
Abstract
Introduction
Superficial venous disease (SVD) is a very common disease and much research has been done towards finding the ideal treatment and discovering the pathophysiology of SVD. Not much is known about the psychological burden of SVD. Current guidelines and scientific publications tend to focus on clinical and physiological aspects of SVD. The aim of this study was to relate the changes in Quality-of-Life (QoL) after SVD treatment to possible changes in psychological distress (PD).
Methods
A prospective cohort was set up with the assistance of 5 specialized vein clinics in the Netherlands. Inclusion criteria were: 18 years of age or older, fluent in Dutch language, C1 to C6 (CEAP) class intended to be primary treated with either endovenous laser(LA), radiofrequency ablation (RFA) and phlebectomy(PHL) or sclerocompression therapy alone (SCT). Patients were divided in two groups:
1. C1-C3 patients treated by SCT
2. C1-C6 patients treated invasively (LA, RFA and PHL)
Outcomes were a disease specific QoL questionnaire (CIVIQ-20) and a questionnaire to assess PD (Hospital Anxiety and Depression Scales (HADS)). This study was approved by the local institutional review board, following the principles outlines in the Declaration to Helsinki. This trial was registered in the ISRCTN registry with study ID ISRCTN12085308
Results
442 patients were included in the study and completed the T0 measurements. Mean age of these patients is 54.4 years (s.d. 12.9, 17-90). Number of females: 349 (79.0%), of males: 93 (21.0%). The mean baseline (T-0) HADS depression (0-3) scale scores is 2.54 (s.d. 0.51, n = 412). The mean one-year difference between T-12 HADS depression (0-3) scale scores and baseline T-0 scores is +0.06. The mean baseline (T-0) HADS anxiety (0-3) scale scores is 2.19 (s.d. 0.5, n = 283). The mean one-year difference between T-12 HADS anxiety (0-3) scale scores and baseline T-0 scores is +0.06. Controlled for baseline scores, gender, age, weight and length(BMI), patients in group 2 (receiving invasive treatment) show significantly higher one-year improvement in the QoL of their psychological state of mind than patients in group 1 (receiving SCT and having C1,2,3) (beta 0.158 p = 0.002).
Conclusions
The significant improvement in psychological, QoL and clinical scores that we observe after successful invasive treatment compared to no significant improvement after SCT and the lack of psychological distress in patients with “simple” SVD indicates that SCT is mainly performed for cosmetic reasons. One could thus argue that reimbursement of SCT as a stand-alone medical treatment is debatable.
Background
Superficial venous disease (SVD) is a very common disease, in the Western world up to 60% of adults suffer from different stages of SVD, ranging from simple spider veins to venous ulcers.1,2
Extensive research has been done towards finding the ideal treatment and discovering the pathophysiology of SVD. Only a small percentage of the available literature investigates patient-reported Quality-of-Life (QoL) in relation to SVD. Since the introduction of Patient-reported Outcome Measures (PROMs) in guidelines, protocols and standard care the availability of QoL data regarding SVD has increased. 3
Although publications investigating Psychological Distress (PD) in patients suffering from SVD are available, 4 none has tried to link the PD to the severity of the disease and the according treatment indication. (cosmetic v.s. medical indication) Questions are manifold and unanswered, like: Is PD related to simply the severity of SVD or to disease specific or generic QoL? Do patients with PD, next to the severity of the disease differ according to relevant demographics such gender and age? Can PD eventually be influenced by interventions for SVD? Do physicians underestimate the burden of SVD? Do we treat a cosmetic nuisance, or do we really improve the QoL of patients? No studies have assessed the intervention effects in SVD with both QoL and PD to answer these questions.
In order to relate QoL, PD, clinical severity of SVD, before and after an intervention, prospectively acquired data in a cohort of patients are collected, together with demographics like, age, gender, treatment type, etc., are included with a minimum follow-up of one year. In order to investigate this a predefined conceptual model with hypotheses regarding the underlying relations between the variables is necessary.
