
Abstract
A child’s diagnosis with autism spectrum disorder (ASD) can be an extremely stressful time for families. Researchers suggest that the period immediately following ASD diagnosis is a key time for professionals to guide families by providing appropriate information about support options. This article describes a family support program, developed by Autism Spectrum Australia (Aspect). The Early Intervention Readiness Program (EIRP) is delivered during the challenging post-diagnosis period. During program involvement, families are provided with information and management strategies related to ASD-associated behaviors, and support options are identified. The EIRP aims to strengthen family confidence and facilitate a smooth transition into appropriate early intervention services. Preliminary program evaluation outcomes indicate that following program involvement, participants perceive a significant increase in their confidence in their understanding of ASD and capacity to independently make decisions about related supports. Participant post-program evaluations also verify the EIRP to be a useful post-ASD diagnosis support.
Autism spectrum disorder (ASD) is characterized by persistent difficulties with communication and social interaction, with accompanying restricted or repetitive behaviors (American Psychiatric Association, 2013). The prevalence of ASD diagnosis is continuing to rise (Hansen, Schendel, & Parner, 2015), and there is a parallel increase in the demand for appropriate intervention and support services (Nedft, Koegel, Singer, & Gerber, 2010).
A child’s diagnosis with ASD is an event rarely forgotten by families, and the stressful nature of the process of ASD assessment and diagnosis is well documented (Braiden, Bothwell, & Duffy, 2010; Keenan, Dillenburger, Doherty, Byrne, & Gallagher, 2010). It is therefore acknowledged that the provision of specialized information and support immediately following a child’s ASD diagnosis is crucial (Cutress & Muncer, 2014; Keen, Couzens, Muspratt, & Rodger, 2010). General information on ASD and treatment options can be made available to parents by the assessment service provider during the diagnostic process (Rhoades, Scarpa, & Salley, 2007). It is however also recognized that many families are not offered the individualized information needed to effectively understand their child’s diagnosis and unique challenges, and to facilitate informed decision making about the interventions and supports most suitable for their family (Banach, Iudice, Conway, & Couse, 2010; Dunst, Trivette, & Hamby, 2007; Mansell & Morris, 2004; Shields, 2001). Moreover, when professional guidance following a child’s ASD diagnosis is inadequate many parents can feel overwhelmed (Valentine, Rajkovic, Dinning, & Thompson, 2010).
Inadequacies or hesitation in the provision of professional guidance following a child’s ASD diagnosis may be reflective of shortcomings in the training of diagnostic professionals about the extensive range of ASD-associated behaviors and empirically supported treatment options (Skellern, McDowell, & Schluter, 2005). Consequently, key opportunities for enhancing family knowledge about the disorder, and facilitated referral to appropriate services can be overlooked (Rhoades et al., 2007). Families are known to independently turn to potentially unreliable and overwhelming sources, including the Internet, to source this fundamental information (Grant, Rodger, & Hoffmann, 2016), with confusion and potential delay in the access of suitable intervention supports a common result (Mackintosh, Myers, & Goin-Kochel, 2005). In addition to intensifying family uncertainty and stress, limited access to the information needed for a family to improve their understanding of their child’s ASD behaviors can also have an impact on the outcomes of the early intervention and education programs the family subsequently progresses to engage in (Osborne, McHugh, Saunders, & Reed, 2008; Pisula, 2011; Siller, Reyes, Hotez, Hutman, & Sigman, 2014).
A number of studies have suggested that when parents are supported in developing their understanding of their child’s individual challenges and given effective strategies to self-manage these challenges, a decrease in parent stress and an increase in confidence in their knowledge and autonomy can result (Farmer & Reupert, 2013; Keen et al., 2010; Shields, 2001).
In recognition of the lack of post-ASD diagnosis family support services in Australia, Farmer and Reupert (2013) developed a group parent education program: the “Understanding Autism and Understanding My Child With Autism” (UA) program. The UA program is designed to support families by improving their understanding of the nature of ASD and associated communication, sensory, social, learning, and behavioral difficulties. Within their program evaluation, Farmer and Reupert reported that the UA program can increase parental recognition of their child’s individual challenges and their confidence in managing and supporting their child’s behaviors. A significant decrease in anxiety was also recognized, with the authors attributing this to the parent’s improved ability to independently access appropriate information and support.
