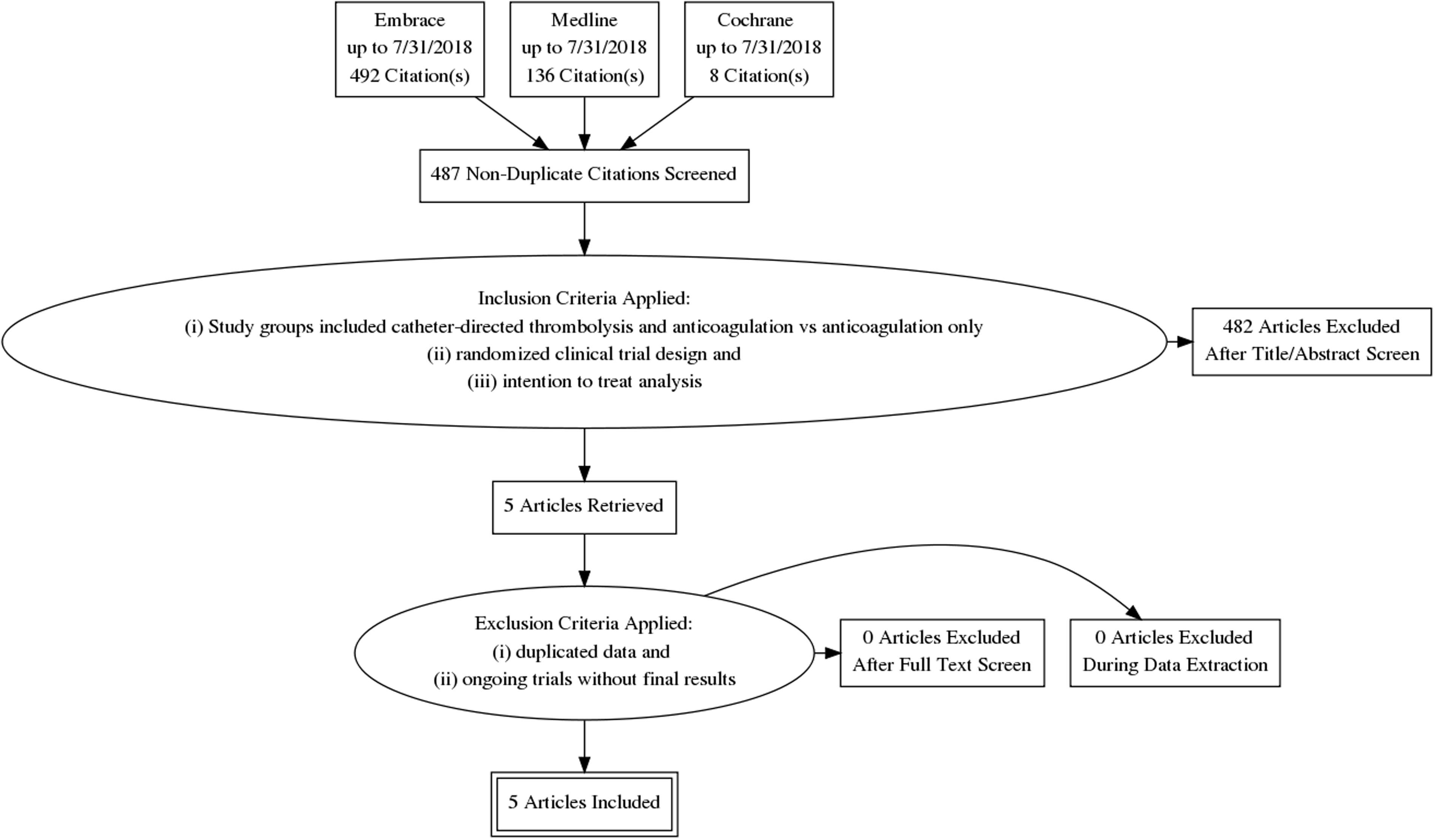
PRISMA flow diagram.
Baseline studies characteristics.
