
Abstract
Background
It is mostly challenging to ablate great saphenous vein (GSV) completely including the below-knee level.
Objective
The aim of this study was to evaluate the effectiveness of cyanoacrylate ablation (CAA) and catheter directed foam sclerotherapy (CDFS) combination in full length ablation of GSV with mid-term results.
Materials and Methods
Patients undergoing CAA and CDFS of the GSV between January 2015 and December 2021 were reviewed. Preoperative and postoperative CEAP class, symptoms, recurrence, and Doppler findings were compared.
Results
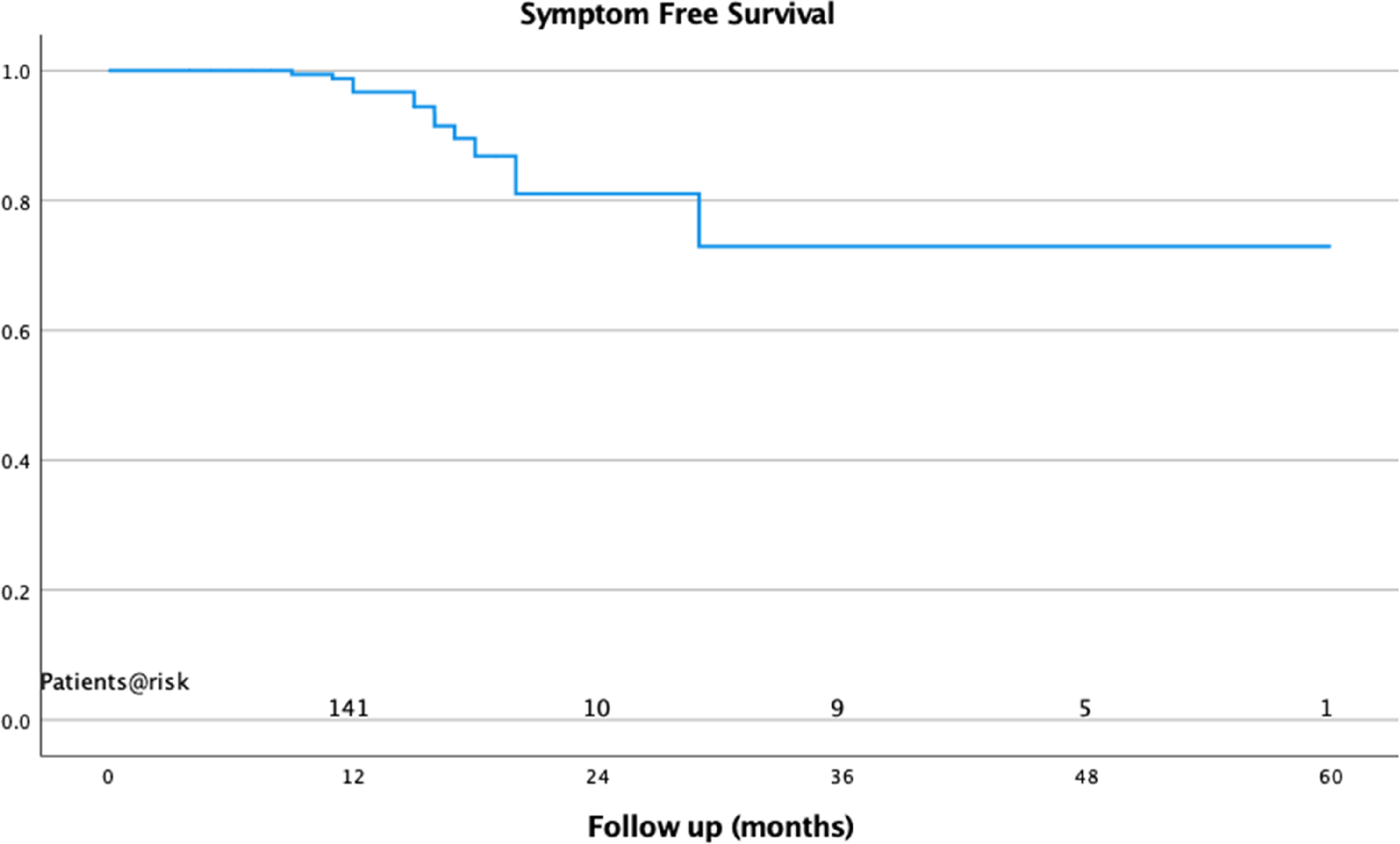
Postoperative overall closure rate at the first year was 99.5% ± 0.01 and at 5 years was found to be 93.8 ± 0.02%. Symptom free survival rate at the first year was 98.8% ± 0.01 and the cumulative 5-years symptom free survival rate was 73.0 ± 0.10%. Venous Clinical Severity Scores decreased from 5.9 ± 1.3 to 0.8 ± 0.4. Aberdeen Varicose Vein Questionnaire scores decreased from 19.7 ± 6.1 to 4.7 ± 1.8.