The purpose of this article is to describe the Early Intervention Readiness Program (EIRP), a family support program developed in response to the limited availability of comprehensive and individualized support for families during the challenging post-ASD diagnosis period. The core objective of the EIRP is to strengthen parent knowledge and confidence to independently coordinate and commence appropriate early intervention and support services. Information and support is provided about autism-associated behaviors and management strategies. Available intervention and support options are also identified and discussed with parents.
Program Objectives and Development
The EIRP fundamentally acknowledges the lack of professional guidance and the stressful nature of the post-ASD diagnosis period for many families. As such, the purpose of the EIRP is to address this shortfall by offering the personalized information needed to support the family’s understanding of their child’s individual challenges and to develop awareness of the interventions and supports that are relevant and available to their child and family.
The core components of the EIRP derive from a pilot study of the program and a review of the literature which emphasized the importance of the availability of comprehensive and reliable information about ASD (Farmer & Reupert, 2013; Hall & Graff, 2010; Osborne & Reed, 2008). As a result, the provision of accurate and individualized information surrounding ASD-associated behaviors was prioritized during the EIRP development.
Studies have shown that families who have received support during the post-diagnosis period have explicitly acknowledged the value of guidance with navigating region-specific supports (Mulligan, Steel, MacCulloch, & Nicholas, 2010; Russa, Matthews, & Owen-DeSchryver, 2015). For this reason, the EIRP involves professional guidance in identifying local interventions, education, and support options, with the aim of facilitating informed decision making, effective service transitions, and ongoing family engagement.
Other family priorities identified by researchers are the provision of strategies that families can implement at home to manage challenging behaviors (Ludlow, Skelly, & Rohleder, 2012), support communication and interaction (Whitaker, 2002), and source “next step” information (Valentine et al., 2010). While awaiting the commencement of relevant intervention services, families who participate in the EIRP are offered practical resources and strategies to support their child’s skill development and behavior management.
The EIRP is designed as a family-centered program. Family-centered and individualized programs are flexible and responsive to the unique strengths, needs, and priorities of each family (Dempsey & Keen, 2008; Dunst et al., 2007; McConkey et al., 2010). They have also been associated with reductions in parental stress (Russa et al., 2015) and have been strongly linked to parent reports of an increase in their confidence in supporting their child’s behaviors (Espe-Sherwindt, 2008; MacKean, Thurston, & Scott, 2005; Wade, Mildon, & Matthews, 2007).
One core difference between the EIRP and the UA program is the means of service delivery. Financial constraints associated with travel and reliable child care can present a significant barrier for some families, and ultimately can limit the family’s ability to access consistent support (Mackintosh et al., 2005). In consideration of these difficulties, the EIRP is delivered individually to families, predominately within the family home.
Overall, the post-diagnosis support offered through the EIRP aims to strengthen family functioning and foster the expansion of family support networks. Specifically, through supporting a family’s access to relevant and reliable ASD information and resources, the program endeavors to facilitate informed and autonomous decision making about suitable interventions and, in turn, promote a reduction in parent stress.
Program Structure and Implementation Procedures
All components of the EIRP are offered at no cost to participating families. All children involved in the EIRP have either recently been diagnosed with ASD, or have been identified by their referral source as displaying characteristics of ASD, with a confirmed diagnosis yet to be received. Families can self-refer to the EIRP, or be referred by an involved service (e.g., early childhood education setting, public health service) or professional (e.g., pediatrician, psychologist). EIRP sessions are conducted by an EIRP interventionist, being a speech pathologist, occupational therapist, or psychologist. Program interventionists are assigned to families, predominantly based on family location.
Subsequent to family referral to the EIRP, a 30-minute initial phone call is made to confirm their suitability for program engagement. To establish this, families are specifically asked (a) whether they feel they fully understand their child’s ASD diagnosis, (b) whether they have begun to consider or commence any early intervention or support services for their child and family, and (c) whether they are aware of, and are in need of, assistance with applying for any relevant funding opportunities. If, from this initial phone discussion, it is clear that a family is in need of information about ASD and associated services, supports, and funding options, an initial face-to-face consult is offered. Although EIRP consultations are principally delivered within the family home, sessions can also occur in another location (e.g., child’s early childhood education setting) if preferred by a family.
