
Abstract
Introduction
Vascular malformations (VascM) are difficult to diagnose and manage because of their heterogeneous presentations. Ultrasound represents the first imaging exam for patients with vascular malformations. In some cases, additional and sometimes functional imaging will be necessary to confirm the diagnosis or to highlight a vascular network of drainage. Doppler ultrasound could be not enough and a certain number of complementary examinations are then required. Contrast-enhanced ultrasound (CEUS) is used in current practice in the vascular field and in particular the monitoring of aortic stents.
Method
We present here the interest of using CEUS in VascM through a review of the literature. The search was carried out from Pubmed from 1975 to 2023 using the following keywords « vascular malformation » and « contrast enhanced ultrasound » / « venous malformation” and “contrast enhanced ultrasound”/ “venous malformation and contrast enhanced ultrasound”.
Results
The first search found 887 articles. Among them, 124 articles were retained after the selection of the formats. After reading the abstracts, only 9 articles were retained due to the non-selection of articles dealing with other explorations or irrelevance, as they did not deal with vascular malformation. At the end, 17 articles were selected.
Discussion and conclusion
CEUS allows very usefull dynamic analysis of the perfusion in the diagnosis of VascM . CEUS with time analysis is a promising imaging method for the evaluation of perfusion before and after percutaneous treatment of vascular malformations. Area under the curve reduction indicates therapy-induced changes in perfusion. Nevertheless, CEUS is not yet a standardized test for diagnosing or characterizing peripheral vascular malformations. However, its safety allows it to be used for the diagnosis and even the follow up of the VascM. Unfortunately, we haven’t been able to find any randomized studies comparing CESU with other techniques.
Introduction
Vascular malformations (VascM) are difficult to manage because of their heterogeneous presentations. The first step will be to confirm the diagnosis with slow or fast flow vascular malformation and to classify it according to the the International Society for the Study of Vascular Anomalies (ISSVA) classification. 1 Ultrasound represents the first imaging exam for patients with vascular malformations. It is the first line of non-invasive examination and can be sometimes sufficient. 2 In some cases, additional and sometimes functional imaging will be necessary to confirm the diagnosis or to highlight a vascular network of drainage. 3 The aim will be to establish the extension of the VascM as well as the hemodynamic connection, especially in pre-therapeutic assessment (possibilities of per cutaneous or endovascular access of the lesion and prediction of the drainage veins for diffusion of the sclerosing product). Doppler ultrasound could be not enough and a certain number of complementary examinations are then required.
Contrast-enhanced ultrasound (CEUS) is ultrasound enhanced by injection of a specific non-iodinated contrast agent through an intravenous route. CEUS is used in current practice in the vascular field and in particular the monitoring of aortic stents. In some cases, it allows to avoid the use of tomographic scanning with the potential side effects of the injection of iodinated contrast product.
We present here the interest of using CEUS in VascM through a review of the literature. We will address the question of the interest of CEUS in the exploratory and therapeutic time as well as the possible perspectives of this technique.
Method
A review of the literature was conducted on the use of contrast ultrasound in the exploration of vascular malformations. Two authors (AA and SB) carried out the bibliographical research in parallel with the different keywords. The search was carried out from Pubmed from 1975 to 2023 using the following keywords « vascular malformation » and « contrast enhanced ultrasound » / « venous malformation” and “contrast enhanced ultrasound”/ “venous malformation and contrast enhanced ultrasound”. For the search “venous malformation and contrast enhanced ultrasound”, only the formats of type « clinical trial », « meta-analysis », « randomized controlled trial » and « review » have been retained. Articles dealing with « contrast-enhanced magnetic resonance imaging », « contrast-enhanced tomographic scanning » and « contrast-enhanced echocardiography » were excluded. Publications dealing with pathologies other than vascular malformations were excluded.
