
Abstract
Objective
This study aims to compare the efficacy and safety of AngioJet rheolytic thrombectomy vs. catheter-directed thrombolysis in patients with acute lower extremity deep vein thrombosis.
Methods
Between the period of February 2015 and October 2016, 65 patients with documented acute lower extremity deep vein thrombosis were treated with catheter-directed intervention. These patients were divided into two groups: AngioJet group and catheter-directed thrombolysis group. Comparisons were made with regard to efficacy and safety between these two groups.
Results
In the AngioJet group, complete or partial thrombus removal was accomplished in 23 (72%) and 3 (9%) patients, respectively. In the catheter-directed thrombolysis group, complete or partial thrombus removal was accomplished in 27 (82%) patients and 1 (3%) patient, respectively. In the AngioJet group, the perimeter difference between the suffered limb and healthy one declined from 5.1 ± 2.3 cm to 1.4 ± 1.2 cm (P < 0.05). In the catheter-directed thrombolysis group, the perimeter difference declined from 4.7 ± 1.6 cm to 1.5 ± 0.9 cm (P < 0.05). The mean urokinase dose was 0.264 ± 0.135 million units in the AngioJet group and 1.869 ± 0.528 million units in the catheter-directed thrombolysis group (P < 0.05). The duration of thrombolysis was 4.2 ± 1.7 h in the AngioJet group and 73.6 ± 18.3 h in the catheter-directed thrombolysis group (P < 0.05). The occurrence of complications in these two groups was 19% and 18%, respectively (not significant).
Conclusion
AngioJet rheolytic thrombectomy is a new, safe and effective approach for treating acute lower extremity deep vein thrombosis. When compared to catheter-directed thrombolysis, this treatment provides similar success with lower urokinase dosage and shorter duration of thrombolysis.
Introduction
Lower extremity deep venous thrombosis (LEDVT) is a common venous disease in clinic.1,2 Pulmonary embolism (PE) can be induced by thrombus shedding in the acute stage of LEDVT. Anti-coagulation therapy is the standard treatment for LEDVT at present. 3 However, anticoagulation therapy cannot dissolve thrombus and restore valve function, while thrombus organization often occurs and is accompanied by post-thrombotic syndrome (PTS), which manifests as pain and edema of the lower limbs, pigmentation of skin, and venous ulcer.4–7 Catheter-directed thrombolysis (CDT) can open deep veins as early as possible to protect venous valve function. Therefore, it has higher value in preventing PTS. However, the time for catheter thrombolysis is longer, and the dose for thrombolysis is higher than pharmacomechanical thrombolysis, which not only causes the patient to be inconvenient in bed but also increases the risk of bleeding and other complications, especially bleeding in important organs, such as the brain.8,9 AngioJet is a rheological thrombectomy device. Its Power Pulse™ Delivery technology couples drug thrombolysis with mechanical rheological pumping, and has a satisfactory curative effect in treating acute LEDVT. This study aims to compare the efficacy and safety of AngioJet rheolytic thrombectomy vs. CDT in patients with acute lower extremity deep vein thrombosis. The report is detailed as follows.
Subjects and methods
This study was conducted in accordance with the declaration of Helsinki. This study was conducted with approval from the Ethics Committee of the first Affiliated Hospital of Soochow University. Written informed consent was obtained from the participants.
Subjects
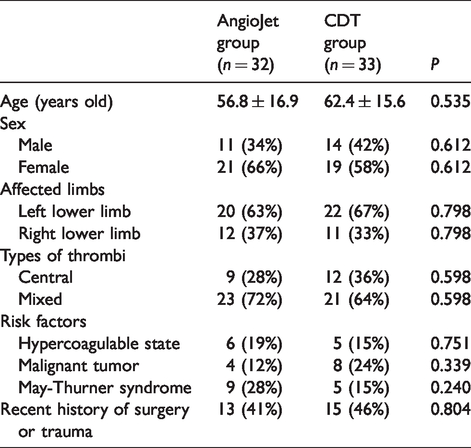
From February 2015 to October 2016, 65 patients with acute LEDVT, who were admitted to the First Affiliated Hospital of Suzhou University and the Third People's Hospital of Yancheng City, were enrolled into the present study. All patients exhibited significant edema of the affected limbs and were diagnosed by ultrasound Doppler. However, contraindications for anticoagulation and thrombolytic therapy were excluded. Patients were randomly assigned into two groups: AngioJet group and CDT group. There were no statistically significant differences in general data between these two groups of patients (Table 1).
General data between these two groups of patients.
