
Abstract
Objectives
Cyanoacrylate closure (CAC) procedure has become an alternative treatment method that has become increasingly popular in the treatment of chronic venous insufficiency (CVI) in recent years. The present study was designed to assess the feasibility, tolerance, results, and efficacy of CAC for truncal varicosities in elderly population.
Methods
In this retrospective single-center observational cohort study, CAC procedure was performed in 160 patients (184 limbs) with truncal varicose vein insufficiency. The patients were divided into two groups: elderly group, and younger group. The primary outcome of this study was to assess the feasibility, tolerance, and safety of the CAC procedure for truncal varicosities in elderly population over 70 years. The Venous Clinical Severity Score (VCSS), visual analogue scale of pain (VASP) and occlusion rate of the treated target veins of the patients were evaluated and compared among groups. The secondary outcomes were to evaluate and compare technical success, mortality, major adverse events, and other postoperative complications between the groups.
Results
All operations were carried out under local anesthesia. There were no technical failures or device-related complications. Anatomic success rate was 100% after procedures. The occlusion rate for the elderly group at 2 weeks, 6 months, and 12 months was 100%, 92.3%, and 92.3%, respectively, while the occlusion rate for the younger group was 100%, 97%, and 94.7%, respectively. There was no significant difference in occlusion rates between two groups (p > .05) (Log Rank = 0,231). Improvement in the VCSSs was statistically significant between baseline and 12 months after procedure in both groups (p < .001). Improvement in the VASPs was statistically significant between baseline and 2 weeks after procedure in both groups (p < .001). There were no symptoms or signs of sural nerve injury, hematoma, or phlebitis in either group.
Conclusions
Although it has some potential risks, it is conceivable that the CAC procedure may be applied in selected fit elderly patients for the treatment of CVI. Age appeared to have no effect on the early and mid-term prognosis of the CAC procedure performed in the study cohort.
Introduction
Chronic venous insufficiency (CVI) is a major health concern that impairs people’s quality of life and can lead to serious complications. 1 CVI affect 20%–60% of individuals, according to population-based research. 2 Furthermore, the reported prevalence of severe CVI in the elderly is 0.5–3%. 3 CVI is a pathology that is more often neglected, especially in older men, and whose diagnosis and treatment is disrupted.
Elderly patients may have more comorbidities, and their CVI is frequently worse than in youngers. Relief of symptoms and improving quality of life are the primary goals in the treatment of CVI in the elderly population. Wearing medical compression stockings (MCS) and venoactive drugs are recommended as initial treatment modalities. 4 However, it may be difficult for elderly population to adapt to these treatments in daily life, especially in terms of wearing MCS. Therefore, when these patients present to vascular surgery clinics with more advanced and worse legs, alternative surgical or interventional treatment options may be required. 5
In the treatment of CVI, minimally invasive techniques are related to reduced morbidity and faster recovery times than traditional surgery. These techniques have been demonstrated to be effective in the treatment of symptomatic varicosities and venous ulcers. 6 However, the cyanoacrylate closure (CAC) procedure is an attractive alternative to other procedures because it is less invasive, performed with local anesthesia, does not require tumescence, and does not need post-procedure MCS wearing. 7 Despite numerous studies showing improvements in symptoms and quality of life in the elderly, there is a lack of data on the safety and results of CAC procedures in this patient group.5,8
For these reasons, the present study was designed to assess the feasibility, tolerance, results, and efficacy of CAC for truncal varicosities in elderly population over the age of 70.
Methods
Patient selection and study design
This retrospective single-center observational cohort study was carried out between January 2020 and April 2021 in the cardiovascular surgery department of the Yozgat City Hospital, Turkey. CAC procedure was performed in 160 patients (184 limbs) with great saphenous vein (GSV) or small saphenous vein (SSV) insufficiency.
The patients were divided into 2 groups: elderly group, with 30 limbs of 28 patients aged 70 years or older; and younger group, with 154 limbs of 132 patients, who were younger than 70 years. In the elderly group, CAC procedure was performed in 15 (50%) limbs of male and in 15 (50%) limbs of female. In the younger group, CAC procedure was performed in 52 (33.8%) limbs of male and 102 (66.2%) limbs of female. Perioperative data and clinical outcomes were investigated and compared between two groups. All clinical, demographic, and perioperative data were obtained through review of original hospital and physician records.