Material and methods
A prospective cohort study was set up including patients with SVD in five specialized venous clinics in the Netherlands. Inclusion criteria were: 18 years of age or older, fluent in Dutch language, C1 to C6 (CEAP) class intended to be primary treated with either endovenous laser (LA), radiofrequency ablation (RFA) and phlebectomy (PHL) or liquid sclerocompression therapy (SCT) alone. The SCT group includes small varicose veins unfit for phlebectomy.
Patients with previous venous treatment or deep vein thrombosis or deep vein insufficiency in their medical history were excluded.
In the Netherlands treatment of spider, reticular and small varicose veins with SCT is considered cosmetic and not reimbursed by healthcare insurance companies. In order to allow proper statistical analysis of this consideration, patients were divided in two groups:
C1-C3 patients treated by SCT C1-C6 patients treated invasively (LA, RFA and PHL)
All patients received a venous Duplex before the treatment, following the clinical practice guidelines of the Dutch Society of Vascular Surgery and Dermatology.
Compression sclerotherapy of spider, reticular and small varicose veins was performed with using polidocanol 0,5% and 1% (Aethoxysklerol®, Kreussler Pharma) in a liquid form.
The patients in group 1 did not have any (Duplex confirmed) signs of deep vein insufficiency or superficial main branch(such as great, small or anterior accessory saphenous vein) insufficiency.
Varicose vein removal was performed with micro-stab phlebectomy, under local anesthesia.
RFA treatments were performed with the ClosureFast (previously VNUS) (Medtronic) under local anesthesia.
LA treatments were performed with the VenaCure (AngioDynamics) under local anesthesia.
Patients demographics were noted and they were asked to complete, before, 6 and 12 months after treatment (T0, T6, T12) a disease specific QoL questionnaire (the CIVIQ-20) 5 and a well-established scale to measure PD (Hospital Anxiety and Depression Scales (HADS)). 6
The HADS consists of a seven-item depression scale (HADS-dep) and a seven-item four-point scale (0-3) anxiety scale (HADS-anx). Higher scores (0-21) are supposed to show higher distress. The HADS instrument is made in such a way that its scores are not influenced by somatic pathology.
The Chronic Venous Insufficiency Quality-of-Life Questionnaire (CIVIQ) 5 is a disease-specific instrument to measure QoL in SVD patients. It consists of 20 five-point Likert items containing four overall scales: a Pain, Physical Problems, Social Problems and Psychological Problems scale. The four scales are presented as VAS scales (0 (max)-100 (no problems)).
Hypotheses
We hypothesize that an increased clinical severity and impaired QoL in SVD will also increase PD and that an invasive intervention (group 2) will show larger improvements compared to SCT (group 1). The aim of our study is not to prove the effect of the therapy on the psychological burden, but the psychological burden of SVD itself.
We assume that disease-specific QoL impairment has an impact on generic experienced daily-life PD, and not the other way around. For instance, particular perceptions of patients regarding the condition of the veins in their legs are supposed to affect the full range of their feelings of depression or anxiety in everyday life. The conceptual relationship between perceived impairment and generic distress is assumed to be one-way recursive, that is: depression or anxiety will not affect the specific perceptions of impairment.