Therapeutic methods
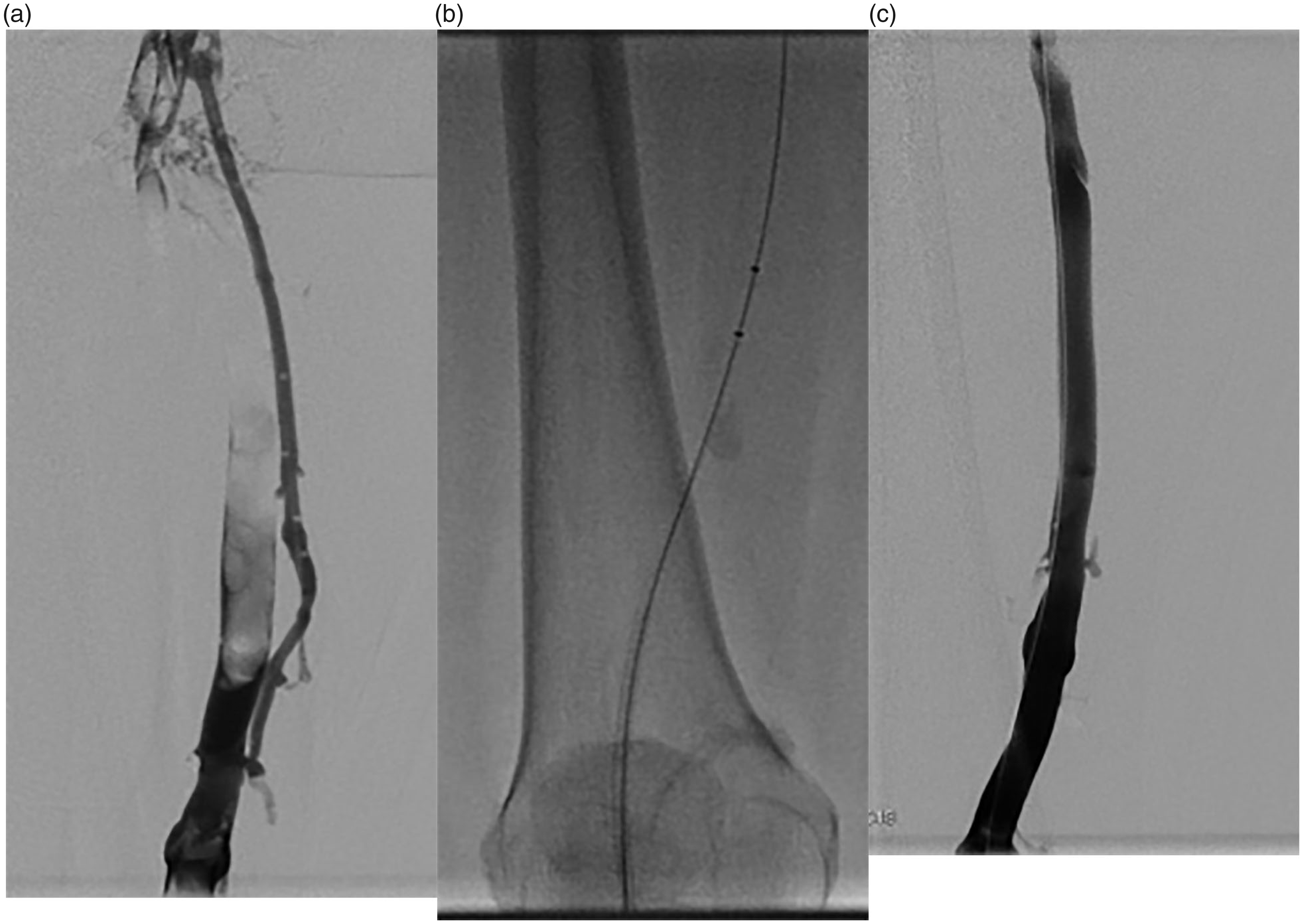
Anti-coagulation treatment: Patients were treated with subcutaneous injection of low-molecular-weight heparin combined with oral warfarin to make the international normalization ratio reach 2.0–3.0 and treated with the oral use of warfarin for 6–12 months, according to the risk factor. Placement and removal of the inferior vena cava filter: Inferior vena cava filters were placed and removed based on the 2011 Expert Consensus on the Standards of Implantation and Removal of Inferior Vena Cava Filters (OptEase, Cordis). Thrombolysis and thrombectomy: The ultrasound-guided puncture of the affected popliteal vein was carried out, and the vascular sheath was placed. In the AngioJet group, an AngioJet thrombectomy catheter (Solent™ Omni, Boston Scientific) was placed into the popliteal vein. First, local spraying thrombolytic mode Power Pulse™ Delivery was chosen, normal saline-containing urokinase (250 ml of normal saline + 300,000 U of urokinase) was injected into the thrombus from the proximal end to the distal end, and the dosage of injection was determined according to the range of thrombus. After waiting for 20–30 min, the rheological suction mode was chosen to suck the thrombus out of the body (Figure 1). If the angiography revealed an incomplete thrombus clearance, thrombus aspiration was performed again. Total blood loss was controlled within 200 ml. If there were still residual thrombus at the end of the treatment, a thrombolytic catheter (Pulse Spray, AngioDynamics) were placed, and 400–600,000 U/day of urokinase was continuously injected. In the CDT group, thrombolytic catheters were placed and passed through the deep venous thrombosis; the thrombolytic segment with lateral holes was placed within the thrombus, the head end of thrombolytic catheter was sealed with the metal inner core, and urokinase was continuously injected using a micropump at a rate of 400–600,000 U/day. The angiography was performed every 24 h to understand the thrombolysis and adjust the position of the thrombolytic catheter. The thrombolysis was discontinued when the deep vein was unobstructed, plasma fibrinogen was <1 g/l, or serious complications, such as bleeding, occurred during thrombolysis. Iliac vein repair: For the patients who had restored patency of deep vein blood flow and limited iliac stenosis, the balloon catheter with a diameter of 10–12 mm was used for dilation. If the contraction was obvious after dilation, a metal self-expanding stent with a diameter of 12–14 mm (E-luminexx, Bard) was placed. A 42-year-old female patient with left LEDVT underwent ultrasound-guided popliteal vein puncture and sheathing. The angiography revealed a large number of filling defects in the femoral vein (a). A Solent™ Omni catheter was placed for the AngioJet rheolytic thrombectomy (b). The re-examination angiography revealed that the thrombus was completely removed (c).
Every patient was followed up through outpatient visits. We checked the geometry and patency of the veins every three months.
Observation indexes
The difference in thigh circumference between affected and unaffected sides before and after the operation: The patient was placed in the supine position, and the difference in thigh circumference at 20 cm from the upper margin of the patella between the affected limb and unaffected limb before and after the operation was measured and calculated. Deep venous thrombosis clearance rate: According to the results of the first and last venography, the effects of the thrombus clearance were classified into three types by two or more interventional doctors with a senior professional title: complete clearance (100%), most clearance (50–99%), and partial clearance (<50%). Dose of urokinase and thrombolytic time: The dose of urokinase and time from the beginning to the end of urokinase injection were calculated. The occurrence of complications.