The research involved patients with GSV or SSV insufficiency diagnosed with colored Doppler ultrasonography (CDUS). The Clinical, Etiologic, Anatomic, and Pathophysiologic (CEAP) classification was used to classify all patients. 9 The following variables were recorded: Visual Analog Scale-Pain (VASP) scores, Venous Clinical Severity Score (VCSS), 10 type of veins treated, mean diameter of the treatment segment, and simultaneous mini-phlebectomy. This research comprised CVI patients who were diagnosed with CDUS by a single radiologist. In all patients, the CDUS procedure was performed while standing, and reflux was assessed using manual compression.
Patients over the age of 20 with CEAP class ≥ C2 varicose veins, GSV diameter of ≥5.5 mm, SSV diameter of ≥4 mm, and venous reflux of ≥2 s were eligible. Patients with a GSV diameter of <5.5 mm, SSV diameter of <4 mm, patients who want other treatment modalities, chronic or acute thrombophlebitis, deep venous insufficiency or thrombosis, allergy to local anesthetics, systemic infection, hypercoagulability condition, pregnancy or lactation, previous treatments using other procedures, congenital vascular malformations, symptomatic peripheral arterial disease, and pulmonary embolism were excluded.
A single cardiovascular surgeon evaluated all patients by using CDUS prior to the operation. The CAC procedures were carried out in a sterile operating room under local anesthesia. General or spinal anesthesia was not administered to any patient. The same surgeon immediately assessed the efficacy of the vein ablation using CDUS following CAC. Patients were asked to return for a follow-up examination 2 weeks later. Further follow-up visits were conducted 6 and 12 months following the procedures, during which clinical and CDUS evaluations were performed. A radiologist performed the control CDUS assessment. A cardiovascular surgeon conducted a preoperative and postoperative comparison of clinical outcomes using the CEAP, VASP scores, and VCSS before the intervention, 2 weeks, 6 months, and 12 months after the procedure between both groups. Patients were also advised to attend to the clinic if they had swelling, rash, leg discomfort, red or darkened skin surrounding the painful area, or shortness of breath.
Procedure details
The VenaBlock® (Invamed, Ankara, Turkey) Venous Closure System was used for all CAC procedures under ultrasound supervision (Figure 1). The operation was performed in either a supine or prone position. The patient’s leg was first disinfected and draped in a sterile manner. A 6-Fr introducer sheath was inserted into the targeted vein after administering local anesthesia. The catheter was advanced to the saphenofemoral (SFJ) or saphenopopliteal junction (SPJ), depending on the target vein, and was positioned 3 cm distal to the SFJ or SPJ. The technique involved segmental pullback and target vein-junction side compression after a total of 1.5–2 mL of cyanoacrylate administration into the catheter. During the procedure, injection of cyanoacrylate into the skin and subcutaneous tissues at the exit site of the catheter was prevented. Approximately 30 seconds, the ultrasound probe and manual compression were used to apply a final compression to the ablated target vein segment and junction side. Complete occlusion of the target vein with normal blood flow at the junction level and deep veins was confirmed by CDUS. In our clinical practice, mini-phlebectomies are routinely performed under local anesthesia in the treatment of a small number of accompanying varicose tributaries after CAC ablation of truncal venous insufficiency. Following CAC, a concurrent mini-phlebectomy was performed under local anesthesia. The index leg was wrapped with a full-length elastic bandage and the patients were asked to unwrap it after 24 hours. 6-Fr sheath catheter and components of the VenaBlock® venous closure system.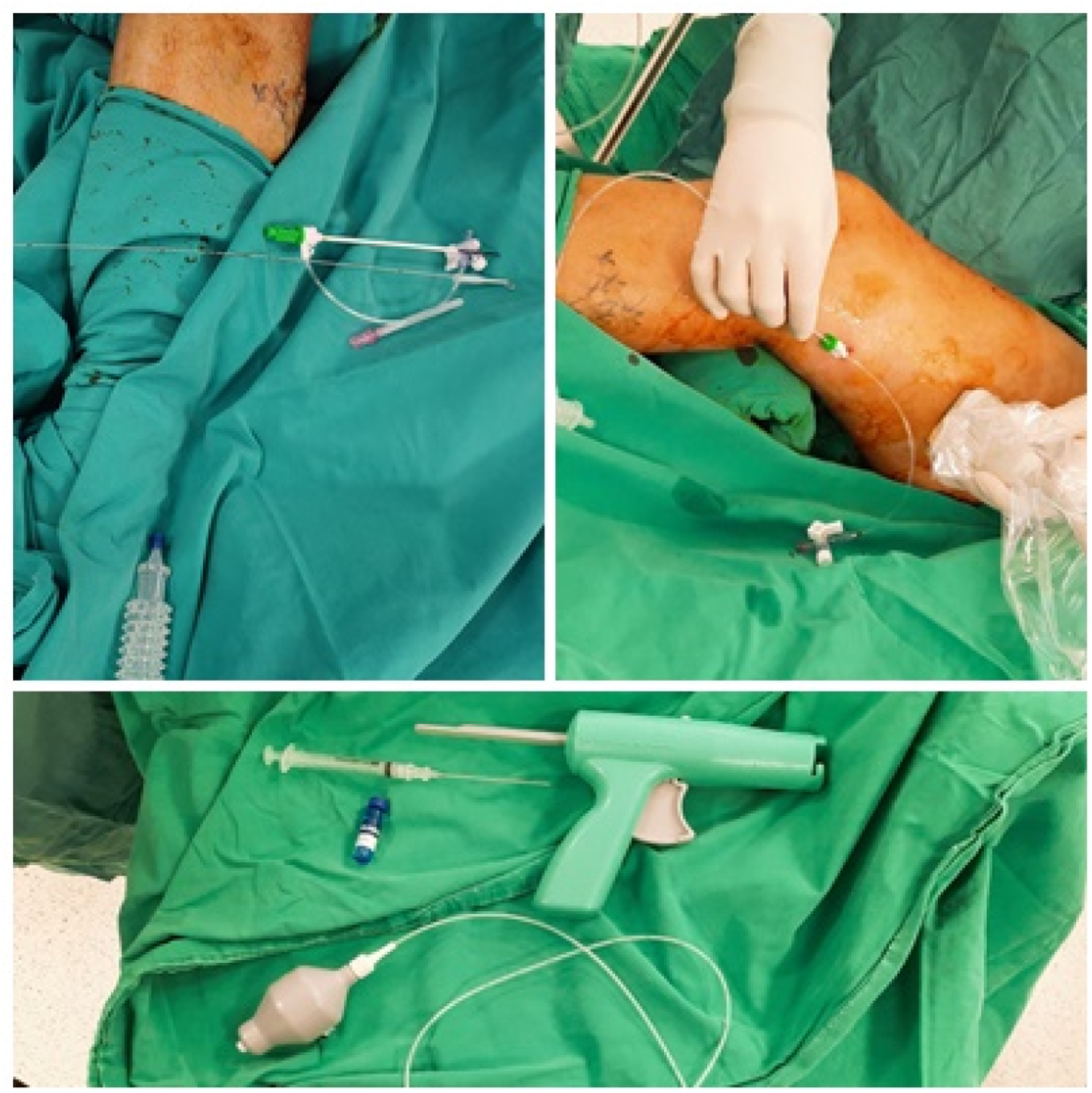
Study endpoints and postoperative follow-up
All patients underwent two-week, six-month, and twelve-month follow-ups, and CDUS evaluations were performed to collect outcome data. The radiologist assessed CDUS of the treated target vein before the procedure and during the follow-up period.
The primary outcome of this study was to assess the feasibility, tolerance and safety of the CAC procedure for truncal varicosities in elderly population over 70 years. The VCSS and occlusion rate of the treated target veins of the patients were evaluated and compared among groups at the two-week, six-month, and twelve-month visits. Total occlusion or nearly complete occlusion (defined as <5-cm segment of flow in the treated vein) of the treated vein was described as technical success. Recanalization or treatment failure was defined as a >5-cm segment of patency in the treated vein. 11 CEAP scores of the patients were evaluated and compared at the twelve-month visits. Tolerance to treatment was assessed using the visual analogue scale of pain (VASP: 0 indicated no pain, 10 represented the worst pain reported by the patient), with the patient being questioned immediately after the procedure was completed. Furthermore, tolerance was evaluated using the VASP for all patients two weeks after the procedure.
The secondary outcomes were to evaluate and compare technical success, mortality, major adverse events, incidence of PLAR and other postoperative complications between the groups.