Initial home-based family consultations are 2 hr in duration and involve the development of a Family Service Profile. The Family Service Profile form is a one-page data collection tool, designed for this program to guide family discussion about the services and supports currently being accessed, and those they may be interested in exploring. The Family Service Profile form contains a list of region-specific services and supports across four key areas: (a) assessment (i.e., ASD diagnostic, developmental or cognitive, communication, sensorimotor, and audiological), (b) intervention (i.e., general practitioner, pediatrician, speech language pathologist, occupational therapist, early intervention group program, or specialized playgroup and early childhood education setting or school), (c) family support (i.e., support groups, counseling or family support services, and respite services), and (d) funding (i.e., Australian federal government funding schemes and health care rebates relevant to children with ASD). Any unlisted services or supports identified by families are also recorded. For each Family Service Profile item, families state whether or not they are interested in acquiring further information about the service or support.
During the initial home-based consultation, families are asked (a) whether they require further information about ASD and their child’s specific difficulties and (b) whether they feel they would benefit from the suggestion of some introductory strategies for supporting their child at home. If a family’s responses to these questions, in addition the outcomes of the Family Service Profile, highlight a need for further information and support, a collaborative decision is made with the family to schedule a subsequent 1.5-hr EIRP follow-up session. Only in circumstances where a family advises that they do not require any further information or support is the EIRP service delivery discontinued.
The frequency and total number of subsequent EIRP sessions delivered to each family is dependent upon the extent of their support needs. Although the precise content of these sessions is individualized to suit each family, to enhance the fidelity and consistency of program, the EIRP interventionists are provided with a customized toolkit, which comprises of (a) concise leaflets, fact sheets, and reliable websites offering information about ASD and associated difficulties; (b) a list of ASD-related intervention and support services, including locations and contact information; (c) information about Australian federal government funding schemes, eligibility criteria, and application procedures; and (d) easy-to-read, evidenced-based and Autism Spectrum Australia (Aspect)–developed parent brochures. These brochures include information on relevant home-management strategies including encouraging communication, using visual supports, understanding sensory needs, positive behavior supports, developing play skills, building self-help skills, positive sleep practices, and supporting transition to school. All EIRP interventionists undertake program delivery training upon appointment to the program.
EIRP sessions support families in six areas. These are described in the following sections.
ASD Information
Where an ASD diagnostic assessment has not been completed with a child prior to their EIRP referral, families are supported in managing a diagnostic assessment process. For families with a child who has a confirmed ASD diagnosis and indicate that they wish to improve their current understanding of ASD, the EIRP interventionists review the information and recommendations outlined in the child’s ASD diagnostic report and develop a plan for providing the EIRP. If a comprehensive diagnostic report is not available, families are asked about their child’s functioning in the skill areas of communication, social interaction, play, self-help, motor performance and behavior, as well as their sensory preferences and interests.
At the first meeting with the family, the interventionist discusses general information about ASD and provides concise printed ASD information and resources from the EIRP interventionist toolkit. In subsequent discussions with the families, individualized information is offered that can provide suggestions on managing the strengths and challenges of their child.
Service Information
Where a family is not aware of, or are yet to commence access to the funding support options available to their child (e.g., Australian federal government funding schemes), information regarding the eligibility criteria and application processes are outlined. As needed, the EIRP interventionists also support families in completing funding application forms. During the sessions, intervention supports and education options that are available to their child are discussed. The interventionist ensures that detailed explanations of the roles of different interventionists (e.g., speech language pathologists, occupational therapists, and psychologists) and plain language summaries of evidence-based interventions are provided.
To develop the families’ capacity to locate reputable information, the interventionists inform families of published articles about ASD therapies and services on the Australian Government–supported Raising Children Network website (The Australian Parenting Website, 2015). Relevant region-specific intervention and education service options are provided.
Decision Making
The EIRP interventionists encourage further family discussions about practical considerations for selecting interventions that are best suited to their child and family. These include reviewing service costs, travel requirements, managing family time, and the suitability learning environments.
Service Transition Support
Once the family has selected the service options they wish to pursue, the EIRP interventionists typically support the parents through child service referral process. The EIRP interventionists usually facilitate service transitions by attending initial family appointments, especially in unfamiliar intervention or education settings.
Family Support
Where a family identifies shortcomings in their existing support network and they express an interest in seeking external family support, region-specific options are offered. These regularly include disability-specific parent support groups, face-to-face or telephone counseling services, and respite services. Family referrals to selected services are often supported by EIRP interventionists, through the attendance at initial appointments, where requested.
Management Strategies
While families are awaiting funding approval or service commencement, practical home strategies are discussed. Strategies, based on the information provided in printed brochures, are discussed and demonstrated. Based on their child’s identified strengths and challenges, the EIRP interventionists promote a dialogue about the family’s goals and priorities.