Conclusion
When techniques are evaluated, CAA and CDFS combination (Glue + Foam) may be preferable as a simple and shorter application with full-length complete occlusion of GSV and less early postoperative discomfort. Long-term outcomes and cost analyses of larger series still need to be documented.
Introduction
Conventional treatments for venous insufficiency are being replaced by newer techniques that can be performed at outpatient clinics. Endovenous laser ablation (EVLA) and radiofrequency ablation (RF) are safe and effective for patients with GSV incompetence, recommended for their high occlusion rates and shorter recovery times.1,2 However these thermal tumescent techniques 3 can cause post operative pain, neural damage caused by thermal energy exposure during operation and bruises caused by multiple needle punctures to deliver perivenous tumescent anesthesia. GSV ablation is typically performed above the knee to prevent sapheneous nerve injury regardless of bleow-knee reflux. Although there are studies describing successful below-knee applications of endovenous thermal techniques, they are not yet routinely used because of the high risk of saphenous nerve injury during below-knee operations.4,5
Foam sclerotherapy is a simple and inexpensive technique but has lower occlusion rates, and potential complications like air embolism, pulmonary embolism, headache and visual disturbances.6,7
A new ablation technique using n-butyl cyanoacrylate (NBCA) avoids tumescent anesthesia and shows promising long term results compared to EVLA and RF ablation.8–10
This study describes a novel technique combining foam sclerotherapy and NBCA which provides high patient comfort and full lenght of GSV ablation.
Material and methods
This retrospective analysis reviewd records of patients treated for GSV insufficiency by the same surgical team.The study was approved by the local ethics committee. The study examined patients who underwent cyanoacrylate ablation (CAA) and CDFS of the GSV from January 2015 to December 2021. The patients were informed about technique and mini-phlebectomy was simultaneously applied to varicose tributaries.
Preoperative and postoperative demographics, Clinical-Etiology-Anatomy-Pathophysiology (CEAP) class, symptoms, and Doppler results were analyzed. Venous Clinical Severity Score (VCSS) and the Aberdeen Varicose Vein Questionnaire (AVVQ) evaluations were conducted pre and postoperatively. 11 Inclusion criteria were symptomatic patients who had CEAP classification of C2-C6 and GSV diameter >5.5 mm with reflux exceeding 0.5 s undergoing CAA and CDFS. The exclusion criteria comprised of reflux of any other vein except GSV, GSV diameter >13 mm, local infection at the puncture site, immobility, peripheral arterial disease, pregnancy, acute thrombophlebitis and acute deep venous thrombosis. Additionally individuals with a known sensitivity to cyanoacrylate and polidocanol were excluded as it stands as the only absolute contraindication for the application of CAA. 12
Procedure
The procedure was performed in an operating room under local anesthesia. The VenaBlock Venous Closure System (Invamed, Ankara, Türkiye) with low viscosity NBCA and a disposable delivery kit was used for CAA application. The GSV was cannulated at the ankle with 6 Fr introducer set under ultrasound guidance. The NBCA catheter was advanced through 6Fr introducer to 3 cm below the saphenofemoral junction (SFJ) and 1.5 ml of NBCA was injected using an injection gun as detailed in a previous study by our team.