Result
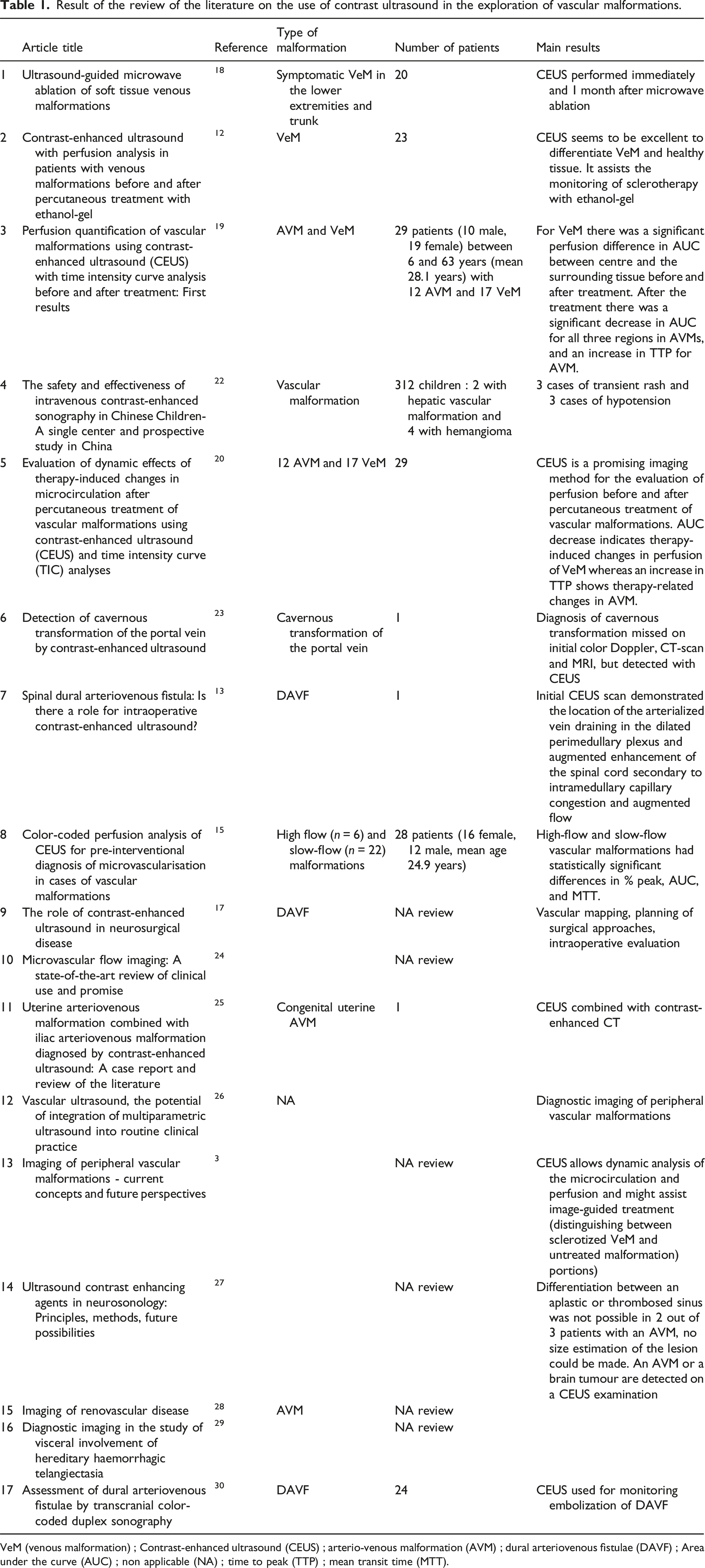
The first Pubmed search from 1975 to 2023 using the following keywords “vascular malformation” and “contrast enhanced ultrasound” found 887 articles (Figure 1). Among them, 124 articles were retained after the selection of the formats of type « clinical trial », « meta-analysis », « randomized controlled trial » and « review ». After reading the abstracts, only 9 articles were retained due to the non-selection of articles dealing with « contrast-enhanced magnetic resonance imaging », « contrast-enhanced tomographic scanning » and « contrast-enhanced echocardiography » (Figure 1). Articles (N = 17) were excluded on the grounds of irrelevance, as they did not deal with vascular malformation. At the end, 17 articles were selected. The types of vascular malformations found and the number of cases with CEUS are shown in Table 