Statistical analysis
All statistical analyses were performed on IBM SPSS 23.0 (IBM Inc., Chicago, IL, USA) software. Continuous variables were expressed in mean ± standard deviation (SD) and range (min–max) values. Categorical variables were expressed in number (n) and percentage (%). Chi-square test was used to compare the two groups for nominal variables. The continuous variables showed normal distribution or not was evaluated with Shapiro Wilk’s test of normality, and homogeneity of variance was evaluated with Levene’s test. Mann–Whitney U test was used to compare two groups for continuous variables without normal distribution. Three-level comparisons were analyzed using the Kruskal–Wallis-H test in cases where there was no normal distribution. Cumulative survival and complete occlusion rates were analyzed using the Kaplan–Meier method. For all tests, p value of <0.05 was considered statistically significant.
Results
Subject characteristics
Baseline demographic, clinical characteristics, and procedural details of the patients.

COPD = chronic obstructive pulmonary disease; CHF = congestive heart failure (CHF).
Data presented as mean ± standard deviation or number (%).*: p < .05 chi-square test, Mann–Whitney U test.

CEAP classification changes at baseline and 12 months between two groups. CEAP = clinical, etiologic, anatomic, and pathophysiologic.
Clinical outcomes
All operations were carried out under local anesthesia. There were no technical failures or device-related complications. Anatomic success rate was 100% after procedures. The surgeon’s immediate post-procedural ultrasonographic examination confirmed complete occlusion in all of the treated target vein segments. Each treated target vein was occluded on CDUS immediately after the procedures, and all veins remained occluded at 2 weeks after in both groups. Complete 12-month follow-up was available for 26 of 28 patients (92.9%) in the elderly group. During the follow-up period, four months after the procedure, an 86-year-old female patient died of pulmonary edema caused by CHF. The other patient (86-year-old female) died 1 week after the operation due to deep vein thrombosis (DVT) and pulmonary embolism (PE). At the six-month follow-up, two patients (7.7%) had partial recanalization in the elderly group. Complete twelve-month follow-up was available for 131 of 132 patients (99.2%) in the younger group. In this younger group, eight months after the procedure, a 57-year-old female patient died due to gastric adenocarcinoma. In the younger group, there was no mortality or major adverse events such as PE related to the procedure during the follow-up. Partial recanalization was observed in seven patients (5.3%) at twelve-month follow-up.
Cumulative occlusion rates were calculated with use of the Kaplan–Meier method. The occlusion rate for the elderly group at 2 weeks, 6 months, and 12 months was 100%, 92.3%, and 92.3%, respectively, while the occlusion rate for the younger group was 100%, 97%, and 94.7%, respectively. There was no significant difference in occlusion rates between two groups (p > .05) (Log Rank = 0,231) (Figure 3). The cumulative complete occlusion rate was calculated by the Kaplan–Meier method for between-group comparisons.
Evaluation of VCSS changes before and after the procedure between two groups.
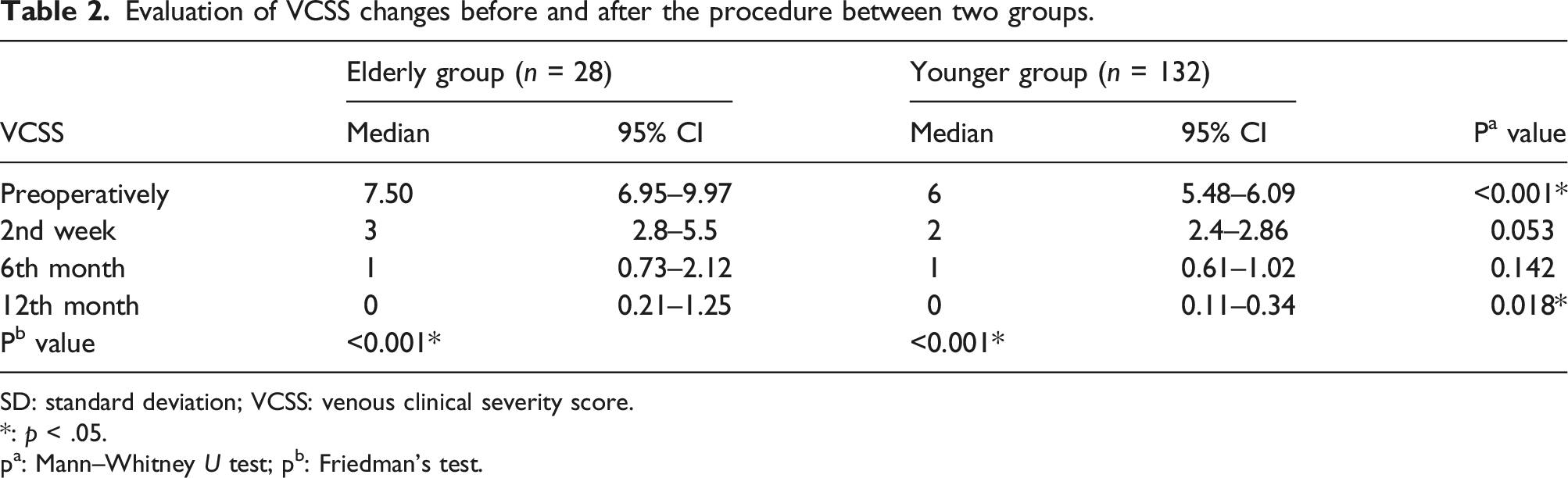
SD: standard deviation; VCSS: venous clinical severity score.