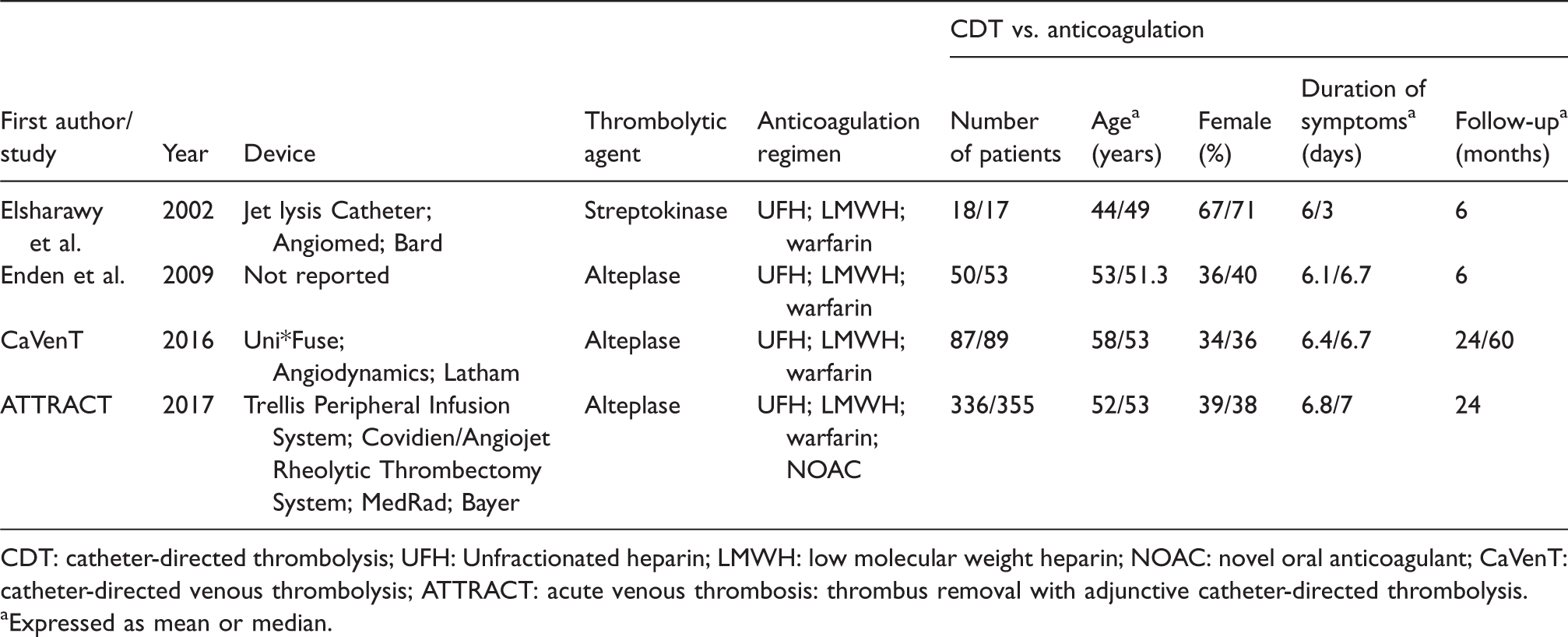
CDT: catheter-directed thrombolysis; UFH: Unfractionated heparin; LMWH: low molecular weight heparin; NOAC: novel oral anticoagulant; CaVenT: catheter-directed venous thrombolysis; ATTRACT: acute venous thrombosis: thrombus removal with adjunctive catheter-directed thrombolysis.
Expressed as mean or median.