At the beginning of each EIRP session, the information that was introduced during the previous session is reviewed to confirm understanding. Extended discussions or questions about issues that the families are encountering are also encouraged.
The decision to terminate EIRP service provision is made collaboratively with each family. Given the different support needs of each family, there is no prescriptive criterion for program completion. A discussion about service cessation is usually initiated by an EIRP interventionist once a family has indicated that they feel sufficiently confident in their understanding of their child’s diagnosis and challenges, and they have begun to successfully engage in the service and support options investigated during the program involvement.
Evaluation
Participants
Families from the Hunter Region of New South Wales, Australia, participated in this preliminary evaluation of the EIRP. Fifty-seven percent (n = 77) of the 135 referrals were received from other early intervention service providers, including local early intervention referral or support agencies, public allied health staff, and other non-ASD-specific early intervention services. Twenty-eight (21%) direct referrals from parents who had independently learned of the service (e.g., via website or another parent) were also received. The remainder of referrals were received from diagnostic professionals, specifically pediatricians and psychologists (13%, n = 18) and early education setting or school staff (9%, n = 12).
The children referred to the program were aged between 0 and 7 years, with a mean age of 3.8 years (SD = 1.51). Seventy-eight percent (n = 105) of the children who were referred were male. Seventy-one percent (n = 96) of the children had a confirmed diagnosis of ASD prior to their referral to the program, made by either a pediatrician or psychologist. The remaining 29% (n = 39) of the families were awaiting an ASD assessment for their child, or required support to arrange this with a diagnostic professional.
Thirty-four percent (n = 46) of the families who participated in the EIRP had both parents involved in service delivery. This was encouraged to promote shared understanding of information and consistency of strategy implementation. One percent of participating families (n = 2) included the father only, with 61% (n = 83) involving participation of the mother only. In 3% of families (n = 4), one additional member (i.e., grandparent or school representative) participated in the program alongside a child’s mother.
Informed, written consent to participate in the evaluation was obtained from families prior to the commencement of the EIRP. Participation in the evaluation was not a requirement of ongoing program involvement. At any stage, families could choose to withdraw from the program or request the exclusion of their information from the evaluation.
Of the 135 families who were referred to the EIRP within the 20-month research period, 114 received support through ongoing EIRP sessions. Four families withdrew from the program prior to the collection of post-program data. A total of 62 families completed the program within the 20-month program evaluation period (duration of the funding). The mean number of EIRP follow-up sessions conducted with families was 5.8.
Measures
To evaluate the impact of the EIRP on family confidence and their perceptions of the effectiveness of the program, the following measures were used:
Family Confidence Scale
A Family Confidence Scale was created for the purpose of this evaluation and used to examine families’ pre- and post-program confidence. To appraise the clarity and relevance of the questions, the Family Confidence Scale was piloted with six families involved in the EIRP. This data was not included in this program evaluation. The outcome of this pilot was a slight re-phrasing of the questions and structural changes to the measurement tool. As shown in Table 1, the final Family Confidence Scale incorporated six questions, directly related to the six outlined focus areas of the program. Parents rated their responses on a 5-point Likert-type scale: 1 = not at all confident, 2 = slightly confident, 3 = somewhat confident, 4 = very confident, and 5 = extremely confident.
Likert-Type Scale Questions on Pre- and Post-Parent Confidence Measurement Tool.

Note. EIRP = Early Intervention Readiness Program; ASD = autism spectrum disorder.
Both the pre- and post-program Family Confidence Scales were completed in paper form, within EIRP service delivery sessions and with a program interventionist. The potential for participant response bias, particularly following program participation (Beaumont & Sofronoff, 2008) is recognized. The decision for the direct involvement of program interventionists in data collection was deliberate, as the parents had developed a rapport of trust and honesty with their interventionist. Parents completed the post-program survey without any assistance from the interventionists either during the final session, or they took the survey home and posted it back to the program organizer.
Post-Program Survey
A post-program survey was provided to each family who completed their final EIRP service delivery session within the 20-month program evaluation period. Families were offered the option of completing the printed survey either during the session, or afterward, and returning it via post.
The usefulness of the program was evaluated by parents using the post-program survey. As shown in Table 2, the survey incorporated six questions, also derived from the core program focus areas. Parents rated their responses on a 5-point Likert-type scale: 1 = not at all useful, 2 = slightly useful, 3 = somewhat useful, 4 = very useful, and 5 = extremely useful.
Likert-Type Scale Questions on Post-Program Parent Survey.