1. Reviews were mentioned without specifying the number of patients (not mentioned in journal articles) (Table 1). Flow chart of the method of the review of the literature conducted on the use of contrast ultrasound in the exploration of vascular malformations. Result of the review of the literature on the use of contrast ultrasound in the exploration of vascular malformations. VeM (venous malformation) ; Contrast-enhanced ultrasound (CEUS) ; arterio-venous malformation (AVM) ; dural arteriovenous fistulae (DAVF) ; Area under the curve (AUC) ; non applicable (NA) ; time to peak (TTP) ; mean transit time (MTT).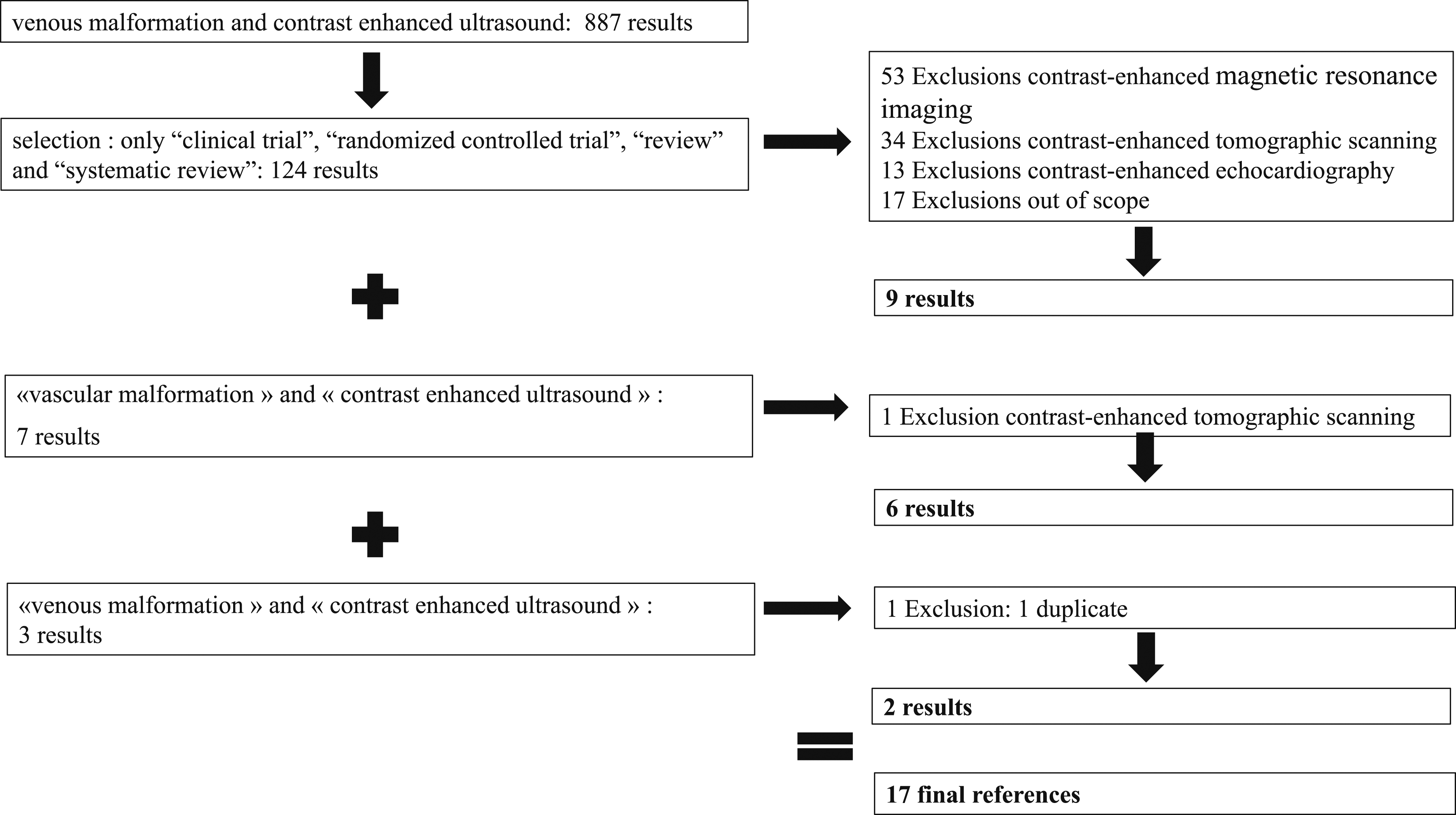
Discussion
Although a review of the literature found little evidence for the use of CEUS in VascM , the articles were unanimous on the value of this exam in VascM, both diagnostically, therapeutically and for the follow up.