The four eligible studies were published between 2002 and 2017. They were conducted in Europe and in the United States. The total number of patients included in the final dataset was 1005 patients, with 491 undergoing CDT plus anticoagulation vs. 514 patients treated conservatively with anticoagulation only. Specifically, ATTRACT accounted for the highest total number of patients in this analysis (n = 692). The mean age for the whole dataset was 52.8 years old and 39% of the population was women. The devices used across the studies varied: The Jet Lysis Catheter (Angiomed, Bard, Karlsruhe, Germany) was used by Elsharawy et al.,13 and the Uni*Fuse Infusion Catheter (Angiodynamics, Latham, NY) was used in the CaVenT trial. The ATTRACT trial used the Trellis Peripheral Infusion System (Covidien, Mansfield, MA) or the Angiojet Rheolytic Thrombectomy System (MEDRAD Interventional – Bayer, Minneapolis, MN). The trial by Enden et al.14 did not report that detail. Regarding the thrombolytic agents, all trials used alteplase except for Elsharawy et al., where streptokinase was used. Anticoagulation regimens did not vary among trials; in the ATTRACT, new oral anticoagulants were used in addition to unfractionated heparin; low molecular weight heparin and warfarin. Supplementary stenting rates were not homogeneous among the procedures. In the Elsharawy 2002 trial, there was only on case were stenting was used (Wallstent endoprosthesis) for the treatment of May–Thurner syndrome