*: p < .05.
pa: Mann–Whitney U test; pb: Friedman’s test.
VASP score changes between two groups during 2 weeks.
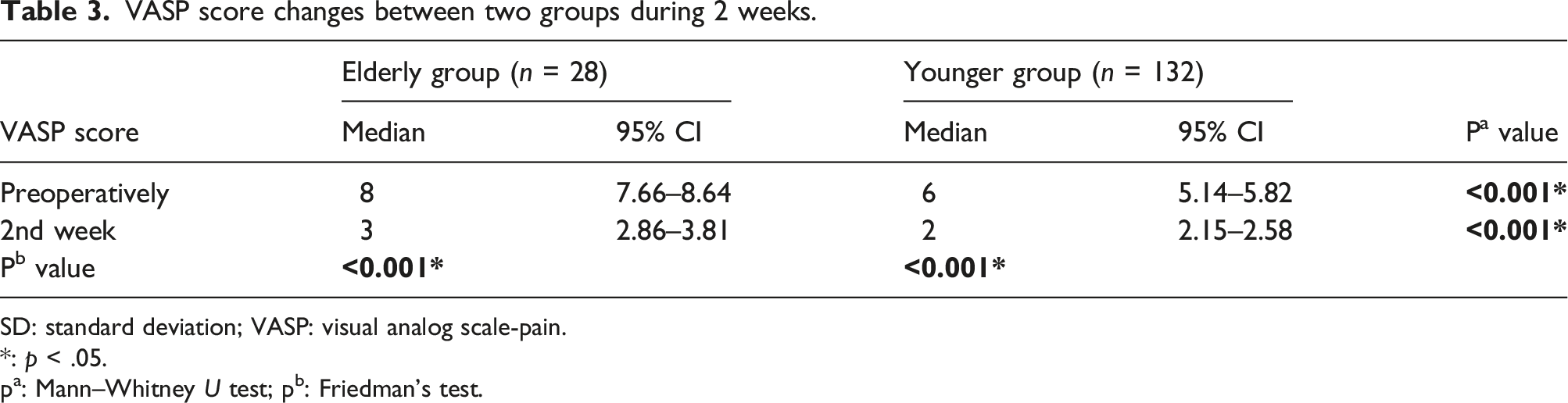
SD: standard deviation; VASP: visual analog scale-pain.
*: p < .05.
pa: Mann–Whitney U test; pb: Friedman’s test.
Adverse events
Complications.

PLAR: phlebitis-like abnormal reaction; DVT: deep venous thrombosis.