Presentation of CEUS
Ultrasound contrast agent (UCA) are microparticle markers of the vascular compartment that enter into resonance in harmonic imaging. Their use in current practice, after intravenous injection, enhances the Doppler echo signal for the study of cerebral vascularization and large vessels. 4 These microbubbles are eliminated by the respiratory route. When used in conjunction with harmonic imaging, they can be used to study the real-time enhancement of parenchyma, particularly in the liver and kidneys, 5 enabling us to study the micro-vascularization that would otherwise escape Doppler echo study. Correlations have been shown between temporal muscle enhancement data and muscle capillary vascularization. 6 This technique is already used in routine practice, particularly in the vascular field, as the evaluation of endoleaks after Endovascular Stent Repair of Abdominal Aortic Aneurysm. 7 In some cases, this avoids the need for injected CT scans, with the potential side-effects of iodinated contrast injection.
In the vascular field, CEUS is used in supra-aortic trunk pathologies to differentiate between carotid or vertebral occlusion and pre-thrombotic stenosis, to assess carotid plaque neovascularization suggestive of plaque instability, 8 and to identify vertebral or carotid dissection. 9 It can be an additional tool for characterizing inflammatory diseases of large vessels and the aorta. 10 CEUS imaging techniques are based on the detection of the microbubble signature by specific imaging modes. They are generally based on the cancellation and/or separation of the linear tissue signal and the use of low acoustic pressure makes it possible to limit the destruction of microbulles and to carry out a real-time study by continuing the scans for several minutes with acoustic powers. Lower and lower. Signal management allows you to have a double image, one with almost complete suppression of signals, the other in gray scale at a low acoustic power providing anatomical identification. The widely used contrast agent is the sulfur hexafluoride microbubble stabilized by a phospholipid envelope (SonoVue®,Bracco, Italy). It allows the study of the enhancement of lesions and parenchyma in continuous mode by permanent inconation. Some products such as Levovist® do not allow continuous imaging because they require high acoustic power to resonate the air microbubbles. The practice is fairly standardized due to the use of a single UCA.
The dose of UCA intravenous CEUS applications in adults is a bolus injection of 1 – 2.4 mL microbubbles (SonoVue®, Bracco, Milan) into an antecubital veinwas carried out, followed by an infusion of 10 mL NaCl. In children the administered amount is estimated depending on the body weight. The dose in children is 0.03 mL/kg, the same as for diagnostic imaging, up to a maximum of 2.4 mL per injection, with an infusion rate of 0.5–1.0 mL/min. 11 UCA are very well tolerated with a low incidence of side effects. They are not nephrotoxic and do not interact with thyroid metabolism. There is no need to check kidney function. UCAs are contraindicated during pregnancy and breastfeeding. Vigilance must be exercised in patients with severe heart failure. They are not recommended in coronary artery disease. There are serious anaphylactoid reactions that require precautions similar to those for other contrast agents.
Diagnostic contribution of CEUS in VascM