10
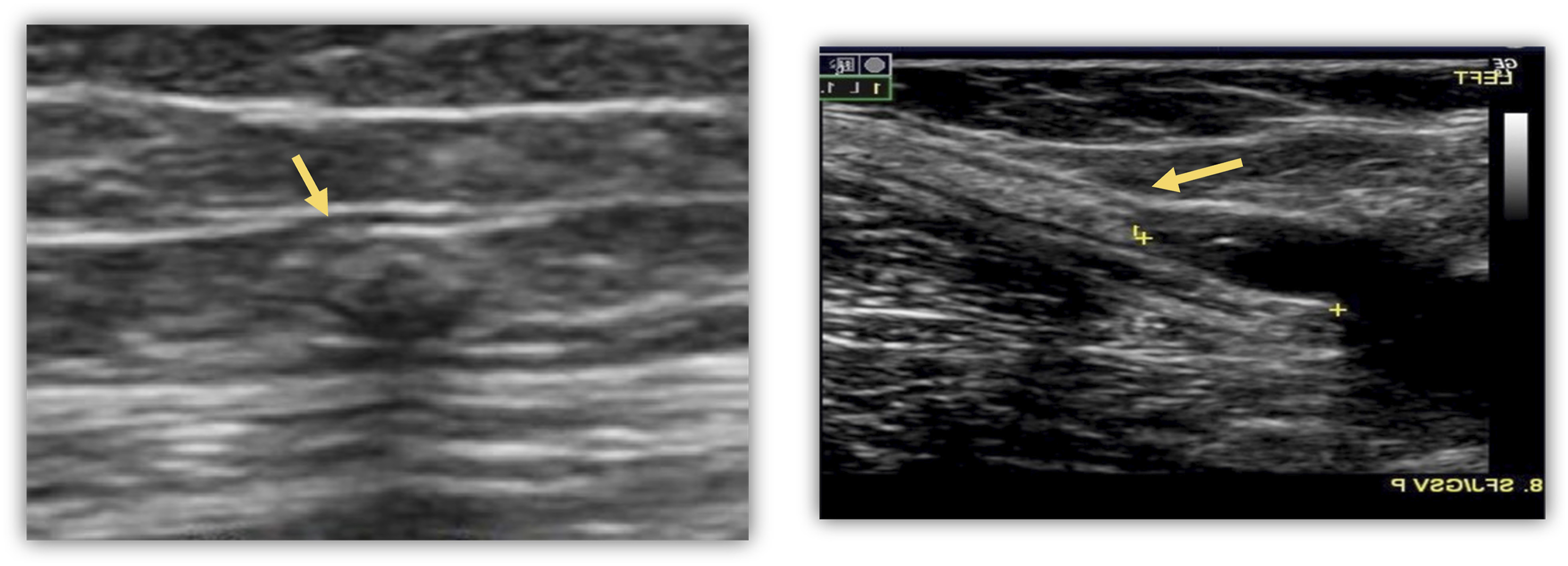
(Images 1 and 2). Access site and application of CAA. Doppler Images showing occluded GSV.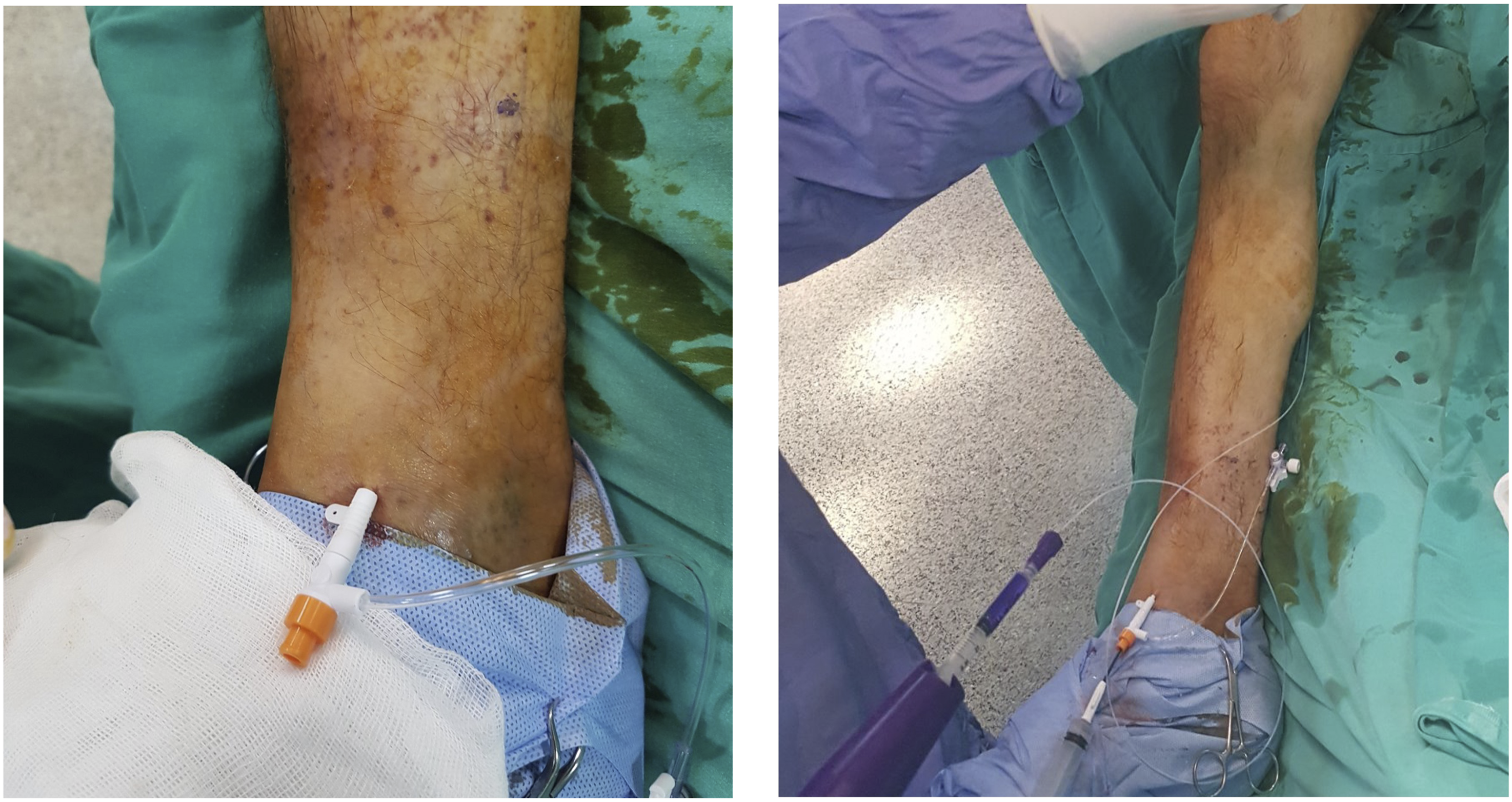
After removing the CAA delivery kit, another vascular catheter was advanced through the introducer placed at the ankle to the endpoint of the polimerized embolizing agent. The extremity was elevated and 10 ml of sclerosant foam prepared with 2 ml of 3% polidocanol (Aethoxysklerol; Kreussler Pharm, Wiesbaden, Germany) was applied. The foam was self made just before the application with Tessari method and applied with a 45° leg elevation. (Image 3). Preparation of foam and application with extremity elevation.
Post procedural management and follow-up
After each procedure, compression bandages were applied fort the first night to all patients, and patients were advised to use compression stockings although it is not routinely recommended. All patients were planned to be discharged on the same day of the procedure and prescribed venoactive medications for 6 months. No activity restrictions were imposed from the first day of the procedure.
Follow-up appointments were scheduled for the first week, and at the 1st, 6th, 12th months, with annual visits thereafter. Doppler ultrasonography was performed to examine GSV occlusion. CEAP clinical class, symptoms, VCSS and AVVQ were regularly recorded. Treatment success was defined as the closure of GSV with no discrete patent segment of more than 5 cm in the treated portion of the GSV.
Statistical analysis
Statistical analyses were conducted utilizing SPSS version 21 (IBM Corp., Armonk, NY) with a significance level of p < .05 was considered statistically significant. Categorical variables are presented as frequencies and percentages, while continuous variables are expressed as means with corresponding standard deviations. Patient characteristics and outcomes were compared employing the T-test for continuous variables and the Chi-square or Fisher exact tests for categorical variables. Event-free survival and closure rates were examined through Kaplan-Meier analysis.
Results
Preoperative demographic. Operative and postoperative variables of the patients in two Groups.