Discussion
The number of elderly adults with varicose veins is increasing in proportion to the growing elderly population. 12 Despite admission with early stage CVI is uncommon in the elderly adults, these individuals admit to the vascular surgery clinics, particularly with advanced manifestations of the disease such as hyperpigmentation, stasis dermatitis and venous ulcers. 13 In support of this notion, in the present study, venous insufficiency was more severe in the elderly group, with significantly more C4 to C6 of the classes of the CEAP clinical classification in the elderly group than youngers before the interventions. However, elderly patients predictably have more comorbidities than youngers. 13 This is consistent with the findings in our study that elderly patients had more advanced disease like HT, COPD and CHF at their initial evaluation. Until recently, the standard strategy in the treatment of CVI in the elderly population was to use MCS and venotonic medications rather than endovenous or surgical intervention. 14 Unfortunately, CVI symptoms deteriorate in this population as a result of ineffective conservative therapy. 15 The elderly population’s inability to wear MCSs unassisted and low compliance with treatment are the primary causes of ineffective conservative treatment.12,16 As a result, when the symptoms seriously impair the patient’s quality of life, an aggressive approach should be considered in addition to medical therapy. The initial treatment approach in our study cohort was conservative therapy (i.e., compression therapy, leg elevation, venoactive drugs). Venous ablation treatment was advised for patients whose symptoms persisted or worsened over a 12-month period, whose activities of daily life were impaired, or who were unable to use MCS due to discomfort. However, the type of treatment strategy to be applied should be determined by individual evaluation for the patients. At this point, the risk-benefit ratio, as well as the patient’s expectations and decision, are crucial in making the treatment decision. In this age group, the most important criterion should be evaluating the patient’s physical condition and improving their quality of life. 17
Endovenous procedures are less invasive than surgical treatment and are associated with faster postoperative recovery times, less discomfort, and fewer complications such as hematoma, groin infection, and nerve injury. 18 In the treatment of CVI, these procedures have been recommended for the treatment of VVs by the Society for Vascular Surgery and the American Venous Forum. 19 Many factors determine the optimum treatment strategy, including the stage of the venous lesion according to the CEAP classification, anatomical location of the lesion, vein diameter, treatment cost, symptoms, and age-dependent concomitant diseases. Endovenous techniques have been an effective treatment choice in the last two decades, particularly in the elderly population. 20 While published studies suggest that these techniques result in considerable clinical and symptomatic benefits, there is no specific publication regarding the CAC procedure in the elderly population yet.5,8,21 When compared to CAC, other ablation methods are associated with more treatment-related discomfort throughout the patient recovery period. 22 In support of this opinion, tolerance of the treatment at two weeks after CAC procedure was excellent in both groups in the present study. Furthermore, general anesthesia was found to be a significant predictor of adverse events such as pulmonary and neurologic complications. 23 To avoid these complications, all CAC procedures in this study were performed in a sterile operating room under local anesthesia. As a result of this experience, neither group had any technical failures or device-related complications linked to the choice of anesthesia.
Because it is less invasive, the CAC procedure may be a strong alternative to other procedures in older population. In recent years, CAC has been widely used as an innovative approach for the treatment of CVI.24–26 It offers various advantages over thermal ablation, including the avoidance of tumescent anesthesia, the lack of nerve damage, and the possibility for patients to return daily activities without restrictions. 27 During the COVID-19 pandemic, CAC played a significant role in the treatment of symptomatic patients under local anesthesia and with the possibility of outpatient therapy.24,27,28 Encouraging occlusion rates of target veins after CAC procedure have been reported in several studies and meta-analyses.29,30 However, an age-specific randomized-controlled study of the outcomes of CAC procedures has not yet been published. It may be considered that CAC procedures for superficial trunk varices may be performed with low risk rates in the elderly population. In the present study, each treated target vein was occluded on CDUS immediately after the procedure, and all veins remained occluded at two weeks control in both groups. Only two limbs of elderly group and seven limbs of younger group showed evidence of partial recanalization on follow-up. Although patients with recanalizations had relatively larger diameter varicosities than other patients, statistical evaluation could not be performed about this subject. At 2 weeks, 6 months, and 12 months of follow-up, there was no difference between the two groups in terms of complete occlusion rates of the treated target vein. As a result, age does not appear to have a role in the development of recanalization after the CAC procedure.
In our series of 160 patients, only one patient in the elderly group died 1 week after the procedure due to DVT and PE. However, there were no serious complications or deaths in the younger group during the perioperative period. Although the present study has promising results about the effectiveness of the CAC procedure for the elderly population, it is difficult to comment on the safety of the procedure. Prospective randomized-controlled trials with larger sample sizes, on the other hand, may be essential in establishing more precise conclusions about its safety. In our clinical practice, CAC is performed more often in an operating room and under local anesthesia. Patients are discharged on the same day after the procedure. In this case, compared to other procedures, the operation is well tolerated, with minimal peri- and postoperative discomfort. 31 In addition, the CAC procedure prevents the consumption of painkiller tablets in elderly patients who are more prone to presenting renal insufficiency. 31 In the present study, both groups showed statistically significant improvement in VASPs between baseline and 2 weeks following procedure. Tolerance and satisfaction were identical for elderly and younger patients. Furthermore, the improvement of VCSSs and CEAPs in both groups was found statistically significant between baseline and 12 months after procedure. These findings suggest that objective improvement not only in venous disease but also in patient-reported symptoms of heaviness, achiness, swelling, throbbing, itching, and appearance.