Vascular malformations VascM are complex congenital lesions comprising an abnormal network of interconnecting vascular channels. They are difficult to manage because of their heterogeneous presentations. First should the lesions be established with the correct diagnosis. Doppler ultrasound is the first line non-invasive examination. It is particularly effective in determining the types of flows (fast or slow). Gray-scale US coupled with color and pulsed wave Doppler is possible to assess both morphological characteristics as well as hemodynamic features useful for diagnosis and allows the delineation between slow-flow lesions (often venous and lymphatic malformations) and high-flow lesions (arteriovenous malformations (AVM)).2,3 It provides information on the hemodynamics often superior to magnetic resonance imaging (MRI). But Doppler ultrasound alone is sometimes not enough efficient. A disadvantage of ultrasound imaging is the lack of precision regarding malformations located in deep tissues, limitation by bone or lung artifact or with regard to the involvement of adjacent critical structures such as the larynx/ pharynx. The Doppler ultrasound has its limits: it depends on the experience of the investigator, as respective parameters such as pulse repetition frequency and color-gain have to be adjusted accordingly. Nevertheless, Doppler ultrasound is usually sufficient to classify the vascular malformation according to the to the ISSVA classification. 1 Sometimes, Doppler ultrasound is not sufficient and additional functional imaging will be necessary to confirm the diagnosis or to establish the vascular network of drainage 3 and the extension (level of cutaneous/subcutaneous/muscular or bone infiltration). All with CEUS identified parameters seem to be excellent tools for differentiating between VascM and healthy tissue. 12 This is how CEUS is used in well-established complementary examinations for morphological characteristics, the extent of the malformation and hemodynamics data enable to study the microvascular circulation of VascM. 3 This can be particularly useful in evaluating deep-seated lesions. CT scans and MRI are, of course, complementary examinations, but CEUS appears to be a minimally invasive and inexpensive examination upstream of CT scans and MRI and especially effective in terms of hemodynamic analysis. While MRI is the imaging modality of choice for assessing the size and degree of VascM, CEUS can provide further definition of lesions that are more difficult to visualize with Doppler ultrasound. 11 CEUS can display a fast crossing of microbubbles from the arterial to the venous structures in extensive high-flow malformations, sometimes demonstrating multiple shunts when using a high resolution technique. 3 CEUS is by exemple useful in identifying the primary feeding artery within dural arteriovenous fistulas (DAVFs). 13
Thanks to study of 93 patients, Sangwan established an algorithm to diagnose different vascular malformations in CEUS based on the delayed of the enhancement with UCA and the time to peak contrast (TTP) in the lesion. 14 A delayed >30 sec of the enhancement and a slow TTP (>40,47 sec) are in favour of a venous malformation. A early onset (<30sec) of an enhancement and a fast fast (<27,16 sec) are in favour of an arteriovenous malformation (AVM). 