and residual left common iliac vein narrowing. In the trial by Enden et al. in 2009, there were in total eight patients out of 50 in the CDT arm who finally received stenting and in 75% of them patency was maintained after six months. In CaVenT trials (2012 and 2016), stenting of the venous lesions was left at the discretion of the operators. In the 2012 trial, 15 patients out of total 90 in the CDT arm finally received stenting. On the other hand, only one patient in the CDT arm (and five in the control group) received stenting in the 2016 trial. Finally in the ATTRACT 2017 trial, where again stenting was left at the discretion of the operators, 82 out of the 237 patients in the CDT group received stenting.
Efficacy outcomes
The overall frequency of all recorded PTS cases (mild, moderate or severe) in patient who underwent CDT was 42.3% (209 out of 491) compared to 53.5% (275 out of 514 patients) in the anticoagulation group. CDT was more likely to prevent overall PTS compared to anticoagulation only (OR: 0.32; 95% CI: 0.12–0.85; p = 0.022; I2=87.2%; Figure 2). CDT was not associated with decreased rates of moderate to severe PTS (OR: 0.33; 95% CI: 0.10–1.03; I2=76.5%; Figure 3), even if a trend towards significance was noticed. Patients treated with CDT were more likely to have patent iliofemoral veins in the follow-up compared to conservative management (OR: 2.69; 95% CI: 1.07–6.75; I2= 55.3%; Figure 4). CDT did not lead to lower rates of future VTE episodes (OR: 0.5; 95% CI: 0.08–3.02, I2=55.1%; Figure 5).