Statistics
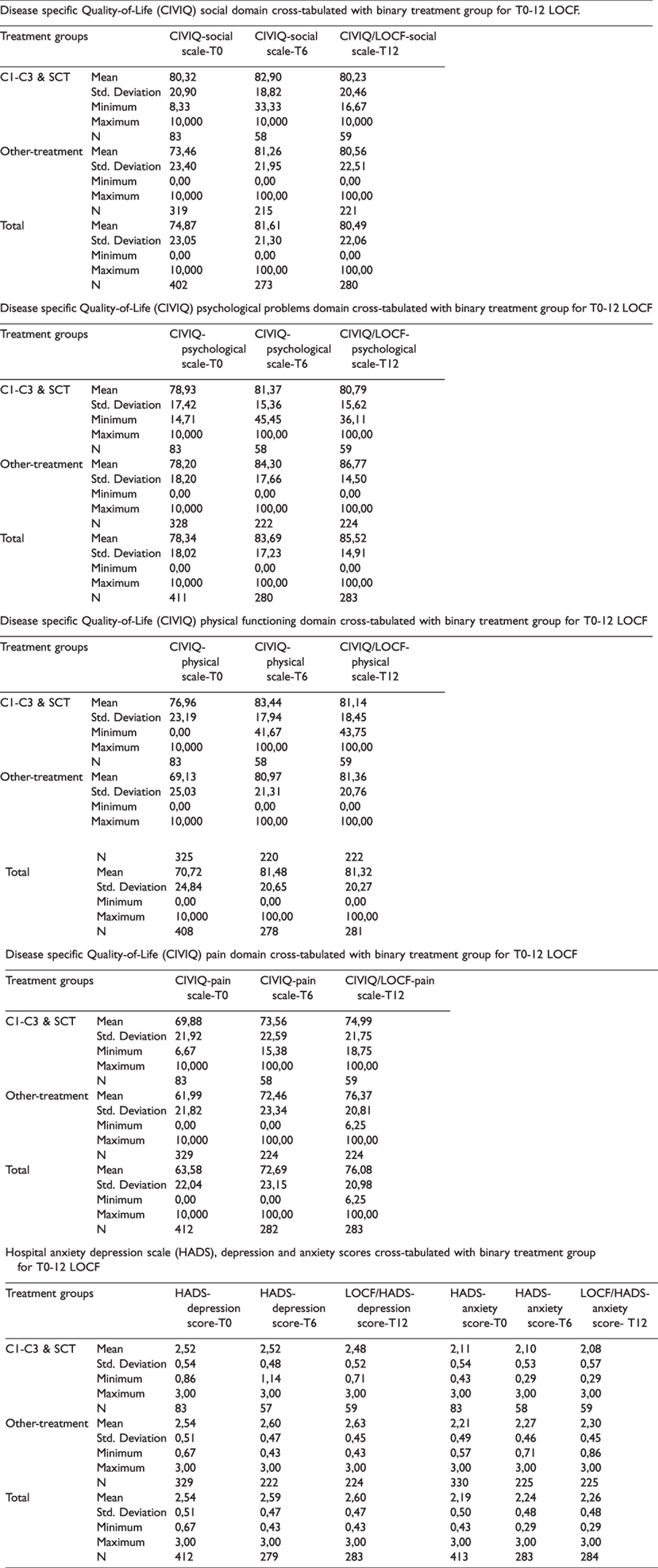
To investigate whether variables show normal distributions the Shapiro-Wilk test is used. If normally distributed, means, standard deviations and numbers of patients are given for metric variables, if not, the minimum and maximum scores are also presented. Categoric variables are shown as frequencies and percentages. Raw outcome variables at baseline (T-0), at 6 months (T-6) and at 12 months (T-12) such as psychic distress and QoL are presented in tables broken down for CEAP (Tables A1–A4) and treatment group (Tables A5–A8). Tables A1–A8 are presented in the Appendix.
CEAP C-class cross-tabulated with treatment type.

SCT: liquid sclerocompression therapy; Strip: Stripping; VNUS: radiofrequency ablation.
To overcome problems of missing data at T-12 the Last-Observation-Carried-Forward (LOCF) technique is performed using data from T-6. Imputed data for T-12 are also displayed in the tables.
Scale constructions with observed items scores usually result in Visual Analogue Scales (VAS) ranging from 0 to 100 (no problems) with exception to the HADS, which ranges from 0 to 3 (no problems).
A p-value of less than 0.05 was considered statistically significant. All data-analysis is performed with IBM SPSS Statistics, version 25.