14 If the lesion doesn’t take contrast, it’s a lymphatic malformation. Compared with MRI, CEUS had an accuracy of 89.6% in characterizing the type of vascular anomaly. CEUS correctly diagnosed additional cases compared with Doppler-US, which would otherwise have required MRI. 14 According to Teusch in a study with 28 patients, TTP is not a significant factor to determine the nature of the VascM, but it highlights a higher percentage of contrast uptake in AVM than in venous malformations. 15 CEUS can be used for differentiation between the different types of malformations as the percentage of peak enhancement and the area under the curve are decreased in fast-flow malformations while the mean transit time is shorter in slow-flow malformations. 15 Unfortunately, we haven’t been able to find any comparative studies between CEUS and other iconographies.
Contribution of CEUS in therapeutic
Besides diagnostic imaging, ultrasound is the imaging modality of choice for needle guidance during percutaneous sclerotherapy, embolization, or Doppler ultrasound-guided biopsies which is the reference treatment for slow-flow malformations. 16 Before considering endovascular treatment of a vascular malformation, the pre-therapeutic workup should evaluate the possibilities of access to the lesion (per cutaneous or endovascular) but also the anatomy of the drainage veins, especially when considering sclerotherapy. The integrity of a venous network enabling functional deep drainage must be verified, as must the mapping of draining veins (size and proximity of any connections to the deep network). The aim is to anticipate potential releases of sclerosing product with prognostic purposes. Doppler ultrasound is sometimes not enough efficient. In most cases, it underestimates venous malformation volume, particularly in muscle-infiltrating forms, and may perform poorly in non-truncular or very deep drainage veins. A certain number of complementary examinations are then required as MRI or CT scanner. CEUS is a minimally invasive exploration technique that may have a place in the exploration of VascM drainage veins, particularly with a view to treatment. CEUS appears as an adjunct guidance modality during intervention.
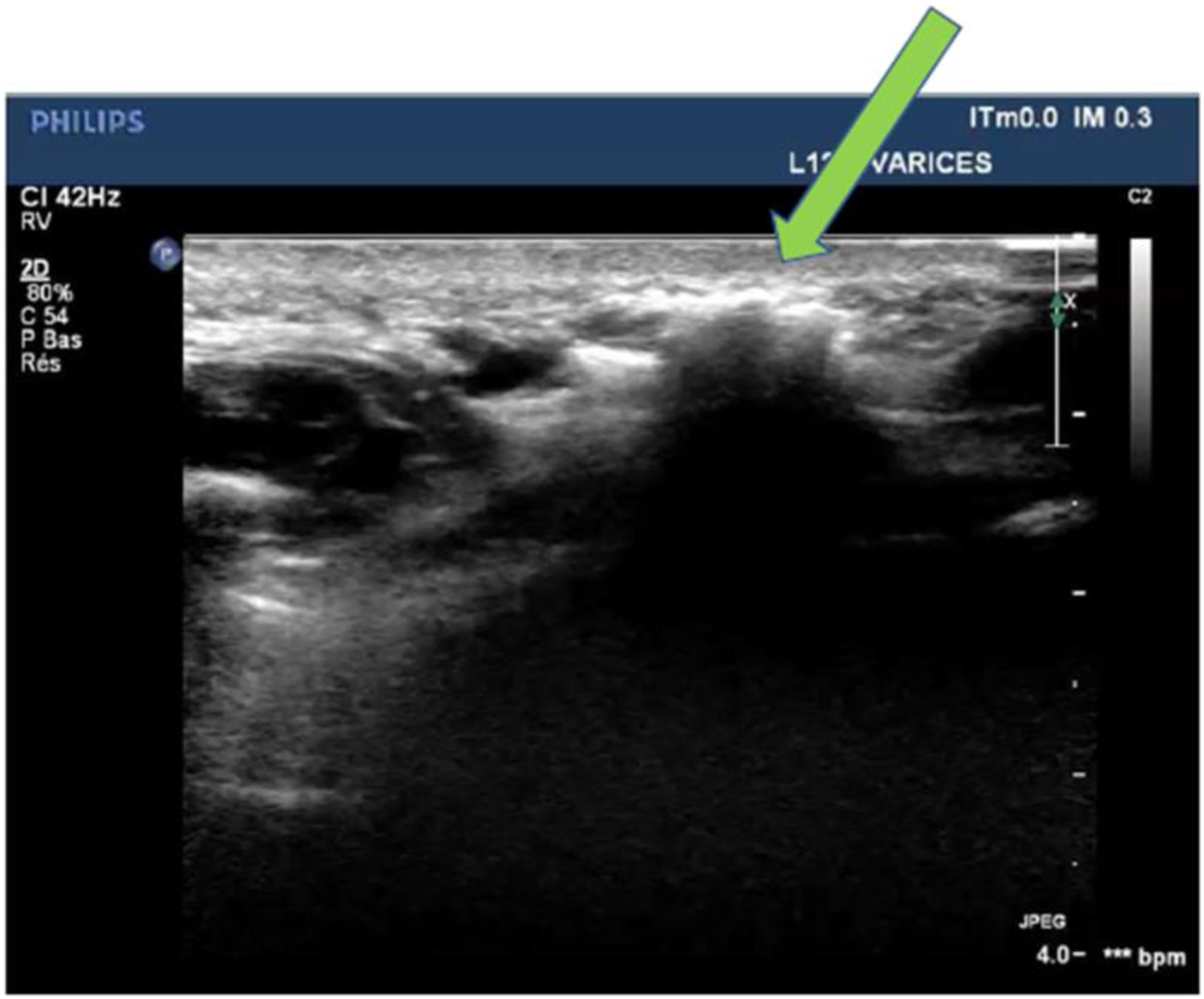
We used this technique in a 35-year-old patient with a vascular malformation of the face in the right cheek (Figure 2(a)). The ultrasonographic appearance was suggestive of a subcutaneous and muscular infiltrating venous malformation. No drainage veins were visualized. The hypothesis was that the Doppler ultrasound underestimated the possible draining veins of this hypoechoic compressive lesion without cyst appearance (Figure 2(b)). CEUS did not reveal any drainage of the venous malformation (Figure 2(c) and (d)). Treatment consisted of a single session of percutaneous ultrasound-guided sclerotherapy with 4 cc of lauromacrogol 400 foam 2% (Figure 3). No diffusion of the sclerosing agent was visualized outside the dimension of the vascular malformation given by the doppler-US, confirming the absence of a drainage vein as previously suggested by CEUS. Venous malformation of the right cheek (green arrow) in a 35-year-old patient/ (a) Echodoppler exploration (b) followed by CEUS (contrast (c) and control (d) Thanks to the patient who gave us his consent for the use and publication of his images. Treatment by sclerotherapy of one venous malformation. Treatment of venous malformation by ultrasound-guided serotherapy with visualization of hyperechoic sclerosing agent (green arrow) and absence of diffusion of sclerosing agent outside the venous malformation. Thanks to the patient who gave us his consent for the use and publication of his images.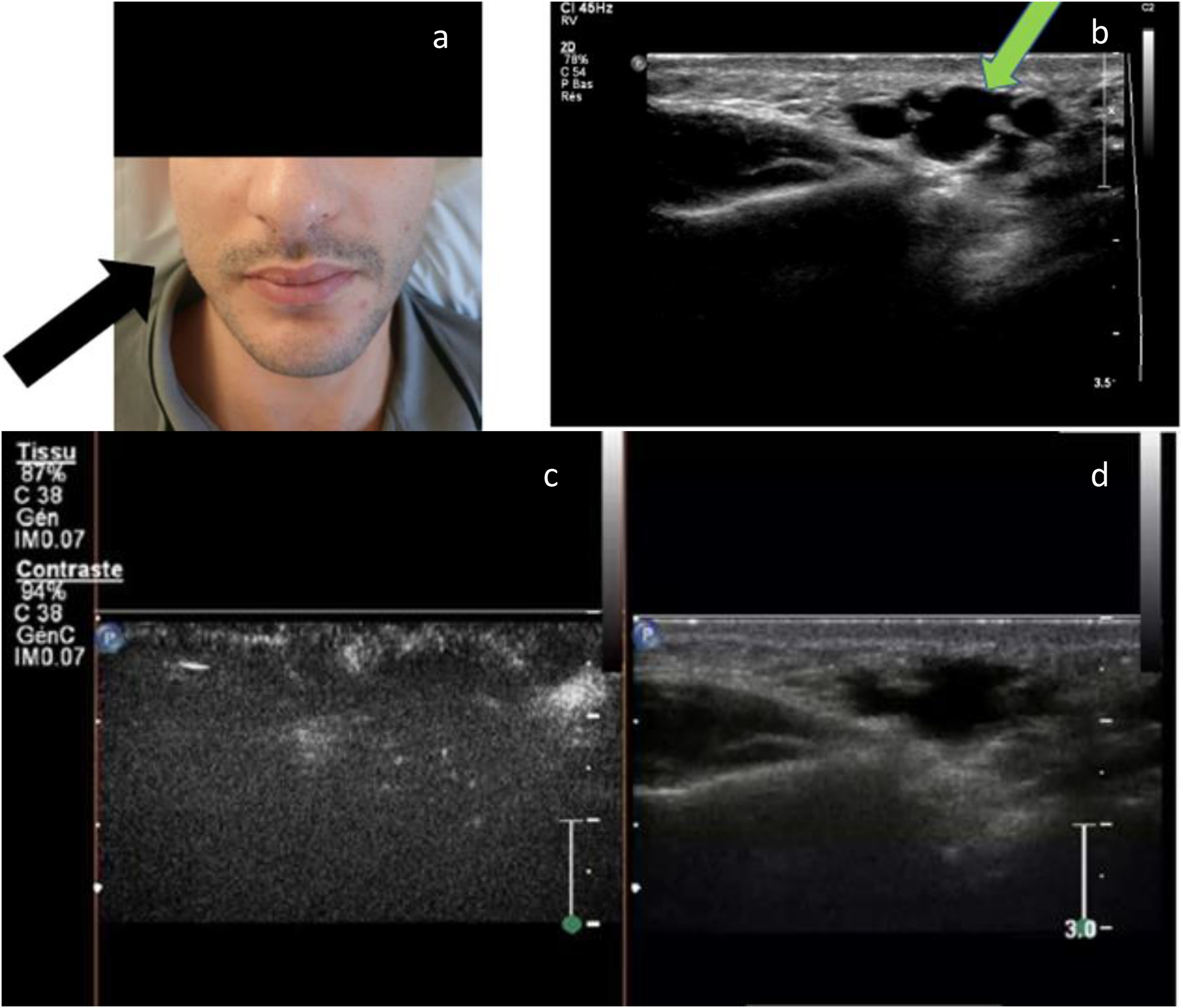