Statistical analysis
Data were statistically analyzed using statistical software SPSS 19.0. Measurement data were expressed as mean ± standard deviation (x ± SD), and compared using independent sample t-test. Count data were expressed in rate and compared using Chi-square test. P < 0.05 was considered statistically significant.
Results
Among the 32 patients who were treated with AngioJet rheolytic thrombectomy, thrombi were completely removed in 23 patients (72%), mostly removed in six patients (19%), and partially removed in three patients (9%). Among the 33 patients treated with CDT, thrombi were completely removed in 27 patients (82%), mostly removed in 5 patients (15%), and partially removed in 1 patient (3%), and the difference in clearance rate between these two groups was not statistically significant. In the AngioJet group, the difference in thigh circumference between the affected and unaffected sides decreased from 5.1 ± 2.3 cm before the operation to 1.4 ± 1.2 cm after the operation, while in the CDT group, the difference in thigh circumference between the affected and unaffected sides decreased from 4.7 ± 1.6 cm before the operation to 1.5 ± 0.9 cm after the operation. The differences before and after the operation in these two groups were statistically significant (P<0.01 in the AngioJet group; P < 0.01 in the CDT group), while the difference between these two groups was not statistically significant. In the AngioJet group, 17 patients (53%) received placement of the inferior vena cava filter, which was significantly less than that in the CDT group (33 patients (100%)). In the AngioJet group, the inferior vena cava filter was removed in 12 patients (70%), while in the CDT group, the inferior vena cava filter was removed in 18 patients (55%), but the difference between these two groups was not statistically significant. In the AngioJet group, nine patients (28%) underwent balloon dilation of the iliac vein due to iliac vein compression, and two of these patients were placed with metal stents. In the CDT group, five patients (15%) underwent balloon dilation of the iliac vein due to iliac vein compression, and the difference between these two groups was not statistically significant. In the AngioJet group, 20 patients (62%) underwent one operation to complete the treatment of filter placement, thrombolysis and thrombectomy, and iliac vein plasty, 12 patients (38%) continuously received thrombolytic therapy with catheter-directed urokinase due to residual thrombus, and all patients completed the thrombolytic therapy within one to two days. The dosage of urokinase was significantly lower in the AngioJet group (264 ± 135,000 U) than in the CDT group (1869 ± 528,000 U), and thrombolytic time was significantly shorter in the AngioJet group (4.2 ± 1.7 h) than in the CDT group (73.6 ± 18.3 h). In the AngioJet group, transient hemoglobinuria occurred in six patients (19%) after the operation, and this spontaneously alleviated after rehydration and hydration. In the CDT group, bleeding complications occurred in six patients (18%). Among these patients, four patients had hematomas at the site of the popliteal vein puncture and catheterization of the affected side, while two patients had upper gastrointestinal bleeding. No other complications, such as PE, were found in both groups, and the difference in the incidence of complications was not statistically significant (Table 2).