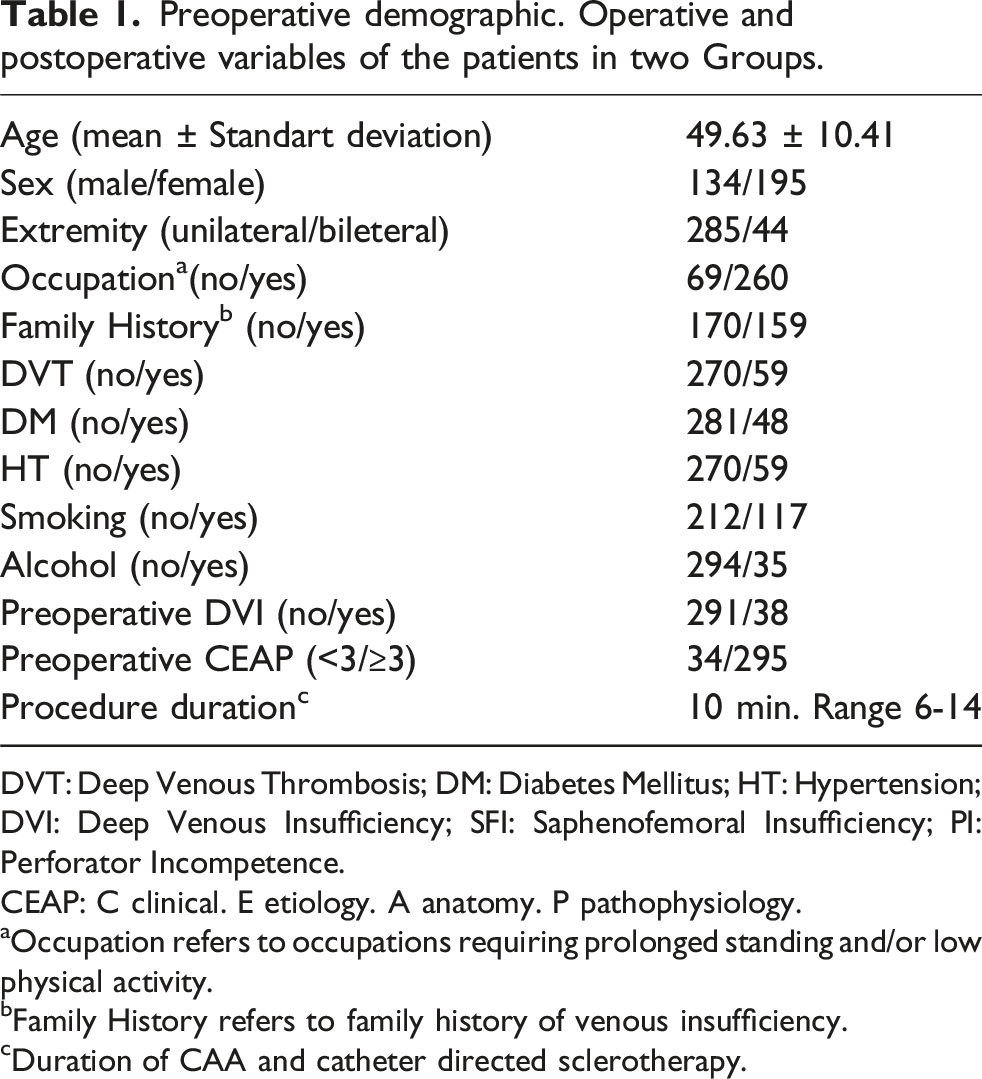
DVT: Deep Venous Thrombosis; DM: Diabetes Mellitus; HT: Hypertension; DVI: Deep Venous Insufficiency; SFI: Saphenofemoral Insufficiency; PI: Perforator Incompetence.
CEAP: C clinical. E etiology. A anatomy. P pathophysiology.
aOccupation refers to occupations requiring prolonged standing and/or low physical activity.
bFamily History refers to family history of venous insufficiency.
cDuration of CAA and catheter directed sclerotherapy.
Preoperative and postoperative CEAP classification of patients.
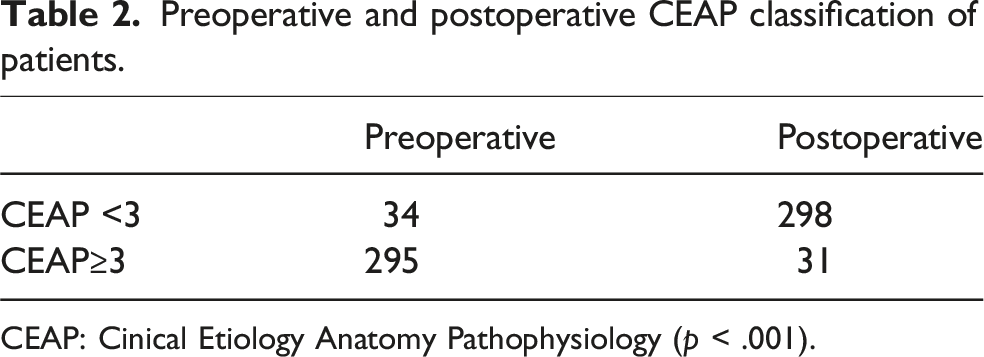
CEAP: Cinical Etiology Anatomy Pathophysiology (p < .001).
Preoperative and postoperative disease severity and Impact on Quality of Life.