During sclerotherapy, ultrasound is used to guide percutaneous access into the vascular channels of a venous malformation. UCA could be directly injected through the needle into the venous malformation to achieve intralesional opacification. 11 CEUS has superior spatial resolution over fluoroscopy, and might improve visualization of an outflow vein and subsequent occlusion. It decreases the risk of non-target sclerotherapy. According to some authors, in the absence of venous drainage, UCA could be directly injected into the intended treatment area to determine the volume of the lesion being treated. 11 We have not found any study comparing the use of UCA in peripheral intravenous versus intra-lesional injections. Indisputably, CEUS should be performed before foam-agent sclerotherapy because of the presence of air. This could induce limits of sonographic evaluation. These conclusions are applicable to lymphatic malformations. Prior to sclerotherapy of lymphatic malformations, one direct percutaneous injection of UCA into a lymphatic cyst with a needle could be realized before the injection of the sclerosing agent. The differences with venous malformation (especially in macrocysts) is that lymphatic liquid aspiration must be first performed, in an attempt to empty the cyst and to determine the volume of the lesion prior to sclerosis. CEUS can provide information on possible communications between cysts and anticipate the need for several points of sclerotherapy injections if there are no communications with the UCA. 11
Apart from sclerotherapy, some malformations require surgical treatment. CEUS could visualize the fistula in DAVF before disrupting the dura mater. The consequence are a reduction of dural damage and a more precise surgical excision. 13 CEUS allowed real-time visualization before and after ligation of the site of the fistula and blood flow changes occurring in the spinal cord and perimedullary plexus. This tool could be possibly with other imaging modalities such as fluorescence angiography Intraoperative. 13 CEUS allows surgeons to distinguish feeding arteries and the AVM nidus from normal vessels in the evaluation of collateral circulation during the procedure. 17
An other exemple is the use of CEUS realized just immediately after a treatment, like in a serie of 20 patients with venous malformations treated with microwave ablation. 18 If any enhancement was present, supplementary ablation was performed immediately in the residual area. Incomplete ablation was confirmed when CEUS showed a contrast-enhancing area suspicious for a residual lesion in the ablation zone and at 1 month after therapy, CEUS was performed again to assess the ablation. 18
Contribution to venous malformation monitoring
After treatment of Venous Malformation (VeM) with a sclerosing agent, CEUS can also be useful in monitoring VeMs. CEUS with TTP analysis is a promising imaging method for the evaluation of perfusion before and after percutaneous treatment of vascular malformations. 