Results
Descriptive statistics
442 patients were included in the study and completed the T0 measurements. Mean age of these patients is 54.4 years (s.d. 12.9, 17-90). Number of females: 349 (79.0%), of males: 93 (21%).
Males are statistically significantly older than females: 57.8 (12.5) vs. 53.4 (12.9), Student t-test p = 0.004.
Out of the 442 patients 288 (65.2%) were included from Zuyderland Medisch Centrum (ZMC), 57 (12.9%) from Phlebology Centre Oosterwal (FCO), 45 (10.2%) from Westfriesgasthuis (WFG), 44 (10.0%) from Braam Clinic (BC) and 8 (1.8%) from Phlebology Centre Grave (FCG).
The frequencies of baseline CEAP classification categories are: C1 29 (6.6%), C2 43 (9.7%), C3 294 (66.5%), C4 54 (12.2%), C5 6 (1.4%) and C6 11(2.5%). For 5 (1.1% of the total) patients the CEAP class score is missing. Eleven (2.5%) of the 442 patients eventually did not get treated(patients who withdrew themselves from the scheduled therapy or clinic visits).
The remaining 431 patients were treated by the following interventions: laser 72 (16.7%), RFA 153 (35.5%), PHL 111 (25.8%) and SCT 84 (19.5%), Miscellaneous (2.5%) being: compression 6 (1.4%), crossectomy 4 (0.9%) and stripping 1 (0.2%).
33.49% of the included patients was lost at 6 months and 50.69% at 12 months(patients who did not respond to mailed questionnaires or on invitations to visit the clinic). LOCF technique was performed using data from T-6, therefore the amount of analyzed responses were higher, than the actual amount of responsive patients at T-12.
CEAP classes per treatment are shown in Table 1. Including center and respective treatment modalities are shown in Table 2.
Treatment center cross-tabulated with treatment type.

Overall
The mean baseline (T-0) HADS DEPRESSION (0-3) scale scores is 2.54 (s.d. 0.51, n = 412).
The mean one-year difference between T-12 HADS depression (0-3) scale scores and baseline T-0 scores is +0.06, so there is a statistically significant, one-year positive change (one-sample t-test P < 0.05).
The mean baseline (T-0) HADS ANXIETY (0-3) scale scores is 2.19 (s.d. 0.50, n = 413).
The mean one-year difference between T-12 HADS anxiety (0-3) scale scores and baseline T-0 scores is +0.06, so there is an overall statistically significant, one-year positive change (one-sample t-test P < 0.05).
Group 1 (C1–C3 with SCT)
The mean baseline (T-0) HADS DEPRESSION (0-3) scale scores is 2.52 (s.d. 0.54, n = 83).
The mean one-year difference between T-12 HADS depression (0-3) scale scores and baseline T-0 scores is -0.04, so there is no improvement at one year.
The mean baseline (T-0) HADS ANXIETY (0-3) scale scores is 2.11 (s.d. 0.54, n = 83).
The mean one-year difference between T-12 HADS anxiety (0-3) scale scores and baseline T-0 scores is -0.03, so there is no improvement at one year.
Group 2 (C1–C6 with an invasive treatment)
The mean baseline (T-0) HADS DEPRESSION (0-3) scale scores is 2.54 (s.d. 0.51, n = 329).
The mean one-year difference between T-12 HADS depression (0-3) scale scores and baseline T-0 scores is +0.09 (3% difference), so there is a statistically significant, one-year positive change (one-sample t-test P < 0.05).
The mean baseline (T-0) HADS ANXIETY (0-3) scale scores is 2.21 (s.d. 0.49, n = 330).
The mean one-year difference between T-12 HADS anxiety (0-3) scale scores and baseline T-0 scores is +0.09 (3% difference), so there is a statistically significant, one-year positive change (one-sample t-test P < 0.05).
Means are also shown in Table 3.
CIVIQ domains vs binary treatment group
Regression analysis
In a linear trend regression analysis, controlled for baseline scores, gender and age, patients in group 2 show significantly higher one-year improvement in the QoL of their psychological state of mind than patients in group 1 (beta 0.158 p = 0.002).