Overall rates of PTS.
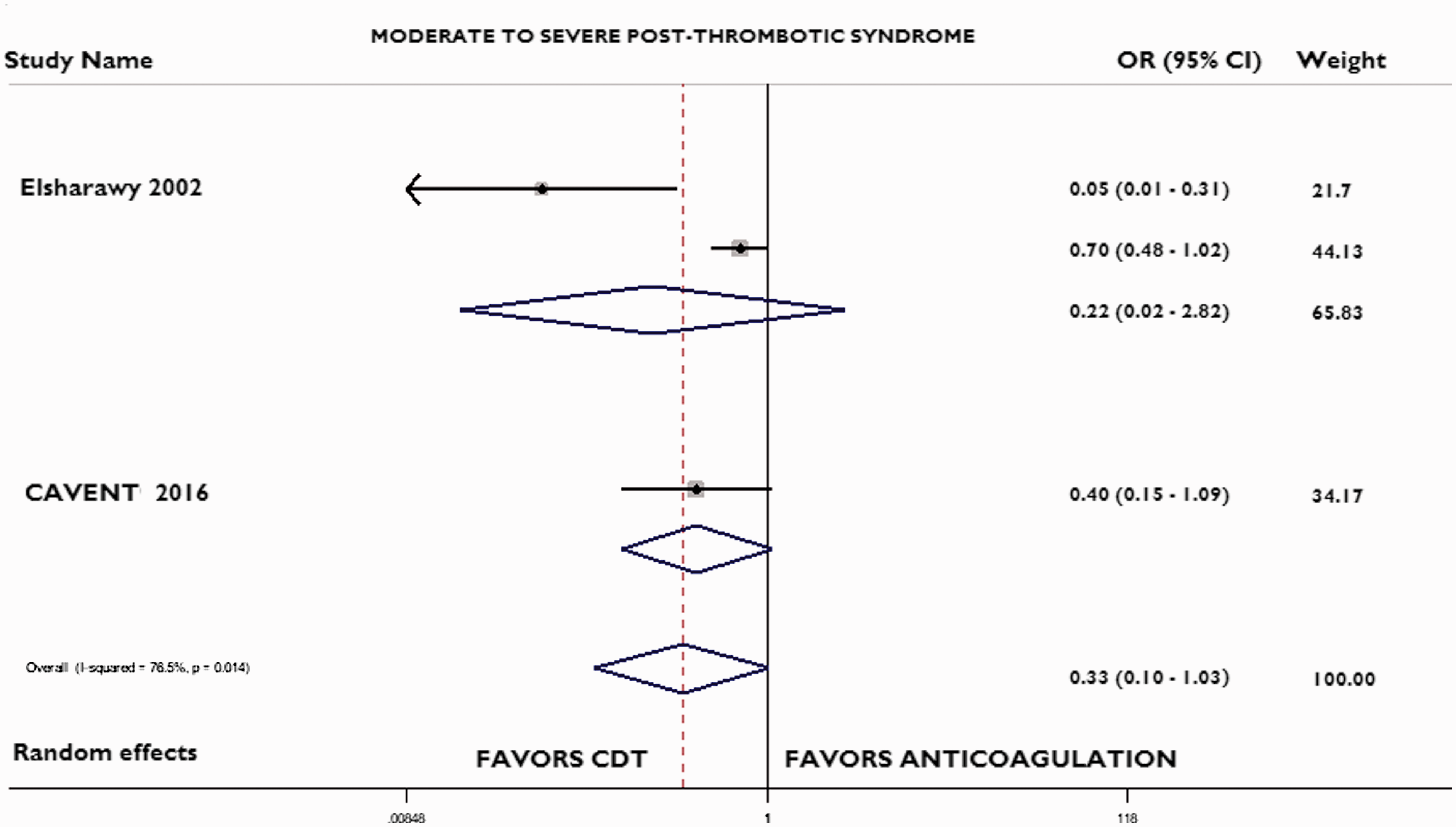
Moderate to severe PTS.
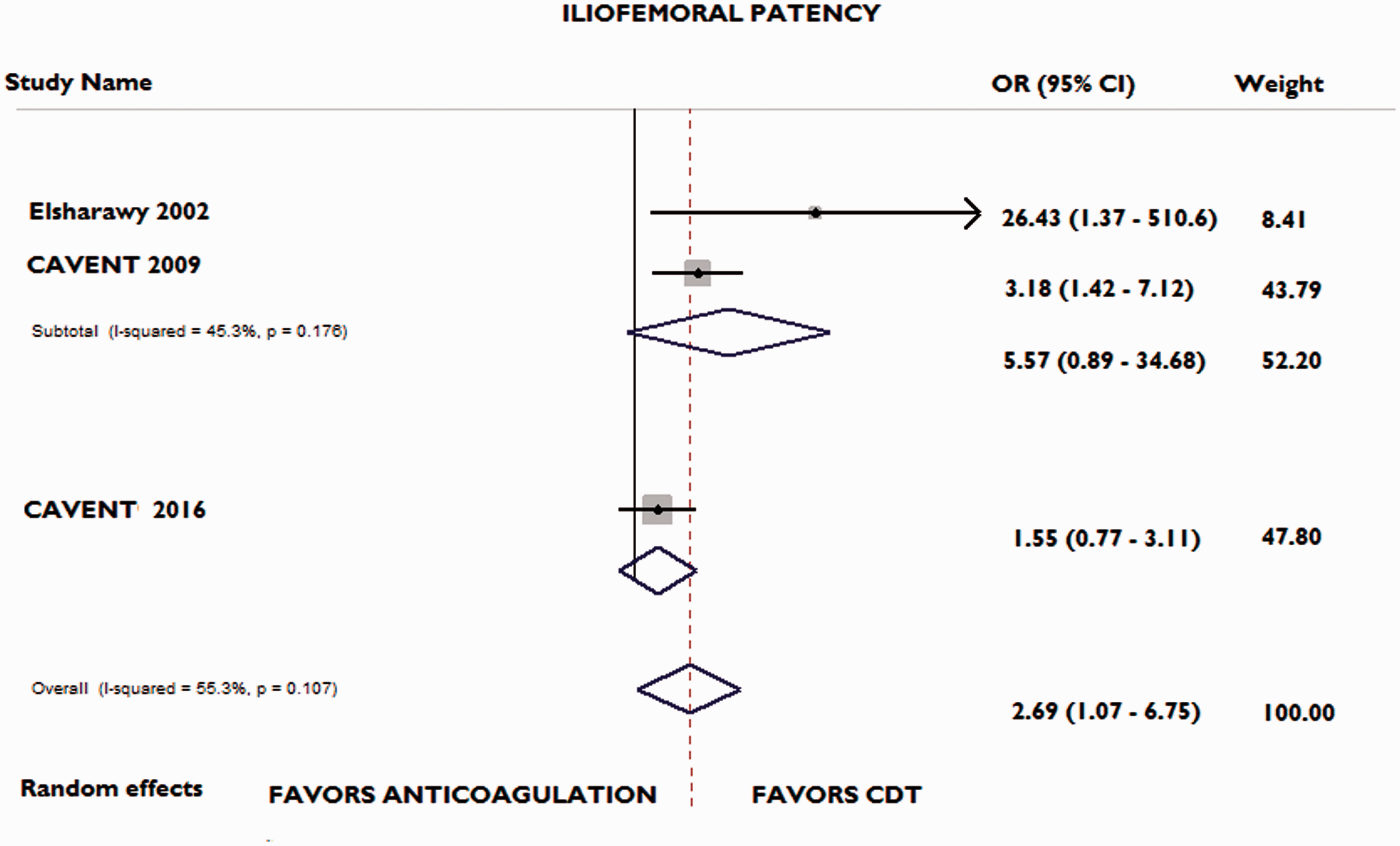
Iliofemoral patency rates.
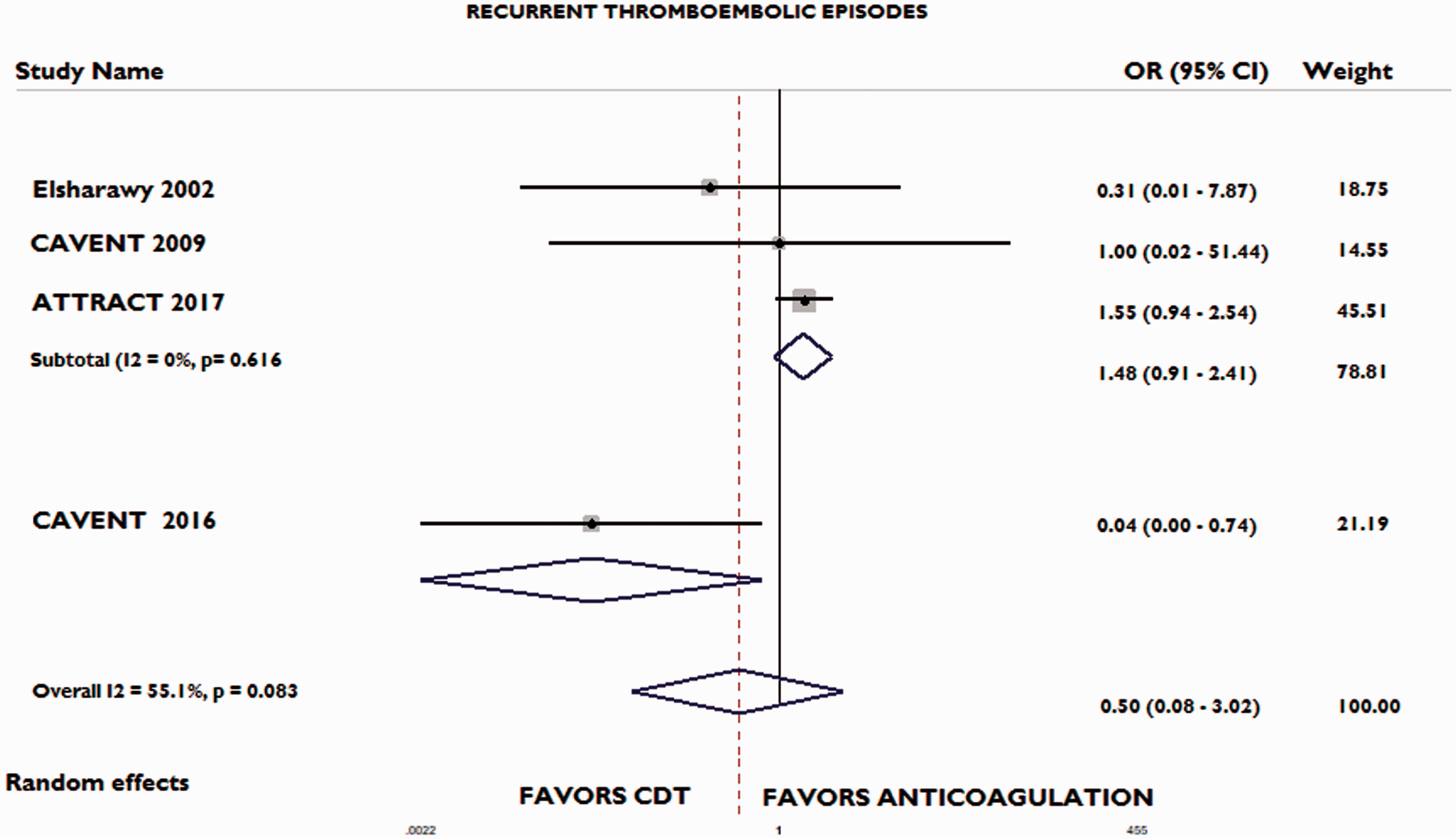
Recurrent thromboembolic episode rates.
Safety outcomes
Rates for bleeding were reported in all four studies included in the meta-analysis. The overall bleeding rates after a follow-up of 24 months in the CDT group was 15.5% (76 out of 491 patients) whereas in the AC only group was 7.8% (40 out of 514 patients). The two groups did not have a statistically significant difference (OR: 4.06; 95% CI: 0.80–20.54; I2=69.7%). The overall death rate in the whole cohort was 1.5%; seven patients in the CDT group compared to eight patients in the AC group. No difference was found between the two groups (OR: 0.99; 95% CI: 0.37–2.38, I2=69.7%).
Sensitivity analysis
A sensitivity analysis was conducted for studies that used alteplase only. The analysis can be seen in the Supplementary materials. No difference was found in the overall PTS rates (OR: 0.45; 95% CI: 0.18–1.13). However, when the analysis was restricted to moderate or severe PTS only, CDT was associated with a decreased rate (OR: 0.64; 95% CI: 0.43–0.96). This finding came in contrast to the overall analysis for moderate to severe PTS and is likely indicative of alteplase superiority. No difference was found in the thromboembolic episodes rates (OR: 0.50; 95% CI: 0.05–5.28). Similarly to the overall analysis, CDT was superior to anticoagulation in terms of iliofemoral patency (OR: 2.16; 95% CI: 1.07–4.35). No difference was observed in bleeding or mortality rates.
Discussion
This was a systematic review and meta-analysis of CDT vs. anticoagulation for the treatment of DVT. The findings of our meta-analysis can be summarized as following: (i) overall PTS was improved in the CDT group, although this benefit was attenuated when the analysis was restricted only to moderate to severe PTS; (ii) iliofemoral patency was improved in patients treated with CDT compared to the anticoagulation only group; (iii) CDT did not increase the rates of bleeding or death in the follow-up period and was equally safe with anticoagulation.
We found that CDT can decrease the overall rate of PTS compared to AC only. However, in our analysis restricted for moderate to severe PTS, no clear statistical difference was found (even though there was a clear trend towards CDT superiority). There are multiple different scoring systems available for PTS classification, but the Villalta score is the most frequently used because it combines ease of use not only for diagnosis and classification but also for follow-up purposes. Our inability to detect a difference may possibly be attributed to the lower incidence of moderate to severe PTS in general. However, given the observed trend, it is reasonable to assume that larger studies would be able to detect a difference.