19 Area under the curve decrease indicates therapy (e.g. sclerosing agent)-induced changes in perfusion of venous malformation whereas an increase in TTP shows therapy-related changes in AVM.19,20 In the largest retrospective series of 197 patients (Wiesinger et al 2018) with 135 VeM, 39 AVM, 8 lymphatic and 15 veno-lymphatic peripheral vascular malformations, CEUS was performed before and after the first percutaneous treatment. After the treatment there was a significant decrease for median Area under the Curve (AUC) in VM in the center from 297.8 (14.5-2167.6) rU down to 243.3 (0.1-1678.8) rU (p = .043) and in the surrounding tissue down to 107.7 (20.2-660.2) rU (p = .018). For the other malformations AUC decreased in the center and the margins as well. TTP rose, however these changes did not reach the level of significance.
CEUS might assist image-guided treatment, while distinguishing between sclerotized venous malformation and untreated malformation aera. 12 It can be applied for assessment of the therapeutic success by monitoring the degree of devascularization. Here, CEUS can quantify perfusion changes by using time–intensity curve analysis in digitally stored cine sequences. 12 TTP and mean transit time (MTT) could distinguish between with ethanol-gel sclerotized VeM portions and untreated malformation parts and thereby might assist the monitoring of sclerotherapy. 12
Its use in other vascular pathologies has demonstrated its safety as well as the possibility of repeating the test over time. 21 No ionizing agents are used with CESU, so the examination does not induce the side effects generally encountered with iodinated contrast media, such as kidney failure and/or allergic problems.
Comparison of CESU with other exploratory techniques
Unfortunately, we haven’t been able to find any randomized studies comparing CESU with other techniques. Despite the advantages of CESU mentioned here, this examination is inevitably more invasive than those without injections (e.g. doppler US, CT scan, MRI). CT scan and MRI are, of course, complementary examinations, but CEUS appears to be a minimally invasive and inexpensive examination upstream of CT scans and MRI and especially effective in terms of hemodynamic analysis. Phlebography is probably the gold standard for hemodynamic analysis in VeM but is not systematically necessary and is invasive due to the often painful puncture and injection of contrast agent.
Conclusion
CEUS allows very usefull dynamic analysis of the microcirculation and perfusion in the diagnosis of VascM. CEUS can be successfully applied for assessment of the therapeutic success by monitoring the degree of devascularization of VascM. CEUS with time analysis is a promising imaging method for the evaluation of perfusion before and after percutaneous treatment of vascular malformations. Area under the curve decrease indicates therapy-induced changes in perfusion. Nevertheless, CEUS is not yet a standardized test for diagnosing or characterizing peripheral vascular malformations. However, its safety allows it to be used for the diagnosis and even the follow up of the VascM.. Unfortunately, we haven’t been able to find any randomized studies comparing CEUS with other techniques. Future research studies are needed to firstly better characterize the CESU criteria for MeV and AVMs in order to include CESU in the diagnostic work-up of vascular malformations.
Footnotes
Acknowledgements
Thanks to the patient who gave us his consent for the use and publication of his images.
Author Contributions
S. Blaise: manuscript writing, A.Achiti: C.Seinturier: S.Blaise: bibliographic search, data analysis, proofreading of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Grenoble University Hospital, France.