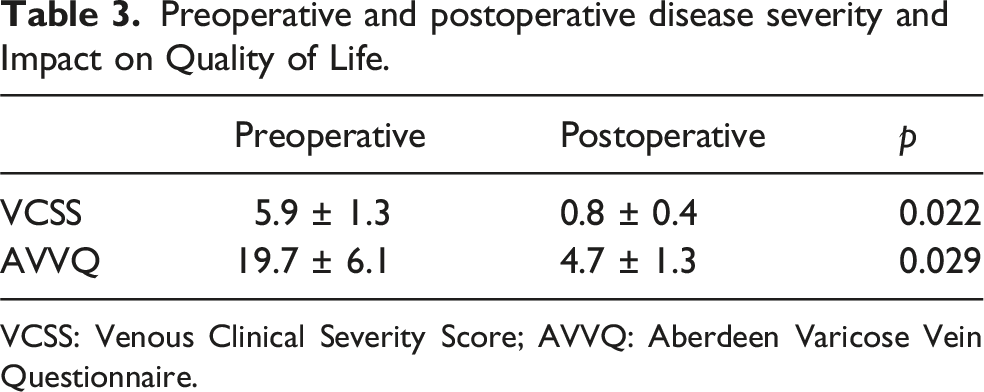
VCSS: Venous Clinical Severity Score; AVVQ: Aberdeen Varicose Vein Questionnaire.
Total occlusion rate at the first year was 99.5% ± 0.01. The 5-years total occlusion rate was 93.8 ± 0.02%. (Figure 1). Symptom free survival rate at the first year was 98.8% ± 0.01 and the cumulative 5-years symptom free survival rate was 73.0 ± 0.10% (Figure 2). Total Occlusion in 5 years: 93.8%±0.02. Standard error never exceeded 10%. Symptom-free survival in 5 years: 73.0%±0.10 Standard error never exceeded 10%.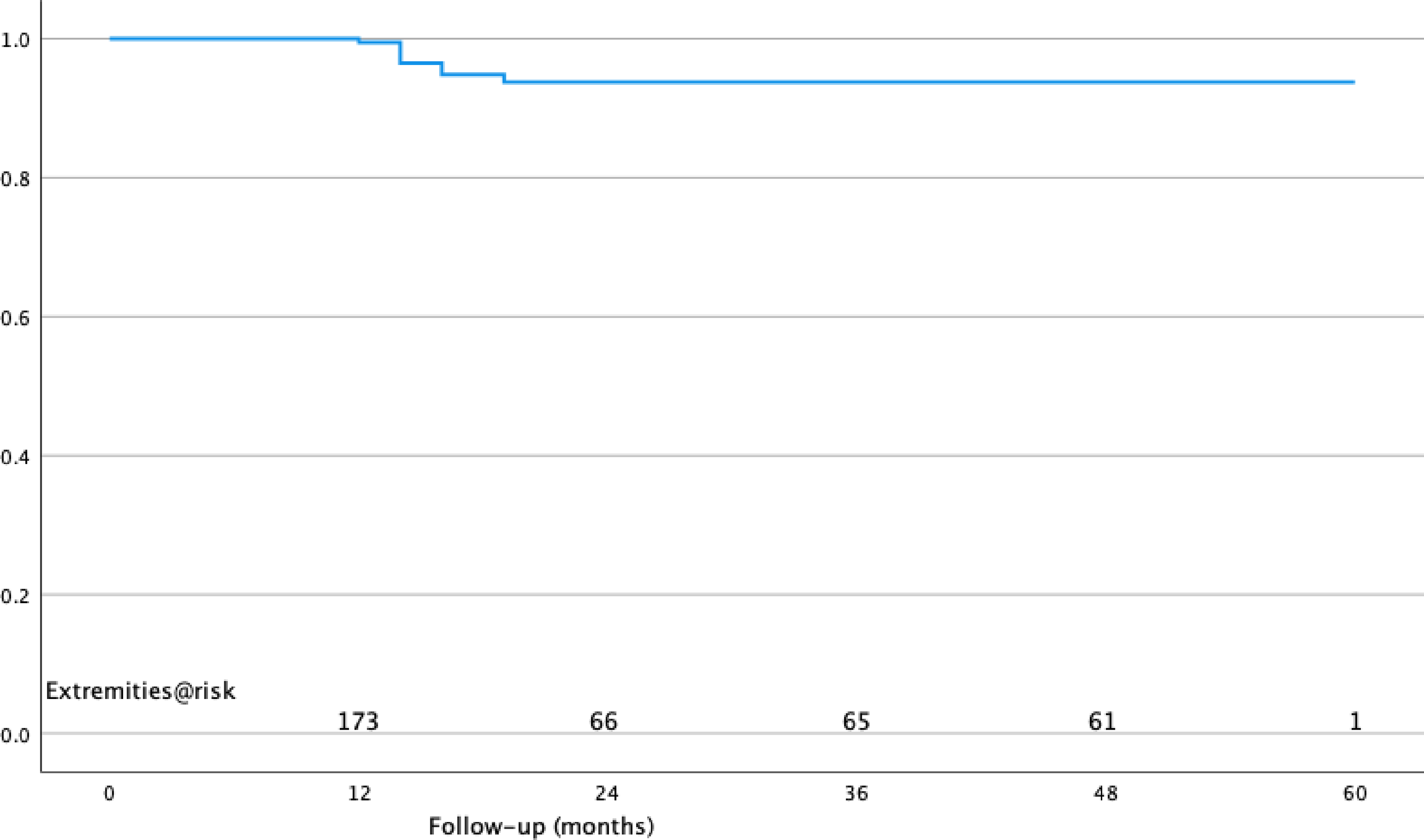
Discussion
Varicose veins and discomfort have an important place in daily practice of a cardiovascular surgeon. Venous insufficiency, with a prevalence of 30-40% in Western societies, decreases self confidence and efficiency of patient because of the physical and cosmetic problems that it causes. Thus, making it a siginificant clinical and social issue. 13
The most common cause of varicose veins and associated symptoms is SFJ incompetence with reflux extending to GSV.14,15 Consequently, eliminating reflux is the first treatment step to prevent persistent symptoms and recurrence. 16 The classical method for achieving this is ligation and division of SFJ.
In recent years, venous insufficieny treatment has become less invasive, with patients demanding minimal or even no incisions, and faster recovery. Consequently conventional surgical techniques are being replaced by newer, less invasive techniques.
EVLA and RF have proven to be safe and effective techniques for patients with GSV incompetence. However some patients may experience recanalization of the GSV. 17 Tumescent anesthesia, which requires multiple needle punctures, and pain caused by thermal damage are also limiting factors for the preference of these techniques.
Foam sclerotherapy is a low-cost, less painful alternative to EVLA and RF. Using a simple method described by Tessari, durable foam is formed with a three-way valve and two syringes. 18 Although studies have shown favourable results with sclerosant foam, the literature indicates the inferiority of ultrasound guided foam sclerotherapy compared with other endovenous techniques.6,19,20 Improved results have been achieved with catheter delivery, ensuring even foam distrubution throughout the vein.20,21