Note. EIRP = Early Intervention Readiness Program; ASD = autism spectrum disorder.
Outcomes
Family Confidence
The Family Confidence Scale measured changes in the confidence ratings of the 62 EIRP participants who completed the program within the evaluation period. As shown in Figure 1, there was a significant difference in parent pre- and post-program ratings for all six Family Confidence Scale questions. Results suggested that following involvement in the EIRP, families reported an increase in their confidence in their understanding of ASD behaviors, their knowledge and level of access of service, and funding options and their capacity to independently make decisions about services. Families also identified an increase in their knowledge of practical home-management strategies and their confidence in their current family support network.
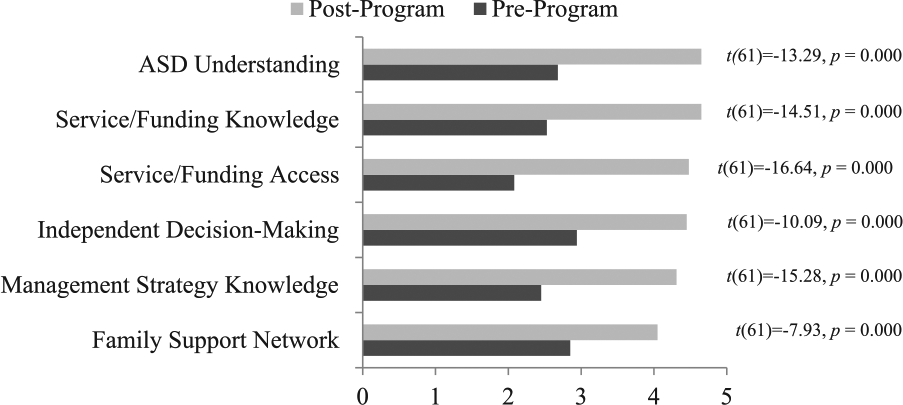
Mean pre- and post-program parent ratings on Family Confidence Scale questions (n = 62).
Program Evaluation
Of the 62 families who finished the program, 55 families also completed a post-program survey that evaluated their perception of the usefulness of the EIRP. A frequency analysis, shown in Figure 2, identified that 84% (n = 46) responded very useful or extremely useful to the six survey questions, outlined in Table 2. These results suggest that the families considered the program to be valuable in developing their understanding of ASD, their knowledge and current level of access of services and funding options, and their independent decision-making capacity surrounding service options. The families also indicated that the EIRP was beneficial in assisting them to expand on their knowledge of strategies to manage ASD behaviors and their current family support network.
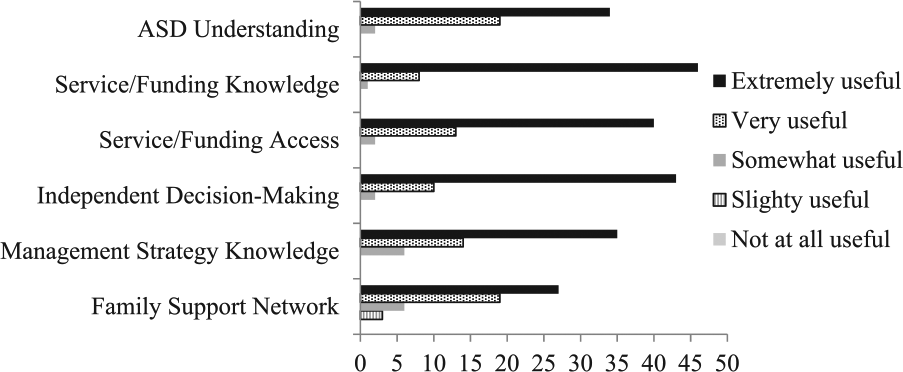
EIRP post-program survey parent responses (n = 55).
Discussion
The outcomes from this preliminary program evaluation suggest that the EIRP, delivered within the challenging post-ASD diagnosis period, significantly increased parental confidence in their understanding of ASD and their capacity to make independent decisions about related supports and services. Participant post-program evaluations also validated the EIRP as a useful means of post-ASD diagnosis support. Despite the need for more extensive research into the impact and effectiveness of the EIRP, overall the findings suggest that the program is beneficial in supporting families in making decisions during the post-ASD diagnosis period.