Complication rates in previous CAC procedure series vary from 3% to 25%.32,33 The overall postoperative minor complications of all patients in the current research were similar between previous studies, with no significant variations between age groups. Because it is a non-tumescent and non-thermal technique, the CAC procedure causes minimal injury to the surrounding tissues and nerve structures. Therefore, the possibility of pain and paresthesia after the procedure is reduced. 34 This is supported by the lack of any symptoms or signs of sural nerve damage, hematoma, or phlebitis in both groups in the current study. Furthermore, vascular surgeons must be aware of PLAR as a complication of CAC, which might lead in morbidity in patients. Erythema, edema, pruritus, discomfort, and tenderness over the treated vein are characteristics of PLAR. It typically resolves within 2 weeks. 35 Localized ecchymosis, tightness, and PLAR were found more frequently in our elderly patients, although there was no statistically significant difference between the age groups. PLAR was a mild to moderate severity and well-tolerated occurrence in both groups, with erythema and itching limited to the skin overlaying the treated target vein. Two weeks of administration of NSAIDs and an antihistamine pomad were sufficient to alleviate symptoms. Furthermore, while severe complications such as DVT and PE are less common with CAC procedure compared to other approaches, it should be highlighted that these complications may directly contribute to morbidity and mortality rates, particularly in the elderly population.29,30 Major complications were more prevalent in the elderly than in the younger group in our study cohort. One of these patients (86-year-old female) was intubated after DVT related PE and died on postoperative day 7. Due to the development of DVT in the other patient (an 80-year-old male), anticoagulant medication was initiated on the fourth postoperative day. At the 6th month follow-up, the patient’s symptoms regressed. In order to decrease postoperative complications, we revised the administration of CAC in accordance with the findings of clinical experience and discussions in the literature. 27 These revisions may result in a considerable reduction in this complication.
The elderly group’s comparatively low complication, mortality, and recanalization rates following the CAC procedure, as well as high patient satisfaction and clinical improvement, may be regarded as encouraging outcomes for future investigations. It should be considered that CAC operations may be performed under local anesthesia to improve patients’ quality of life and reduce complications in the fit elderly population. Unfortunately, due to the study’s methodology, it would be unable to make a conclusive comment regarding how effective or necessary CAC procedures are in the elderly. However, to verify these results, comparative, prospective, long-term, randomized trials remain essential.
Limitations of the study
The results of this study had certain limitations. The aim of this study was to evaluate feasibility and efficacy of CAC in elderly patients. It was not aimed to provide an answer to the topic of what is the best treatment for superficial CVI in elderly adults. The main limitation is that this is a retrospective study and single-center nature with a limited sample. There is no record of long-term outcomes. However, to verify these results, comparative, prospective, long-term, randomized trials remain essential.
Conclusions
Age appeared to have no effect on the early and mid-term prognosis of the CAC procedure performed in the study cohort. There was also no statistically significant difference in postoperative complications between the two age groups. CAC procedure may improve the quality of life of elderly population. However, early outcomes suggest that age may be a risk factor for complications. Although it has some potential risks, it is conceivable that the CAC procedure may be applied in selected fit elderly patients for the treatment of CVI. Further long-term randomized clinical trials are necessary to get a definitive conclusion on the efficacy of this treatment in elderly adults.
Footnotes
Acknowledgements
The material has not been previously published or submitted elsewhere for publication and will not be sent to another journal until a decision is made concerning publication by Phlebology.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This retrospective study has been conducted in accordance with the principles of the Helsinki Declaration and approved by the research ethics committee of Bozok University (No: 2017-KAEK-189_2022.05.12_03). Written informed consent was obtained from each patient.
Guarantor
GY.
Contributorship
Görkem Yiğit (Study design, Data collection, Data analysis and Writing).