Cavezzi et al. identified the gas component as a key factor affecting the sclerosant foam formation, safety and possibly efficacy. 22 Tessari proposed a 1/4 liquid-to-air ratio as optimal for forming dense, durable sclerosant foam after conducting studies with different gas compounds and ratios. 23
In this study sclerosant foam was prepared using Tessari’s method with a liquid-to-air ratio of 1/4. To enhance turbulence a 5 ml and a 10 ml syringe with a three-way valve were utilized. The openings of the three-way valve were rotated approximately 45° for further increase in turbulance, which is important to form dense and long-lasting foam as described in Cavezzi’s study. 22
A 2004 study showed that patients undergoing RF ablation without ligation had more small vessel networks and GSV recanalization at the SFJ compared to those with ligation. 17 Another studty by Uurto et al. reported that ultrasound guided foam sclerotherapy resulted in a reduction of CEAP and VCSS in 63% of patients after 3 months 6 In another study CDFS closure rates were 94.3% at 1 year and 89.4% at 3 years 20 However, this low success rate led to reinterventions and decreased patient satisfaction. All of these findings highlights the importance of SFJ and branhes originating from SFJ on recurrence and patient satisfaction. İslamoğlu introduced a simple and successful technique combining high ligation and CDFS, while Bountouroglou et al. introduced a similar technique, with differences in foam application method.24,25 İslamoğlu preferred CDFS, whereas Bountouroglou utilized ultrasound guidance with the critical distinction being the even distrubution of foam to the vein achieved with the catheter.
A new non-tumescent, non-thermal ablation technique that offers comparable results to thermal tumescent techniques with low viscosity NBCA has been introduced. Daylan and İslamoğlu presented findings indicating a 91.1% overall closure rate at 5 years and a 72% 5-years symptom-free survival rate. These results are consistent with the 5-years extension study of the Veclose trial and other studies comparing CAA with thermal tumescent techniques.10,26–28 A recent Cochrane review also documented similar results for CAA in terms of technical success and recurrence. 29
EVLA, RF and NBCA are mostly applied above knee segment. Some researchers also perform limited GSV segment stripping. 30 These studies report symptom improvement after ablation/stripping of the above-knee segment. The theory suggest that below-knee reflux extends from the proximal part will be treated due to pressure reduction after the procedure.