Also the HADS depression and anxiety scores are affected by treatment modalities. Patients in group 1 show one-year QoL improvement, specifically in the CIVIQ psychological scale, which in turn will have eventually lowering effects on their feelings of depression and anxiety in the HADS score.
In conclusion the HADS anxiety and depression scores are indirectly but significantly determined by the Psychological Scale scores of the CIVIQ questionnaire. A higher (better) CIVIQ score leads to lower (better) HADS scores. The CIVIQ scales are determined by the treatment group, group 2 shows significant improvement compared to group 1.
Discussion
CEAP is based on clinical opinion of physician, scoring the observed clinical symptoms of venous disease. 7 The disease specific QoL assesses the perceived effects of the varicose veins, which are determined by more than just the clinical symptoms (redness, varicose veins, skin changes). 8 The HADS questionnaire (consists of a seven-item depression scale and a seven-item anxiety scale) detecting depression and anxiety in patients with physical problems, without considering the somatic symptoms and physical condition of the patient.
The appearance of different clinical symptoms of SVD may cause emotional disappointment and related psychological distress. 4 There are no validated score systems, measuring PD in SVD. We assumed, that using of the validated HADS questionnaire in combination with the CIVIQ gives an insight in the complexity of psychological distress of patients having SVD. The HADS has been validated and tested with a variety of different somatic pathologies.9,10
Our findings show that patients in group 2 (>C3) have significant, although indirect, higher (worse) HADS scores, in other words, patients in a higher C class suffer from more depression and anxiety.
As shown by these results the burden perceived by the patient is caused by more than just the clinical symptoms - QoL and psychological effects play a large role.
The significant improvement in both psychological (as measured with the HADS) and QoL (as measured with the CIVIQ-20) that we observe after successful invasive treatment could indicate that reimbursement of an invasive treatment is justified. The fact that only SCT for C1-C3 does not improve the psychological, QoL and clinical scores indicates that reimbursement might be questionable (in the line with the reimbursement policy of the Dutch Health Insurances) and could rightfully be classified as a cosmetic treatment.
Perhaps the choice for a specific treatment should not be made based only on a clinical observation, but also be based on the QoL and psychological burden of the disease. For example: a C3 patient with hardly any psychological and QoL impairment will probably only need SCT treatment but a C3 patient with an impaired QoL and psychological burden might benefit of an invasive treatment.
Current guidelines focus mainly on physical observations (C class, duplex ultrasound) and largely disregard QoL and psychosocial impairment. 11 This means that potentially a large number of patients is left untreated because their physical and “visible” disease is considered minor, while their QoL and psychological impairment might be very relevant and significant. A more QoL and psychological centered approach could improve this and would make patient treatment selection more efficient.
Conclusion
Significant psychological, QoL and clinical scores are observed after invasive treatment. SCT alone for C1-C3 does not improve the psychological, QoL and clinical scores. This makes reimbursement questionable for this group and the medical purpose of SCT as a single treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the local institutional review board, following the principles outlines in the Declaration to Helsinki. This trial was registered in the ISRCTN registry with study ID ISRCTN12085308
Guarantor
CHA Wittens.
Contributorship
Conception and design AG, FS, CHA. Analysis and interpretation AG, FS, CHA. Protocol development, gaining ethical approval IAJ, CHA, AG, FS. All authors collected data, reviewed and edited the manuscript and approved the final version of the manuscript.
Acknowledgements
The authors would like to thank the following participants and their institutes: Zuyderland Medical Centre, Heerlen/Brunssum: A.M.J. van der Kleij. E. Eussen. Flebology Centre Oosterwal, Alkmaar: J. Lawson. Westfriesgasthuis, Hoorn: A. Wiersema. Flebology Centre Grave: D. Groeneweg. Braam Clinic, Assen: A. van Goethem.