Program Implications
Although it is acknowledged that children with ASD should commence appropriate intervention as soon as possible, it is also recognized that a sound understanding of the diagnosis is first needed to facilitate informed family decision making and to foster a child’s smooth transition into selected services (Miller, Schreck, Mulick, & Butler, 2012; Osborne et al., 2008). For many families, it is also often difficult to locate reliable information about ASD and how this relates to their child’s individual behaviors and challenges in the post-diagnosis period (Gaspar de Alba & Bodfish, 2011; Gray, Msall, & Msall, 2008).
The EIRP addresses this post-diagnosis information shortfall by providing families with the information needed to develop their confidence in their understanding of ASD and their child’s specific challenges. The finding from the evaluation of the EIRP confirm recent research that has demonstrated that timely access, appropriate frequency, and early intervention and education programs can reduce the need for parents to independently source accurate and individualized ASD information (Farmer & Reupert, 2013; Osborne et al., 2008; Siller et al., 2014).
Family support program engagement can remove the need for families to source ASD information and it has been shown that they can reduce the time delay between the diagnosis and the commencement of suitable intervention supports (Shields, 2001). The results from this evaluation suggest that EIRP engagement can bridge the gap between diagnosis and intervention commencement by supporting parents in accessing services.
Research has highlighted that following an ASD diagnosis confirmation, parents can indicate that it is also then difficult to distinguish which interventions are available and most appropriate for their child (Grant et al., 2016; Valentine et al., 2010). The need to make under-informed decisions about interventions and supports can increase feelings of worry and hopelessness in many families (Mackintosh et al., 2005; Osborne & Reed, 2008; Pisula, 2011). A number of studies have identified that the provision of professional region-specific supports following ASD diagnosis can lead to a reduction in parent anxiety (Farmer & Reupert, 2013; Keen et al., 2010). The EIRP evaluation result concur with these studies as it also found that the provision of supports that are relevant to each child and family led to an increase in parent confidence in accessing relevant ASD support, which in turn improved the parent’s ability to make informed and independent family decisions.
Families also often report feeling “lost” due to the limited availability of information about how to support their child during the post-ASD diagnosis period (Mulligan et al., 2010). Throughout EIRP service delivery, family-specific practical resources are shared with families. The evaluation identified that the increase in their knowledge of strategies that they can do at home to support their child improved their confidence in their ability to support their child.
Offering parents interim professional support during the post-diagnosis period can alleviate family stress during a time when parents can feel that the support network is “doing nothing” (Valentine et al., 2010). Participants in the EIRP evaluation reported improvements in their knowledge of strategies they could use to support their child’s challenges. In future evaluations, we intend to collect data on family stress levels and report on any changes that result after the introduction of strategies to support their child.
Following ASD diagnosis, parents often seek support from their family support network as a means of managing their emotional and physical health (Hall & Graff, 2011). A lack of professional and social supports and networks is the strongest predictor of depression and anxiety in mothers of children with ASD (Boyd, 2002; Gray & Holden, 1992). The EIRP offers individualized guidance in navigating and facilitating access to local family supports. The results from the EIRP evaluation indicated that families who participated in the program felt more confident in their overall family support network as a result of the instruction from the interventionists.
In conclusion, the results from this preliminary evaluation of the EIRP confirms other research that has shown that professional support following a child’s ASD diagnosis can increase family knowledge, confidence, and autonomy. It is expected that this improvement in confidence and knowledge may also lead to a reduction in parent stress, as has been identified in other studies (Farmer & Reupert, 2013; Keen et al., 2010). In light of this, national and international organizations and funding bodies should strongly consider the replication of family support programs, such as the EIRP, where gaps in such services exist.
Future Program Delivery
Ongoing implementation and evaluation of the program could encompass use of standardized measures of parent and child outcomes during their involvement in the EIRP. Specifically, the inclusion of pre- and post-program evaluations of parental stress and child behavior would be valuable in facilitating individualized service delivery and would enable a more objective analysis of the impact of EIRP engagement. A post-program, 2-month follow-up of families could also prove valuable for future program development, as it would provide the opportunity to evaluate whether the management strategies implemented during the EIRP are maintained after the program is finished. In addition, broadening the scope of the EIRP to offer renewed support to families who identify ongoing challenges subsequent to program completion could be considered.
Footnotes
Acknowledgements
We acknowledge the contribution of those involved in the development, delivery, and appraisal of the EIRP including Jessica Fenwick, Eliza Clarke, Joanne McGregor, and Susanna Baldwin. Special appreciation is also extended to the families who have been involved in this program evaluation and to the services that have supported the EIRP through family referral.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This program and research was funded by the Greater Charitable Foundation.