The opposing theory is that reflux in the below-knee segment persists after above-knee ablation. Turton et al. explained that primary insufficiency, structural weakness of this segment, and altered hemodynamics cause neoreflux.31,32 Van Neer et al. reported that 91% of patients who underwent above-knee stripping had persistent reflux in the below-knee segment at 2-years follow up. 30 Theivacumar reported 51% of the patients treated with EVLA above-knee segment have reflux in the below-knee GSV and 89% of the patients with significant below-knee reflux required reintervention. 33 Similary, another study reported a 70% return of below-knee reflux. 15 Below-knee segment reflux is observed in 9%-15% of patients with varicose veins who have a normal SFJ. The extend of reflux affects the incidence of symptoms; with reflux extending to distal causing more symptoms than reflux extending more proximally. 14 Hong’s recent study found persistent below-knee GSV incompetence after above-knee ablation at 6 and 12 months in 61% of patients supporting the idea of structural weakness occuring before the ablation. 3 Additionally, persistent below-knee insufficiency may increase venous pressure leading to a recurrence of varicose veins.
The main purpose of this study is to achieve full lenght ablation with minimal incision while ensuring high patient satisfaction and avoiding complication. Kayssi et al. reported successful cases with coil embolization and foam sclerotherapy combination, but this approach is not aligned with the current minimally invasive trend that can be performed on an outpatient basis. 34 NBCA offers satisfactory result but it is not possible to achieve full length ablation at least in our country. The social security system pays only 1,5 ml of embolizing agent which is insufficient for both above and below-knee ablation.
Therefore we prefered NBCA solely for above-knee, proximal ablation and CDFS for below-knee ablation. This combination provided satisfactory results in long term follow up. In a study comparing the 5-years results of RFA and CAA, the preoperative and postoperative CEAP, VCSS and AVVQ score were similar with our study population. It is possible to claim that this combination offers similar clinical results. 10 (Tables 2 and 3) Also overall closure rate and estimate of symptom free survival rate were similar.
Another notable aspect of this study was the low rate of complicaitions and short duration to return to normal daily activities. Notably, there were no recorded cases of DVT and none of the patients complained from nerve injury. Sapheneous nerve injury is a common complication of venous insufficiency surgery, as the sapneous nerve runs alongside the GSV, particularly in the crural portion, providing sensory innervation to mostly medial aspect of the lower extremity. 35 Injury to this nerve causes paresthesia such as tingling, numbness, hypo or hyperesthesia or burning sensation. The technique offered CAA and CDFS, achieves complete ablation without causing nerve damage due to direct trauma during stripping or heat injury, as seen in thermal ablation techniques. Both CAA and CDFS can be performed under local anesthesia with only one puncture as they are non-thermal non-tumescent. This feature allows the procedure to be performed almost entirely in an outpatient clinic, enabling same day discharge and a rapid return to daily routines.
Our study has several limitations including its retrospective design, lack of comparative data about alternative technique, incomplete data on -the length of vein treated, pre and post operative CEAP distribution and perioperative pain, and a short median follow up time. Additionally, detailed analysis of recurrence sign and symptoms is lacking.
Conclusion
The proposed combination aligns with current treatment trends, often involving only one puncture wound and same-day discharge, minimizing institutional resources. This technique also avoids complications like DVT or nerve damage, as well as the pain, bruising, and paresthesia associated with other thermal tumescent ablation techniques. When all techniques are evaluated, CAA and CDFS combination (glue + foam) may be preferable as a simple and shorter application with full-length complete occlusion of GSV and less early postoperative discomfort. However long-term outcomes and cost analyses in larger series are still needed.
Footnotes
Ethical considerations
This study was approved by the ethics committee of Ege University Medical Researches, number 24-3T/55.
Author Contributors
AD and Fİ conducted the literature review and designed the study. AD and Fİ contributed to developing the study protocol. SK; Kİ gained ethical approval. AYK and Fİ managed patient recruitment. AD and Fİ made data analysis and prepared the initial draft of the manuscript. All authors participated in revising and refining the manuscript and provided final approval of the submitted version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Study institution
Study performed in Ege University Faculty of Medicine Department of Cardiovascular Surgery.
Previous Presentations
UIP World Congress of Phelebology, September 12-16 2022, İstanbul, Türkiye.
Guarantor
Fİ.