Therapeutic effect and complications of patients in the two groups.

aCompared before treatment and after treatment in the AngioJet group, P < 0.01
bCompared before treatment and after treatment in the CDT group, P < 0.01.
Discussion
The AngioJet thrombus clearance system is a rheological mechanical thrombus aspiration device. It can effectively remove thrombus using Bernoulli's principle with different types of catheters, improving the prognosis and reducing the complications of patients.10,11 When working, the driving pump first generates pulse pressure to inject normal saline through the catheter and reverse jet it from the side hole at the head end of the catheter, in order to wash away the thrombus. Furthermore, high-speed saline also produces local low-pressure areas to suck out the broken thrombus particles though the exhaust hole of the catheter. In addition, its Power Pulse™ Delivery technology can switch the machine to local spraying thrombolytic mode. At this time, the pressure the machine exerts on the pump sends the saline-containing thrombolytic drugs into the pump, ejects together through the opening on the catheter, and acts on the thrombus for 20–30 min. Then, the same catheter is placed in for mechanical aspiration, accordingly removing the softened thrombus.
The AngioJet can not only rheologically and mechanically remove thrombosis but also carry out rheolytic thrombectomy by perfusing thrombolytic drugs into the thrombus area through the working catheter, in order to quickly open blood vessels and restore blood flow, improve distal blood supply, reduce urokinase dosage and thrombolytic time, and reduce the potential risk of bleeding.12–14 The present study revealed that the clinical symptoms were alleviated to varying degrees in patients with acute LEDVT after AngioJet rheolytic thrombectomy, and the difference in circumference between the affected and unaffected limbs was significantly reduced after treatment. Furthermore, the venography before and after treatment revealed that the thrombus was completely removed in 72% of patients, and the curative effect was equal to that of CDT. However, the dosage of urokinase and thrombolytic time were significantly lesser than those of CDT.
Inferior vena cava filter placement can effectively prevent the occurrence of fatal PE caused by thrombus shedding, which is commonly used in CDT therapy.15–17 The present study revealed that AngioJet rheolytic thrombectomy can rapidly remove LEDVT and restore blood flow. For patients with May-Thurner syndrome complicated with acute LEDVT and patients with limited LEDVT, when the thrombus can be completely removed by one operation, the thrombotomy can be performed without the protection of a filter. In the AngioJet group, 15 patients were not placed with inferior vena cava filters, and the proportion of filter placement was lower than that in the CDT group. In both groups, no symptomatic pulmonary arterial embolism occurred, and the filters were not removed due to age, economy, and other factors in some patients in both groups.
The blood flow in the distal inflow tract is closely correlated to the patency rate of deep veins. 18 For patients with May-Thurner syndrome complicated with acute LEDVT, although both AngioJet and CDT can remove the thrombus, the anatomical abnormalities cannot be changed, and when only thrombectomy is performed without correcting the lesions of the iliac vein itself, this would likely cause thrombosis recurrence. Hence, the active and effective treatment of iliac vein stenosis is an important link to ensure efficacy. The experience in this treatment is to open the compressed iliac vein as early as possible by balloon dilatation or stent placement, in order to keep the patency of the inflow tract.19,20 This is essential for the prognosis of patients. In these two groups, patients with May-Thurner syndrome were treated with balloon dilation or stent placement, and the patency of blood flow of the iliac vein was recovered after the operation.
Transient hemoglobinuria is caused by the transient increase of plasma-free hemoglobin caused by the destruction of red blood cells induced by the high-speed water column of the AngioJet. It is different from hematuria, and it can spontaneously alleviate on the day of the operation after full intravenous hydration and hydration, maintaining a certain urine volume. Bleeding at the venipuncture point, digestive tract, and urinary tract is an unavoidable complication of CDT. AngioJet rheolytic thrombectomy can significantly reduce bleeding complications by reducing the dosage of urokinase and shortening thrombolytic time. No bleeding complications occurred in the 32 patients in the AngioJet group.
AngioJet rheolytic thrombectomy was equal to CDT in treating LEDVT. However, it significantly reduced the thrombolytic time, the dosage of thrombolytic agents, and the incidence of complications. Furthermore, the present study had a short follow-up duration. Hence, long-term efficacy needs to be observed through further follow-ups.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.