Additionally, our results for moderate to severe PTS were also driven by the ATTRACT trial. 10 In contrast to the Norwegian CAVENT trial, the larger ATTRACT trial did not show a difference with the addition of CDT to AC therapy.10,15 However, CDT was shown to decrease the burden of PTS, leading to less severe forms. Potential reasons explaining the inability of the ATTRACT study to show a difference could be related to the mechanical therapies that were used in the CDT group compared to CAVENT where there was a longer rt-PA infusion protocol. However, as the ATTRACT investigators mentioned in their original study, venography confirmed that their CDT group achieved thrombus removal in an adequate degree and thus other etiologies should be sought. In accordance to that, our analysis shows that CDT was more likely to lead to a patent iliofemoral vein compared to AC only.
CDT was developed in order to create a more localized thrombolysis effect, while mitigating the potential deleterious effects related to systemic thrombolysis such as bleeding. CDT minimizes the dose of thrombolytic required in addition to avoiding systemic exposure while maintaining exposure of the lytic agent to the clot. Currently, guidelines recommendation on CDT remains controversial (2C recommendation). It would be interesting to see how the new guidelines will interpret the results of the available trials and our meta-analysis. Our study showed that CDT can decrease the overall PTS, while there was no significant difference in the bleeding rates between the two groups. Similarly, the mortality rates were not different.
The selection of CDT or AC in daily clinical practice should be individualized and based on a number of factors. Factors that should encourage CDT use include the most severe DVT manifestations such as extensive DVT including common femoral vein and iliac veins, phlegmasia cerulea dolens (phlegmasia alba dolens) acute IVC thrombosis, or rapid thrombus extension despite anticoagulation.5,16,17 Other important factors for consideration include the overall prognosis and the patient’s activity levels and of course the willingness to undergo an invasive procedure. Patients with the higher chance to respond to invasive procedures are those with DVT symptoms of less than two weeks, iliofemoral DVT and patients with a recently formed thrombus.18,19 On the other hand, patients with less risks for developing PTS, including DVT restricted to the calf or femoropopliteal veins or chronic DVT (>28 days) are less good candidates for CDT
Limitations
Our study has a number of limitations. First, different devices were used among the included trials. Second, the anticoagulation group regimens were not exactly the same. Third, the included studies did not provide cost-effectiveness data, successful thrombus removal (complete vs. incomplete) and location of the lesions (iliofemoral vs. femoropopliteal segments). Fourth, the follow-up duration of the included trials varied. All these limitations, potentially led to the high heterogeneity found in our analysis. However, our meta-analysis benefits from its strong statistical design and our adherence to systematic reviews methodology.
Conclusions
This was a systematic review and meta-analysis of RCTs for the use of CDT in the treatment of DVT and prevention of PTS and other DVT-related complications. Our results show that CDT is equally safe with anticoagulation with regard to risk of bleeding, while leading to decreased rates of PTS and improved vein patency. Future studies should try to examine potential superiority of the available devices and see if CDT outcomes in the real-word could be associated with a lower duration of anticoagulation therapy for these patients.
Supplemental Material
Supplemental material for Catheter-directed thrombolysis vs. anticoagulation for the prevention and treatment of post-thrombotic syndrome in deep vein thrombosis: An updated systematic review and meta-analysis of randomized trials
Supplemental Material for Catheter-directed thrombolysis vs. anticoagulation for the prevention and treatment of post-thrombotic syndrome in deep vein thrombosis: An updated systematic review and meta-analysis of randomized trials by Ioannis Mastoris, Damianos G Kokkinidis, Iosif Bikakis, Paraschos Archontakis-Barakakis, Christos A Papanastasiou, Anil Kumar Jonnalagadda, Dimitrios Schizas, Christos Bakoyiannis, Leonidas Palaiodimos and Robert T Faillace in Phlebology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
none.
Guarantor
Dr Mastoris
Contributorship
All Authors contributed to the study design. All authors participated in literature search and data extraction. Dr Mastoris and Dr Kokkinidis wrote the manuscript. Dr Kokkinidis performed the statistical analysis. All Authors participating in reviewing the final manuscript.
Acknowledgments
none.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.